


Abstract
Peptide receptor-targeted radionuclide therapy of somatostatin receptor-expressing tumors is a promising application of radiolabeled somatostatin analogs. Suitable radionuclides are 90Y, a pure, high-energy β-emitter (2.27 MeV), and 177Lu, a medium-energy β-emitter (0.5 MeV) with a low-abundance γ. Methods: Lewis rats, each bearing both a small (approximately 0.5 cm2) and a large (7–9 cm2) somatostatin receptor-positive rat pancreatic CA20948 tumor in their flanks, were used. We investigated the radiotherapeutic effects of [90Y-tetraazacyclododecanetetraacetic acid (DOTA),Tyr3]octreotide, [90Y-DOTA,Tyr3]octreotate, [177Lu-DOTA,Tyr3]octreotate, and the combination of 90Y- and 177Lu-labeled analogs at the same tumor radiation dose (60 Gy). Results: Radiotherapeutic effects of the 90Y- and 177Lu-labeled analogs were found in the rat tumor model. In these animals bearing tumors of different sizes, the antitumor effects of the combination of 50% 177Lu- plus 50% 90Y-analogs were superior to those in animals treated with either 90Y- or 177Lu- analog alone. In smaller tumors, the 90Y radiation energy was not completely absorbed in the tumor, whereas in larger tumors the increased number of clonogenic tumor cells at the fixed level of absorbed dose may account for the failure of 177Lu alone to go completely into remission. Conclusion: This study shows the superior antitumor effects of the combination of 177Lu- and 90Y-somatostatin analogs when compared with either 90Y- or 177Lu-analog alone in animals bearing tumors of various sizes.
Radiolabeled receptor-binding peptides have been shown to be an important class of radiopharmaceuticals for tumor diagnosis and therapy. The specific and high-affinity receptor-binding property of the peptide can be exploited by labeling with a radionuclide and using the radiolabeled peptide as a vehicle to guide radioactivity to tissues expressing a particular receptor. The high affinity of the peptide for its receptor and the internalization of the receptor–peptide complex facilitates retention of the radionuclide in receptor-expressing tumors, whereas its relatively small size facilitates rapid clearance from the blood. Peptides most successfully applied for these purposes are somatostatin analogs that bind to receptors overexpressed on neuroendocrine tumors (1). Peptides labeled with γ- or positron emitters enable noninvasive visualization of receptor-expressing tumors. In addition, when labeled with therapeutic radionuclides these peptides have the potential to eradicate receptor-expressing tumors—an approach referred to as peptide receptor radionuclide therapy (PRRT).
Currently, 90Y, a pure, high-energy β-emitter (2.27 MeV), and 177Lu, a medium-energy β-emitter (0.5 MeV) with a low-abundance γ, are the most frequently used radionuclides in PRRT. We have previously shown that the somatostatin analog [tetraazacyclododecanetetraacetic acid (DOTA),Tyr3]octreotide (DOTATOC) (Fig. 1) can form a stable complex with 90Y (2,3). In rats with subcutaneous tumors, 90Y-DOTATOC effectively controlled tumor growth (4). Studies to determine the therapeutic efficacy of 90Y-DOTATOC in patients with cancer are ongoing at various institutions (5–14). The most promising rate of complete plus partial responses seen in the various 90Y-DOTATOC studies consistently exceeds that obtained with [111In-diethylenetriaminepentaacetic acid]octreotide (15).
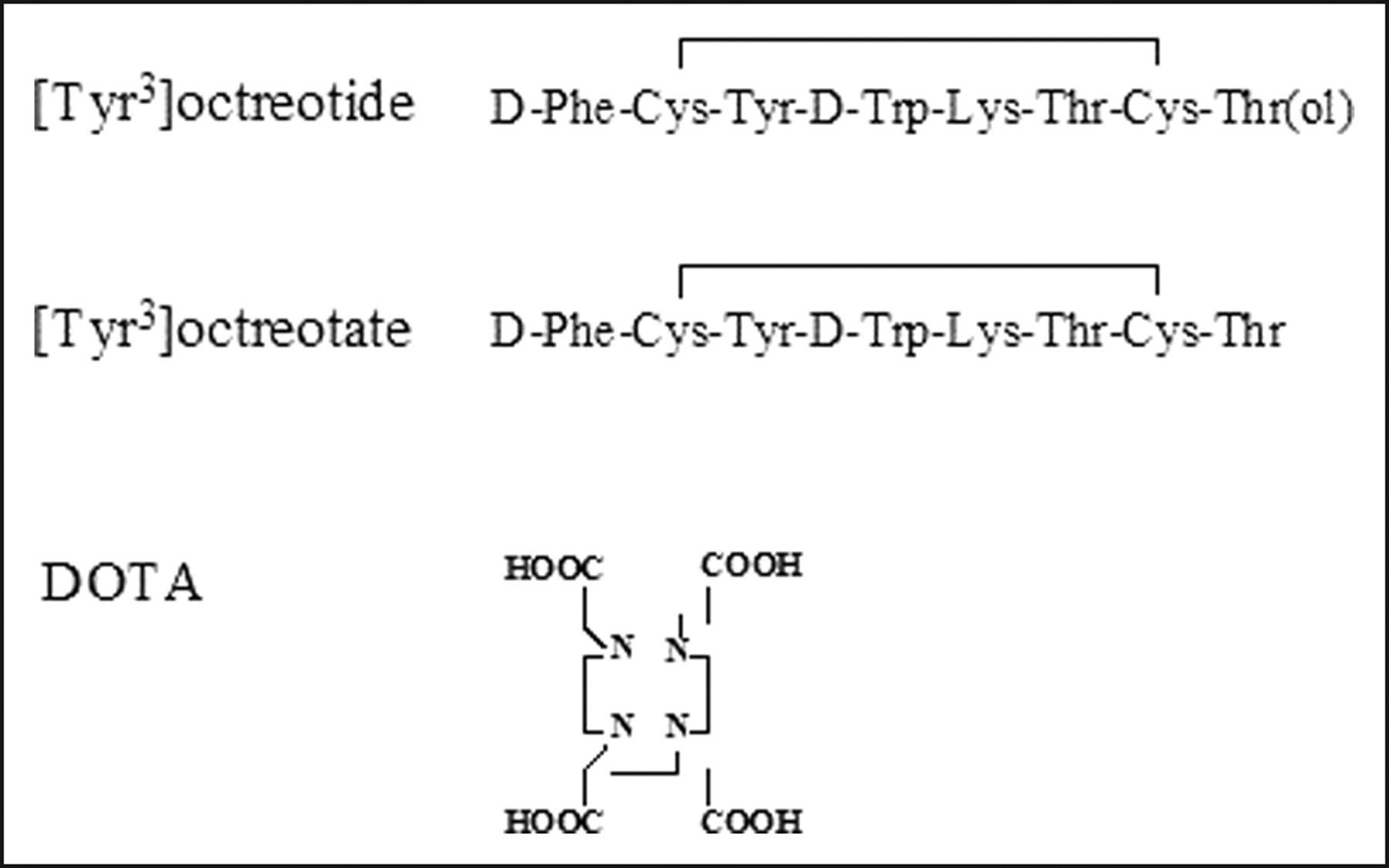
Structures of the somatostatin analogs Tyr3-octreotide and Tyr3-octreotate and of the chelator DOTA.
The new somatostatin analog Tyr3-octreotate has an increased receptor affinity compared with octreotide and Tyr3-octreotide (16,17). We investigated the antitumor effects of [177Lu-DOTA,Tyr3]octreotate (DOTATATE) (Fig. 1) in various models, including a rat liver micrometastatic tumor model and subcutaneous tumor models. 177Lu-DOTATATE showed excellent antitumoral effects in both tumor models (18,19).
When patients with gastroenteropancreatic neuroendocrine tumors were treated with 177Lu-DOTATATE, complete or partial remissions were documented in an impressive 30% of patients and minor responses in 21%, whereas 26% of patients with progressive disease at the start of PRRT showed stabilization (20).
Comparison of the characteristics of the β-emitters 177Lu and 90Y (Table 1) shows that each has specific potential advantages for tumor therapy. 90Y particles have higher energies and longer particle ranges, leading to more radioactivity in the tumor cell per peptide molecule and to a better crossfire through the tumor, which is especially advantageous in larger tumors and in tumors with heterogeneous receptor distribution. The shorter half-life of 90Y leads to a higher dose rate. 177Lu particles, on the other hand, have lower energy and smaller particle range, leading to better absorption in smaller tumors (Table 2). In addition, 177Lu emits γ-radiation with an energy suitable for scintigraphy, enabling dosimetry during PRRT, and also has a longer half-life, making shipping more convenient.
Characteristics of 90Y, 177Lu, and 131I
Percentage Energy Absorption of 90Y and 177Lu β-Emissions in Spheres (23)
In preclinical PRRT studies, good tumor responses were found using either 177Lu-DOTATATE or 90Y-DOTATOC. Effects, however, varied with tumor size, consistent with a computer model of tumor cure that calculated that 177Lu should work optimally in small tumors, whereas 90Y would be better for larger tumors (4,19,21).
The aim of the current studies was to expand on previous studies in rats using the clinically applied somatostatin analogs for PRRT, 177Lu-DOTATATE, 90Y-DOTATOC, or their combination, in rats bearing 2 tumors of different sizes. To exclude the effects of different peptide analogs used in the clinical studies (i.e., octreotate and octreotide), we also studied the PRRT effects of the same peptide analog, DOTATATE, labeled with 90Y or 177Lu.
The combination of different therapy modalities holds interest as a means of improving the clinical therapeutic effects of radiolabeled peptides. This includes the potential of a combination of different radionuclides, such as 177Lu- and 90Y-labeled somatostatin analogs, to reach a wider tumor region.
MATERIALS AND METHODS
Radiolabeled Peptides
90YCl3 (NEN Life Science Products Inc.), 177Lu (IDB Holland BV), and DOTATATE (BioSynthema) were obtained from commercial sources. DOTATOC was synthesized as described in a previous publication (22). 90Y labeling of DOTATOC/DOTATATE and 177Lu labeling of DOTATATE also were performed as described previously (3,19).
Animals
Rat CA20948 pancreatic tumors were grown in the flanks of male Lewis rats (weight, 250–300 g). Five hundred microliters of a cell suspension of CA20948 tumor, prepared from 5 g of crude, viable tumor tissue in 100 mL saline, were injected subcutaneously into one flank, with an injection into the other flank about 3 weeks later. After 7–27 d, rats bearing 2 tumors of different sizes were anesthetized and 90Y-DOTATOC, 90Y-DOTATATE, 177Lu-DOTATATE, or a combination of 90Y- and 177Lu-labeled analogs at the same tumor radiation dose was injected into the dorsal vein of the penis. The specific activities of 90Y-DOTATOC/DOTATATE and 177Lu-DOTATATE were 37 MBq/1.2 μg peptide and 37 MBq/μg peptide, respectively. Groups of 8–15, with an average of 12 rats per group, were studied. Control groups did not receive radiolabeled octreotide.
Tumor growth (determined by measurement of the 2 largest perpendicular diameters using a caliper ruler), animal condition, and body weight were assessed at regular intervals. In addition to 10% loss of original body weight, tumor growth beyond approximately 15 cm2 was used as a progression point at which animals were sacrificed.
Statistical analysis was performed on survival curves using the logrank test (GraphPad Prism 4).
Dosimetry
The dose to rat tumors in grays was calculated assuming uniform distribution of radioactivity in a spheric mass. Only tumor-to-tumor dose was considered, and S values (mean absorbed dose per unit cumulated activity) for 177Lu and 90Y in spheres of appropriate size were used with tumor uptake data from biodistribution studies as described previously (4,19,23).
RESULTS
PRRT Using 177Lu-DOTATATE, 190Y-DOTATOC, and a Combination
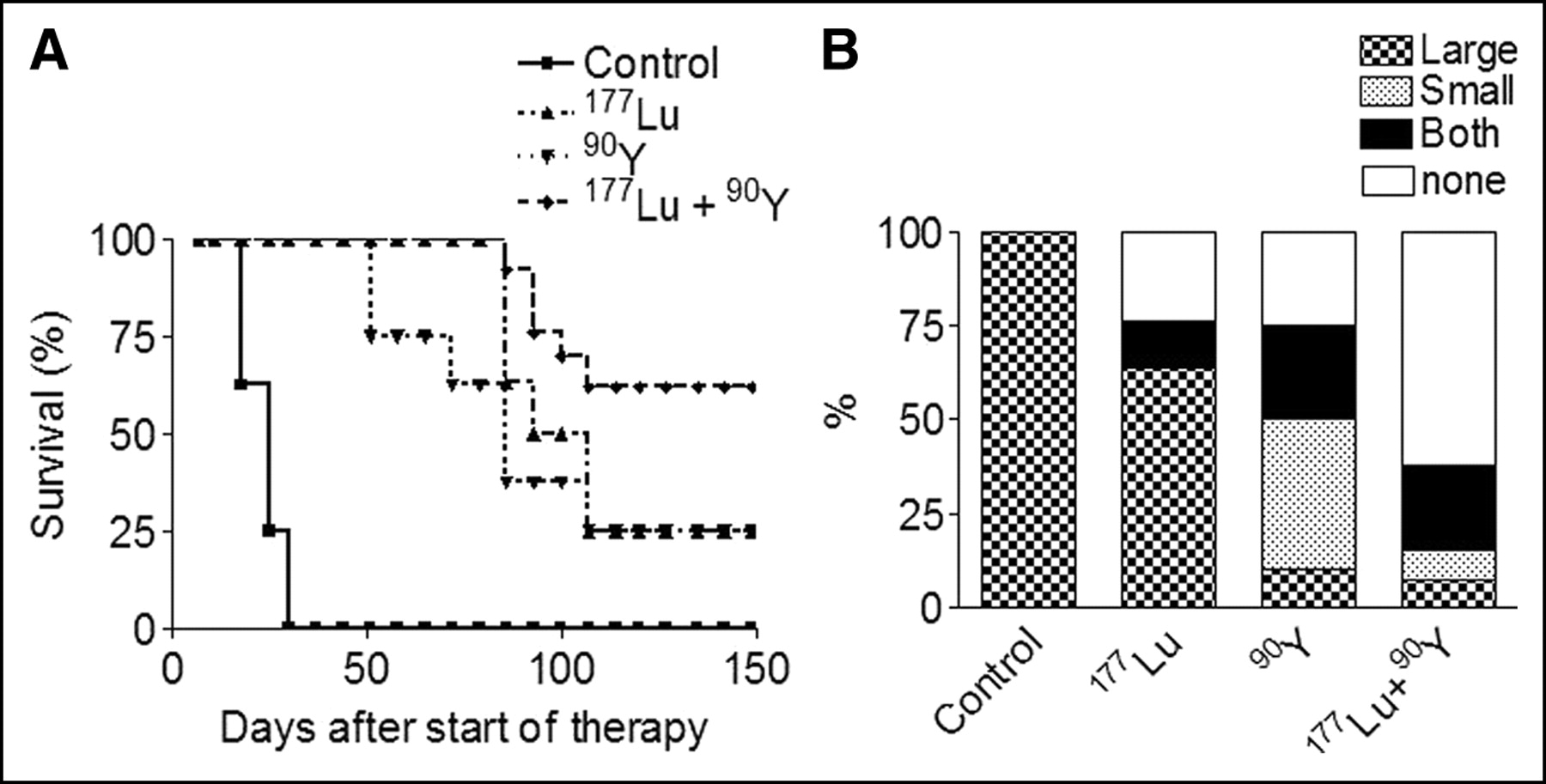
Tumors of rats in the control group and in the group treated with 370 MBq 90Y-DOTA grew excessively, with no survival beyond 150 d (Fig. 2A). Administration of any unlabeled peptide in the same amounts used during PRRT also resulted in no tumor response (data not shown). After injection of 370 MBq 90Y-DOTATOC or 555 MBq 177Lu-DOTATATE, each leading to doses of 60 Gy to the larger tumors, survivals were somewhat better, although in these groups few rats survived the full period of 150 d (the rat equivalent of human 5-y survival). Significantly better (P < 0.001) survival was seen after PRRT with the combination of 185 MBq 90Y-DOTATOC and 278 MBq 177Lu-DOTATATE (Fig. 2A). Areas under the curve were 34, 42, 75, 75, and 130 d for control rats and rats treated with 90Y-DOTA, 90Y-DOTATOC, 177Lu-DOTATATE, and the combination, respectively.

(A) Survival curves of groups of rats (n = 8–15), each bearing both a small (approximately 0.5 cm2) and a large (7–9 cm2) somatostatin receptor-positive rat pancreatic CA20948 tumor in the flanks. Rats were treated with single intravenous administrations of 370 MBq 90Y-DOTATOC (indicated as 90Y), 370 MBq 90Y-DOTA, 555 MBq 177Lu-DOTATATE (indicated as 177Lu), or 185 MBq 90Y-DOTATOC plus 278 MBq 177Lu-DOTATATE (indicated as 177Lu + 90Y). Control rats did not receive radioactivity. (B) Bars indicate the criteria for euthanasia. Rats were sacrificed when size of large tumors, small tumors, or both tumors exceeded 15 cm2. When neither tumor grew, animals were sacrificed at day 150 after therapy.
For the combination of 177Lu- and 90Y-labeled analogs, the median survival (the time point at which 50% of the rats died) was not reached by 150 d, whereas for the other groups this point was at 75 d or less, showing the superior effects of the combination therapy.
Figure 2B illustrates the criteria used for euthanasia in the various rat groups. These included tumor growth beyond the maximum size of 15 cm2 for tumors classified as large at start of therapy, for tumors classified as small at the start of therapy, or for both tumors. When no tumors grew after therapy, animals were sacrificed at day 150 after therapy. Control animals and animals treated with 90Y-DOTA were sacrificed because the large tumor reached 15 cm2 first, although at the same time all small tumors were growing quickly. Only after PRRT with 177Lu-DOTATATE or 90Y-DOTATOC was there sufficient tumor growth inhibition in the large tumor in some animals to allow the small tumor to equal its size. In these animals, the criterion for euthanasia was that both tumors reached 15 cm2. The percentage of such animals was higher after 90Y-DOTATOC than after 177Lu-DOTATATE PRRT, showing the greater capacity of 90Y to control growth in larger tumors. Combination therapy, however, achieved by far the best response, with 60% of animals surviving 150 d after PRRT.
PRRT Using 177Lu-DOTATATE, 90Y-DOTATOC, and a Combination
Tumors of rats in the control group grew rapidly. After injection of 2 × 111 MBq 90Y-DOTATATE (2 injections, 2 weeks apart) or 2 × 278 MBq 177Lu-DOTATATE (2 injections, 2 weeks apart) leading to doses of 60 Gy to the larger tumors, survivals were somewhat better than in the first study. Twenty-five percent of the animals survived the 150 d (Fig. 3A). Significantly better (P < 0.001) survival was observed after PRRT with the combination of 2 × 56 MBq 90Y-DOTATOC and 2 × 140 MBq 177Lu-DOTATATE. Areas under the curve were 18, 88, 96, and 125 d for control rats and rats treated with 90Y-DOTATATE, 177Lu-DOTATATE, and the combination, respectively.
(A) Survival curves of groups of rats (n = 8–15), each bearing both a small (approximately 0.5 cm2) and a large (7–9 cm2) somatostatin receptor-positive rat pancreatic CA20948 tumor in the flanks. Rats were treated with 2 intravenous administrations (2 wk apart) of 2 × 111 MBq 90Y-DOTATOC (indicated as 90Y), 2 × 278 MBq 177Lu-DOTATATE (indicated as 177Lu), or 2 × 56 MBq 90Y-DOTATOC plus 2 × 140 MBq 177Lu-DOTATATE (indicated as 177Lu + 90Y). Control rats did not receive radioactivity. (B) Bars indicate the criteria for euthanasia. Rats were sacrificed when size of large tumors, small tumors, or both tumors exceeded 15 cm2. When neither tumor grew, animals were sacrificed at day 150 after therapy.
For the combination of 177Lu- and 90Y-labeled analogs, median survival was not reached by 150 d, whereas for the other groups it was ≤95 d, showing the superior effects of the combination therapy.
Figure 3B illustrates the criteria used for killing in the various rat groups. Again, control animals were killed when the “large” tumor reached 15 cm2 first. Only after PRRT with 177Lu-DOTATATE or 90Y-DOTATOC was there sufficient tumor growth inhibition of the large tumor in these animals to allow the small tumor to equal at least the large tumor in size. By far the best response was reached after combination therapy, with 62% of the animals surviving 150 d after PRRT.
These data show again the promise of PRRT using 177Lu and 90Y and the potential of the combination of these radionuclides with different β-energies and particle ranges to achieve higher cure rates in tumors of various size.
DISCUSSION
PRRT using radiolabeled somatostatin analogs is a promising new treatment option for patients with metastasized, somatostatin receptor-positive neuroendocrine tumors. One advantage of PRRT is that radiation can be delivered selectively not only to (large) primary tumors but also to subclinical tumors and metastases that are too small to be imaged and thereby identified for surgery or external beam radiotherapy. Clinical trials have demonstrated that both 177Lu and 90Y are suitable β-emitting radionuclides for PRRT. 177Lu and 90Y differ markedly in their physical properties, including half-life, path length, and type of energy emissions (Table 1). Potential advantages of 177Lu for PRRT include a longer half-life, an emission spectrum that allows for dosimetric studies and therapy using the same compound, and β-particle ranges suitable for small tumors (Table 2). By contrast, 90Y emits β-particles with longer path lengths and higher energies and so may be preferable to 177Lu for patients with bulky disease, poorly vascularized solid tumors, or tumors with heterogeneous receptor distribution. However, given the high tumor-absorbed doses for patients receiving PRRT and the relatively long particle range of 90Y β-emissions used for PRRT, there is a possibility of large absorbed doses to tissues adjacent to or surrounding small tumors. Because tumors may be adjacent to critical organs, normal tissues may receive large absorbed doses.
Sparks et al. (24) studied the deposition of energy from emissions of 131I (with characteristics similar to 177Lu) and 90Y to assess the possible magnitude of absorbed doses in tissues adjacent to tumors. Mathematic models were constructed to simulate situations such as tumor wrapped around a small cylinder (e.g., a nerve or artery), tumor against a tissue (e.g., the pericardium or wall of any gastrointestinal tract organ), and tumor surrounded by any soft tissue. The absorbed dose for tissues close to tumors containing 90Y ranged from 24% of tumor absorbed dose at 1 mm from the tumor to 103% of tumor absorbed dose for small structures (such as nerves or arteries) surrounded by tumor. For tissues close to tumors containing 131I, this range was 4%–46%. This study showed that when absorbed doses to tumors are high, absorbed dose to adjacent tissues can also be high, potentially causing toxicities. Doses to adjacent tissues vary with tumor size and the energy of the radionuclide. 90Y seems less suitable for PRRT of small tumors, because very small tumors will not be able to absorb all electron energy emitted by 90Y in the tumor cells (4) (Table 2).
177Lu β-emissions, on the other hand, have energies and particle ranges much more suitable for treatment of small tumors. However, with the increase of clonogenic cells in larger tumors, the probability of cure decreased more rapidly than with 90Y. This might be explained by a lack of uniformity of the activity distribution over the tumor, because for nonuniform activity distributions, even at the same average dose, a higher energy emitter will produce a more uniform and therefore more effective absorbed dose distribution. Another relevant factor in the comparison of 177Lu and 90Y is the difference in half-life. Because 177Lu has a longer half-life, it will take longer to deliver the same dose as 90Y (i.e., the dose rate will be lower). This will render it less effective, because the tumor cell population will have more time for proliferative regeneration.
To treat patients with tumors of various sizes with nonhomogenous receptor distribution, a possible solution might therefore be the use of a combination of radionuclides (e.g., the high-energy 90Y for large tumors and a low-energy β-emitter, such as 177Lu, for smaller tumors and metastases).
These results showed striking radiotherapeutic effects achieved by the combination of 177Lu- and 90Y-labeled somatostatin analogs in tumors of different size, in agreement with a mathematical model evaluating tumor curability using 22 different β-emitting radionuclides in relation to tumor size (21). The model yielded an optimal tumor size for curability for the different radionuclides. The optimal tumor diameter calculated for 90Y was 34 mm, in the same range as the larger tumor diameters in the studies, and the optimal tumor diameter calculated for 177Lu was 2 mm, in the same range as the smaller tumor diameters in our studies.
Although this report focuses on the effects of combination therapy using simultaneous administration of 177Lu- and 90Y-somatostatin analogs, another interesting option is repeated administration with these analogs (e.g., an initial administration of 90Y-labeled analog to treat the larger tumors, followed by 177Lu-labeled analog in the next treatment cycle(s) for treatment of smaller metastases).
CONCLUSION
These studies show the potential of the combination of radionuclides with different β-energies and particle ranges to achieve higher cure rates in tumors of various sizes.
Acknowledgments
The authors thank Dr. Joseph O’Donoghue for expert discussions.
Footnotes
Received June 7, 2004; revision accepted Sep. 16, 2004.
For correspondence or reprints contact: Marion de Jong, PhD, Department of Nuclear Medicine, Erasmus Medical College, Dr Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: m.hendriks-dejong{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Evaluation of 177Lu-OncoFAP-23, a Multivalent FAP-Targeted Radiopharmaceutical Therapeutic for Solid Tumors
- Tandem Isotope Therapy with 225Ac- and 177Lu-PSMA-617 in a Murine Model of Prostate Cancer
- Dosimetry in Radiopharmaceutical Therapy
- Combination Strategies to Improve Targeted Radionuclide Therapy
- Dosimetry Estimate and Initial Clinical Experience with 90Y-PSMA-617
- Penetrating the Barriers to Successful {alpha}-Radioimmunotherapy
- First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease
- Preclinical Evaluation of a Tailor-Made DOTA-Conjugated PSMA Inhibitor with Optimized Linker Moiety for Imaging and Endoradiotherapy of Prostate Cancer
- Somatostatin Receptor-Targeted Radiopeptide Therapy with 90Y-DOTATOC and 177Lu-DOTATOC in Progressive Meningioma: Long-Term Results of a Phase II Clinical Trial
- GEP-NETS UPDATE: Radionuclide therapy in neuroendocrine tumors
- In Vivo Localization of 90Y and 177Lu Radioimmunoconjugates Using Cerenkov Luminescence Imaging in a Disseminated Murine Leukemia Model
- Radiobiologic Optimization of Combination Radiopharmaceutical Therapy Applied to Myeloablative Treatment of Non-Hodgkin Lymphoma
- Cohort Study of Somatostatin-Based Radiopeptide Therapy With [90Y-DOTA]-TOC Versus [90Y-DOTA]-TOC Plus [177Lu-DOTA]-TOC in Neuroendocrine Cancers
- In Vitro Evaluation of Targeted Antisense 177Lu Radiotherapy
- Hepatic arterial infusion enhances DOTATOC radiopeptide therapy in patients with neuroendocrine liver metastases
- 4-Step Renal Dosimetry Dependent on Cortex Geometry Applied to 90Y Peptide Receptor Radiotherapy: Evaluation Using a Fillable Kidney Phantom Imaged by 90Y PET
- Treatment of Metastatic Carcinoid Tumors With Radiolabeled Biologic Molecules
- Somatostatin analogues in the control of neuroendocrine tumours: efficacy and mechanisms
- Radiolabeled and Native Antibodies and the Prospect of Cure of Follicular Lymphoma
- Nuclear Uptake and Dosimetry of 64Cu-Labeled Chelator Somatostatin Conjugates in an SSTr2-Transfected Human Tumor Cell Line
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- Auger Electrons: Lethal, Low Energy, and Coming Soon to a Tumor Cell Nucleus Near You
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- 89Zr as a PET Surrogate Radioisotope for Scouting Biodistribution of the Therapeutic Radiometals 90Y and 177Lu in Tumor-Bearing Nude Mice After Coupling to the Internalizing Antibody Cetuximab