


Abstract
A promising application of radiolabeled somatostatin analogs is peptide receptor–targeted radionuclide therapy of somatostatin receptor–expressing tumors. A suitable radionuclide is 90Y, which emits high-energy β-particles with a pathlength of several millimeters in tissue, making it especially promising for treatment of large tumors. Methods: We investigated the radiotherapeutic effect of different activities (111 and 370 MBq) of [90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA)0,Tyr3]octreotide in Lewis rats bearing somatostatin receptor–positive rat pancreatic CA20948 tumors of different size (0.08–15 cm2) in their flank. Results: Dose-dependent radiotherapeutic effects of 90Y-labeled octreotide in this rat tumor model were found. Tumor control (100% complete response) was found in animals bearing tumors of 3–9 cm2 (mean, 7.8 cm2) after intravenous injection of the highest activity (370 MBq [90Y-DOTA0,Tyr3]octreotide). In rats bearing tumors of ≤1 cm2 or ≥14 cm2, the effects were less pronounced (50% and 0% complete response, respectively). In tumors of ≤1 cm2 the 90Y radiation energy will not be absorbed completely in the tumor, whereas in tumors of ≥14 cm2 the increased number of clonogenic and probably hypoxic tumor cells may explain the failure to reach a cure. Conclusion: This study shows the ability of [90Y-DOTA0,Tyr3]octreotide to control tumor growth, especially in medium-sized tumors. The effect of radionuclide therapy appeared to be dependent on tumor size at the onset of therapy.
Cells express on their cellular membranes a variety of receptor proteins with high affinity for regulatory peptides, including somatostatin. Somatostatin receptors are integral membrane glycoproteins, ubiquitously distributed throughout the body. Five different human somatostatin receptor types have been cloned. All subtypes bind somatostatin with high affinity, whereas the more stable analog octreotide (Fig. 1) binds with high affinity to the somatostatin receptor subtype 2 (SST2) and with decreasing affinity to subtypes SST5 and SST3. It shows no binding to subtypes SST1 and SST4 (1–4).

Structures of octreotide, [Tyr3]octreotide, and DOTA.
Alterations of somatostatin receptor expression during disease, like overexpression in many neoplasia, can be exploited by imaging techniques. Peptide receptor scintigraphy with the small radioactive somatostatin analog [111In-diethylenetriaminepentaacetic acid (DTPA)0]octreotide appears to be a sensitive and specific technique to detect in vivo somatostatin receptor–expressing tumors (5,6).
A new and fascinating application is the use of radiolabeled somatostatin analogs for peptide receptor–targeted radionuclide therapy. Because 111In emits not only γ-rays, which are used for scintigraphy, but also short-range Auger and conversion electrons, an effect on tumor cell proliferation could be expected. In clinical (7–10) and preclinical (11,12) studies, evidence of tumor response to treatment with 111In-labeled [DTPA0]octreotide was indeed shown.
For radiotherapeutic applications, other radionuclides have also been proposed. Preclinical therapy studies using 90Y- and 64Cu-labeled octreotide and 88Re-labeled RC-160 have been reported, and all showed at least inhibition of tumor growth (12–17). 90Y is a β-particle emitter with a maximum electron energy of 2.3 MeV and a mean range in tissue of up to 12 mm. [Tyr3]octreotide (Fig. 1), which has a higher binding affinity for SST2 than for octreotide itself, has recently been derivatized with the chelator 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA) (Fig. 1), enabling stable radiolabeling with 90Y. Preclinical and clinical studies with [DOTA0,Tyr3]octreotide showed favorable biodistribution and tumor uptake characteristics (18–20). Three different clinical trials on the safety and antiproliferative effects of [90Y-DOTA0,Tyr3]octreotide in patients with neuroendocrine tumors started recently (21–25).
This article expands the initial findings using 90Y-labeled octreotide and gives the results of studies that evaluated the radiotherapeutic effects of 2 different activities (111 and 370 MBq) of [90Y-DOTA0,Tyr3]octreotide in a rat tumor model. The experiments were performed on Lewis rats bearing the somatostatin receptor–positive rat pancreatic CA20948 tumor in their flank. Furthermore, we investigated the influence of tumor size (approximately 0.1–15 cm2) at the onset of therapy on the therapeutic effects.
MATERIALS AND METHODS
Labeled Peptides
90YCl3 was from NEN Life Science Products Inc. (Boston, MA). [DOTA0,Tyr3]octreotide was synthesized as published (26). 90Y labeling of [DOTA0,Tyr3]octreotide was performed as described (18).
Preclinical In Vivo Radionuclide Therapy Experiments Using Radiolabeled Somatostatin Analogs
Rat CA20948 pancreatic tumors were grown in the flank of male Lewis rats (250–300 g; Harlan, Horst, The Netherlands). These rats were injected subcutaneously in both flanks, each with 500 μL of a cell suspension of CA20948 tumor, prepared from 5 g crude, viable tumor tissue in 100 mL saline. After 7–27 d, rats bearing tumors of different size were anesthetized and [90Y-DOTA0,Tyr3]octreotide was injected into the dorsal vein of the penis. The specific activity of [90Y-DOTA0,Tyr3]octreotide was 37 MBq/1.2 μg peptide. Groups of 7–10 rats (typically, 8 rats) were studied. The control group did not receive radiolabeled octreotide. Tumor growth (by measurement of the 2 largest perpendicular diameters using a caliper ruler), animal condition, and body weight were determined at regular intervals. At more progressed stages of the CA20948 tumor, central necrosis may occur with rupture to the surface. Besides loss of >10% of original body weight and tumor growth beyond approximately 20 cm2, tumor necrosis was an indication to kill the rats.
Partial response was defined as at least 50% reduction of the product of 2 perpendicular tumor diameters versus pretreatment values. Complete response was defined as 100% reduction of this product; in addition, this response was defined to last for at least 150 d.
Dosimetry
To determine tumor uptake of [90Y-DOTA0,Tyr3]octreotide for dosimetry, male Lewis rats, bearing rat CA20948 pancreatic tumors of approximately 1 g, were used. Rats were injected under ether anesthesia with 3 MBq (12 μg) 90Y-labeled [DOTA0,Tyr3]octreotide in 200 μL saline into the dorsal vein of the penis. At the indicated time points, rats were killed under ether anesthesia. Tumors were collected and the bremsstrahlung radioactivity in these samples was determined using an LKB-1282-Compu-gamma system (LKB Instruments, Gaithersburg, MD).
The absorbed dose to the rat tumors was calculated assuming uniform distribution of radioactivity in a spheric mass. Tumor-to-tumor absorbed dose was taken into account, and S values (mean absorbed dose per unit cumulated activity) for 90Y in spheres of 1 and 10 g were used as described (27).
RESULTS
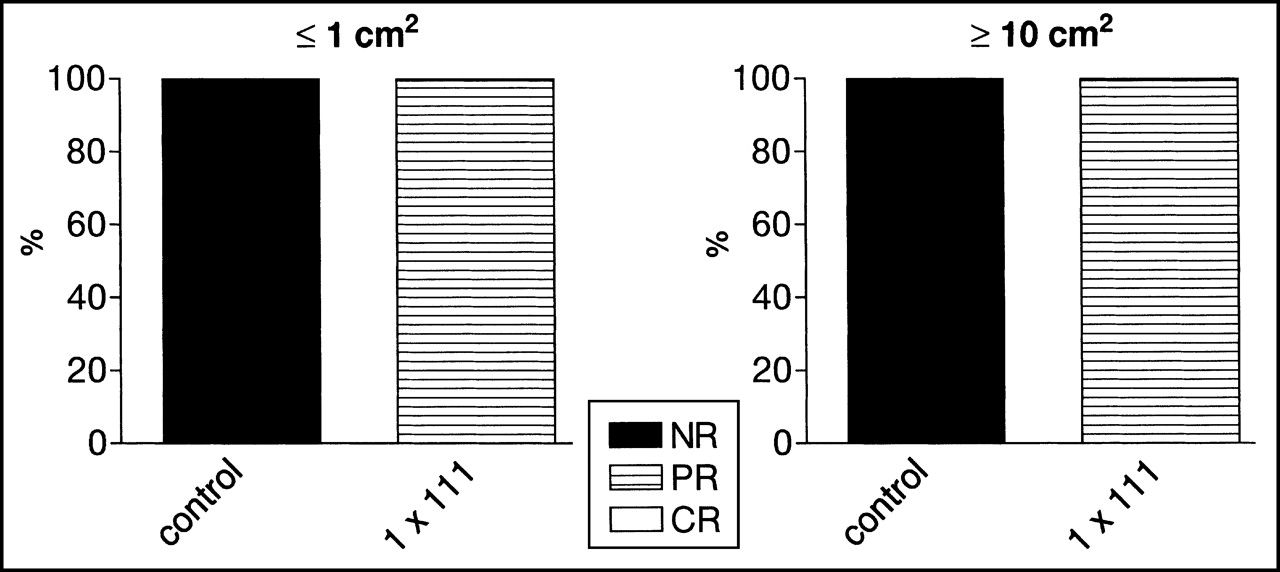
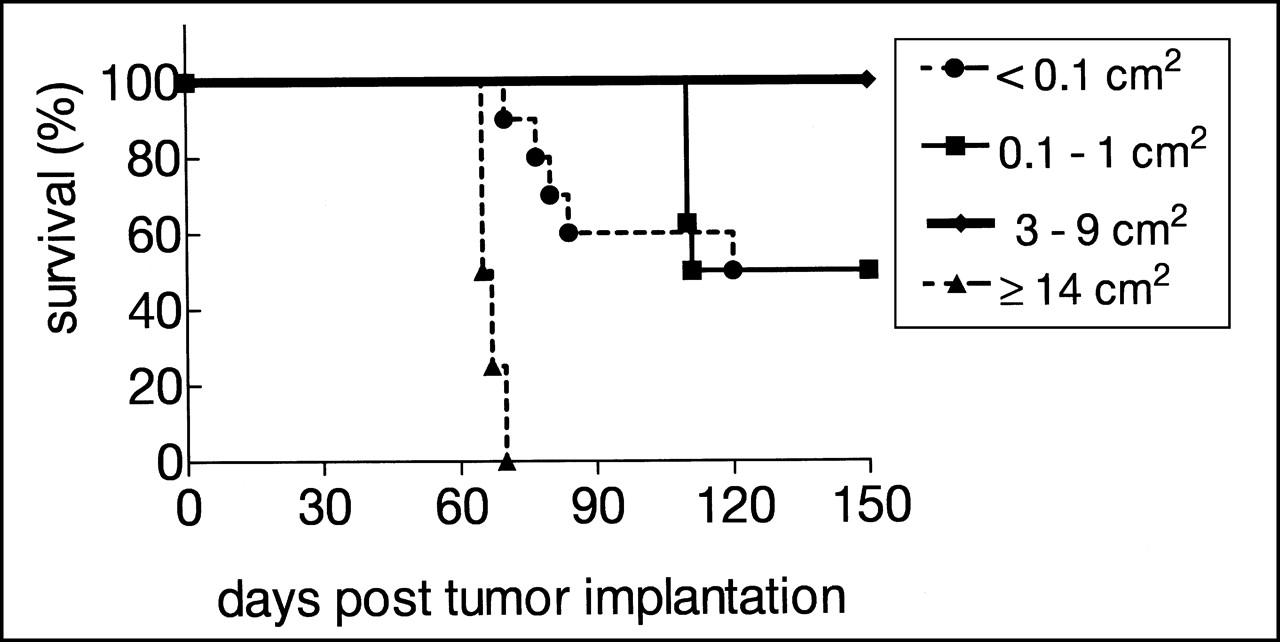
Tumors of the rats in the control group grew excessively and no survival beyond 150 d was found: 0% complete response and also 0% partial response were reached (Figs. 2 and 3). Administration of unlabeled peptide in the same amount as used during radionuclide therapy also did not result in any tumor response (data not shown). After injection of 111 MBq [90Y-DOTA0,Tyr3]octreotide, 100% partial response was found in all rats independent of the tumor size (Fig. 3). Median survival times (the time at which 50% of the rats have died) were 63 and 53 d for small and larger tumors, respectively, after 111 MBq [90Y-DOTA0,Tyr3]octreotide (Table 1). After the highest activity (370 MBq [90Y-DOTA0,Tyr3]octreotide) was administered, these data were 131 and 66 d, respectively, indicating that the results of therapy are dose dependent. After 370 MBq [90Y-DOTA0,Tyr3]octreotide, 50% complete response and 50% partial response were found for the tumors of ≤1 cm2. For the larger tumors (≥14 cm2), only 100% partial response was reached (Fig. 4). Furthermore, the 370-MBq activity also resulted in a difference in the survival curves for these groups of animals with tumors of ≤1 cm2 versus tumors of ≥14 cm2 (Fig. 5). To complete the picture, we also investigated the effect of this activity, 370 MBq [90Y-DOTA0,Tyr3]octreotide, on very small (≤0.1 cm2) and medium-sized (3–9 cm2; mean, 7.8 cm2) tumors. The effects of therapy on growth of the medium-sized tumors are shown in Figure 6. Treatment with a single injection of 370 MBq [90Y-DOTA0,Tyr3]octreotide resulted in complete tumor regression in all animals with medium-sized tumors in about 3 wk. In these rats, a very impressive 100% tumor-free survival (Fig. 5), and thus 100% complete response (Fig. 4), was reached, whereas in rats with tumors of ≤0.1 cm2 after the same activity, the results were less convincing (Figs. 5 and 6). A 50% cure was found in this group, the same figure found for the group of rats with tumors of ≤1 cm2.

Survival curves of rats bearing small (≤1 cm2; solid line) vs. large (≥10 cm2; dashed line) CA20948 tumors after no administration (control) or 111 MBq [90Y-DOTA0,Tyr3]octreotide administration. For all groups, n = 8.
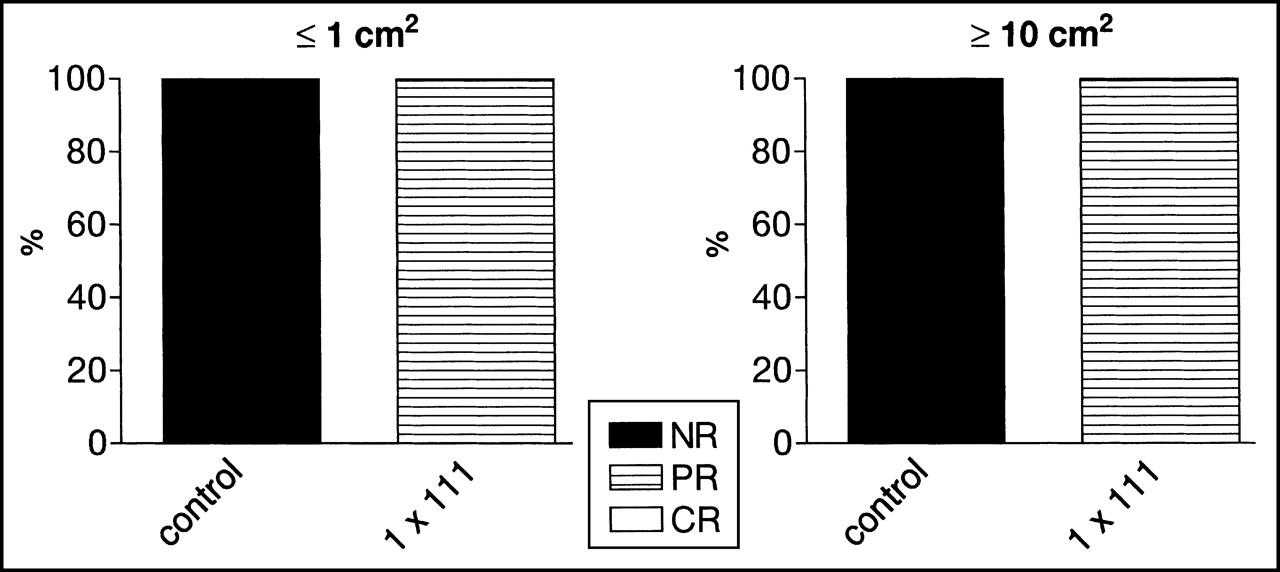
Tumor responses found in rats bearing small (≤1 cm2) vs. large (≥10 cm2) CA20948 tumors after no administration (control) or 111 MBq [90Y-DOTA0,Tyr3]octreotide administration. NR = no response; PR = partial response; CR = complete response. For all groups, n = 8.
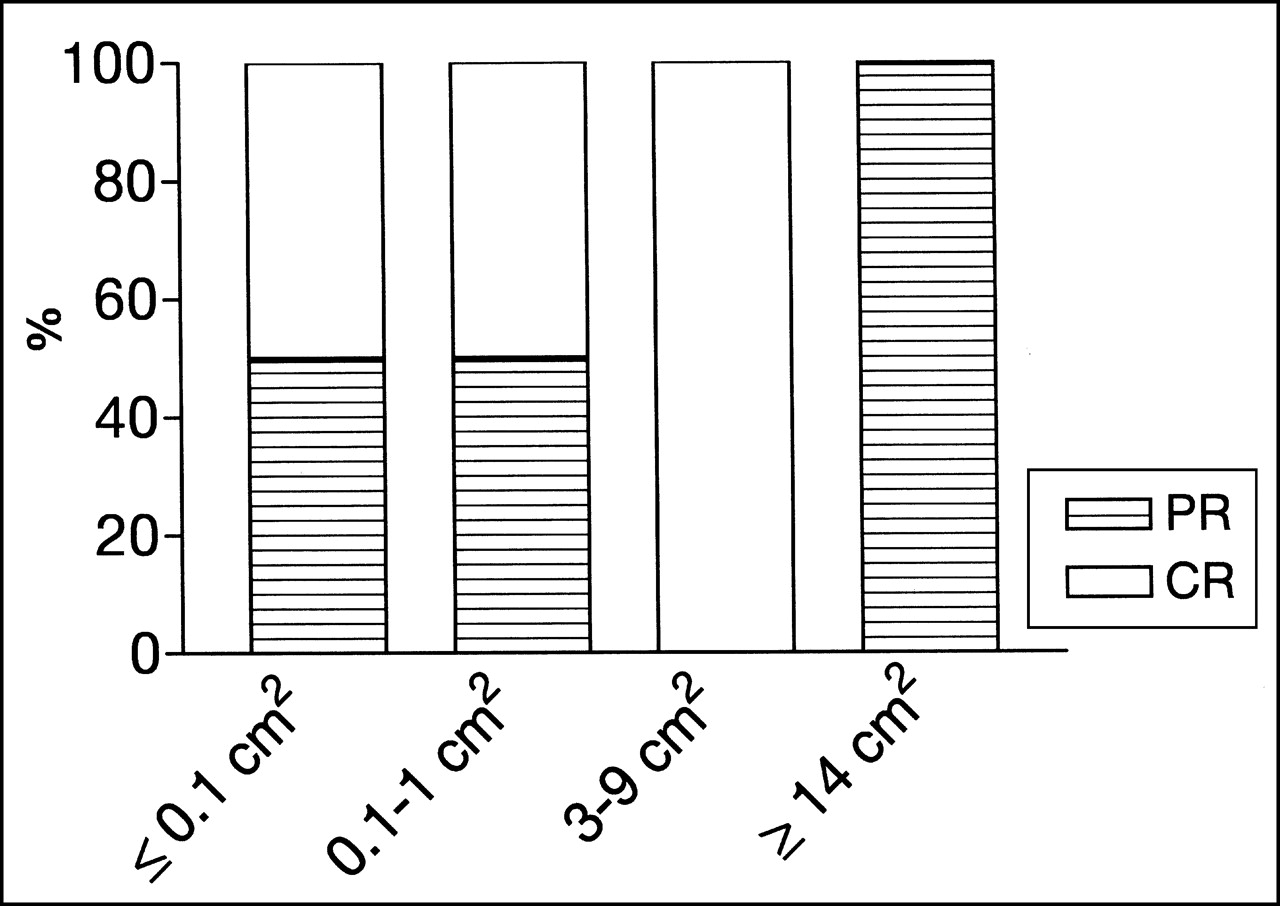
Tumor responses found in rats bearing very small (≤0.1 cm2; n = 10), small (≤1 cm2; n = 8), medium (3–9 cm2; n = 7), or large (≥14 cm2; n = 8) CA20948 tumors after 370 MBq [90Y-DOTA0,Tyr3]octreotide administration. PR = partial response; CR = complete response.

Survival curves of rats bearing very small (≤0.1 cm2; n = 10), small (≤1 cm2; n = 8), medium (3–9 cm2; n = 7), or large (≥14 cm2; n = 8) CA20948 tumors after 370 MBq [90Y-DOTA0,Tyr3]octreotide administration.
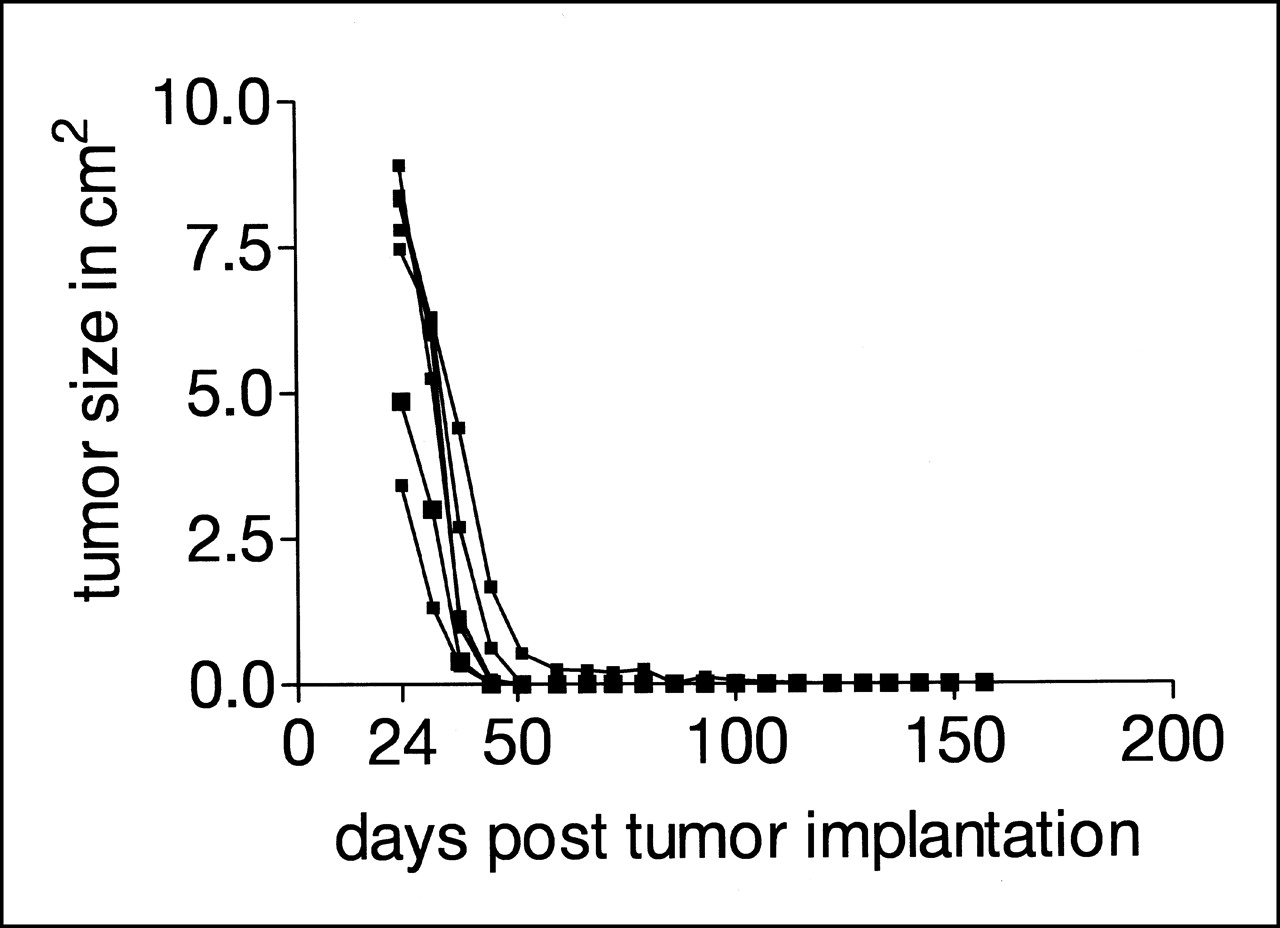
Tumor volumes (3–9 cm2 at onset of therapy on day 24) in rats as function of time after implantation and injection of 370 MBq [90Y-DOTA0,Tyr3]octreotide at 24 d after implantation (n = 7).
Median Survival Time for Rats Bearing CA20948 Tumors of Different Sizes After Injection of Indicated Activities of [90Y-DOTA0,Tyr3]Octreotide
Estimation of tumor absorbed dose was based on biodistribution study data obtained in this rat model (Table 2), with the same unlabeled peptide amount as used in the high-dose therapy studies (12 μg peptide). Using these biodistribution data, estimated tumor absorbed doses were calculated, resulting for [90Y-DOTA0,Tyr3]octreotide in 130 mGy/MBq (for a 1-g tumor) and 160 mGy/MBq (for a 10-g tumor). The absorbed tumor doses for the highest administered activity of 370 MBq are 48 Gy (1-g tumor) to 60 Gy (10-g tumor). Tumor uptake (in percentage injected activity per gram of tumor) in tumors of 1 versus 10 g was not significantly different (data not shown); the lower calculated absorbed doses in the 1-g tumors result from smaller absorbed fractions of the 90Y radiation energy in these tumors.
Radioactivity in CA20948 Rat Tumors
DISCUSSION
Radionuclide therapy using radiolabeled peptides involves the use of these compounds to deliver a cytotoxic dose of radiation to tumor cells. Our results clearly show the ability of [90Y-DOTA0,Tyr3]octreotide to control tumor growth in the rat pancreatic CA20948 tumor model. Complete responses (100%) were measured in the animals bearing medium-sized tumors after 370 MBq [90Y-DOTA0,Tyr3]octreotide.
In this study, a difference was found in the radiotherapeutic effects of [90Y-DOTA0,Tyr3]octreotide in tumors of different sizes. On the basis of a mathematic model examining tumor curability in relation to tumor size for 22 different β-emitting radionuclides, the optimal tumor diameter calculated for 90Y was 34 mm (28), in the same range as the medium-sized tumors used in our studies. Tumors smaller than the optimal size will not absorb all radiation energy of the 90Y electrons and, therefore, will be less vulnerable to this treatment because a substantial part of the disintegrating energy escapes and is deposited outside the tumor volume, as was the case in tumors of ≤1 cm2. Therefore, a better effect of 90Y in the 8-cm2 tumors than in the small tumors in our study could be expected and was indeed found. However, in larger tumors (10–15 cm2), an increased number of clonogenic, presumably hypoxic, cells are present, which have to be sterilized to achieve a cure, thereby limiting radiocurability.
One advantage of radionuclide therapy using radiolabeled peptides is that radiation can be delivered selectively not only to (large) primary tumors but also to subclinical tumors and metastases, which are too small to be imaged and thereby treated by, for example, surgery or external beam radiotherapy. However, 90Y seems less suitable for this latter purpose, as shown in this study, because very small tumors will not be able to absorb all electron energy emitted by 90Y in the tumor cells. To treat patients with tumors of different sizes, a possible solution might therefore be the use of a combination of radionuclides (e.g., the high-energy 90Y for large tumors and an Auger electron emitter or a low-energy β-emitter for smaller tumors and metastases).
The success of the therapeutic strategy relies on the total amount of radioligand that accumulates within tumor cells, which among other things depends on the receptor affinity and rate of internalization of ligand and receptor. We studied internalization of radiolabeled [DOTA0,Tyr3]octreotide in rat pancreatic tumor cells. This process appeared to be receptor specific and temperature dependent, as was found for [111In-DTPA0]octreotide as well (29,30). Furthermore, the amount of radioligand taken up in the tumor may depend on the total amount of unlabeled peptide coinjected and thus on changes in specific activity of the radiolabeled peptide attributed to increase or decrease of the amount of unlabeled peptide (31,32). Changes in specific activity attributed to increase in radioactivity, but with stable peptide concentrations, did not influence tumor uptake over a long range of activities (data not shown).
The CA20849 flank tumor has been shown to be a good model for radionuclide therapy using radiolabeled somatostatin analogs. Significant tumor growth delay but no cure was found in rats bearing small tumors after radionuclide therapy with activities as high as 3 times 740 MBq [64Cu-1,4,8,11-tetraazacyclotetradecane-N,N′,N″N‴-tetraacetic acid (TETA)]octreotide or [64Cu-TETA,Tyr3]octreotate, the first compound given either fractionated or as a single injection (15,16). Dose fractionation induced significantly increased tumor growth inhibition compared with that in rats given a single injection. However, the single 555-MBq activity of [64Cu-TETA]octreotide was bound to twice the amount of peptide compared with the 278-MBq activity. Therefore, partial saturation of the receptors using the single high activity and thus relatively lower uptake of radioactivity in the tumor may have contributed to these findings. Tumor growth inhibition was also found after treatment of CA20948 tumor–bearing rats with [90Y-DTPA0-benzylacetamido,Tyr3]octreotide (13). Using 370 MBq [90Y-DOTA0,Tyr3]octreotide per kilogram, the same group observed complete tumor reduction in 5 of 7 rats (14), in accordance with our current findings.
Recently, [90Y-DOTA0,Tyr3]octreotide has also been introduced in the clinic in different phase 1 and 2 studies. Otte et al. (23,24) described 29 patients who received 4 or more injections of [90Y-DOTA0,Tyr3]octreotide with ascending activity at intervals of approximately 6 wk (cumulative activity, 6,120 ± 1,347 MBq/m2) with the aim of performing an intrapatient dose-escalation study. In total, 127 single treatments were given. In 8 of these 127 single treatments, total activities of ≥3,700 MBq were administered. Twenty of the 29 patients have shown disease stabilization (no tumor growth), 2 a partial remission, 4 a reduction of tumor mass of <50%, and 3 a progression of tumor growth.
Paganelli et al. (21) treated 20 patients, who received 3 equal intravenous injections of [90Y-DOTA0,Tyr3]octreotide. Cohorts of 5 patients were treated starting with 1.1 GBq per fraction in escalating dosage (0.4-GBq increments) in subsequent groups. Complete and partial tumor mass reduction was measured in 25% of the patients along with 55% showing stable disease and 20% progressive disease.
Valkema et al. (25) performed a phase 1 study with [90Y-DOTA0,Tyr3]octreotide to define the maximum tolerable single dose and 4-fraction dose of [90Y-DOTA,Tyr3]octreotide in 22 patients with progressive neuroendocrine tumors. Before treatment, the patients underwent quantitative [86Y-DOTA0,Tyr3]octreotide PET to predict the renal exposure expected with [90Y-DOTA0,Tyr3]octreotide. Escalating activities of 0.9, 1.8, 2.8, and 3.7 GBq/m2 were repeated 3 or 4 times every 6 wk. The cumulative renal absorbed dose was limited to 27 Gy. Because intravenous amino acids were shown to reduce renal exposure, patients received amino acids with [90Y-DOTA0,Tyr3]octreotide. The median follow-up time in the study was 14 mo. Two partial and 3 minor tumor responses were seen: 10 patients had stable disease and 12 patients had symptomatic improvement. In 2 patients with insulinoma, 72-h fasting tests normalized. The maximum cumulative [90Y-DOTA0,Tyr3]octreotide absorbed dose was approximately 26 GBq, without reaching the maximum tolerable dose (25).
CONCLUSION
Radionuclide therapy with [90Y-DOTA0,Tyr3]octreotide is a promising treatment modality for patients bearing SST2-positive tumors. The effects of therapy in our rat tumor model were dependent on tumor size. The best response was achieved in medium-sized tumors of approximately 8 cm2.
Acknowledgments
The authors thank Prof. Helmut R Mäcke (Basel, Switzerland) for the supply of [DOTA0,Tyr3]octreotide.
Footnotes
Received Mar. 14, 2001; revision accepted Aug. 20, 2001.
For correspondence or reprints contact: Marion de Jong, PhD, Department of Nuclear Medicine, University Hospital Rotterdam, 3015 GD Rotterdam, The Netherlands.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 90Y-Edotreotide for Metastatic Carcinoid Refractory to Octreotide
- Treatment of Metastatic Carcinoid Tumors With Radiolabeled Biologic Molecules
- Combined Molecular Targeting for Cancer Therapy: A New Paradigm in Need of Molecular Imaging
- Trifunctional Somatostatin-Based Derivatives Designed for Targeted Radiotherapy Using Auger Electron Emitters
- Therapeutic Efficacy of a 188Re-Labeled {alpha}-Melanocyte-Stimulating Hormone Peptide Analog in Murine and Human Melanoma-Bearing Mouse Models
- Candidates for Peptide Receptor Radiotherapy Today and in the Future
- Combination Radionuclide Therapy Using 177Lu- and 90Y-Labeled Somatostatin Analogs
- A Stylized Computational Model of the Rat for Organ Dosimetry in Support of Preclinical Evaluations of Peptide Receptor Radionuclide Therapy with 90Y, 111In, or 177Lu
- Optimization of Radioimmunotherapy of Renal Cell Carcinoma: Labeling of Monoclonal Antibody cG250 with 131I, 90Y, 177Lu, or 186Re
- New Advances in Peptide Receptor Radionuclide Therapy