


Abstract
Although acquisition of 99mTc-sestamibi myocardial perfusion SPECT (MPS) with the patient in the prone position is commonly used to minimize attenuation artifacts, the impact of combined prone and supine imaging on the prognostic evaluation of coronary artery disease (CAD) has not been determined. The prognostic implications of MPS obtained in both prone and supine positions in patients with perfusion defects on supine MPS were evaluated. Methods: We studied 3,834 patients who were monitored for 24.2 ± 6.0 mo after rest 201Tl/stress 99mTc-sestamibi MPS acquired during 1994–1995, when prone acquisition was performed only in patients with inferior wall perfusion defects that might represent attenuation or motion artifact. Results: During follow-up, there were 132 hard events (cardiac death or myocardial infarction) and 375 total events (hard events or late myocardial revascularization). Overall, patients who underwent prone and supine acquisitions had similar characteristics to those who underwent supine-only imaging, with the exception of being more commonly male. In multivariable analysis, there were similar independent predictors for hard events and total events; the type of acquisition (prone and supine or supine-only) was not a significant predictor of either of these outcome events. After risk adjustment, the predicted event rates were nearly identical for patients undergoing prone and supine compared with supine-only studies. Both observed and predicted hard event rates of patients with normal prone and supine versus supine-only imaging were very low (observed, 0.7%/y and 0.5%/y, respectively; predicted, 1.5% over 24 mo for both). There was no reduction in the higher rates of events associated with abnormal scan results with the combination of prone and supine imaging. Conclusion: Patients with inferior wall defects on supine MPS that are not present on prone MPS have a low risk of subsequent cardiac events, similar to that of patients with normal supine-only studies.
Myocardial perfusion imaging has traditionally been performed with the patient in the supine position. Supine images, however, are often associated with diaphragmatic attenuation of the inferior wall, thus subject to false-positive inferior wall defects that reduce test specificity (1,2). In 1989, Esquerre et al. (3) demonstrated that, for 201Tl myocardial perfusion SPECT (MPS), imaging patients in the prone position markedly improved the specificity in evaluating inferior wall abnormalities by minimizing diaphragmatic attenuation (Fig. 1). A subsequent study from our group described overall sensitivity and specificity of 80% and 93% of prone MPS for the diagnosis of coronary artery disease (CAD) (4). After finding that prone MPS might cause false-positive anteroseptal defects (4), we decided to perform routine supine SPECT, with an additional prone SPECT acquisition in patients with inferior wall perfusion defects whose MPS studies would have been interpreted as abnormal by supine MPS alone, but in whom the defects in might represent attenuation or other artifact (5).

Postexercise 99mTc-sestamibi MPS images of 83-y-old asymptomatic man. Perfusion defect is noted in inferior and inferoapical walls in poststress supine images. Poststress prone images are normal, demonstrating that apparent perfusion defect is secondary to soft-tissue attenuation. Normal wall motion was noted on gated SPECT.
The incremental prognostic value of MPS using supine images for predicting cardiac outcomes has been demonstrated (6,7), and a normal MPS study has been shown to be associated with a low risk of events. However, the prognostic value of normal MPS with the addition of prone images to scan interpretation has not yet been assessed. Although prone imaging may decrease artifacts, the elimination or reduction of perfusion defects may also mask defects truly representing CAD, thus adversely affecting patient prognosis. The purpose of this study was to determine (a) whether patients with perfusion defects in the supine images who subsequently undergo prone MPS that is interpreted as normal have the same low event rate as patients with normal supine-only scans and (b) whether the results associated with increasing scan abnormality are similar in patients undergoing prone and supine or supine-only imaging.
MATERIALS AND METHODS
Study Population
We identified 4,466 consecutive patients who underwent dual-isotope MPS with either exercise or adenosine stress between January 1, 1994, and December 31, 1995. During this time, our standard protocol was to perform a prone MPS acquisition only in patients in whom an inferior wall perfusion defect observed in the supine study was considered to be possibly artifactual and would have resulted in an overall interpretation as equivocal or abnormal.
Patients with known valvular heart disease or cardiomyopathy (n = 64), as well as those who had myocardial revascularization within 60 d of the index MPS (8) (n = 395), were excluded. Of the initial population, 173 patients (4.5%) were lost to follow-up. The study therefore consisted of 3,834 patients, of whom 3,179 (83.0%) underwent supine imaging only and 655 (17.0%) underwent both supine and prone imaging.
Rest 201Tl Imaging
All patients underwent rest 201Tl/stress 99mTc-sestamibi MPS as previously described (9). For rest imaging, weight-adjusted 201Tl (111–167 MBq [3.0–4.5 mCi]) was injected intravenously and acquisition was performed 10 min after injection.
Exercise Myocardial Perfusion Protocol
Patients performed a symptom-limited treadmill exercise test using a standard Bruce protocol. Leads aVF, V1, and V5 were continuously monitored and a 12-lead electrocardiogram (ECG) was recorded at each minute of exercise. At peak exercise, a weight-adjusted dose of 99mTc-sestamibi (925–1,480 MBq [25–40 mCi]) was injected, and exercise was continued for 1 min after injection. MPS acquisition was initiated 30 min after isotope injection. Whenever possible, β-blockers and calcium channel blockers were discontinued 48 h before testing, and nitrates were discontinued at least 6 h before testing.
Adenosine Myocardial Perfusion Protocol
Patients were instructed not to consume caffeine-containing products for 24 h before the test. Adenosine was infused intravenously at a rate of 140 μg/kg/min for 6 min. At the end of the third minute of infusion, weight-adjusted 99mTc-sestamibi was injected. Image acquisition was initiated approximately 60 min after isotope injection.
During both types of stress, blood pressure was measured and recorded at rest, at the end of each stress stage, and at peak stress. Maximal degree of ST segment change at 80 ms after the J point of the ECG was measured and assessed as horizontal, upsloping, or downsloping. ECG responses were considered positive when ≥1 mm of horizontal or downsloping or ≥1.5 mm of upsloping ST segment depression developed at 80 ms after the J point in patients with normal baseline ECG, negative when these changes were absent, and nondiagnostic when baseline changes in the ECG precluded interpretation during exercise.
MPS Acquisition Protocol
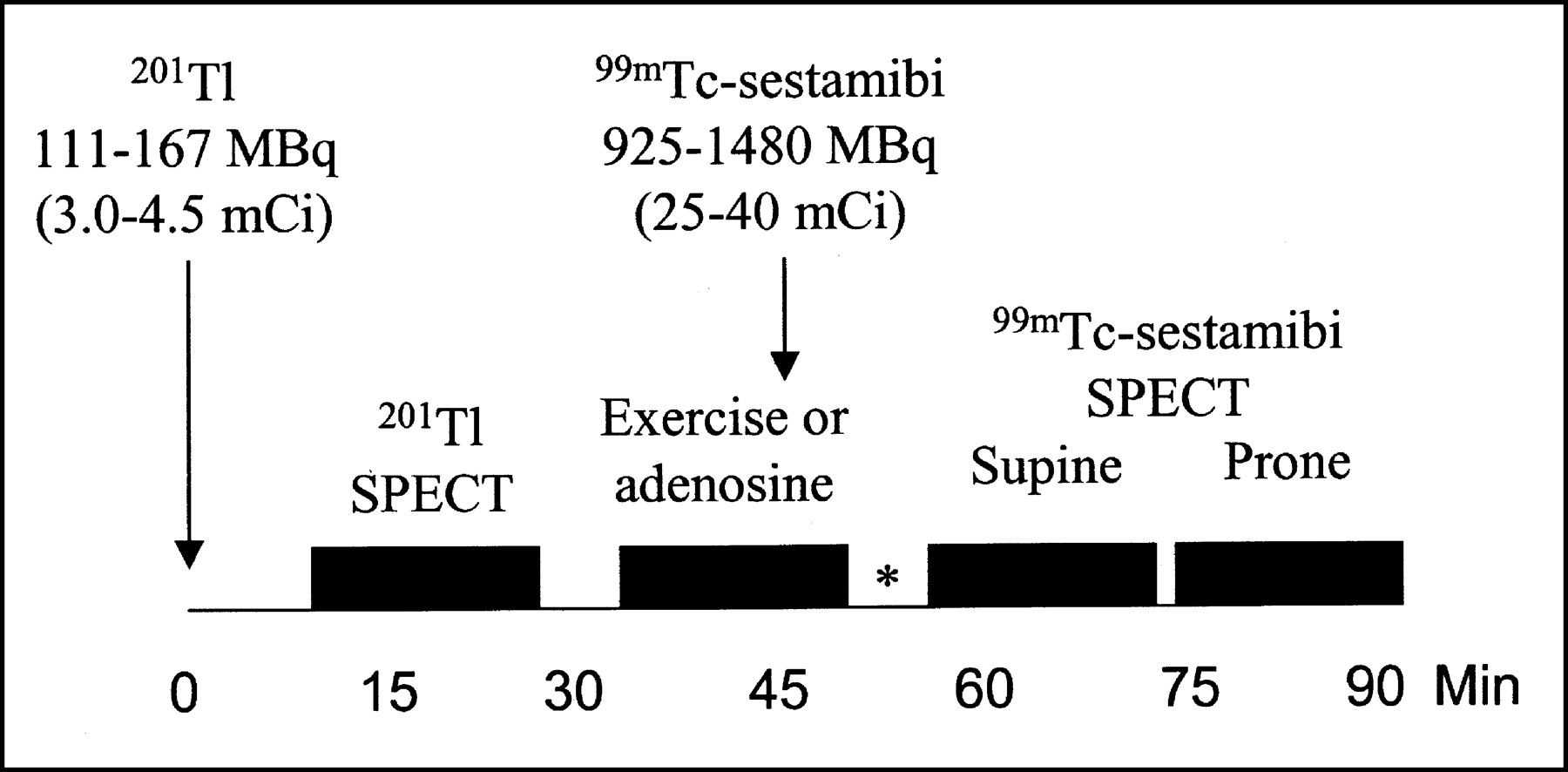
MPS acquisitions (Fig. 2) were performed with a large-field-of-view gamma camera and a high-resolution collimator, obtaining projections over a semicircular 180° arc. For 201Tl imaging, 2 energy windows were used: a 30% window centered on 70 keV and a 20% window centered on the 167-keV peak. For 99mTc-sestamibi, a 15% window centered on the 140-keV peak was used. Acquisition protocols for poststress supine imaging used 32 projections, with 25 s per projection for a dual-head camera, and 64 projections, with 20 s per projection for a single-head camera. For poststress prone acquisition, 15 s per projection were used, with 32 or 64 projections for dual- or single-head, respectively. For rest 201Tl, 32 projections and 35 s per projection were used for the dual-head and 64 projections with 25 s per projection for single-head.
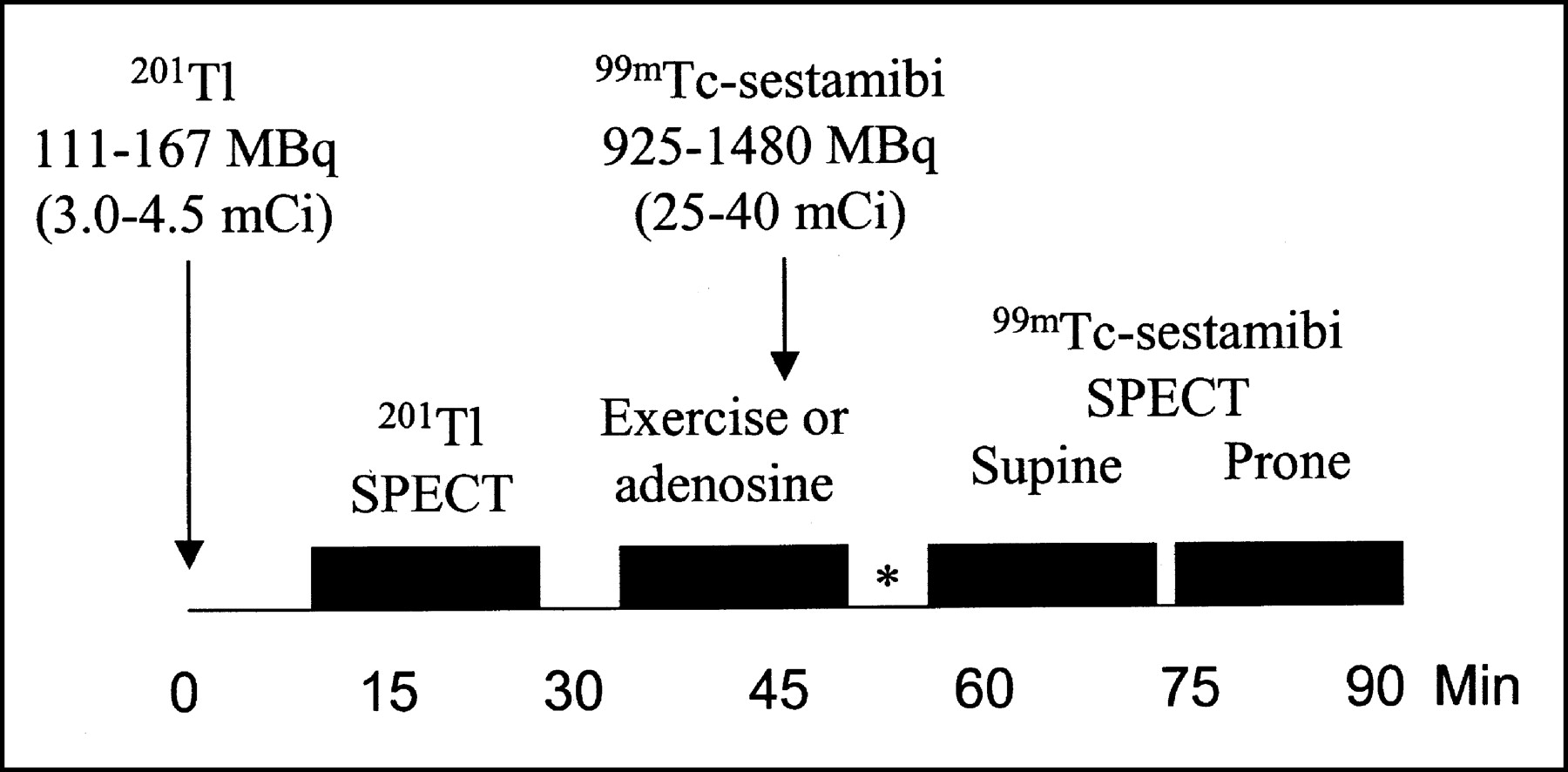
Injection and acquisition protocol for prone and supine MPS study. *15 min for exercise, 1 h for no walk adenosine (adapted and reprinted with permission of (24)).
Image Interpretation
Semiquantitative visual interpretation was performed with short-axis and vertical long-axis myocardial tomograms and a 20-segment model, as previously described (10). These segments were assigned on 6 evenly spaced regions in the apical, midventricular, and basal slices of the short-axis views and 2 apical segments on the midventricular long-axis slice. Each segment was scored by consensus of 2 experienced observers using a 5-point scoring system (0 = normal, 1 = equivocal, 2 = moderate reduction of isotope uptake, 3 = severe reduction of uptake, and 4 = absence of detectable tracer uptake in a segment). When a segment demonstrated a lower score on either supine or prone imaging than in the other position, the lower score was assigned to that segment. On the basis of the number and severity of segments with scores >2, the observers judged the study results as normal, probably normal, equivocal, probably abnormal, or definitely abnormal (10).
To further define the study results as normal or abnormal, the summed stress score (SSS) was considered, from addition of the scores of the 20 segments of the stress 99mTc-sestamibi images (10). SSSs of <4 were considered normal, between 4 to 8 mildly abnormal, and >8 moderately to severely abnormal. For purposes of this study, the SSS had to be <4 and the final interpretation had to be normal or probably normal for the study to be considered normal. Similarly, patients with equivocal, probably abnormal, and definitely abnormal final MPS interpretations were grouped as abnormal.
Patient Follow-Up
Patient follow-up was performed by scripted telephone interview by individuals blinded to the patients’ test results. Hard events were defined as either cardiac death, as noted and confirmed by review of death certificate and either hospital chart or physician’s records, or nonfatal myocardial infarction, as evidenced by the appropriate combination of symptoms, ECG, and enzyme changes. Total events were defined as hard events or late revascularization (>60 d after the index MPS study) (8). Patients were monitored for 24.2 ± 6.0 mo (all for at least 1 y).
Likelihood of CAD
The prescan likelihood of CAD was calculated with CADENZA (Advanced Heuristics Inc.), using Bayesian analysis of prescan patient data (11). For the patients who underwent adenosine stress testing, the history and resting ECG information were considered, whereas for those who underwent exercise stress testing, the prescan likelihood of CAD included history and exercise test information.
Statistical Analysis
Continuous variables were expressed as mean value ± SD and compared using a Student t test with correction for multiple comparisons when appropriate. Comparisons of categoric variables were computed by a χ2 statistic. A P value of 0.05 was used to define statistical significance in univariate analysis. A Cox proportional hazards model was used to identify variables independently associated with cardiac events. Multivariable models were developed using hard or total events as the endpoints of interest. In this study, the goal of modeling was to determine all potential confounders of the relationship between MPS results and adverse outcomes. This approach included setting a threshold of P < 0.20 for entry into the model. Hence, the likelihood of finding a significant relationship between prone imaging and increased risk of adverse events would be maximized.
RESULTS
Patient Population
The 3,179 patients who underwent supine-only imaging and 655 patients who underwent supine and prone imaging are characterized in Table 1. Patients who had prone and supine acquisitions were more frequently male than patients who had supine-only MPS. By all other comparators, the groups were not significantly different.
Patient Characteristics
Table 2 demonstrates patient characteristics by MPS acquisition types and normal or abnormal MPS results. Within each acquisition type, differences were as follows: for patients undergoing prone and supine imaging, those with abnormal studies were more frequently male, had a higher prescan likelihood of CAD, and had more frequent abnormal rest ECG than patients with normal scans. For patients studied in the supine position only, those with abnormal studies were significantly older and more frequently male, with a history of myocardial revascularization, were on digitalis, and had a higher prescan likelihood of CAD. Comparing patients with normal scans by the 2 acquisition types, the only significant difference was the higher frequency of males in the prone and supine group. Comparing patients with abnormal scans, not only were the patients undergoing prone and supine more often male than those undergoing supine MPS alone, but also they less frequently had prior revascularization, were on digitalis or had rest ECG abnormality, as well as had a lower SSS.
Patient Characteristics by MPS Acquisition Types and Normal or Abnormal MPS Results
Outcome Events
During follow-up, there were 132 hard events (52 myocardial infarctions and 83 cardiac deaths) and 375 total events. Overall, the annualized hard event rate was 1.8% and the total event rate was 5.2%. Event rates were higher for patients undergoing adenosine stress: 3.2% of hard events per year and 7.4% of total events per year, versus 1.1% and 4.2% of hard and total events per year, for exercise stress (P < 0.001). Patients imaged only in the supine position had, with adenosine or exercise stress, hard event rates of 3.6% and 1.0% and total event rates of 7.8% and 4.0%, respectively (P < 0.001 for comparison between adenosine and exercise stress). Patients who had prone and supine imaging had, with adenosine or exercise stress, hard event rates of 1.6% and 1.1% and total event rates of 5.5% and 5.3%, respectively (P > 0.05).
Table 3 demonstrates annualized event rates according to scan results and type of stress for patients imaged in prone and supine or supine-only positions. Of note, 368 of 655 patients with equivocal or abnormal supine MPS who underwent additional prone imaging had normal final interpretations. In both acquisition types, hard and total event rates increased with worsening scan results, although this did not reach statistical significance in patients who underwent adenosine stress and prone and supine acquisition. Importantly, the annualized hard event rate was as low in patients with normal prone and supine scans as in those with normal supine studies. Furthermore, for each category of SSS, hard and total event rates, with either exercise or adenosine stress, were not significantly different between patients in the prone and supine and supine-only groups.
Annualized Event Rates
Univariate Predictors of Cardiac Events
Descriptive characteristics and nuclear variables of patients with events versus those without events during follow-up are presented in Tables 4 and 5 for hard events and total events, respectively. Patients with hard events demonstrated greater abnormality in all variables assessed with the exception of hypertension (borderline higher in the event group), smoking, family history of early CAD, and angina. Of importance, there was also no difference in the frequency of prone and supine or supine-only acquisitions in the patients with and without hard events. Regarding total events (Table 5), those with events demonstrated a greater abnormality in most variables. The variables that were not significantly different between these groups were hypercholesterolemia, smoking, family history of early CAD, angina, shortness of breath, and abnormal rest ECG. As with hard events, there was also no difference in the frequency of prone and supine or supine-only acquisitions in the patients with and without total events.
Univariate Predictors of Hard Events
Univariate Predictors of Total Events
Multivariable Predictors of Events
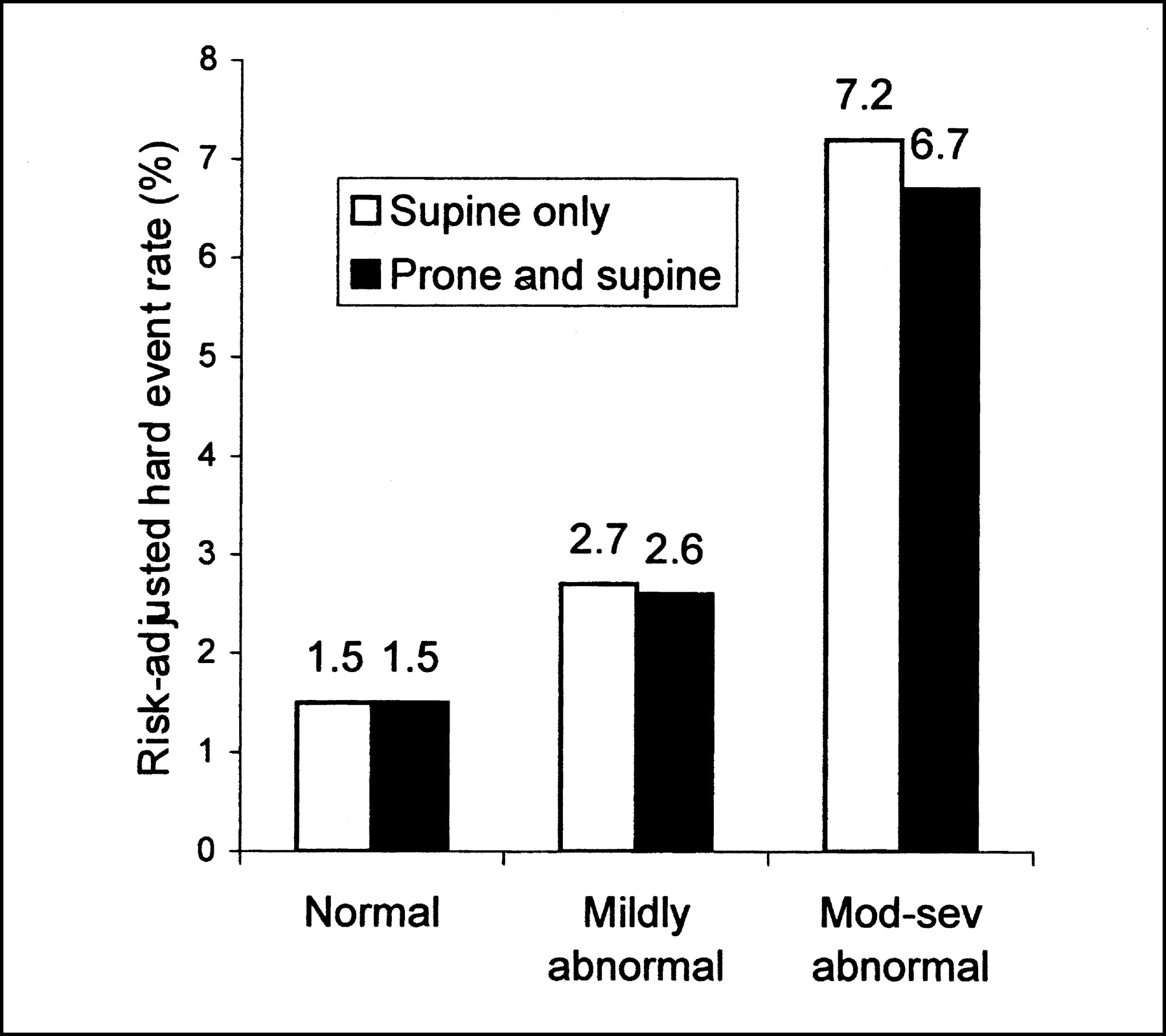
In the overall study population, Cox proportional hazards analysis revealed that age (χ2 = 9.2, P = 0.002), a history of myocardial infarction (χ2 = 4.5, P = 0.03), digitalis use (χ2 = 12.1, P < 0.0001), adenosine stress (χ2 = 10.0, P = 0.002), and the SSS (χ2 = 38.2, P < 0.0001) constituted the model most predictive of hard events. For total events, age (χ2 = 13.4, P = 0.001), digitalis use (χ2 = 15.3, P = 0.0001), adenosine stress (χ2 = 9.2, P = 0.003), and the SSS (χ2 = 84.2, P < 0.0001) constituted the most predictive model. Figures 3 and 4 illustrate that, after risk adjustment using the multivariable model, hard and total event rates were not significantly different between patients who underwent supine-only or prone and supine acquisitions.

Risk-adjusted hard event rates in patients undergoing supine-only or prone and supine acquisition, according to MPS interpretation. P < 0.0001 across scan categories; P > 0.05 for comparisons between supine-only or prone and supine. Mod-sev = moderately to severely abnormal.
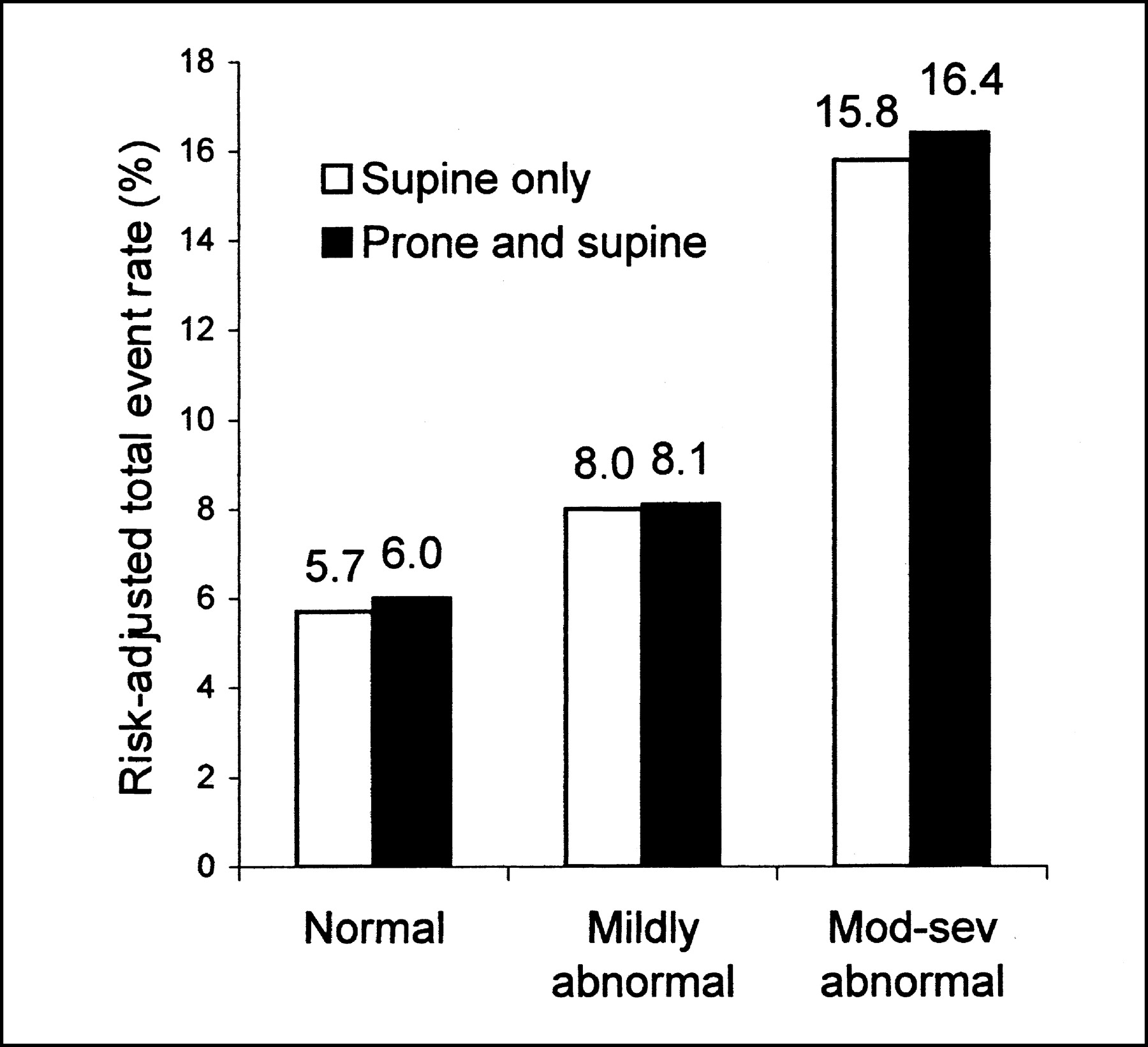
Risk-adjusted total event rates in patients undergoing supine-only or prone and supine acquisition, according to MPS interpretation. P < 0.0001 across scan categories; P > 0.05 for comparisons between supine-only or prone and supine. Mod-sev = moderately to severely abnormal.
DISCUSSION
To our knowledge, this is the first study to address the prognostic value of MPS acquired in the combined prone and supine positions. In this study, patients with supine MPS demonstrating findings that would have rendered the interpretation of the inferior wall as equivocal or abnormal underwent prone imaging, and their findings were compared with those of a larger group of patients from the same time period who underwent supine-only MPS. Overall, patients who underwent prone and supine acquisitions had similar characteristics as those who underwent supine-only imaging, with the exception of being more commonly male. In univariate analysis, the type of acquisition (supine-only or prone and supine) was not a significant predictor of either hard or total events. In addition, in a multivariable analysis, the predictors of hard events and total events were similar; the type of acquisition (prone and supine or supine-only) was not a significant predictor of either of these outcome events. After risk adjustment using the multivariable models for hard events or total events, predicted event rates were almost identical for patients undergoing prone and supine compared with supine-only studies. Importantly, both the observed and predicted hard event rates of patients with normal prone and supine versus supine-only imaging were very low (observed, 0.7%/y and 0.5%/y, respectively; predicted, 1.5% over 24 mo for both). Furthermore, there was no reduction in the higher rates of events associated with abnormal scan results with the combination of prone and supine imaging.
Although MPS has been demonstrated to have high sensitivity and specificity for detection of CAD as well as excellent prognostic value, a common problem with MPS is artifactual reduction in apparent radiotracer uptake in the inferior left ventricular wall attributed to diaphragmatic attenuation, which can result in false-positive interpretations. With either 201Tl or 99mTc-sestamibi studies (1,2), though less frequent in the latter, diaphragmatic attenuation may impair either sensitivity or specificity of MPS for detection of CAD, depending on whether it is overestimated (i.e., a true defect is falsely attributed to attenuation) or underestimated (an attenuation defect is falsely considered a perfusion defect). With the use of gated MPS, the distinction of true from artifactual defect can be more easily made (12); however, a problem remains, because with gated MPS, true myocardial perfusion defects due to subendocardial infarction that are associated with a normal contraction pattern might be falsely attributed to soft-tissue attenuation (13). Nonuniform attenuation correction has also been shown to improve the specificity and normalcy rate of MPS (14–16). This approach, however, requires specialized hardware and software and, in some implementations, may overcorrect the inferior wall, leading to lower sensitivity for detection of a true perfusion defect (17). By comparison, the approach of prone and supine imaging, described in this article, can be performed on virtually any SPECT camera without the need for specialized hardware or software.
The prone position results in an anterior shifting of the heart and a lowering of the diaphragm and the subphrenic organs, so that performing MPS acquisition in this position reduces the interposition of these tissues and organs between the inferior wall and the SPECT camera (3). The use of the prone position for 201Tl imaging has been shown to result in improvement of specificity for the diagnosis of right coronary artery disease and overall improvement in accuracy compared with supine imaging (4,18–20). Higher absolute counts have been reported in the inferior wall with prone imaging with both 201Tl (4,18) and 99mTc-sestamibi (19,20). The use of prone MPS acquisitions alone, however, may be associated with an artifactual anteroseptal or anterior defect (4), presumably caused by attenuation from a rib or the sternum, which is associated with the closer approximation of the heart and these structures in the prone position. In our experience, when we attempted prone MPS only to reduce the frequency of artifactual inferior abnormalities, the associated anterior distribution artifacts, raising the possibility of left anterior descending CAD, were even more problematic, frequently resulting in unnecessary referral to catheterization; thus, we would not recommend prone-only MPS acquisitions.
Because of the inferior and anterior wall artifacts associated with supine and prone MPS, respectively, we introduced the use of combined prone and supine MPS acquisitions in our group in 1994. The patients included in this article were chosen from a period in which we used the combined acquisitions only when there was a perceived abnormality on the supine MPS acquisitions. After finding that approximately 20% of our patients were requiring additional prone studies (655/3179 [17%] in this study), because of the disruption of the imaging schedule by the unpredictable need for the additional prone acquisitions, we initiated routine supine and prone acquisitions on all patients in 1996. It is worth noting that this combined supine and prone approach is probably only applicable to radiotracers that do not rapidly redistribute, such as 99mTc-sestamibi or 99mTc-tetrofosmin. Because of the problem of rapid redistribution of 201Tl associated with mild coronary stenoses (21), sequential supine and prone imaging after stress is less applicable with this agent, since the disappearance in the prone position of a defect observed with supine MPS might be a consequence of redistribution within a true defect.
Several limitations of the supine and prone MPS technique should be mentioned. The combined imaging requires additional camera time that may not be available in many laboratories. Additionally, a small proportion of patients cannot lie in the prone position for the time required for MPS. Effective attenuation-correction methods have been developed that may prove to be more efficient than the combined supine and prone approach (14,22,23). Regarding our study design, because the supine images were interpreted before the prone images, the supine results influenced the combined supine and prone interpretation. However, it was not our intent to demonstrate that prone imaging is superior to supine but, rather, that the combined approach is more effective than supine imaging alone. Furthermore, although prone imaging affected our final interpretation, we do not have information as to how often the addition of prone imaging changed patient management. Whereas the patients in this study had only inferior wall defects in the supine position that were further evaluated with prone imaging, we have noted that other attenuation artifacts (e.g., breast) and motion artifacts seen in supine MPS are also clarified by the addition of prone imaging; this anecdotal experience requires further study.
CONCLUSION
The combined use of prone and supine MPS acquisition was associated with the same event rates by MPS results as those in patients with supine-only studies. Importantly, normal prone MPS in patients with initially equivocal or abnormal supine MPS had the same low event rates as those in patients with normal supine-only studies. Since decisions for catheterization after MPS are frequently based on risk assessment, our findings suggest that the addition of the prone acquisition to supine MPS might lead to more appropriate clinical decisions.
Acknowledgments
This work was supported in part by a grant from Bristol-Myers Squibb Medical Imaging Inc. (Billerica, MA) and by the CAPES (Coordenacao de Auxilio de Pessoal de Nivel Superior), Brazil.
Footnotes
Received Dec. 10, 2002; revision accepted Mar. 28, 2003.
For correspondence or reprints contact: Daniel S. Berman, MD, Department of Imaging, Cedars-Sinai Medical Center, 8700 Beverly Blvd., Room A-041, Los Angeles, CA 90048-1865.
E-mail: Daniel.berman{at}cshs.org
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative Clinical Nuclear Cardiology, Part 1: Established Applications
- Evaluating the Role of Routine Prone Acquisition on Visual Evaluation of SPECT Images
- Are Shades of Gray Prognostically Useful in Reporting Myocardial Perfusion Single-Photon Emission Computed Tomography?
- Stress Thallium-201/Rest Technetium-99m Sequential Dual Isotope High-Speed Myocardial Perfusion Imaging
- Assessment of Severity of Coronary Artery Stenosis in a Canine Model Using the PET Agent 18F-Fluorobenzyl Triphenyl Phosphonium: Comparison with 99mTc-Tetrofosmin
- The Prognostic Value of Normal Exercise Myocardial Perfusion Imaging and Exercise Echocardiography: A Meta-Analysis
- Combined Supine and Prone Quantitative Myocardial Perfusion SPECT: Method Development and Clinical Validation in Patients with No Known Coronary Artery Disease
- Prone Versus Supine Patient Positioning During Gated 99mTc-Sestamibi SPECT: Effect on Left Ventricular Volumes, Ejection Fraction, and Heart Rate
- The year in cardiac imaging
- False-Positive Findings on Myocardial Perfusion SPECT
- Automatic Quantification of Myocardial Perfusion Stress-Rest Change: A New Measure of Ischemia
- Implication of Prognostically Significant Negative Results on Prone SPECT