


Article Figures & Data
Figures
- FIGURE 1.
Postexercise 99mTc-sestamibi MPS images of 83-y-old asymptomatic man. Perfusion defect is noted in inferior and inferoapical walls in poststress supine images. Poststress prone images are normal, demonstrating that apparent perfusion defect is secondary to soft-tissue attenuation. Normal wall motion was noted on gated SPECT.
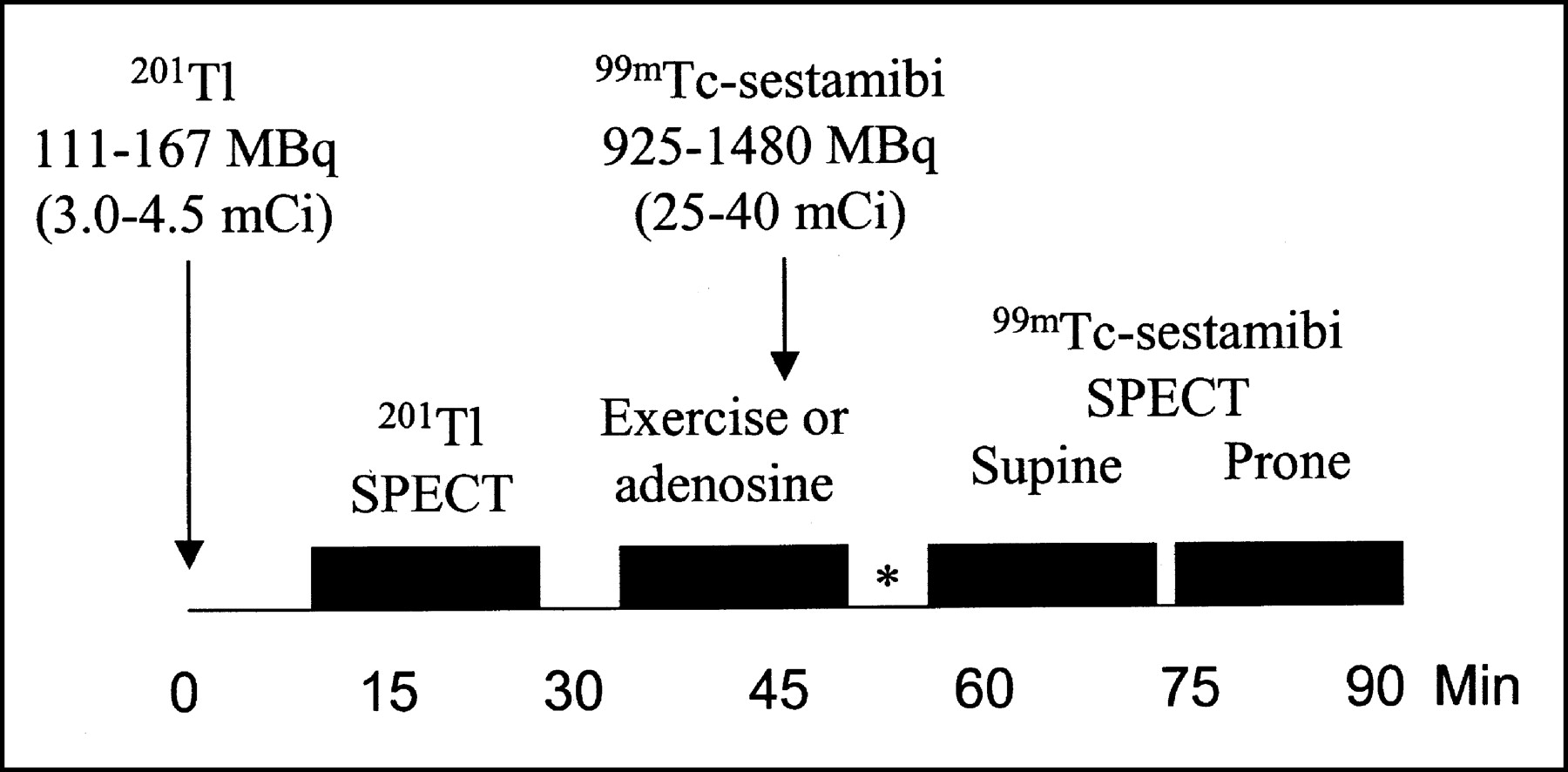
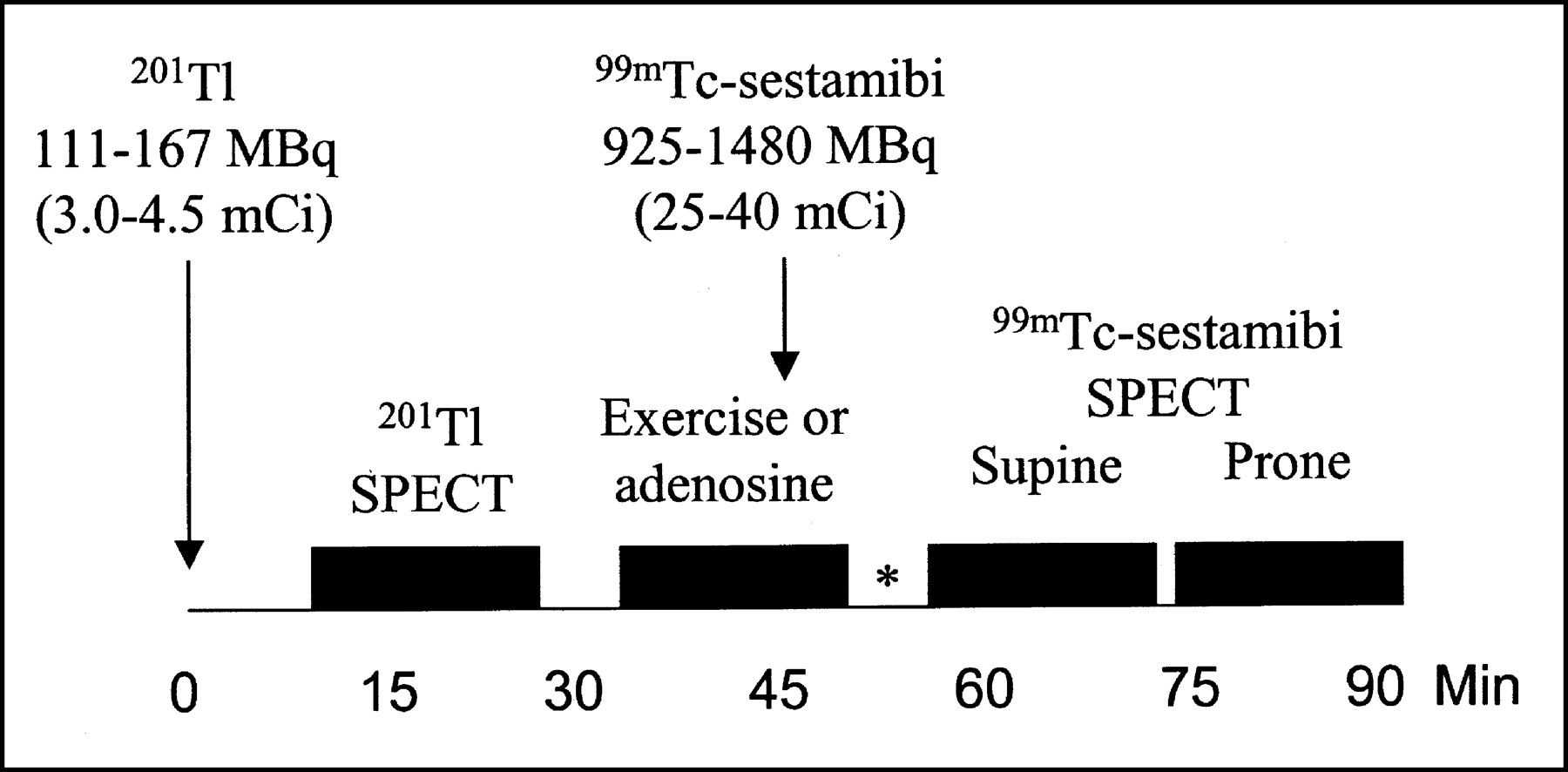
- FIGURE 2.
Injection and acquisition protocol for prone and supine MPS study. *15 min for exercise, 1 h for no walk adenosine (adapted and reprinted with permission of (24)).
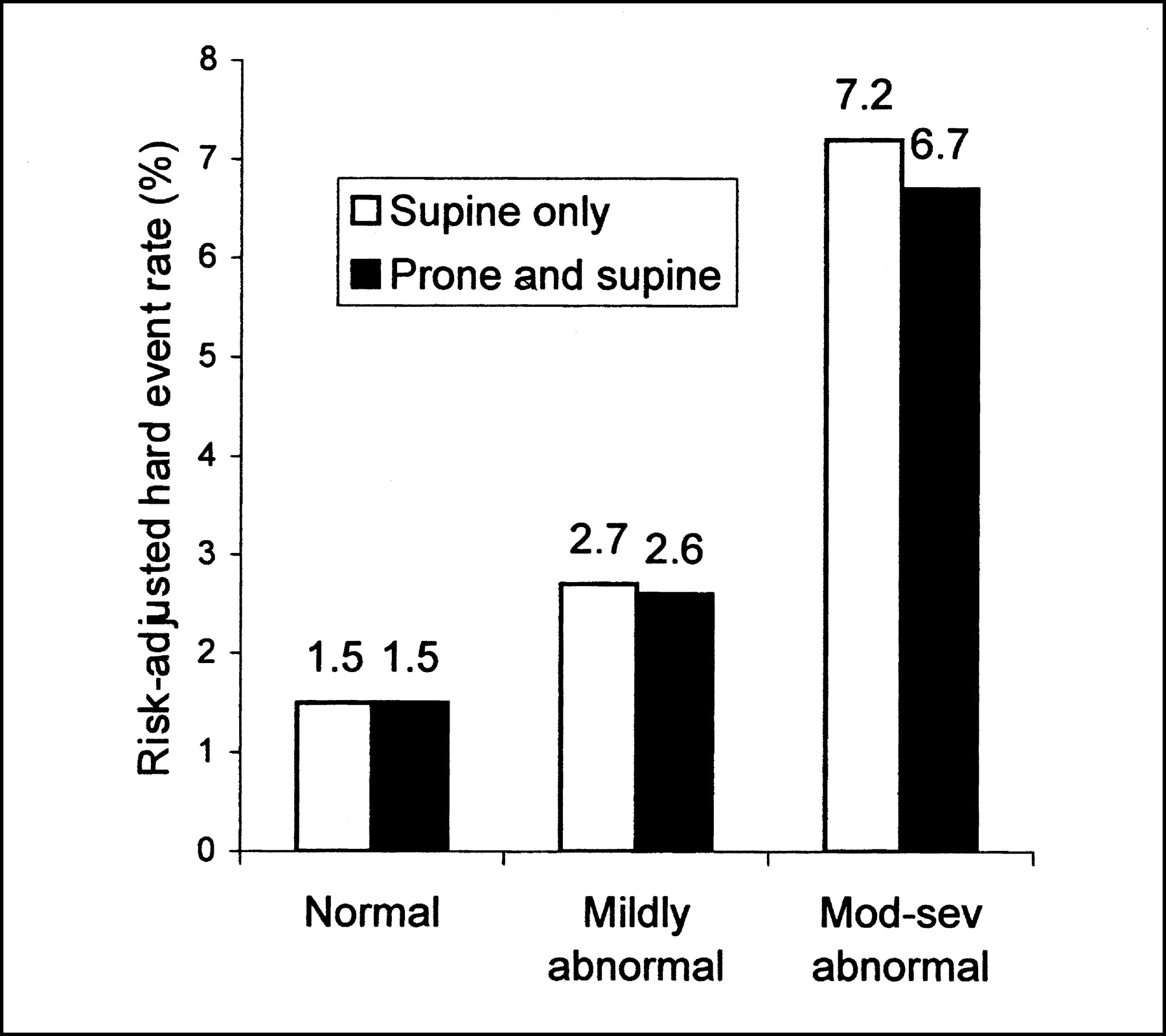
- FIGURE 3.
Risk-adjusted hard event rates in patients undergoing supine-only or prone and supine acquisition, according to MPS interpretation. P < 0.0001 across scan categories; P > 0.05 for comparisons between supine-only or prone and supine. Mod-sev = moderately to severely abnormal.
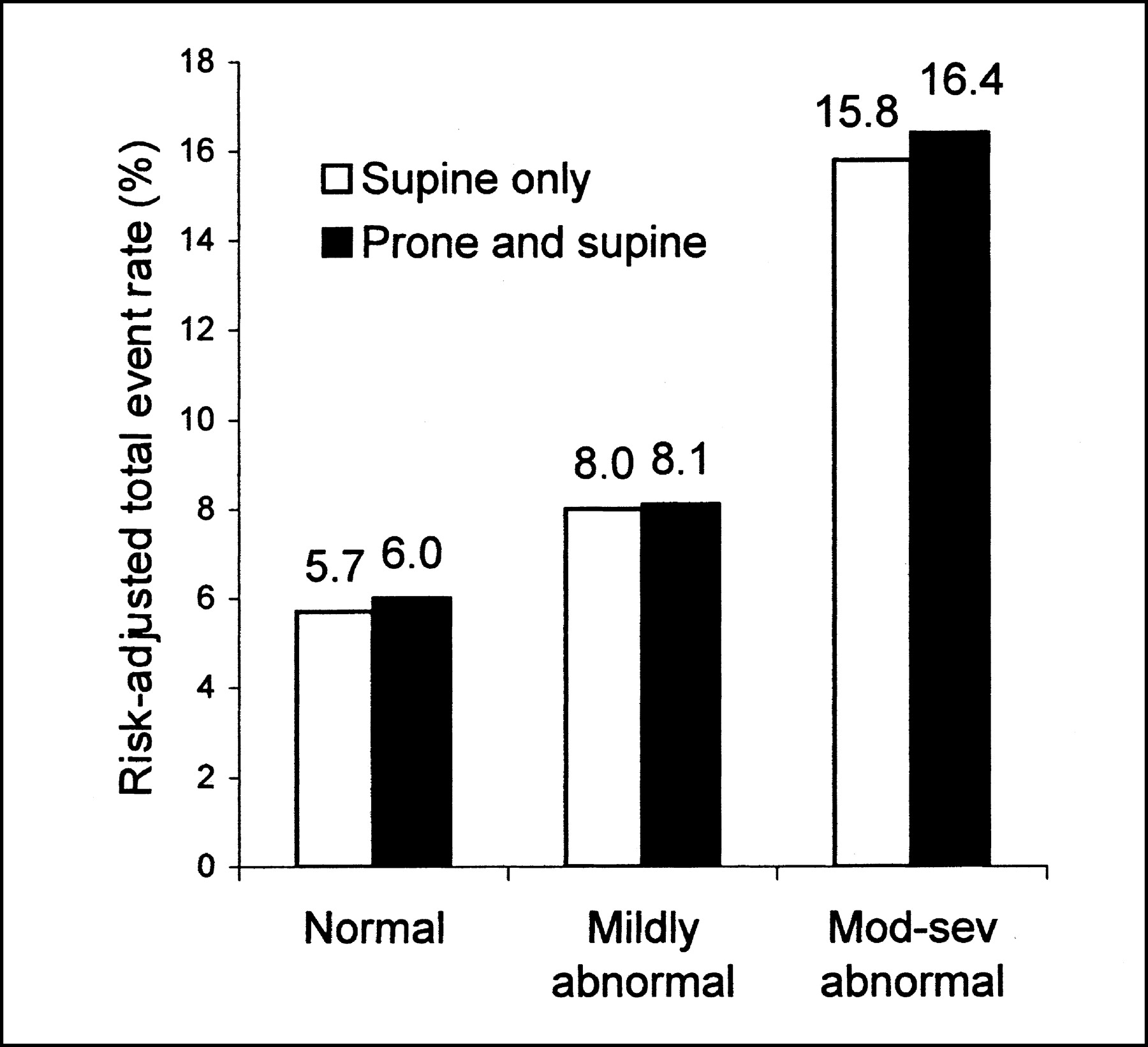
- FIGURE 4.
Risk-adjusted total event rates in patients undergoing supine-only or prone and supine acquisition, according to MPS interpretation. P < 0.0001 across scan categories; P > 0.05 for comparisons between supine-only or prone and supine. Mod-sev = moderately to severely abnormal.


Tables
Characteristic Prone and supine (n = 655) Supine-only (n = 3,179) Age (y) 66.7 ± 11.1 65.7 ± 12.3 Male sex 487 (74.4) 1,899 (59.7)* Hypertension 319 (48.7) 1,499 (47.2) Diabetes 100 (15.3) 467 (14.7) Hypercholesterolemia 328 (50.1) 1,466 (46.1) Smoking 81 (12.4) 381 (12.0) Family history of CAD 169 (25.8) 862 (27.1) History of MI 155 (23.7) 800 (25.2) History of revascularization 216 (33.0) 1,044 (32.8) Digitalis use 44 (6.7) 269 (8.5) Angina 246 (37.6) 1,216 (38.3) Shortness of breath 35 (5.3) 178 (5.6) Adenosine stress 217 (33.1) 1,071 (33.7) Prescan likelihood of CAD 0.39 ± 0.36 0.36 ± 0.34* Abnormal rest ECG 464 (70.8) 2,308 (72.6) SSS 6.3 ± 8.8 6.5 ± 9.3 ↵* P < 0.05.
MI = myocardial infarction.
Values in parentheses are percentage.
- TABLE 2
Patient Characteristics by MPS Acquisition Types and Normal or Abnormal MPS Results
Characteristic Prone and supine (n = 655) Supine-only (n = 3,179) Normal (n = 368) Abnormal (n = 287) Normal (n = 1,880) Abnormal (n = 1,299) Age (y) 64.4 ± 11.3 69.7 ± 10.1 63.0 ± 12.6 69.7 ± 10.6* Male sex 260 (70.7) 227 (79.1)* 958 (51.0)† 941 (72.4)*‡ Hypertension 172 (46.7) 147 (51.2) 799 (42.5) 700 (53.9) Diabetes 38 (10.3) 62 (21.1) 205 (10.9) 262 (20.2) Hypercholesterolemia 183 (49.7) 145 (50.5) 847 (45.1) 619 (47.7) Smoking 44 (12.0) 37 (12.9) 228 (12.1) 153 (11.8) Family history of CAD 92 (25.0) 77 (26.8) 495 (26.3) 367 (28.3) History of MI 23 (6.3) 132 (46.0) 144 (7.7) 656 (50.5) History of revascularization 56 (15.2) 160 (55.7) 165 (8.8) 799 (61.5)*‡ Digitalis use 24 (6.5) 20 (7.0) 108 (5.7) 161 (12.4)*‡ Angina 128 (34.8) 118 (41.1) 756 (40.2) 460 (35.4) Shortness of breath 16 (4.3) 19 (6.6) 82 (4.4) 96 (7.4) Adenosine stress 97 (26.4) 120 (41.8) 490 (26.1) 581 (44.7) Prescan likelihood of CAD 0.34 ± 0.30 0.44 ± 0.34* 0.33 ± 0.29 0.45 ± 0.35* Abnormal rest ECG 228 (62.0) 236 (82.2)* 1,164 (61.9) 1,144 (88.1)*‡ SSS 0.5 ± 0.9 13.8 ± 8.7* 0.5 ± 0.9 15.2 ± 9.1*‡ Rate Prone and supine (n = 655) Supine-only (n = 3,179) Normal Mildly abnormal Moderately to severely abnormal Normal Mildly abnormal Moderately to severely abnormal Total Hard events (%) 0.7 0.5 2.9* 0.5 1.6 4.8* Total events (%) 2.8 7.9 9.3* 1.8 7.7 11.9* n 368 97 190 1,880 382 917 Exercise Hard events (%) 0.6 0.9 2.8* 0.4 0.7 3.2* Total events (%) 2.6 10.0 9.9* 1.5 7.0 10.1* n 271 57 110 1,390 231 487 Adenosine Hard events (%) 1.0 0 3.1 1.1 3.3 6.8* Total events (%) 3.2 5.1 8.5 2.6 8.9 14.2* n 97 40 80 490 151 430 ↵* P < 0.05 across scan categories.
Predictor With hard events (n = 132) Without hard events (n = 3,702) Age (y) 72.1 ± 11.5 65.7 ± 12.0* Male sex 98 (74.2) 2,288 (61.8)* Hypertension 73 (55.3) 1,745 (47.1) Diabetes 31 (23.5) 536 (14.5)* Hypercholesterolemia 46 (34.8) 1,748 (47.2)* Smoking 18 (13.6) 444 (12.0) Family history of CAD 39 (29.5) 992 (26.8) Digitalis use 32 (24.2) 281 (7.6)* History of MI 71 (53.8) 884 (23.9)* History of revascularization 70 (53.0) 1,190 (32.1)* Angina 50 (37.9) 1,412 (38.1) Shortness of breath 19 (14.4) 194 (5.2)* Adenosine stress 78 (59.1) 1,210 (32.7)* Prescan likelihood of CAD 0.46 ± 0.34 0.37 ± 0.31 Position Prone 17 (12.9) 638 (17.2) Supine 115 (87.1) 3,064 (82.8) Abnormal rest ECG 16 (12.1) 111 (3.0)* SSS 16.5 ± 11.4 6.1 ± 8.9* ↵* P < 0.05.
MI = myocardial infarction.
Values in parentheses are percentage.
Predictor With total events (n = 375) Without total events (n = 3,459) Age (y) 69.5 ± 10.4 65.5 ± 12.2* Male sex 277 (73.9) 2,109 (61.0)* Hypertension 197 (52.5) 1,621 (46.9)* Diabetes 85 (22.7) 482 (13.9)* Hypercholesterolemia 177 (47.2) 1,617 (46.7) Smoking 46 (12.3) 416 (12.0) Family history of CAD 106 (28.3) 925 (26.7) Digitalis use 52 (13.9) 261 (7.5)* History of MI 170 (45.3) 785 (22.7)* History of revascularization 222 (59.2) 1,038 (30.0)* Angina 142 (37.9) 1,320 (38.2) Shortness of breath 27 (7.2) 186 (5.4) Adenosine stress 170 (45.3) 1,118 (32.3)* Prescan likelihood of CAD 0.50 ± 0.34 0.37 ± 0.31* Position Prone 67 (17.9) 588 (17.0) Supine 308 (82.1) 2,871 (83.0) Abnormal rest ECG 53 (14.1) 263 (7.6) SSS 13.2 ± 10.6 5.7 ± 8.7* ↵* P < 0.05.
MI = myocardial infarction.
Values in parentheses are percentage.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative Clinical Nuclear Cardiology, Part 1: Established Applications
- Evaluating the Role of Routine Prone Acquisition on Visual Evaluation of SPECT Images
- Are Shades of Gray Prognostically Useful in Reporting Myocardial Perfusion Single-Photon Emission Computed Tomography?
- Stress Thallium-201/Rest Technetium-99m Sequential Dual Isotope High-Speed Myocardial Perfusion Imaging
- Assessment of Severity of Coronary Artery Stenosis in a Canine Model Using the PET Agent 18F-Fluorobenzyl Triphenyl Phosphonium: Comparison with 99mTc-Tetrofosmin
- The Prognostic Value of Normal Exercise Myocardial Perfusion Imaging and Exercise Echocardiography: A Meta-Analysis
- Combined Supine and Prone Quantitative Myocardial Perfusion SPECT: Method Development and Clinical Validation in Patients with No Known Coronary Artery Disease
- Prone Versus Supine Patient Positioning During Gated 99mTc-Sestamibi SPECT: Effect on Left Ventricular Volumes, Ejection Fraction, and Heart Rate
- The year in cardiac imaging
- False-Positive Findings on Myocardial Perfusion SPECT
- Automatic Quantification of Myocardial Perfusion Stress-Rest Change: A New Measure of Ischemia
- Implication of Prognostically Significant Negative Results on Prone SPECT