


Abstract
The synthetic leucine amino acid analog anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (anti-18F-FACBC) is a recently developed ligand that permits the evaluation of the L-amino acid transport system. This study evaluated the whole-body radiation burden of anti-18F-FACBC in humans. Methods: Serial whole-body PET/CT scans of 6 healthy volunteers (3 male and 3 female) were acquired for 2 h after a bolus injection of anti-18F-FACBC (366 ± 51 MBq). Organ-specific time–activity curves were extracted from the reconstructed data and integrated to evaluate the individual organ residence times. A uniform activity distribution was assumed in the body organs with urine collection after the study. Estimates of radiation burden to the human body were calculated on the basis of the recommendations of the MIRD committee. The updated dynamic bladder model was used to calculate dose to the bladder wall. Results: All volunteers showed initially high uptake in the pancreas and liver, followed by rapid clearance. Skeletal muscle and bone marrow showed lower and prolonged uptake, with clearance dominated by the tracer half-life. The liver was the critical organ, with a mean absorbed dose of 52.2 μGy/MBq. The estimated effective dose was 14.1 μSv/MBq, representing less than 20% of the dose limit recommended by the Radioactive Drug Research Committee for a 370-MBq injection. Bladder excretion was low and initially observed 6 min after injection, well after peak tracer uptake in the body organs. Conclusion: The PET whole-body dosimetry estimates indicate that an approximately 370-MBq injection of anti-18F-FACBC yields good imaging and acceptable dosimetry. The nonmetabolized nature of this tracer is favorable for extraction of relevant physiologic parameters from kinetic models.
The development of radiolabeled synthetic amino acids for PET takes advantage of mechanisms governing protein metabolism, which are elevated in malignant tissues (1,2). In 1978, Washburn et al. reported on the development of aminocyclobutane carboxylic acid (3), a synthesized L-leucine analog for imaging, labeled with 14C (4). This radiotracer demonstrated 6:1 tumor:tissue uptake, little renal excretion, and high pancreatic uptake. Subsequently, a radiotracer for human imaging, 1-aminocyclobutane-1-11C-carboxylic acid (11C-ACBC), was developed at the Oak Ridge National Laboratory by Washburn et al. (5). More recently, an automated radiosynthesis for 11C-ACBC developed at the University of Tennessee at Knoxville for a small medical cyclotron was reported by Goodman et al. (6).
In 1999, we reported the synthesis of an ACBC analog in which a fluorine atom replaces a hydrogen atom (7). A triflate precursor is then radiolabeled with 18F-fluorine, yielding anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (anti-18F-FACBC). This radiotracer seems to demonstrate similar imaging characteristics to 11C-ACBC, yet with the advantage of the 110-min half-life of 18F-fluorine. This longer half-life allows sufficient time for incorporation of 18F-fluorine into the radiopharmaceutical during manufacture and quality control and permits multidosing from a single-batch production, more practical imaging protocols, and regional shipment to satellite facilities with PET or coincidence cameras. Because of its low brain background uptake, anti-18F-FACBC has been reported to have utility in the evaluation of primary and metastatic neoplasia to the brain (8). More recently, we reported elevated uptake of anti-18F-FACBC in patients with prostate carcinoma (9).
This study estimated the whole-body radiation burden of the synthetic amino acid analog anti-18F-FACBC in humans. Radiation dosimetry calculations were performed according to the recommendation of the MIRD committee.
MATERIALS AND METHODS
Synthesis of 18F-FACBC
The preparation of 18F-FACBC has been previously reported (10) and involves a fully automated synthesis developed for the computer-programmable chemistry process control unit (Siemens). Briefly, no-carrier-added 18F-fluoride and Kryptofix 222 (Merck)/K2CO3 were heated with the triflate precursor, syn 1-tert-butylcarbamate-3-trifluoromethanesulfonoxy-cyclobutane-1-carboxylic methyl ester, to afford the 18F-intermediate anti-1-tert-butylcarbamate-3-18F-fluoro-cyclobutane-1-carboxylic methyl ester. After hydrolytic conversion of the 18F-intermediate to anti-18F-FACBC, the acidic solution was automatically passed serially through an ion retardation resin followed by 1 alumina N SepPak cartridge (Waters) and 1 HLB Oasis reverse-phase cartridge (Waters) and finally through a sterilization filter to afford the final product with a pH of 5–7. The decay-corrected radiochemical yield of the desired product was 24%, and its radiochemical purity was 99% at 80 min from the end of bombardment.
Subjects
Six healthy volunteers, 3 male (mean age [±SD], 41 ± 19 y; mean weight, 97 ± 16 kg) and 3 female (mean age, 54 ± 7 y; mean weight, 105 ± 24 kg), were recruited and asked to provide written informed consent. Subjects were restricted to having no prior cancer history and underwent a routine physical examination and blood work before the study and 1 wk after injection. The protocol was approved by the Institutional Review Board of Emory University and performed under the supervision of a research nurse and a radiologist.
PET and Reconstruction
Scans were performed on a Discovery LS (GE Healthcare) operating in 2-dimensional mode and using CT for attenuation correction (11). Serial whole-body scans were acquired for 120 min after a bolus injection of anti-18F-FACBC (366 ± 51 MBq, 136.9–192.4 GBq/mmol). Volunteers were scanned in the supine position starting either from the top of the head or from the mid thigh to image any early elevated uptake in the brain or lower abdominal regions, respectively. The whole-body scans were initially acquired for 1 min per bed position to capture blood clearance and then were gradually increased to 4 min to maintain reasonable counting statistics over decay. Six whole-body PET examinations, of approximately 6–7 bed positions (typical timing sequence of 1, 2, 3, 3, 4, and 4 min per bed position per whole-body scan), yielded 6 individual time frames for each bed position.
Scans were corrected for randoms and scatter using the models implemented by the software supplied by the manufacturer of the scanner, and scans were corrected for attenuation as estimated by the CT image. Data were reconstructed using the manufacturer-provided ordered-subset expectation maximization algorithm with no applied decay correction. A postimaging gaussian filter of 5.45 mm in full width at half maximum and a loop filter of 3.91 mm in full width at half maximum were applied. Images were analyzed with software (developed by the authors) running on a Pentium 4 (Intel Corp.) computer (operating system, Microsoft; computer hardware, IBM) in the IDL (ITT Visual Information Solutions) environment. Regions of interest were drawn on fused PET and CT images within the boundaries of organs showing moderate to high uptake of anti-18F-FACBC. The heart muscle was outlined along the left ventricle wall, which showed moderate to low uptake in the early frames, and the heart contents were defined by a region drawn in the left ventricle cavity. Anti-18F-FACBC uptake in bone marrow is moderate and regions were identified in the iliac and vertebral marrow. For those organs with low uptake such as the gallbladder and stomach, region boundaries were defined on the registered CT images acquired before the emission examination. Similarly, the large expanse and low uptake of the skeletal bone and intestinal structures complicated region drawing and were therefore lumped in the whole-body contribution. The activity distribution in individual organs was assumed to be homogeneous, with special care given to the bladder. Bladder regions of interest were carefully drawn to encompass the entire cavity regardless of any observed excretion. The thymus, thyroid, testes, and ovaries were not evaluated in this study because of the low uptake and difficulty in delineating soft-tissue boundaries in these organ regions. Each region of interest was applied to the appropriate bed position in the serial whole-body series, verified visually for proper placement, and returned in units of Bq/cm3 of tissue.
Dosimetry
Individual organ residence times were calculated by trapezoidal integration of the time–activity curves, assuming only physical decay beyond the last data point. These values were then adjusted on the basis of the standard reference man (12), divided by the injected activity, and averaged across both sexes. MIRDOSE provided estimates of radiation dose based on the calculated residence times (13). The dynamic bladder model updated by the MIRD committee was used to estimate the most favorable time for the initial bladder void to minimize the dose to the urinary bladder wall. This estimate was based on several initial bladder volumes and a conservative urinary secretion rate of 0.25 and 0.5 mL/min during the day and night, respectively (14).
RESULTS
Two of the female volunteers had a history of hysterectomy, and very low uptake was observed in the uterus of the third female volunteer; therefore, a residence time for the uterus was not included in the dosimetry calculations. All volunteers showed initially high uptake in the pancreas and liver, followed by a rapid biologic clearance (Fig. 1). Skeletal muscle and bone marrow showed prolonged uptake, with clearance dominated by the tracer half-life. The persistent uptake in muscle and its large skeletal mass resulted in the highest residence organ time (Table 1). The remainder of activity not accounted for in organ regions was assumed to be distributed evenly throughout the body. No focal or elevated uptake was observed in the intestinal track, on the cortical or trabecular bone surfaces or in the smaller regions of the thymus, thyroid, testes, and ovaries. The critical organs were found to be the liver, followed by the pancreas (Table 2).

Time–activity curve of anti-18F-FACBC in liver, pancreas, muscle, brain, and bladder. Monoexponential fit applied to bladder clearance was used to extract biological compartment half-times for the dynamic bladder model (14).
Individual Organ Residence Times for Anti-18F-FACBC
Mean Radiation-Absorbed Dose Estimates for Anti-18F-FACBC Obtained from MIRDOSE Adult Model
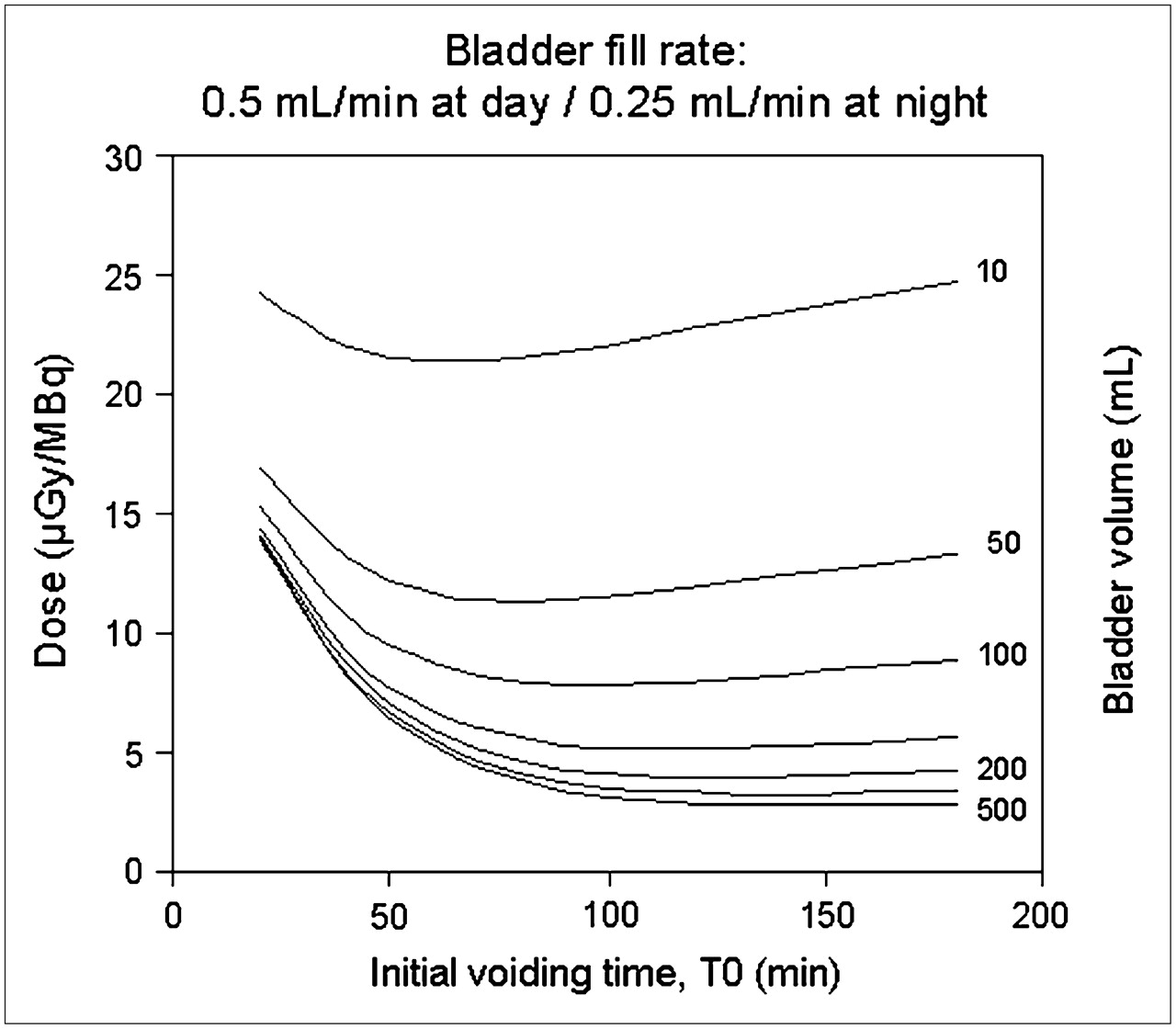
The bladder biologic half-times were estimated by fitting the time–activity curves with a monoexponential function and separating the biologic and physical decay constants. One patient's study was delayed 45 min between acquisition of the first and second whole-body scans, allowing for a reasonable estimate of a delayed bladder biologic compartment half-time. Thus, 2 compartments were applied in the dynamic bladder model, consisting of 28- and 378-min half-times. Dose contribution to the urinary bladder wall from the bladder contents using the updated dynamic bladder model was found to be approximately one fifth of the critical organ value, with an optimum excretion time of 60–120 min after radiopharmaceutical injection (Fig. 2). Both the urinary bladder wall dose calculated from MIRD and the updated dynamic bladder model gave comparable results.
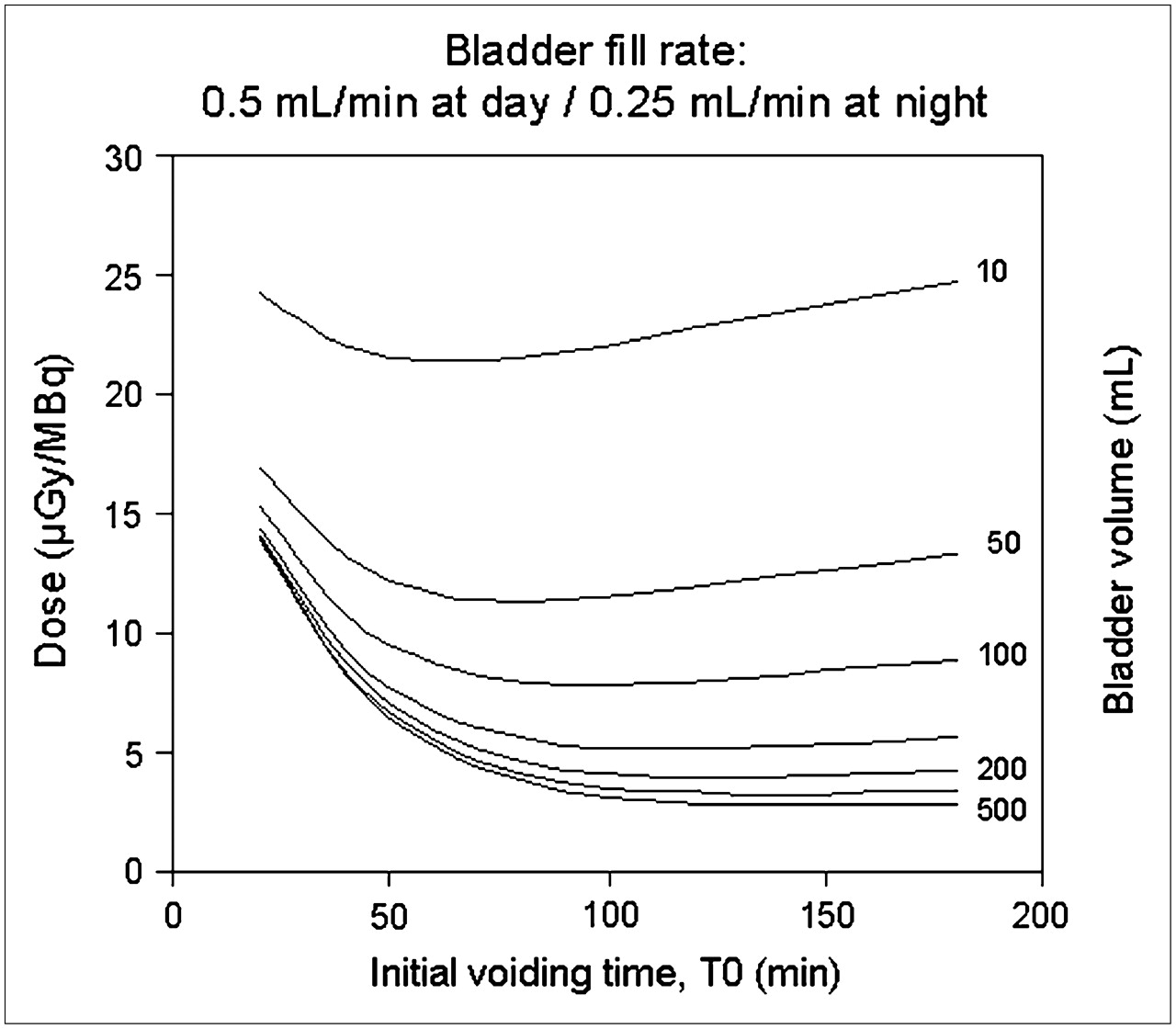
Results of the bladder dynamic model (14). Abscissa represents initial voiding interval from time of injection (T0). Set voiding interval of 3 h follows initial voiding interval.
DISCUSSION
The dosimetry estimates compared favorably with previous anti-18F-FACBC dosimetry estimates (15) and other amino acid–type radiotracers. For example, Pauleit et al. estimated the total-body effective dose for O-(2-18F-fluoroethyl)-l-tyrosine at 16.5 μSv/MBq (16), which is similar to the effective dose of 14.1 μSv/MBq calculated for anti-18F-FACBC. The highest organ dose for O-(2-18F-fluoroethyl)-l-tyrosine, 60 μGy/MBq, was in the urinary bladder wall. This dose was approximately 3 times higher than that for anti-18F-FACBC in the urinary bladder wall, considering a conservative dynamic bladder model estimate (23 μGy/MBq at a 1-h initial void time, Fig. 2A). As with any radiotracer excreted in the urine, we would recommend frequent intake of fluids and frequent voiding.
The nonmetabolized nature of anti-18F-FACBC is favorable when normal and malignant tissue kinetics are followed. Anti-18F-FACBC may prove especially useful in body regions in which background uptake of that tracer is lower than background uptake of 18F-FDG, such as the brain and genitourinary systems, but more studies are required.
CONCLUSION
Dosimetry estimates of the synthetic amino acid radiotracer anti-18F-FACBC fall within the acceptable limits published by the Radioactive Drug Research Committee (10 Code of Federal Regulations 21, part 361). A 370-MBq injection of anti-18F-FACBC results in an effective dose of 5.2 mSv and an estimated absorbed dose of 19.3 mGy to the critical organ, the liver. In summary, anti-18F-FACBC may prove useful for imaging brain and pelvic tumors because of its low native uptake within the brain and the urinary bladder.
Acknowledgments
This work was supported by a grant from Nihon Medi-Physics Co., Ltd.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 24, 2007.
- Accepted for publication March 16, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Differences in Failure-Free Survival After Salvage Radiotherapy Guided by Conventional Imaging Versus 18F-Fluciclovine PET/CT in Postprostatectomy Patients: A Post Hoc Substratification Analysis of the EMPIRE-1 Trial
- First-in-Human PET Imaging and Estimated Radiation Dosimetry of L-[5-11C]-Glutamine in Patients with Metastatic Colorectal Cancer
- Characterizing and Mitigating Bladder Radioactivity on 18F-Fluciclovine PET/CT
- Evaluation of Prostate Cancer with Radiolabeled Amino Acid Analogs
- Anti-3-18F-FACBC (18F-Fluciclovine) PET/CT of Breast Cancer: An Exploratory Study
- Anti-1-Amino-3-18F-Fluorocyclobutane-1-Carboxylic Acid: Physiologic Uptake Patterns, Incidental Findings, and Variants That May Simulate Disease
- 18F-ML-10, a PET Tracer for Apoptosis: First Human Study
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Assessment of Human Biodistribution and Dosimetry of 4-Fluoro-11{beta}-Methoxy-16{alpha}-18F-Fluoroestradiol Using Serial Whole-Body PET/CT
- Fluorine-18-{alpha}-Methyltyrosine Positron Emission Tomography for Diagnosis and Staging of Lung Cancer: A Clinicopathologic Study