


Article Figures & Data
Figures
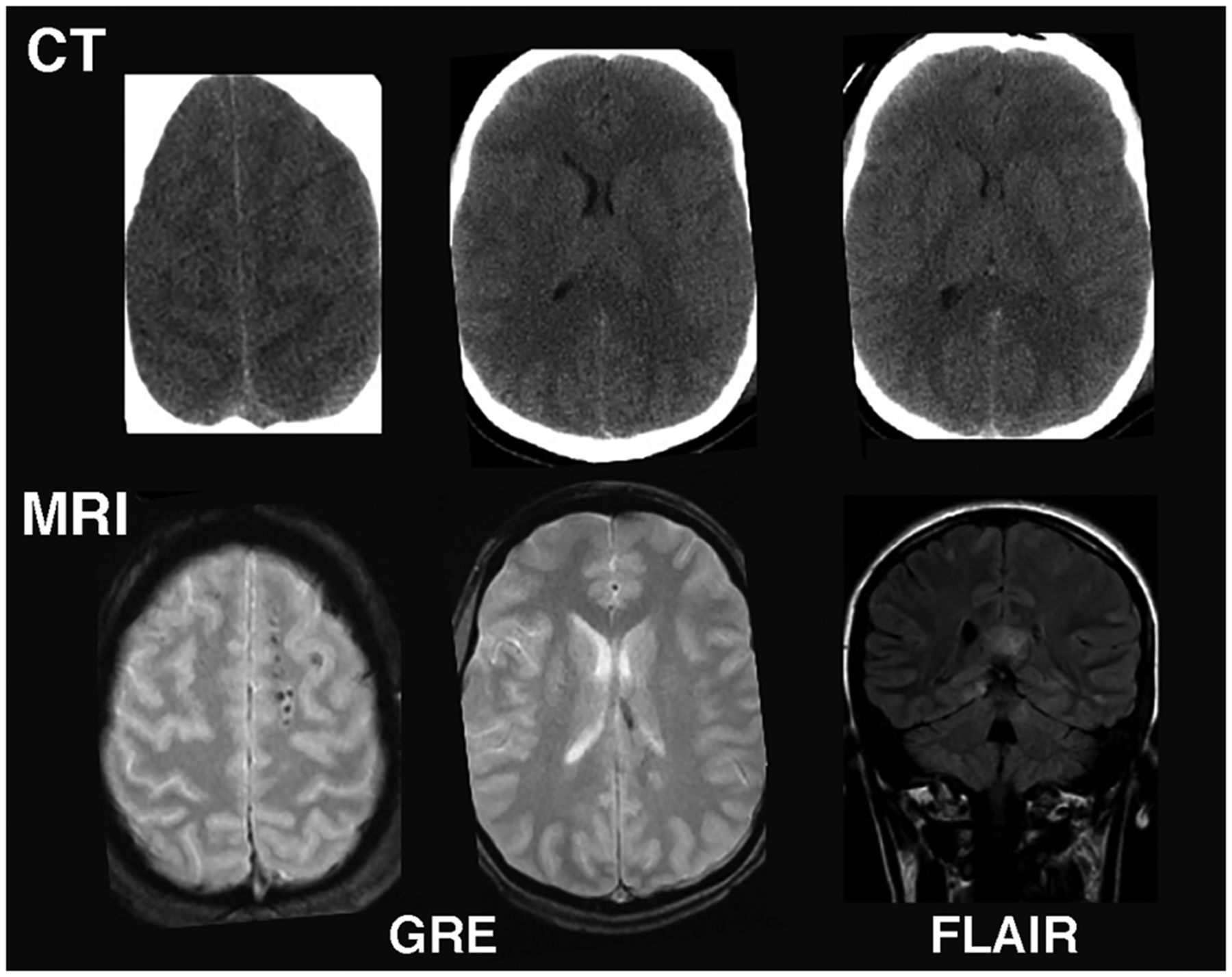
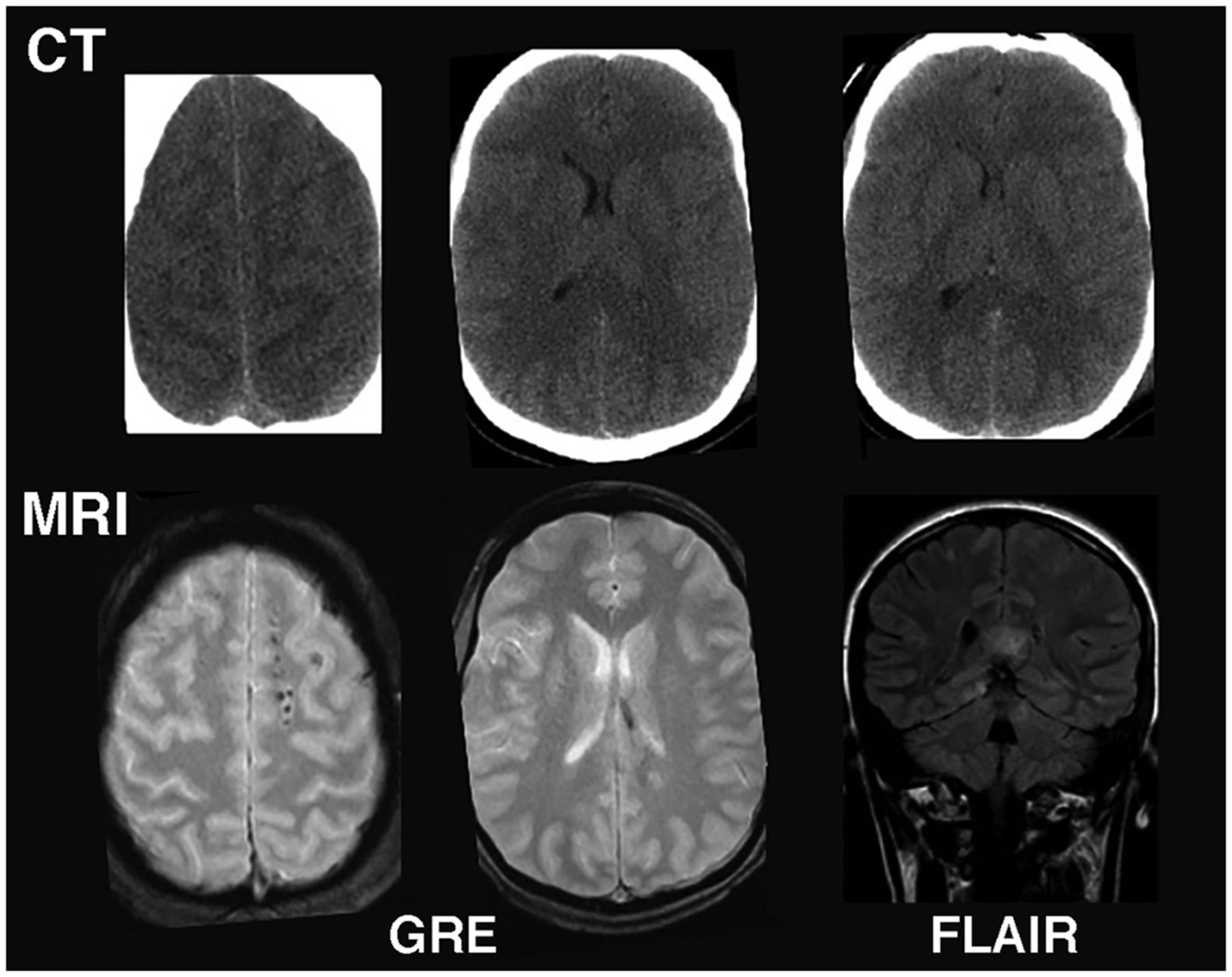
- FIGURE 1.
MRI vs. CT for imaging acute mTBI: Example from mTBI patient in which CT was read as normal. However, subsequent MRI showed multiple small, elliptic lesions in white matter on gradient-echo image and callosal hyperintensity on fluid-attenuated inversion recovery image, indicating diffuse axonal injury. FLAIR = fluid-attenuated inversion recovery; GRE = gradient echo.
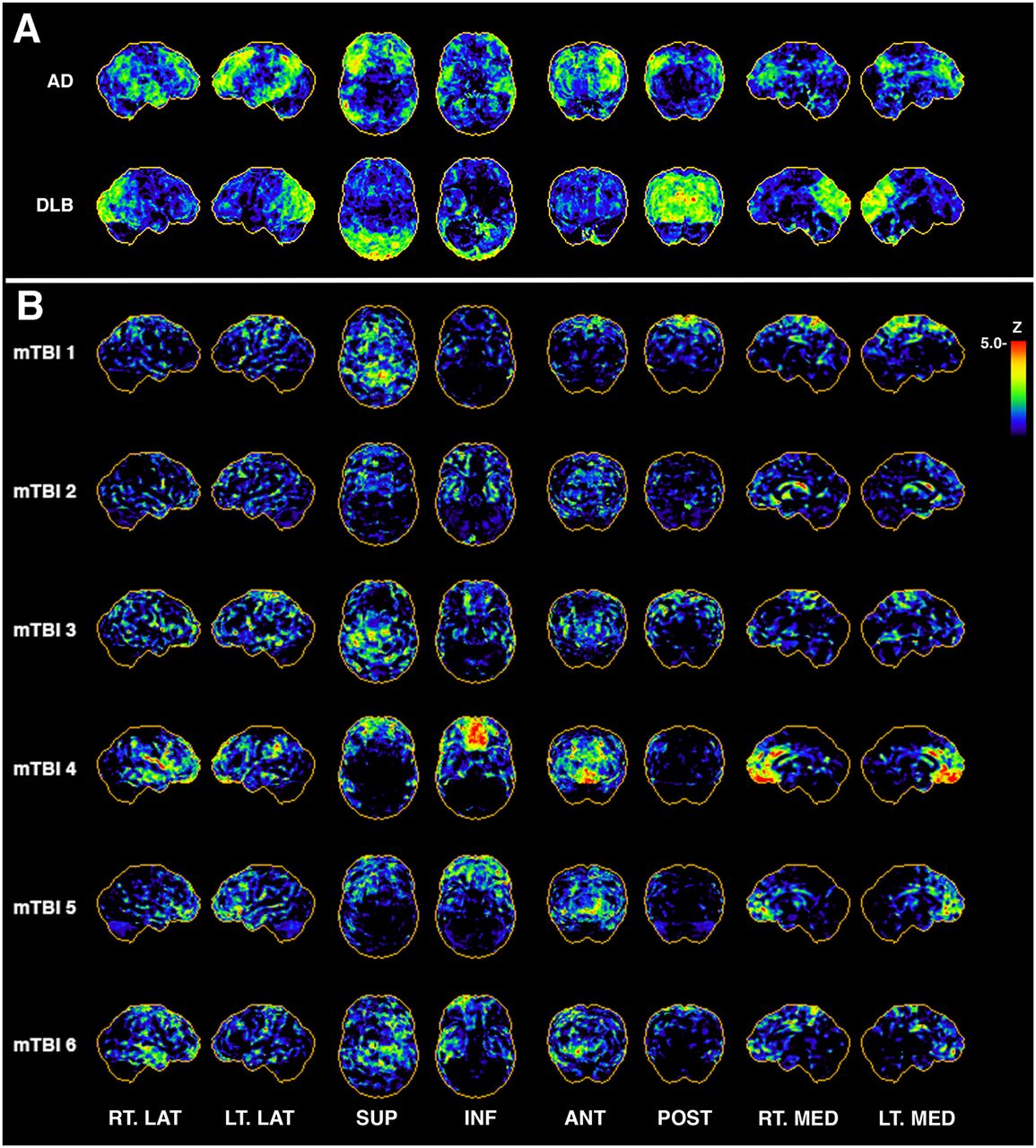
- FIGURE 2.
In patients with AD and dementia with Lewy bodies, typical hypometabolic patterns vs. randomly selected cases of repeated mTBI from exposure to blasts. (A) Representative 3-dimensional stereotactic surface projection (3D-SSP) z score map from patient clinically diagnosed with AD shows typical AD pattern of hypometabolism in posterior cingulate cortex and in parietal, temporal, and frontal lobes, with relative sparing of sensorimotor cortex. Diffuse Lewy body dementia is generally characterized by hypometabolism in occipital regions on 18F-FDG PET imaging. (B) Selected examples of 3D-SSP maps from veterans with multiple blast TBI exposures indicate pattern heterogeneity across subjects. Rows are single-subject 3D-SSP z score maps of hypometabolic voxels compared with reference database of age-matched community controls (n = 9). ANT = anterior; DLB = dementia with Lewy bodies; INF = inferior; LT. LAT = left lateral; LT. MED = left medial; POST = posterior; RT. LAT = right lateral; RT. MED = right medial; SUP = superior.
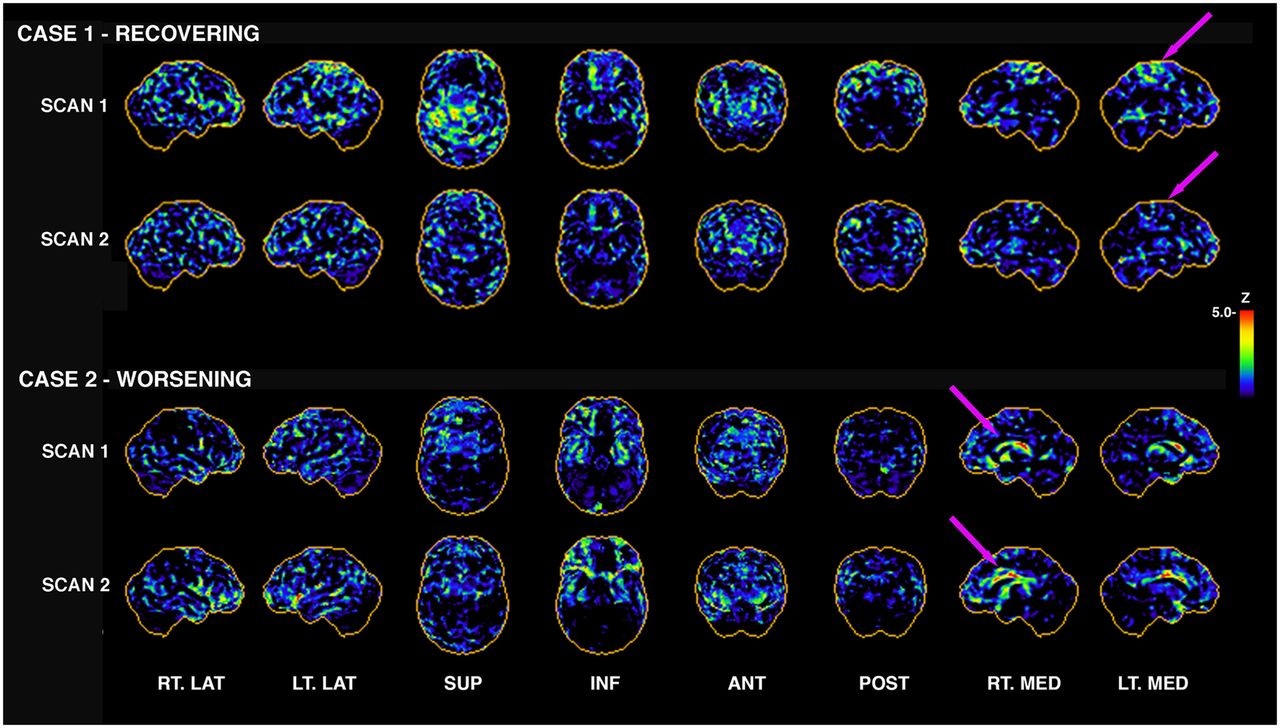
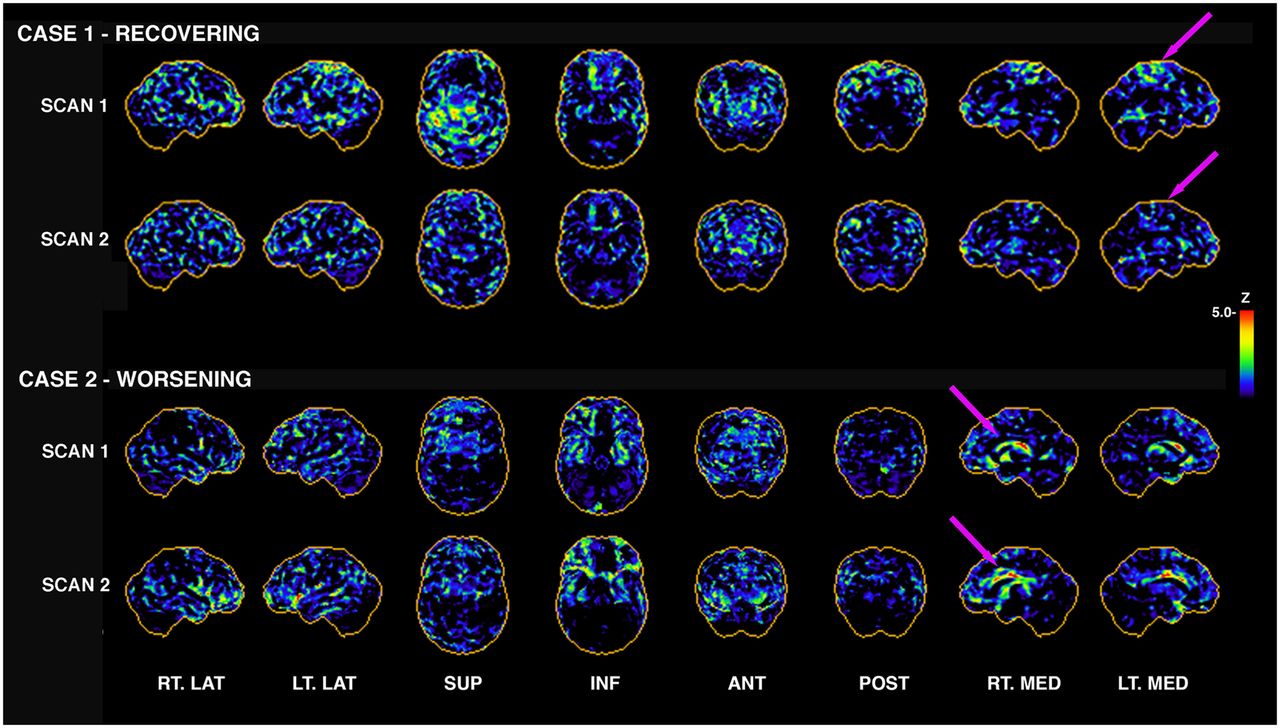
- FIGURE 3.
Longitudinal 18F-FDG PET in individuals with repeated mTBI from blast. Subjectively, one can appreciate that 18F-FDG PET from case 1 appears to be recovering; that is, there are fewer apparent hypometabolic pixels in scan 2 than in scan 1 (arrows indicate some regional differences). This subject had 44% decrease in number of hypometabolic voxels globally from scan 1 to scan 2. However case 2 indicates the opposite, with 46% increase in number of hypometabolic voxels globally. Not all cases are this clear-cut; some showed clear evidence of reorganization, with some regions increasing and others decreasing in total number of hypometabolic pixels (Fig. 4). Initial scans were 3–5 y after last blast, with 1–2 y interval between scans. ANT = anterior; INF = inferior; LT. LAT = left lateral; LT. MED = left medial; POST = posterior; RT. LAT = right lateral; RT. MED = right medial; SUP = superior.
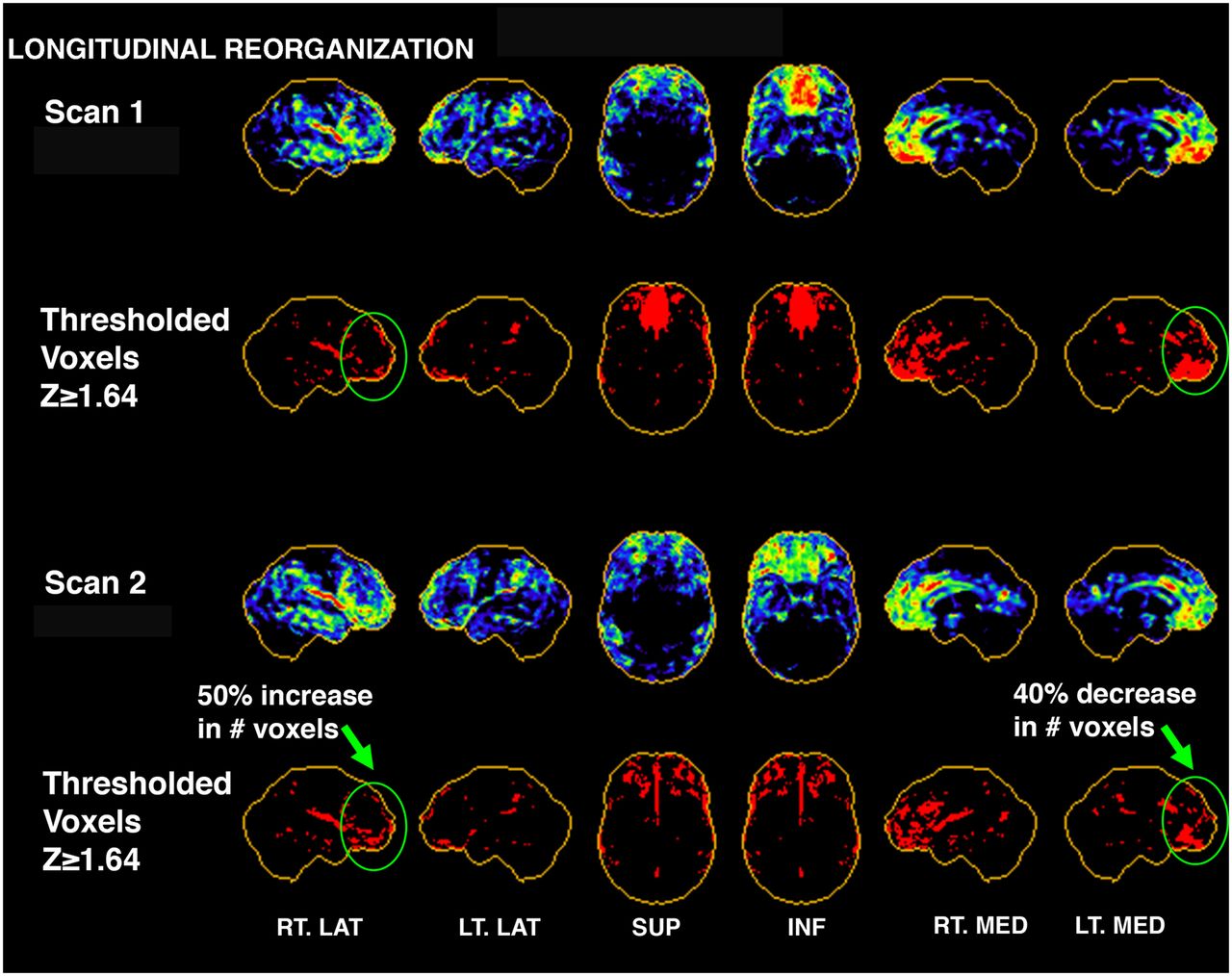
- FIGURE 4.
Three-dimensional stereotactic surface projection maps showing example of reorganization in single mTBI subject from scan 1 to scan 2. Casual visual inspection may conclude that subject’s scans have improved because severely hypometabolic region of inferior medial frontal lobe on scan 1 has improved subjectively by scan 2. This was supported in thresholding analysis (second and bottom rows), which indicated 40% decrease in number of voxels with z score ≥ 1.64 (hypometabolic voxels) for that region. However, analysis of 26 regions covering entire brain indicated that other regions, such as right lateral frontal region, actually became more hypometabolic (50% increase in hypometabolic voxels)—likely a result of reorganization and compensation over time. This subject also showed an 8% increase in hypometabolic voxels globally from scan 1 to scan 2. ANT = anterior; INF = inferior; LT. LAT = left lateral; LT. MED = left medial; POST = posterior; RT. LAT = right lateral; RT. MED = right medial; SUP = superior.
Tables
GCS Terminology Clinical definitions and background Most reported symptoms ≤8 Severe brain injury LOC > 6 h, PTA > 24 h Mobility problems, spasticity, weakness or paralysis, ataxia, sensory impairment, fatigue, speech difficulties, epilepsy 9–12 Moderate brain injury LOC between 15 min and 6 h or PTA for up to 24 h Tiredness; headaches; dizziness; difficulties with thinking, planning, organizing, memory, concentration, and word finding; irritability; anxiety 13–15 Mild brain injury (concussion) LOC < 15 min PTA < 1 h Dizziness, nausea, confusion, inability to process or retain information, sensitivity to light, vision distortion Subconcussive impacts Short LOC or no LOC, Short PTA, or no PTA Asymptomatic LOC = loss of consciousness; PTA = posttraumatic amnesia.
Adapted from “Advanced Trauma Life Support: Course for Physicians,” American College of Surgeons, 1993. There is no overall consensus on optimal definitions for brain injury with varying levels of severity. Most studies integrated in this review adhered to listed definitions.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}