


Abstract
Somatostatin receptor (sstr) scintigraphy for imaging and sstr analogs for treatment have been used for more than 20 y. An important improvement in recent years was the introduction of peptide receptor radionuclide therapy with radiolabeled sstr agonists, such as [90Y-DOTA0,Tyr3]octreotide or [177Lu-DOTA0,Tyr3]octreotide (90Y- or 177Lu-DOTATOC, respectively) and [177Lu-DOTA0,Tyr3]octreotate (177Lu-DOTATATE). PET/CT with 68Ga-labeled sstr agonists, such as 68Ga-DOTATOC, 68Ga-DOTATATE, and [68Ga-DOTA,1-Nal3]octreotide (68Ga-DOTANOC), plays an important role in staging and restaging neuroendocrine tumors. Most importantly, sstr scintigraphy and sstr PET/CT can distinguish patients who will qualify for and benefit from peptide receptor radionuclide therapy. This characteristic of sstr targeting is important because it allows a personalized treatment approach (theranostic approach). Until recently, it was thought that internalization of the radiolabeled agonist was mandatory for sstr-mediated imaging and therapy. It was Ginj et al. who proposed in 2006 the paradigm shift that radiolabeled sstr antagonists may perform better than agonists despite the lack of internalization. Despite the rather limited number of head-to-head comparisons of sstr antagonists and agonists, the superiority of sstr antagonists was demonstrated in several cases. From a small library of sstr antagonists, the analog JR11 (Cpa-c[d-Cys-Aph(Hor)-d-Aph(Cbm)-Lys-Thr-Cys]-d-Tyr-NH2), an antagonist with selectivity for sstr subtype 2, showed the best overall characteristics for sstr subtype 2 targeting and was therefore selected for clinical translation. JR11 is under clinical development as a PET imaging agent when labeled with 68Ga (68Ga-NODAGA-JR11 or 68Ga-OPS202) and as a therapeutic agent when labeled with 177Lu (177Lu-DOTA-JR11 or 177Lu-OPS201). In this article, we discuss the development and current status of radiolabeled sstr antagonists. Evidence based on preclinical work, on quantitative in vivo autoradiography of human tumor slices, and on human data now supports a shift to sstr antagonists.
- neuroendocrine tumors
- somatostatin receptor antagonists
- peptide receptor radionuclide therapy
- somatostatin receptor PET/CT
Somatostatin receptors (sstr), especially sstr subtype 2 (sstr2), are highly attractive targets for imaging and treatment of patients with neuroendocrine tumors (NETs) and neuroendocrine neoplasias, respectively. For example, sstr scintigraphy for imaging and sstr analogs (SSA) for treatment have been used for more than 20 y. Important improvements in recent years were the introduction of peptide receptor radionuclide therapy (PRRT) with radiolabeled sstr agonists, such as 90Y- or 177Lu-DOTATOC and 177Lu-DOTATATE, and the introduction of sstr PET/CT with (mainly) 68Ga-labeled sstr agonists, such as DOTATOC, DOTATATE, and DOTANOC (1). sstr PET/CT currently plays an important role in detection of the primary tumor, detection of an unknown primary tumor, staging, restaging, and assessment of the treatment response in patients with NETs (2). Furthermore—and most importantly—sstr scintigraphy and sstr PET/CT can distinguish patients who will qualify for and benefit from PRRT and treatment with SSA. This characteristic of sstr targeting is important because it allows a personalized treatment approach (theranostic approach).
NETTER-1 was the first large, randomized, controlled phase 3 trial evaluating 177Lu-DOTATATE for PRRT in patients with midgut NETs. Progression-free survival rates at month 20 were 65.2% in the 177Lu-DOTATATE group and 10.8% in the control group (high-dose SSA) (3). An interim analysis showed that PRRT has a tendency for longer overall survival than SSA. The results of this trial, first published in an abstract in 2015 (4), already had an impact on the current treatment recommendation and algorithm. PRRT is now recommended by the European Neuroendocrine Tumor Society as second-line treatment after progression under treatment with SSA in patients with metastatic grade 1 or 2 midgut NETs (5). This development indicates that sstr targeting with radiolabeled tracers is relevant not only for imaging but also for treatment of patients with NETs.
An important development in the field of sstr targeting was the recent introduction of sstr antagonists, which seemed to recognize more binding sites on receptors and which showed favorable pharmacokinetics and better tumor visualization than agonists, despite very poor internalization rates (6,7). Current preclinical and clinical evaluations of radiolabeled sstr antagonists for imaging and therapy and their clinical potential, not only in NETs but also in other tumors, are discussed here.
PRECLINICAL DEVELOPMENT OF RADIOLABELED SSTR ANTAGONISTS
In 1996, Bass et al. found that the inversion of chirality at positions 1 and 2 of the octapeptide (octreotide family) converted an agonist into a potent antagonist (8). Soon after, structure–activity relationship studies by Hocart et al. revealed different potent antagonists (9). These antagonists were used as lead structures by Jean Rivier (Salk Institute for Biologic Studies, La Jolla, CA), Jean Claude Reubi (University of Bern, Bern, Switzerland), and Helmut R. Mäcke (University Hospital of Basel, Basel, Switzerland) in collaboration for the development of new sstr antagonists, including DOTA conjugates, for labeling with radiometals (6,10).
First Generation of Radiolabeled sstr Antagonists
The first radiolabeled sstr antagonists were based on the sstr2-selective analog sst2-ANT or BASS (Table 1), developed by Bass et al. (8), and the sstr3-selective antagonist sst3-ODN-8, developed by Reubi et al. (11). Both antagonists were labeled with 111In via the chelator DOTA and were evaluated in vivo using human embryonic kidney (HEK) cell line 293 stably transfected with sstr2. A direct comparison of 111In-DOTA-BASS (50% inhibitory concentration [IC50], 9.4 ± 0.4 nM [mean ± SEM] (6)) and high-affinity 111In-diethylenetriaminepentaacetic acid (DTPA)-TATE (IC50, 1.3 ± 0.2 nM (12)) revealed that tumor uptake for the radiolabeled sstr2 antagonist was 2-fold higher, despite its lower affinity. The same was true for 111In-DOTA-sst3-ODN-8 in a comparison with 111In-DOTANOC in HEK–sstr3 xenografts. Also surprising was the long-lasting tumor uptake of 111In-DOTA-BASS and 177Lu-DOTA-BASS, considering the lack of internalization (13). Conversely, the sstr2 antagonist BASS labeled with 64Cu via the chelator 4,11-bis(carboxymethyl)-1,4,8,11-tetraazabicyclo[6.6.2]hexadecane (CB-TE2A) (64Cu-CB-TE2A-BASS) did not show higher tumor uptake than the agonist 64Cu-CB-TE2A-octreotate in sstr2-positive AR42J xenografts (14). However, in all studies, radiolabeled sstr antagonists recognized a larger number of binding sites in vitro than did agonists (6,14).
Somatostatin Analog Affinities
Second Generation of Radiolabeled sstr Antagonists
The initial indications that antagonists may be superior to agonists led to the design of more potent sstr2 antagonists with improved affinity (10); several were studied as radiotracers (15,16).
On the basis of the new sstr2 antagonist LM3 (p-Cl-Phe-cyclo(d-Cys-Tyr-d-Aph(Cbm)-Lys-Thr-Cys)d-Tyr-NH2), various PET imaging agents were developed using 3 different macrocyclic chelating systems (DOTA, NODAGA, and CB-TE2A) and 2 PET radiometals (68Ga and 64Cu) (16). This study clearly demonstrated that the chelate makes a difference in the affinity and pharmacokinetics of the radiolabeled sstr2 antagonists. For instance, the sstr2 affinity of 68Ga-NODAGA-LM3 was 10-fold higher than that of 68Ga-DOTA-LM3, whereas 64Cu-CB-TE2A-LM3 showed almost no washout from the tumor up to 24 h after injection (unexpected for a noninternalized radioligand)—not the case with 64Cu-NODAGA-LM3. These findings may be important if therapy with the β−-emitter 67Cu (half-life, 62 h) is being considered. However, the ratios of tumor to normal tissue were remarkably higher for 64Cu-NODAGA-LM3; this parameter is important for good image contrast.
A more comprehensive study involving the evaluation of 3 different sstr2 antagonists—LM3, JR10 (p-NO2-Phe-c[d-Cys-Tyr-d-Aph(Cbm)-Lys-Thr-Cys]-d-Tyr-NH2), and JR11 (Cpa-c[d-Cys-Aph(Hor)-d-Aph(Cbm)-Lys-Thr-Cys]-d-Tyr-NH2)—in combination with 2 chelators (DOTA and NODAGA) and various (radio)metals—including In(III), Y(III), Lu(III), Cu(II), and Ga(III)—clearly demonstrated the extremely high sensitivity of the antagonists to modifications such as complexation with distinct radiometals or substitution of a chelator by another (15). The gallium-labeled DOTA analogs had lower affinity for sstr2 than the respective Y(III)-DOTA, Lu(III)-DOTA, or In(III)-DOTA counterparts. Interestingly, however, substitution of DOTA by the NODAGA chelator was able to substantially increase the binding affinity of the Ga(III)-NODAGA analogs, compared with the Ga(III)-DOTA analogs. That study illustrated the great potential of the antagonists, because even a low-affinity antagonist was shown to be slightly superior to a high-affinity agonist, outweighing the affinity differences. More specifically, 68Ga-DOTA-JR11, having a dramatically lower affinity for sstr2 (∼150-fold) than 68Ga-DOTATATE (Table 1), showed a tumor uptake that was 1.3-fold higher, and 68Ga-NODAGA-JR11, having a 6-fold lower affinity than 68Ga-DOTATATE (Table 1), showed a tumor uptake that was up to 1.7-fold higher (15).
Of the radiolabeled sstr2 antagonists mentioned so far, the analog JR11 performed the best in preclinical settings. JR11 was selected for clinical development as a PET imaging agent labeled with 68Ga using the chelator NODAGA (68Ga-NODAGA-JR11 or 68Ga-OPS202) and as a therapeutic agent labeled with 177Lu using the chelator DOTA (177Lu-DOTA-JR11 or 177Lu-OPS201).
Preclinical Evaluation of Radiolabeled sstr Antagonists for Treatment
Three preclinical studies investigating different aspects of the use of radiolabeled antagonists for PRRT have been published. These studies focused on the new therapeutic agent 177Lu-DOTA-JR11 (177Lu-OPS201) and explored its biodistribution, pharmacokinetics, dosimetry, and therapeutic effect. The studies were performed in 3 different animal models: 2 tumor-bearing murine models for a comparison to the established agonist 177Lu-DOTATATE (17,18) and 1 tumor-free porcine model for dosimetry purposes (19).
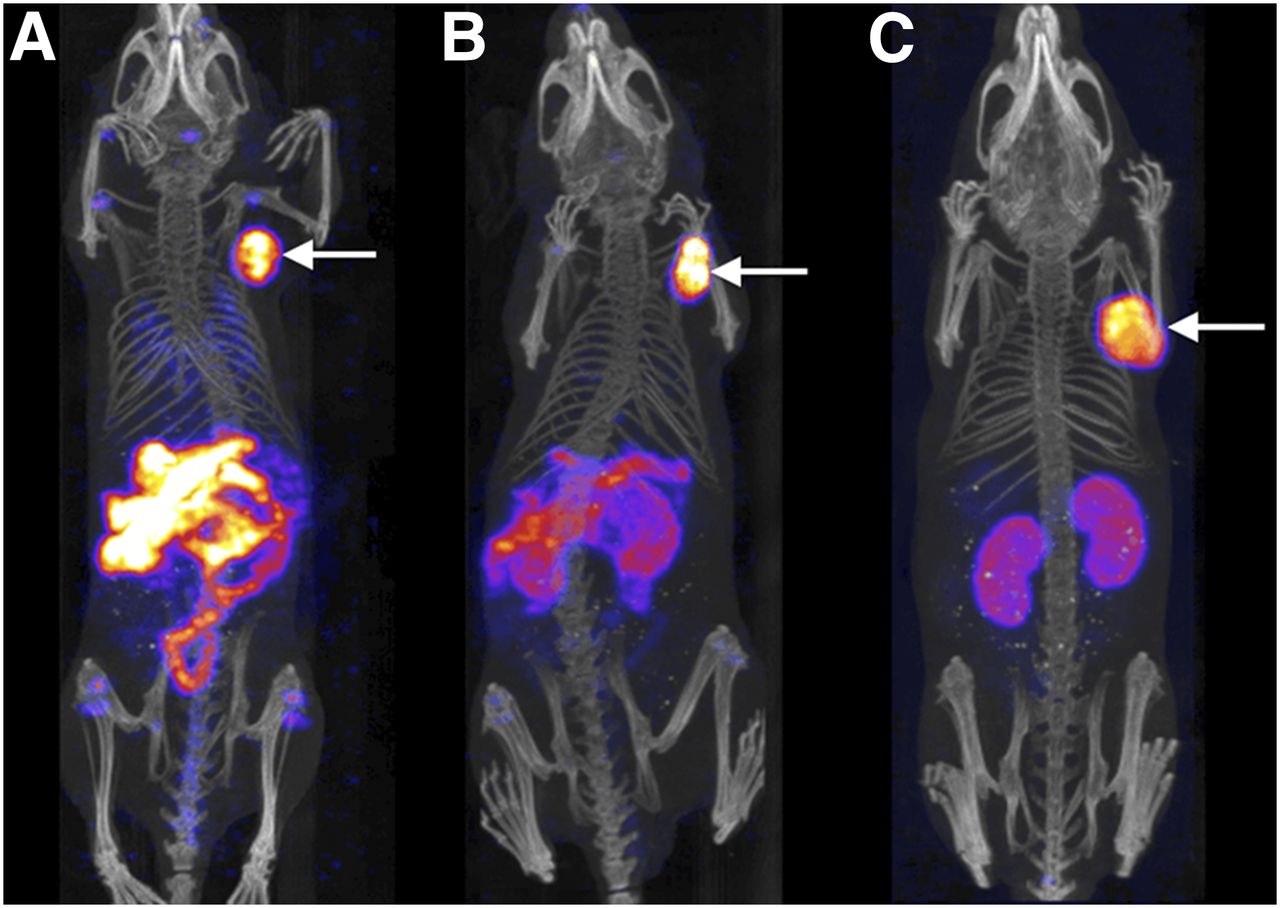
A head-to-head comparison of 177Lu-DOTA-JR11 and 177Lu-DOTATATE was performed with HEK–hsstr2 (human sstr2) xenografts (18). After administration of 10 pmol of peptide, 177Lu-DOTA-JR11 showed significantly higher tumor uptake (23.9 ± 4.5 percentage injected activity per gram) than 177Lu-DOTATATE (17.8 ± 4.4 percentage injected activity per gram) at 4 h after injection. Most importantly, this increase persisted over time, resulting in a tumor radiation dose that was 2.6 times higher for the radiolabeled sstr2 antagonist than for the agonist (18). The results of the mass escalation study were impressive, showing that optimization of the administered peptide amount enabled substantial suppression of the background activity, whereas tumor uptake was not significantly affected (Fig. 1). Consequently, increasing the administered amount of 177Lu-DOTA-JR11 to a certain extent (from 10 to 200 pmol) may improve the safety profile of PRRT and reduce potentially hematologic toxicity (18).

Nano-SPECT/CT maximum-intensity-projection images of HEK–hsstr2 xenografts 4 h after administration of 20 pmol (A), 200 pmol (B), and 2,000 pmol (C) of 177Lu-DOTA-JR11 (177Lu-OPS201). Increase in peptide amount significantly decreased background activity, whereas tumor uptake (arrows) was not significantly affected. (Adapted from (18).)
Using H69 xenografts, Dalm et al. reported tumor uptake that was 5 times higher for 177Lu-DOTA-JR11 than for 177Lu-DOTATATE at 4 h after injection and a tumor radiation dose that was 4.4 times higher after the administration of approximately 300 pmol of each radiotracer (17). In an in vivo therapy study, compared with 177Lu-DOTATATE, 177Lu-DOTA-JR11 resulted in a higher median survival rate (71 vs. 61 d) and in a longer delay (1.4 times) in tumor growth (26 ± 7 vs. 18 ± 5 d). Despite the fact that 88% ± 1% of the sstr2 antagonist remained on the surface of the cells, 177Lu-DOTA-JR11 showed higher uptake and caused at least 60% more DNA double-strand breaks than 177Lu-DOTATATE, for which the internalization rate was high (74% ± 3%) (17).
In addition to 177Lu-DOTA-JR11, Nicolas et al. investigated 90Y- and 111In-DOTA-JR11 as potential therapeutic alternatives (18). 90Y-DOTA-JR11 showed an approximately 20% lower tumor-to-kidney uptake ratio than 177Lu-DOTA-JR11 while having an approximately 5 times higher effective dose, both of which negatively affected its therapeutic index in comparison to the 177Lu-labeled compound. Nicolas et al. also showed that 111In-DOTA-JR11 cannot be used as a surrogate of 90Y-DOTA-JR11 because of differences in their pharmacokinetics and affinity for sstr2 (18). Whether Auger electron emitters in combination with antagonists can be applied to PRRT remains unclear, but 111In-DOTA-JR11 exhibits excellent properties as an imaging agent.
Novel Indications for Tumor Targeting with Radiolabeled sstr Antagonists
The better performance of radiolabeled sstr antagonists than of agonists was also impressively demonstrated with human tumor specimens (20). About 60 human tissue samples from different tumors were analyzed by in vitro receptor autoradiography to compare the binding capacities of 125I-JR11 (sstr2 antagonist) and 125I-Tyr3-octreotide (sstr2 agonist) in successive tissue sections. The sstr2-binding affinities (IC50s) of both 125I-labeled tracers were similar (20). Both radioligands efficiently bound to sstr2 in different tumor tissues. However, in all cases, the radiolabeled antagonist 125I-JR11 bound to more sstr2 sites in different tumors—with uptake from 3.8 to 21.8 times higher—than the agonist 125I-Tyr3-octreotide (Table 2). Such significantly increased binding may not only increase the localization accuracy for tumors and metastases but also increase the efficacy of therapeutic interventions with radiolabeled sstr antagonists. Of particular interest is the fact that tumors other than gastroenteropancreatic NETs and lung NETs become targets for sstr2 antagonists despite low sstr2 densities; these tumors include breast cancer, small cell lung cancer, renal cell cancer, non-Hodgkin lymphomas, pheochromocytomas, and medullary thyroid cancer (Table 2). These tumors are not among those currently being routinely investigated with sstr imaging.
Sstr2 Binding in Different Tumors
These in vitro human tumor data, together with the in vivo animal tumor data, are strong arguments that radiolabeled antagonists should be clinically tested in a wide range of tumors, including those other than NETs. Radiolabeled sstr2 antagonists should be useful not only for tumor imaging but also for targeted radionuclide therapy (theranostic approach).
CLINICAL DEVELOPMENT OF RADIOLABELED SSTR ANTAGONISTS
Initial Human Studies with Diagnostic sstr Antagonists
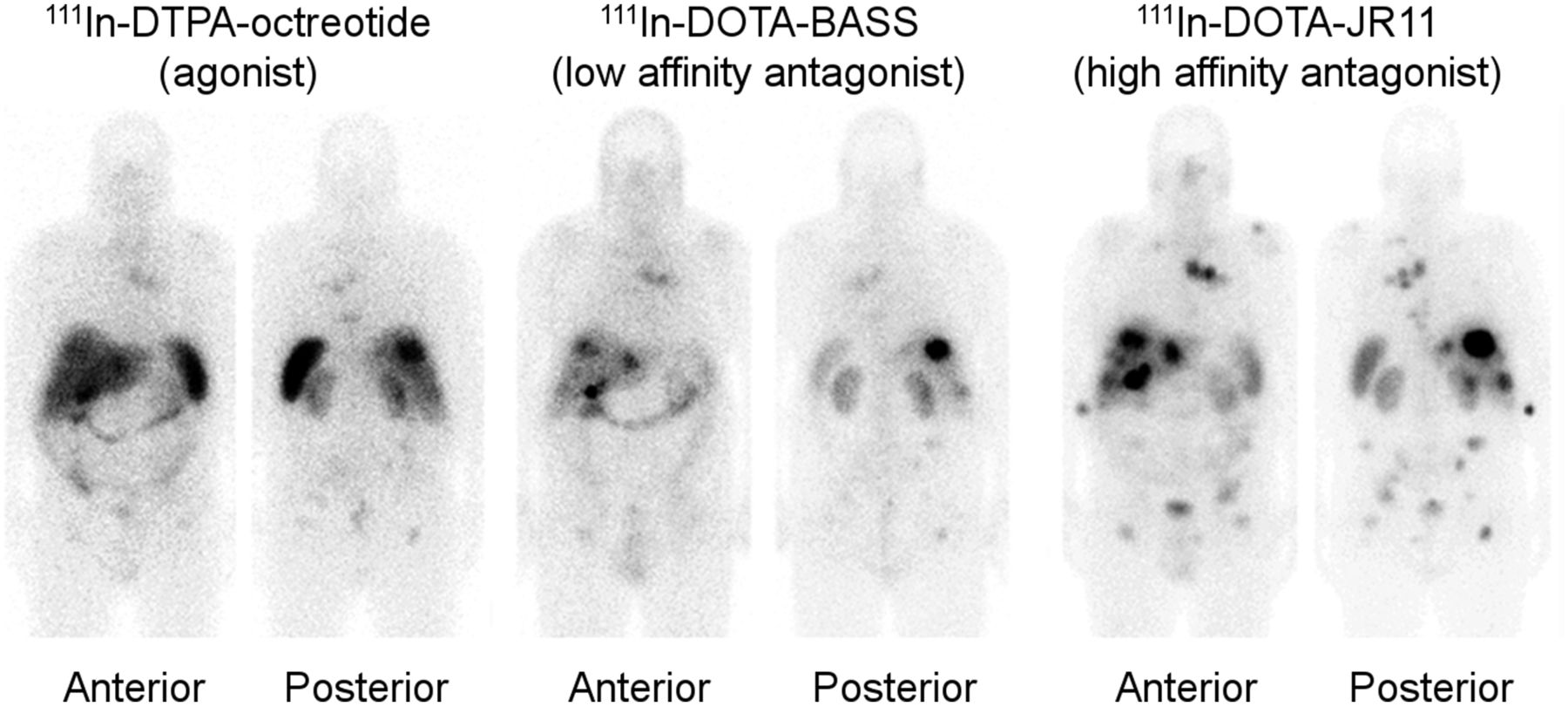
There is preclinical evidence that the higher tumor uptake and better tumor-to-background contrast of radiolabeled sstr2 antagonists than of agonists (15) may improve the image quality and detection rate of sstr SPECT and PET. A pilot study in 5 patients with NETs or thyroid cancer provided the first evidence that sstr imaging with the sstr2 antagonist 111In-DOTA-BASS was more effective than that with the U.S. Food and Drug Administration–approved radiotracer 111In-DTPA-octreotide (OctreoScan; Mallinckrodt); the main advantages of the radiolabeled sstr2 antagonist were higher tumor uptake (4-fold), higher tumor-to-liver background ratios (∼2-fold), and a greater number of detectable lesions (25/28 lesions vs. 17/28 lesions) (7). Figure 2 shows 111In-DTPA-octreotide, 111In-DOTA-BASS, and another sstr2 antagonist (111In-DOTA-JR11) with improved sstr2 affinities in the same patient. The affinity profiles of all 3 radiotracers are shown in Table 1.
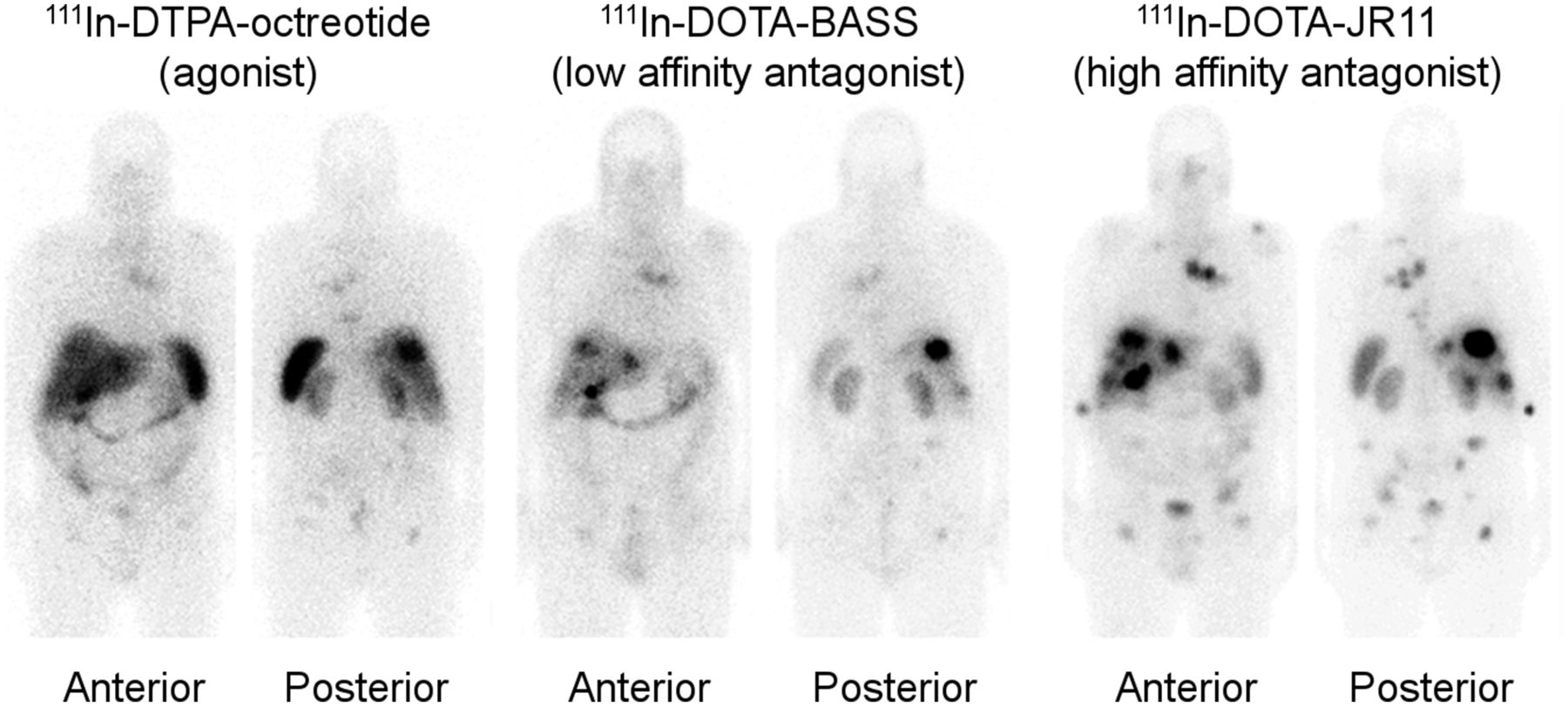
Comparison of 111In-DTPA-octreotide, 111In-DOTA-BASS, and 111In-DOTA-JR11 scintigraphy 24 h after administration of radiotracer in same patient with metastatic NET of unknown origin (grade G2). High-affinity sstr2 antagonist 111In-DOTA-JR11 showed higher tumor uptake and detected many more metastases than sstr agonist 111In-DTPA-octreotide and sst2 antagonist 111In-DOTA-BASS.
On the basis of affinity studies and preclinical results, the sstr2 antagonist 68Ga-NODAGA-JR11 (Table 1) was selected for further clinical PET development. A phase 1/2 study comparing, in the same patients, PET/CT with 2 microdoses of 68Ga-NODAGA-JR11 (68Ga-OPS202) and PET/CT with 68Ga-DOTATOC was recently conducted (ClinicalTrials.gov identifier: NCT02162446). That study indicated increased image contrast for both doses of 68Ga-NODAGA-JR11 because of lower hepatic, intestinal, and pancreatic uptake, which, in turn, resulted in sensitivity and diagnostic accuracy higher than that of 68Ga-DOTATOC PET/CT for staging well-differentiated to moderately differentiated gastroenteropancreatic NETs (21). A “theranostic pair”—68Ga-DOTA-JR11 and 177Lu-DOTA-JR11 (Table 1)—was also investigated in NET patients in a single-center study (ClinicalTrials.gov identifier: NCT02609737).
Initial Human Studies with Therapeutic sstr Antagonists
There is preclinical evidence that radiolabeled sstr2 antagonists generate higher tumor doses and larger numbers of DNA double-strand breaks than agonists, resulting in better treatment efficacy (17,18). Indeed, sstr2 antagonist 177Lu-DOTA-JR11 was more effective than sstr2 agonist 177Lu-DOTATATE in a first-in-human study with 4 patients who had metastasized neuroendocrine neoplasias (grades G1–G3); the most relevant findings of that study were higher tumor doses (3.5-fold) (because of longer residence time and higher tumor uptake), higher tumor-to-kidney dose ratios (>2-fold), tumor doses of up to 487 Gy after treatment with 3 cycles (total, 15.2 GBq) of 177Lu-DOTA-JR11, and high metabolic stability of 177Lu-DOTA-JR11 (because no metabolites were found in the urine) (22). Figure 3 shows a comparison of 177Lu-DOTA-JR11 scintigraphy and 177Lu-DOTATATE scintigraphy as well as 3-dimensional voxel dosimetry analysis in patient 4 of that study. 177Lu-DOTA-JR11 (177Lu-OPS201) is currently being evaluated in a phase 1/2 multicenter study (ClinicalTrials.gov identifier: NCT02592707) and in a theranostic study (ClinicalTrials.gov identifier: NCT02609737).
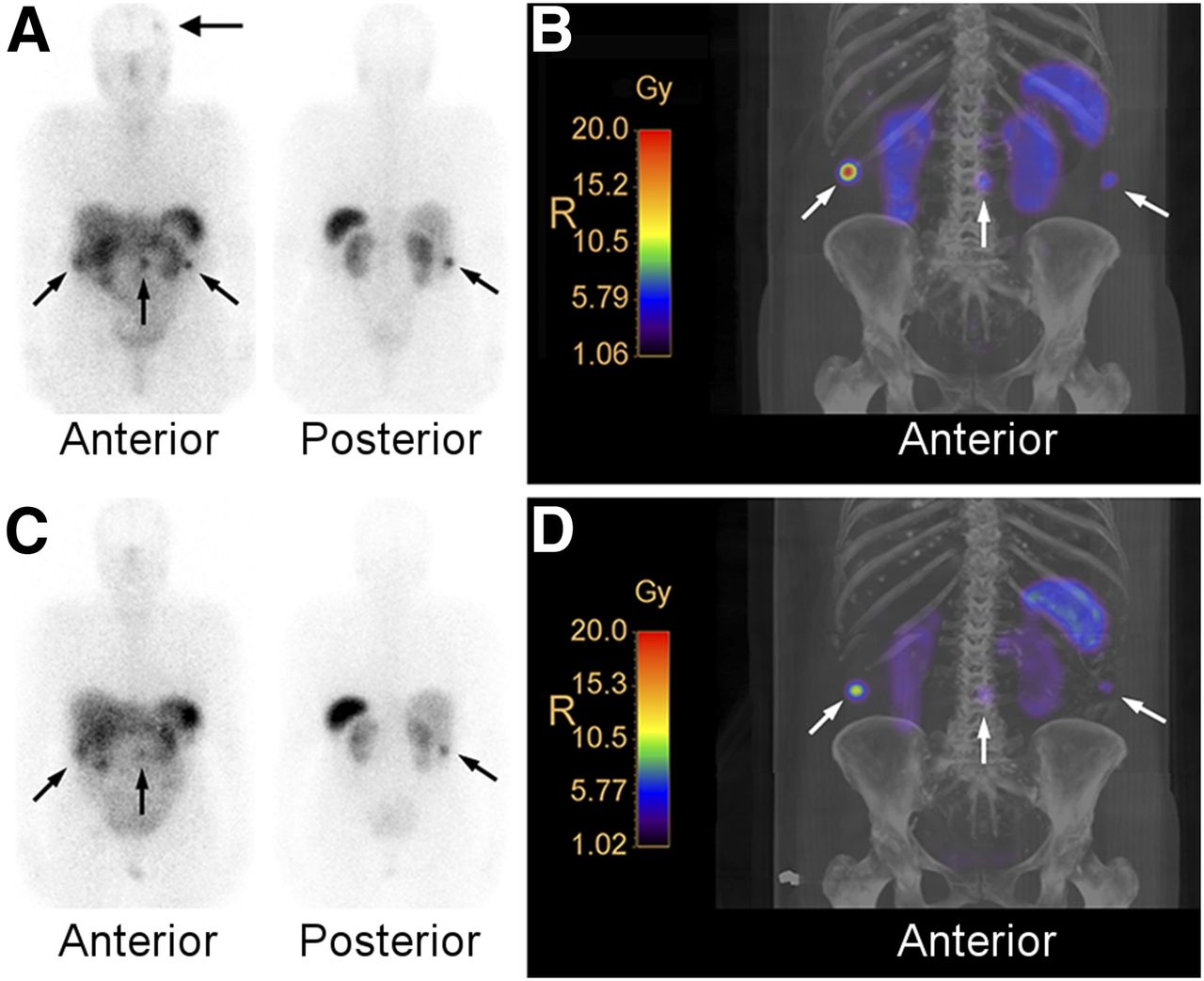
Comparison of 177Lu-DOTA-JR11 (A and B) and 177Lu-DOTATATE (C and D) in same patient with metastatic NET of ileum (grade G2). Planar scintigraphy 24 h after injection of 1,086 MBq of 177Lu-DOTA-JR11 (A) and corresponding maximum-intensity-projection (MIP) image of isodose curves (B). Planar scintigraphy 24 h after injection of 994 MBq of 177Lu-DOTATATE (C) and corresponding MIP image of isodose curves (D). Interval for injections was 3 wk. Large black arrow in A shows possible meningioma. Small black and white arrows show tumor lesions. Three-dimensional voxel dosimetry analysis revealed tumor doses of 4.2–20 Gy/GBq for 177Lu-DOTA-JR11 and 1.5–8.5 Gy/GBq for 177Lu-DOTATATE (see scales in B and D).
FUTURE DEVELOPMENTS
Further evaluation of the diagnostic–therapeutic pair 68Ga-NODAGA-JR11–177Lu-DOTA-JR11 is warranted in larger-scale multicenter clinical trials as a theranostic approach in patients with gastroenteropancreatic NETs and other NETs. Other tumors that should be evaluated further with sstr antagonists are breast cancer, small cell lung cancer, renal cell cancer, non-Hodgkin lymphomas, pheochromocytomas, medullary thyroid cancer, and other neoplasms with sstr2 expression, including tumors with low levels of sstr2 expression. Optimizing the antagonist peptide amount, hepatic intraarterial injection, and use of alternative radionuclides (such as α-emitters and β+-emitters) with longer half-lives may further improve sstr targeting with radiolabeled antagonists. Last, but not least, other receptor systems, such as the gastrin-releasing peptide receptor and cholecystokinin receptor subtype 2, are alternative targets for radiolabeled antagonists.
CONCLUSION
Until recently, it was thought that internalization of the radiotracer was mandatory for sstr-mediated imaging and therapy. In 2006, Ginj et al. proposed that radiolabeled sstr antagonists may perform better than agonists despite the lack of internalization (6). Recent advantages described in this article provide evidence that radiolabeled sstr antagonists have the potential to improve imaging and therapy not only of NETs but also of tumors that have not yet been the focus of sstr targeting. There is now evidence for a shift from radiolabeled sstr agonists to antagonists.
DISCLOSURE
Damian Wild is a consultant for Ipsen Pharma SAS. No other potential conflict of interest relevant to this article was reported.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 7, 2017.
- Accepted for publication April 26, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison of the tolerability of 161Tb- and 177Lu-labeled somatostatin analogues in the preclinical setting
- 68Ga-SSO-120 PET for Initial Staging of Small Cell Lung Cancer Patients: A Single-Center Retrospective Study
- The Emergence of Somatostatin Antagonist-Based Theranostics: Paving the Road Toward Another Success?
- Targeted {alpha}-Emitter Therapy with 212Pb-DOTAMTATE for the Treatment of Metastatic SSTR-Expressing Neuroendocrine Tumors: First-in-Humans Dose-Escalation Clinical Trial
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy
- A Prospective, Randomized, Double-Blind Study to Evaluate the Safety, Biodistribution, and Dosimetry of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 in Patients with Well-Differentiated Neuroendocrine Tumors
- Peptide Receptor Radionuclide Therapy with 67Cu-CuSarTATE Is Highly Efficacious Against a Somatostatin-Positive Neuroendocrine Tumor Model
- Revisiting Weight-Normalized SUV and Lean-Body-Mass-Normalized SUV in PET Studies
- Head-to-Head Comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: A Prospective Study
- Training Requirements for Theranostics: A Unique Opportunity for Collaboration
- Combination of 5-Fluorouracil with Epigenetic Modifiers Induces Radiosensitization, Somatostatin Receptor 2 Expression, and Radioligand Binding in Neuroendocrine Tumor Cells In Vitro
- New Developments in Peptide Receptor Radionuclide Therapy
- Sensitivity Comparison of 68Ga-OPS202 and 68Ga-DOTATOC PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase II Imaging Study
- Theranostic Concepts: More Than Just a Fashion Trend--Introduction and Overview