


Editor’s note: SNMMI and the European Association of Nuclear Medicine periodically define new standards/guidelines for nuclear medicine practice to help advance the science of nuclear medicine and to improve the quality of service to patients. Newsline is pleased to publish this somewhat abbreviated version of this most recent guideline with wide relevance to many practitioners and patients. The complete version is available at: https://www.snmmi.org/ClinicalPractice/content.aspx?ItemNumber=6414 and includes relevant background and important liability statements and acknowledgments.
I. INTRODUCTION
Differentiated thyroid cancers (DTC) are slow-growing tumors with very low disease-specific mortality rates for local−regional disease (5-y survival: 99.9% for localized disease, 98.3% for regional metastatic disease). However, distant metastatic disease is associated with significantly worse prognosis (5-y survival: 54.9%) (1). Standard-of-care management for DTC includes risk-adapted surgery, postoperative 131I therapy, and thyroid hormone therapy. In uncommon cases of radioiodine-refractory tumors, additional therapy may include reoperative surgical intervention, external radiotherapy, and interventional radiology for treatment of locoregional metastases and multikinase or tyrosine kinase inhibitors for treatment of distant metastatic disease.
II. EPIDEMIOLOGY AND CLASSIFICATION
Thyroid neoplasms are the most common endocrine tumors, with an annual incidence of 8−9 cases/100,000 people, with substantial variability between and within populations. DTC accounts for >90% of cases, is more frequent in women, and has excellent specific mortality and prognosis in most cases. The rising incidence of thyroid cancer observed in the last 30 y is mainly due to detection of small (≤ 2 cm) tumors as a result of increased and improved imaging (2). However, larger tumors (>2 and >5 cm) have also increased in incidence; therefore, a concomitant true rise in thyroid cancer incidence is possible (3). DTC is biologically and functionally heterogeneous, with different molecular pathways impacting cancer cell biology. The BRAF V600E mutation is particularly associated with reduced expression of all thyroid-specific genes involved in iodine metabolism, resulting in variably decreased responsiveness to 131I therapy (4). For the main clinical and pathologic characteristics of DTC, see Table 1 (5).
Differentiated Thyroid Cancer: Clinical and Pathologic Characteristics (5)
III. DIAGNOSIS
Neck ultrasound (US), serum thyroid-stimulating hormone (TSH), and thyroid scintigraphy are used to select high-risk nodules for fine-needle aspiration (FNA) and filter out low-risk nodules from inappropriate additional procedures. Findings on US that are suspicious for thyroid cancer include hypoechogenicity, solid consistency, microcalcifications, irregular margins, extrathyroidal extension (ETE), and a taller-than-wide shape (6). Sonomorphologic nodule features have been used by several groups to produce a standardized risk assessment for thyroid malignancy, named the Thyroid Imaging Reporting and Data System (TIRADS) (7,8). In the absence of suspicious cervical lymph nodes, FNA is discouraged for nodules <1 cm, and the decision to aspirate larger nodules is guided by the TIRADS score in the context of nodule size. Cytologic findings are classified according to risk of malignancy using the Bethesda System for Reporting Thyroid Cytopathology (9). Certain cytologies are indeterminate, such as follicular neoplasm (or suspicious for follicular neoplasm), and the newly defined noninvasive follicular thyroid neoplasm with papillary-like nuclear features. In such cases, FNA can be complemented by assessment of specific molecular alterations (e.g., BRAF or TERT mutations, RET fusions), as well as molecular imaging with 99mTc-MIBI or 18F-FDG (10).
IV. THERAPY STRATEGIES
The current strategy for DTC management is a risk-stratified approach based on information from surgical histopathology, molecular markers, postoperative thyroglobulin (Tg) levels, and anatomic/functional imaging studies (6).
A. Surgical Treatment for DTC
(Near-) total thyroidectomy was traditionally performed in most DTC patients, with lobectomy reserved for cytologically indeterminate nodules or patients with unifocal micro-papillary thyroid cancer (PTC) <1 cm. Current American Thyroid Association (ATA) guidelines recommend lobectomy for patients with unifocal intrathyroidal low-risk DTC in the absence of additional risk factors (i.e., no clinical evidence of nodal metastases, cN0), although high-level evidence is lacking (6). Management of low-risk DTC between 2 and 4 cm is a topic of debate; although a lobectomy may be proposed, total thyroidectomy is still largely advised, especially in Europe (11). Active surveillance has been recommended as an alternative to lobectomy for unifocal micro-PTC with no extracapsular extension or lymph node metastases (12). The decision for active surveillance is based primarily on age-related risk of progression, individual surgical risk factors, and patient preference (13). In all other cases, total thyroidectomy remains the preferred surgical approach.
Cervical lymph nodal metastases occur in 20%–60% of patients with DTC, and this nodal involvement varies from clinically relevant macrometastasis to seemingly clinically irrelevant micrometastases (14,15). When lymph nodal metastases are diagnosed preoperatively, central and/or lateral neck compartment dissection reduces the risk of locoregional recurrence. Prophylactic central neck dissection may improve regional control for invasive tumors (T3–T4), but it is discouraged for low-risk DTC, because potentially associated morbidities (i.e., hypoparathyroidism and recurrent laryngeal nerve damage) are not justified by a significant clinical benefit (16). Preoperative neck US generally suffices to plan surgery; however, additional cross-sectional imaging (e.g, contrast-enhanced CT, MRI) is used in locally advanced disease to inform the surgical approach. When iodinated contrast media are administered for preoperative CT, sufficient time (i.e., 4–6 wk) for elimination of iodine load is required before performing radioiodine imaging and therapy.
PET/CT with 18F-FDG could be perfomed preoperatively in more aggressive DTC histotypes (i.e., poorly differentiated thyroid cancer or Hürthle cell carcinoma) and anaplastic thyroid cancer (17). After surgery, the risk of structural disease recurrence and/or persistence is assessed using the 3-tier (low, intermediate, high) stratification recommended by the ATA in 2009 and modified in 2015 (6), whereas the risk of mortality from thyroid cancer is estimated using the American Joint Commission on Cancer/TNM staging system (18).
B. Postoperative 131I Therapy
The goal of therapeutic 131I administration after total thyroidectomy is outlined based on standardized definitions as follows: remnant ablation, adjuvant treatment, or treatment of known disease (19,20). Upon integration of various parameters, including clinical/pathologic data and laboratory and imaging information, 131I therapy is administered for the following reasons: (1) to eliminate normal thyroid tissue remnant in low-risk patients, thereby ensuring undetectable or minimal serum Tg levels (in the absence of neoplastic tissue), which facilitates follow-up (remnant ablation); (2) to irradiate suspected but unproven sites of neoplastic cells in low-intermediate– and intermediate-risk patients as determined by histopathologic features, thereby reducing the risk of disease recurrence (adjuvant treatment); and (3) to treat persistent or recurrent disease in patients with demonstrated metastatic disease (treatment of known disease).
The impact of 131I therapy on clinical outcomes of thyroid cancer has been demonstrated in several large data series. An analysis of 2,936 DTC patients in the National Thyroid Cancer Therapy Cooperative Study Group (NTCTCS) reported improved overall survival (OS) and disease-specific survival in patients with advanced tumors and regional and/or distant metastatic disease who received postoperative 131I therapy (21). An updated analysis of 4,941 patients in the NTCTCS study with a median follow-up of 6 y (longest follow-up, 25 y) confirmed improved OS in stage III and IV patients and also demonstrated improved disease-free survival for stage II patients receiving 131I therapy (22). A metaanalysis of 31 patient-cohort studies regarding the effectiveness of 131I therapeutic administration demonstrated a statistically significant effect on improving clinical outcomes at 10 y, with decreased risk for locoregional recurrence (RR, 0.31; CI, 0.2–0.49) and an absolute risk reduction of 3% for distant metastatic disease (23). An analysis of the National Cancer Database comprising 21,870 intermediate-risk patients (mean follow-up, 6 y; longest follow-up, 14 y) demonstrated that adjuvant 131I treatment improved OS, both for younger (<45 y) and older (≥65 y) subsets of patients. Adjuvant 131I therapy was associated with a 29% reduction in risk of death for all patients (24). The beneficial effects of postoperative 131I therapy are most evident in patients with locoregionally advanced and distant metastatic disease (stages IVA, IVB, and IVC). An analysis of the National Cancer Database comprising 11,832 patients demonstrated that administration of 131I therapy was associated with significantly improved 5- and 10-y survival for both PTC and follicular thyroid cancer (FTC) patients, regardless of pathologic substage (stages IVA, IVB, or IVC), as follows: mortality rates in the PTC cohort (n = 10,796) at 5 and 10 y were 11% and 14%, respectively, in patients who received 131I therapy, compared to 22.7% and 25.5%, respectively, in patients who received none; mortality rates in the FTC cohort (n = 1,036) at 5 and 10 y were 29.2% and 36.8%, respectively, in patients who received 131I therapy, compared to 45.5% and 51%, respectively, in patients who received none (25). For patients with distant metastases, a delay of >6 mo in administration of 131I therapy is associated with decreased survival, demonstrated after a follow-up period of only 5–6 y (26).
C. Preparation for 131I Therapy
Evaluation with radioiodine scintigraphy and therapy is scheduled at a minimum of 4 wk after surgery, which allows time for patient preparation and for reaching postoperative Tg plateau levels, used as a marker for residual thyroid tissue and/or metastatic thyroid cancer after total thyroidectomy. Tg is synthesized exclusively in the thyroid follicular cells as a precursor of thyroid hormones, and manipulation of the thyroid gland during surgical resection releases significant Tg amounts in the systemic circulation. Tg is subsequently metabolized in the liver with a mean elimination half-life (Tg t1/2) of 65.2 h (27). Correct timing of serum sampling for Tg measurement in regard to surgery is important, and measurements should not be performed sooner than 25 d after total thyroidectomy to allow for clearance of the postsurgical Tg peak (10 × Tg t1/2) (27). Tg levels must always be interpreted in the context of concomitant TSH level (unstimulated vs. stimulated Tg) and type of TSH stimulation (endogenous vs. exogenous) (28). Tg antithyroglobulin antibodies (TgAb) need to be measured in conjunction with Tg in each serum sample provided for Tg testing. Every specimen needs TgAb testing to authenticate that the Tg measurement is not compromised by TgAb interference. When present, TgAb concentrations can be monitored as a surrogate tumor marker (29).
Patient preparation for optimal 131I uptake by residual thyroid tissue and metastatic disease includes 1–2 wk of low-iodine diet (LID) and adequate TSH stimulation (TSH ≥30 mIU/L measured 1–3 d prior to 131I administration) by either thyroid hormone withdrawal (THW) or recombinant human TSH (rhTSH) stimulation (30,31). However, a recent article showed that lower TSH levels may be sufficient for remnant ablation without influencing remnant ablation success rates (32). For childbearing females (12–50 y old) a negative pregnancy test is required within 72 h of 131I administration or prior to the first rhTSH injection (if used), unless the patient is status posthysterectomy or postmenopausal.
Dietary deprivation of stable iodine (127I) restricts consumption of iodine to <50 μg/d and is important for minimizing interference with 131I uptake. In a study of 120 patients (LID group, n = 59; control group, n = 61) LID preparation decreased 24-h urinary iodine excretion by 83% and increased radioiodine uptake in thyroid remnants by 65% (P < 0.001) as compared with controls. The efficacy of 131I treatment (assessed at 6 mo and defined by absent neck activity and Tg < 2 ng/mL) was also improved by LID: successful ablation was achieved in 65% of LID patients compared with 48% of patients in the control group (P < 0.001) (33).
Dietary iodine consumption varies widely, depending on ethnic culinary behavior, with reported average iodine intake of 195 μg/d for U.S., 469 μg/d for Korean, and 544 μg/d for Japanese individuals (34–36).
Patient compliance with LID can be confirmed by measurement of spot urinary iodine (U.S. reference range, 26–705 μg/L) or urinary iodine/creatinine ratio (I/Cr) (U.S. reference range, <584 μg/g); The World Health Organization defines iodine status based on urinary iodine concentrations as insufficient iodine intake, <99 μg/L; adequate iodine intake, 100–199 μg/L; iodine intake above requirements, 200–299 μg/L; and excessive iodine intake, ≥300 μg/L (37).
In preparation for 131I therapy the state of iodine deprivation induced by LID is considered adequate when spot urinary iodine is <100 μg/L and optimal when urinary iodine is <50 μg/L (or I/Cr is <50 μg/g) (38,39). A study of 101 patients comparing 2- and 4-wk LIDs showed no significant difference in urinary iodine levels, both periods resulting in optimal I/Cr for 131I therapeutic administration (i.e., <50 μg/g) (40). Moreover, depending on patients’ perceived difficulty with dietary iodine deprivation, compliance with LID may decrease as the duration of the diet is extended. Patients should be informed to avoid dietary supplements with high iodine content (e.g., iodine tablets [Iodoral], spirulina tablets, red dye food colorants). In addition, radiologic contrast agents and iodine-based antiseptics should be avoided for at least 4–6 wk prior to 131I therapy administration. A medication review should always be performed, and amiodarone usage should be replaced with a different antiarrhythmic drug followed by serial serum/urinary iodine measurements over 3–6 mo after amiodarone discontinuation to ascertain clearance of excessive iodine load before 131I treatment. Even when urinary iodine levels do not reach optimal values, the use of 131I therapy should be discussed in cases of advanced thyroid cancer. Table 2 contains dietary information regarding LID preparation (41).
Specific Dietary Instructions for Preparatory Low-Iodine Diet (Recommended Low-Iodine Diet Prior to Radioiodine Scintigraphy and Therapy [41])*
TSH is used for increasing sodium-iodide symporter (NIS) expression and function in metastatic lesions (and residual thyroid tissue), with the goal of increasing the diagnostic (Dx) sensitivity of 131I scintigraphy and radiation absorbed dose to target lesions. The 2 major approaches for TSH stimulation are:
(1) Endogenous TSH stimulation, obtained through thyroid hormone deprivation following total thyroidectomy, thus inducing a hypothyroid state that must be carefully explained to patients in order to avoid major adverse consequences. For example, patients must be informed about precautions regarding driving and/or restrictions on operating heavy machinery, because severe but reversible impairments in attention and reaction time have been observed (42).
The hypothyroid stimulation protocol (THW) has 2 variants employed worldwide in practice (although insufficient evidence is available to prefer one over the other): Levothyroxine (T4) withdrawal for 4 wk. This interval is determined by the T4 elimination half-life (T4 t1/2) of 7 d and the physiologic pituitary response to declining T4 concentrations. An acceptable variation involves repeated measurements of TSH during the second, third, and/or fourth wk of THW to expedite Dx radioiodine whole-body scanning (DxWBS) and/or 131I therapy whenever possible, timing it to TSH measurement of >30 mU/L in cases of metastatic disease (43). A level of unpredictability for scheduling imaging and/or therapeutic 131I administration is associated with this latter approach. Lower TSH levels may be sufficient for thyroid remnant ablation in low-risk patients, according to a single study that found no influence of TSH levels on postoperative 131I remnant ablation success (defined as stimulated Tg <1 ng/mL). The study involved 1,873 patients without distant metastases and a majority (∼80%) with stage I–II disease (of whom 15% had TSH <30 mU/L and demonstrated higher median Tg levels, suggestive of larger volumes of thyroid remnant tissue). Because NIS activity and, consequently, 131I uptake are TSH mediated in a dose- and time-dependent manner, the area under the curve obtained by the TSH level plotted against time may achieve sufficient stimulation to result in uptake of therapeutically effective 131I activities for ablation of thyroid tissue remnants that have high-constitutive NIS expression and function (32). However, the Guidelines Committee advises that this study’s findings cannot be extrapolated to high-risk patients and/or patients undergoing further 131I therapy for recurrent, persistent, or metastasized disease.
The second THW variant is levothyroxine/liothyronine (T4/T3) substitution for the first 2 wk, followed by discontinuation of T3 for 2 wk. This interval is based on T3 t1/2 of 0.75 d. In practice, T4 is stopped and replaced by T3 in a typical dose of 25 μg once or twice daily (depending on age and body weight). This regimen is well tolerated and has the advantage of minimizing hypothyroid symptoms (44).
TSH levels occasionally remain suboptimal for 131I therapy in patients with large thyroid remnants after surgery, in patients with limited pituitary functional reserve (e.g., history of head trauma, brain external-beam radiation, pituitary surgery, obesity, other comorbidities), or in patients with functional metastatic disease. Correlation of laboratory results with findings on postoperative Dx radioiodine scintigraphy is helpful for determining the etiology of suboptimal TSH elevation. This helps guide further steps in management, such as surgical resection for large thyroid remnants or bulky residual cervical metastatic disease, or dosimetry-guided 131I therapy for secretory distant metastases. For patients with limited pituitary functional reserve, it is advisable to proceed with administration of exogenous TSH stimulation (rhTSH injections) to avoid further delay in 131I therapy administration and limit hypothyroid symptoms (rhTSH augmentation protocol).
(2) For exogenous TSH stimulation: The patient continues T4 treatment and undergoes preparation with an LID. TSH elevation is obtained through administration of rhTSH (Thyrogen® stimulation protocol): a 0.9-mg rhTSH injection is administered intramuscularly on 2 consecutive d, followed by 131I therapy administration at 48–72 h (45). When Dx 131I scanning is performed as an integral part of 131I therapeutic protocols (theranostics), the tracer 131I activity is administered after the second rhTSH injection and the WBS scan is obtained 24 h later, followed by subsequent 131I therapy administration.
The choice of preparation method (THW vs. rhTSH) must be individualized for each patient. The balance of published data show that for normal thyroid tissue (i.e., thyroid remnant ablation), rhTSH and THW stimulation are equivalent, because normal thyroid tissue has constitutive high expression of highly functional NIS and does not require prolonged TSH stimulation for adequate 131I uptake and retention. However, metastatic thyroid cancer has lower density and poorer functionality of NIS; therefore, TSH elevation over time (area under the curve of TSH stimulation) is important to promote increased 131I uptake and retention in tumors (46,47). In the setting of metastatic disease, it is possible to use rhTSH stimulation on an off-label basis. However, the combination of THW preparation and dosimetry-guided 131I therapy is favored when clinically safe and the necessary expertise for dosimetry is available (45,48,49). Tumor vs. critical organ (e.g., bone marrow, lung) radiation absorbed dose (Gy) after rhTSH vs. THW-stimulation protocols needs further evaluation. Furthermore, no studies have yet reported relevant outcome measures (i.e., survival) with rhTSH and THW in patients with distant metastases.
The use of rhTSH is a more complex issue in the setting of adjuvant treatment, because this concept has been introduced only after studies employing rhTSH for remnant ablation were completed. As a result, there are no clear data in the literature allowing us to assess which of the 2 alternatives is better in the setting of adjuvant therapy separately from the setting of remnant ablation, especially with modern criteria for excellent response. However, rhTSH is registered for use for initial postoperative 131I therapy in patients up to and including N1 M0 disease. Therefore, in the case of adjuvant treatment, rhTSH and THW should both be considered in accordance with the individual medical characteristics of the case, economic feasibility, quality of life, and expected efficacy (20).
D. Postoperative Thyroglobulin Measurement
Although postoperative serum Tg measurement can provide valuable information with regard to the likelihood of achieving remission or having persistent or recurrent disease in response to an initial therapy, its predictive value regarding residual disease is significantly influenced by a wide variety of factors, as follows: the amount of residual thyroid cancer and/or thyroid remnants, TSH level at the time of Tg measurement, functional sensitivity of the Tg assay, time elapsed since total thyroidectomy, Tg cutoff used for analysis, and individual risk of having radioiodine-avid locoregional or distant metastasis (50). The fundamental role of Tg measurement in monitoring of DTC implies the need for high-quality Tg assays. A major problem that hampers accurate Tg measurement is the interference in the Tg assay by Tg antibodies (TgAb) and heterophile antibodies (HAb), resulting in under- or overestimation of the serum Tg concentration (51). Immunometric Tg assays are subject to a high-dose hook effect, leading to inappropriately normal or low Tg values in sera with very high Tg concentrations, which require dilution for accurate measurement (52). Absolute threshold values for Tg, whether the patient is prepared with THW or rhTSH, remain controversial. Several authors proposed that postoperative Tg values of about 10 ng/mL after THW and of 1 ng/mL after rhTSH stimulation achieve the best balance of sensitivity and specificity for predicting recurrent or persistent disease over time and poorer survival (45,53). Notably, because such results were obtained in patients treated with 131I following thyroidectomy, they cannot be translated to those patients treated by surgery alone and used to decide for/against postsurgical 131I administration. Indeed, some studies not only excluded patients with TgAb from analysis but also excluded patients showing evidence of extracervical metastases, introducing additional selection bias. Iodine-avid tissue with a corresponding undetectable stimulated serum Tg is detected in up to 20% of DTC patients by posttreatment WBS (PT-WBS). Moreover, up to 6% of such patients had confirmed locoregional or distant metastases in addition to thyroid tissue remnants (54,55). In a retrospective study, Matrone et al. (56) reported on a group of 505 low- to intermediate-risk DTC patients who had undergone total thyroidectomy and rhTSH-aided ablation with 1.1 GBq 131I. Just before ablation, a neck US was performed and Tg levels on thyroxine were measured using a high sensitive assay (i.e., functional sensitivity of 0.1 ng/mL). A planar PT-WBS was performed and compared with preablation basal Tg and US assessments. Among the main findings, 150 patients had Tg levels <0.1 ng/mL and 1 of 150 showed cervical persistence of disease; 287 patients had Tg levels between 0.1 and 1.0 ng/mL, 15 of whom had nodal or distant metastases; and 68 patients had Tg levels exceeding 1.0 ng/mL, 11 of whom had neck metastases. Notably, in the 3 patients with lung metastases, basal Tg levels were 0.11, 0.12, and 0.94 ng/mL. A basal Tg level of 0.75 ng/mL was measured in 1 additional case of bone metastasis. This article submitted further evidence that basal Tg < 1 ng/mL cannot be used to rule out the presence of distant metastases; 2 of the 4 patients with distant metastases had Tg levels of 0.11 and 0.12 ng/mL (56).
Recently, Schlumberger et al. (57) reported 5-y outcomes of ESTIMABL1, a randomized trial comparing 4 strategies of 131I administration following thyroidectomy in low-risk thyroid cancer. In this study, the rate of patients with persistent structural disease after 131I ablation was similar in 3 subgroups of stimulated Tg ranges (i.e., ≤1, >1–≤5, and > 5–<10 ng/mL) (58). In summary, with regard to decision-making on the need for postoperative 131I administration, it appears that the serum Tg value is more helpful in identifying patients for whom the administered 131I activity should be higher, rather than in identifying patients who do not require 131I therapy.
E. Radioiodine Therapy Planning
An important goal of 131I therapy is individualized treatment that maximizes benefit and reduces risk for each patient who belongs to a risk category associated with improved outcomes after 131I therapy. There are 2 approaches to 131I therapy delivery: the approach integrating functional imaging information obtained with postoperative preablation Dx radioiodine (123I, 131I, or 124I) scans in the management algorithm (i.e., functional imaging-guided approach; theranostics) and the approach based on clinical–pathologic factors and institutional protocols (i.e., risk-adapted approach). The approach chosen depends on local factors, including quality of surgery, availability of and expertise with various imaging modalities, and physician as well as patient preferences.
F. Management and Integration of Functional Diagnostic Radioiodine Imaging
This theranostic approach to 131I administration involves acquisition of a postoperative Dx radioiodine (123I, 131I, or 124I) scan for planning 131I therapy. DxWBS is performed with the intent of identifying and localizing regional and distant metastatic disease and for evaluating the capacity of metastatic deposits to concentrate 131I. Depending on institutional protocols, findings on DxWBS may alter management, such as providing guidance for additional surgery or altering the prescribed 131I therapy, either by adjusting empiric 131I activity or by performing dosimetry calculations for determining the maximum tolerated therapeutic 131I activity (MTA) for treatment of distant metastatic disease. Also, unnecessary 131I therapy may be avoided if DxWBS finds no evidence of residual thyroid tissue or metastatic disease and the stimulated Tg is <1 ng/mL in the absence of interfering TgAb (59). Information acquired from DxWBS may also lead to additional functional metabolic imaging with 18F-FDG PET/CT when non-iodine–avid metastatic disease is suspected (based on Tg elevation out of proportion to findings on DxWBS). Wherever available, it is preferable for postoperative DxWBS to be performed using integrated multimodality imaging (i.e., SPECT/CT).
DxWBS with or without SPECT/CT may detect metastases in normal-size cervical lymph nodes (not appreciated on postoperative neck US), may identify pulmonary micrometastases (which are too small to be detected on routine chest x-ray and may remain undetected on CT), and may diagnose bone metastases at an early stage before cortical disruption is visible on bone x-rays or CT. Because 131I therapy is most effective for smaller metastatic deposits, early identification of regional and distant metastases is most important for successful therapy (60,61).
Clinical experience with Dx 123I scans demonstrated their usefulness in thyroid cancer management: preablation 123I WBS provided additional critical information in 25% of 122 patients, by revealing unsuspected regional or distant metastases and thus guiding administration of higher 131I therapeutic activities or revealing unexpected large thyroid remnants (62). In a cohort of 152 consecutive patients referred for postoperative 131I ablative therapy, the information provided by Dx 123I WBS led to a change in prescribed therapeutic 131I activity in 49% of cases compared to the recommended 131I activities based on surgical pathology alone (63). In a study based on review of 355 Dx radioiodine scans (after administration of 37–148 MBq [1–4 mCi] of either 123I or 131I) the imaging findings altered management in 29% of cases (64). Similar conclusions have been reached by other investigators who demonstrated that the information obtained from Dx 131I WBS changed the prescribed therapeutic 131I activity in 58% of cases (65).
A study comparing sensitivity for disease detection for Dx 74–185 MBq (2–5 mCi) 123I WBS versus 111–185 MBq (3–5 mCi) 131I WBS (both performed after THW protocol) demonstrated that, although 123I is adequate for imaging residual thyroid tissue, it appears to be less sensitive than 131I for imaging thyroid cancer metastases: 123I missed metastases shown by 131I in the neck, mediastinum, lungs, and bone. No lesion was better seen with 123I than with 131I (66). Other authors also found Dx 123I WBS to be insensitive for metastatic disease detection and attributed this finding to the short half-life of 123I (13 h), limiting imaging to no later than 24 h postinjection, which is too short for optimizing tracer tumor uptake (67). In addition to the radioiodine isotope used, the preparation protocol (THW vs. rhTSH stimulation) also has an impact on the Dx sensitivity of DxWBS for disease detection: across 2 phase 3 clinical trials enrolling 358 patients, rhTSH-stimulated DxWBS failed to detect remnant and/or cancer localized to the thyroid bed in 16% of patients in whom it was detected by a DxWBS obtained after THW. In addition, the rhTSH-stimulated DxWBS failed to detect metastatic disease in 24% of patients in whom it was detected by a THW DxWBS (68–70).
In a group of 320 thyroid cancer patients referred for postoperative 131I therapy, Dx 131I WBS with SPECT/CT imaging obtained after THW protocol detected regional metastases in 35% of patients and distant metastases in 8% of patients. This information changed staging in 4% of younger and 25% of older patients (71). Both imaging data and stimulated Tg levels acquired at the time of Dx 131I WBS were consequential for 131I therapy planning, providing information that changed clinical management in 29% of patients compared to a management strategy based on clinical and surgical pathology information alone (72).
The benefits of integrating Dx 131I WBS in the management algorithm of intermediate- and high-risk thyroid cancer for guiding 131I therapeutic administration have been demonstrated in a group of 350 patients evaluated to assess therapy response with a median follow-up of 3 y after primary treatment strategy (surgery and postoperative 131I therapy): complete response (CR) to therapy was achieved in 88% patients with locoregional disease and in 42% patients with distant metastases after a single 131I therapeutic administration (73). Further studies for evaluating long-term outcomes need to be performed.
Depending on the type of patient preparation, Dx radioiodine (123I or 131I) activities such as 37–74 MBq (1–2 mCi) for THW protocols and 110–148 MBq (3–4 mCi) for rhTSH-stimulation protocols are frequently used (39). The higher tracer activity (3–4 mCi) employed for rhTSH-stimulation protocols is to compensate for the competitive inhibition exerted by the iodine content of T4 (levothyroxine) on the uptake of radioiodine (131I or 123I) in thyroid tissue or metastatic lesions (74). T4 contains 63.5% iodine by molecular weight. The interference of T4 stable iodine content on radioiodine uptake is not surprising if we consider that the amount of iodine in 1.1 GBq (30 mCi) is only 5 µg, as compared to 50 µg stable iodine content in a daily dose of T4 (75). The dilution of radioiodine with nonradioactive iodine from any source may degrade WBS image quality and reduce the effectiveness of 131I therapy. Replacement of levothyroxine with liothyronine (T3) during the preparation period for rhTSH-stimulation protocols has been proposed for decreasing the dilution effect of nonradioactive iodine on the uptake of radioiodine (74). T3 has lower iodine content per molecule (only 56.6% of T4 iodine content) and exerts an equivalent biologic effect by administration of ¼ of the necessary T4 dose (76). In addition to an LID, this therapeutic interchange from T4 to T3 during the preparatory period for rhTSH-stimulation protocol resulted in a further decrease in 24-h urinary iodine excretion by 56% as compared to T4 treatment (74).
Optimization of imaging acquisition parameters and current SPECT/CT gamma camera technology permit good quality visualization of distant metastatic disease using 37 MBq (1 mCi) 131I Dx activity (71,72,77,78).
In all cases, 131I therapy should be followed by acquisition of PT-WBS to determine therapeutic 131I localization, which is routinely used to complete postoperative staging. However, the day to perform the PT-WBS after therapeutic 131I administration remains controversial, ranging from 2–10 d (79). PT-WBS acquisition on 2 separate days may be valuable, as demonstrated by Salvatori et al. (80) in a group of 134 patients who underwent both early (at 3 d) and delayed (at 7 d) scans: 80.5% of detected lesions were concordant on both early and delayed scans; however, 7.5% of lesions were detected only on the early scans, whereas 12% of lesions were detected only on the delayed scans. By performing both early (at 3–6 d) and delayed (at 10–11 d) PT-WBS, Hung et al. (81) reported that 28% of nodal metastases, 17% of lung metastases, and 16% of bone metastases were visible only on the early scans. This is consistent with the observation that 131I therapeutic activities produce destructive cellular effects with resultant increased rates of 131I loss from the tissue; this accelerated tissue 131I loss after treatment may account for discrepancies reported between DxWBS and delayed PT-WBS in earlier studies, which has been interpreted as “stunning,” as well as differences observed between early and delayed PT-WBS (82). However, delayed PT-WBS acquisition provides the advantage of increased contrast resolution due to time-dependent 131I clearance from normal tissues. Chong et al. (83) reported in a group of 52 patients that 22% of lung metastases and 33% of bone metastases were visible only on the delayed PT-WBS (obtained at 7 d). Similarly, Kodani et al. (84) reported in a group of 24 patients that 29% of lung metastases and 20% of bone metastases were visible only on the delayed PT-WBS (obtained at 7–9 d).
Hybrid imaging with SPECT/CT improves the accuracy of PT-WBS and should be done whenever possible. A systematic review of 14 original research articles describing the incremental value of 131I SPECT/CT demonstrated significant clinical benefit in terms of staging, risk stratification, alteration of management, and/or follow-up of DTC (85). This is especially important when DxWBS is not performed or when PT-WBS shows additional foci of activity as compared to DxWBS (86). A high level of concordance between DxWBS and PT-WBS findings has been demonstrated in 2 large single-institution data series from Stanford University (98% concordance in a group of 280 patients) and the University of Michigan (92% concordance in a group of 303 patients) (71,87). In summary, DxWBS is valuable for 131I therapy planning in the paradigm of thyroid cancer theranostics (88).
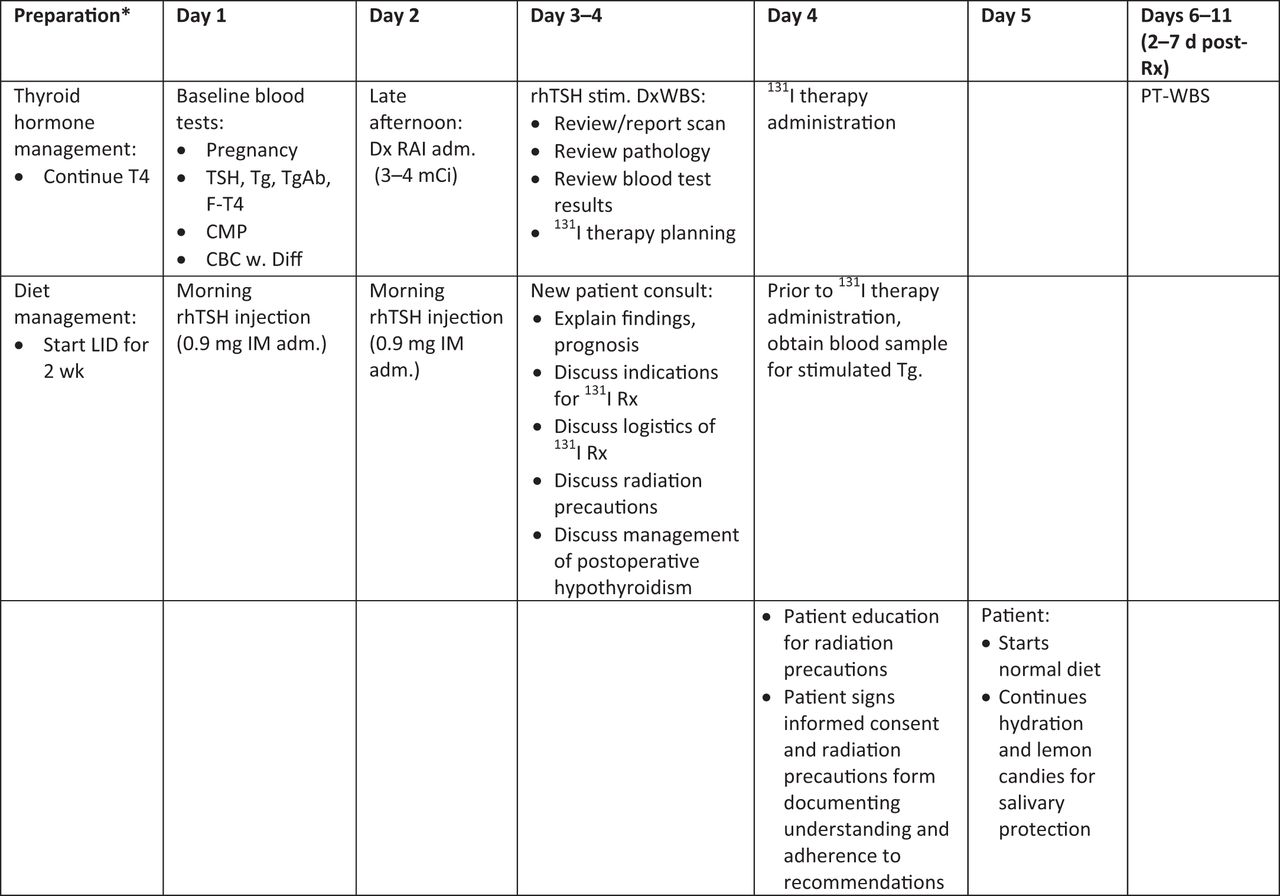
DxWBS scintigraphy performed in follow-up evaluation after initial postoperative 131I administration is important to (1) establish a new baseline after postoperative 131I therapy (89); (2) determine interval response to 131I treatment; and (3) assess the patient’s thyroid cancer status. Along with basal and stimulated-Tg testing and cross-sectional anatomic imaging, the results of follow-up DxWBS contribute to dynamic risk restratification, which is usually performed at 6–12 mo after initial treatment strategy (surgery and postoperative 131I therapy). For patients with rising Tg levels, DxWBS and PET/CT evaluation can be scheduled sequentially to assess for recurrent and/or metastatic disease and evaluate tumor biologic behavior for determining whether the patient would benefit from additional 131I therapy (73). Of importance, a recent report examining the results of a large Surveillance, Epidemiology, and End Results Program database (28,220 patients diagnosed with DTC between 1998 and 2011) showed that follow-up DxWBS performed after primary treatment of DTC are the only imaging studies associated with improved disease-specific survival, demonstrating the clinical benefit of 131I theranostics for DTC management (90). Figures 1 and 2 provide sample protocols for integration of DxWBS evaluation, 131I therapy delivery, and PT-WBS imaging after THW and after rhTSH stimulation, respectively. Figures 3 and 4 present sample protocols for dosimetry-guided radioiodine theranostics after THW and after rhTSH stimulation, respectively.

Sample protocol for 131I theranostics after thyroid hormone withdrawal (THW). *Initial consultation is recommended to discuss preparation protocol with patient and family and explain logistics and expectations of 131I therapy and radiation precautions. RAI = radioiodine; T4 = levothyroxine; T3 = liothyronine; Dx RAI adm. = diagnostic radioiodine activity administration; DxWBS = diagnostic radioiodine whole-body scan; CMP = comprehensive metabolic panel; CBC = complete blood count; RAI Rx = 131I therapy; PT-WBS = posttherapy 131I whole-body scan; rhTSH = recombinant human TSH, Thyrogen®; LID = 2 wk of low-iodine diet; TSH = thyroid-stimulating hormone; F-T4 = free thyroxine; Tg = thyroglobulin.
Sample protocol for 131I theranostics after rhTSH-stimulation. *Initial consultation is recommended to discuss preparation protocol with patient and family and explain logistics and expectations of 131I therapy and radiation precautions. RAI = radioiodine; T4 = levothyroxine; CMP = comprehensive metabolic panel; CBC = complete blood count; Dx RAI adm. = diagnostic radioiodine activity administration; Dx WBS = diagnostic radioiodine whole-body scan; RAI Rx = 131I therapy; PT-WBS = posttherapy 131I whole-body scan; THW = stimulation protocol by thyroid hormone withdrawal; rhTSH = recombinant human TSH; LID = 2 wk of low-iodine diet; TSH = thyroid stimulating hormone; F-T4 = free thyroxine; Tg = thyroglobulin.

Sample protocol for 131I theranostics with dosimetry after thyroid hormone withdrawal (THW). *Initial consultation is recommended to discuss preparation protocol with patient and family and explain logistics and expectations of 131I therapy and radiation precautions. RAI = radioiodine; T4 = levothyroxine; T3 = liothyronine; CMP = comprehensive metabolic panel; CBC = complete blood count; Dx RAI adm. = diagnostic radioiodine (123I, 131I) activity administration; DxWBS = diagnostic radioiodine whole-body scan; 131I Rx = 131I therapy; PT-WBS = posttherapy 131I whole-body scan; THW = stimulation protocol by thyroid hormone withdrawal; LID = 2 wk of low-iodine diet; TSH = thyroid stimulating hormone; F-T4 = free thyroxine; Tg = thyroglobulin.
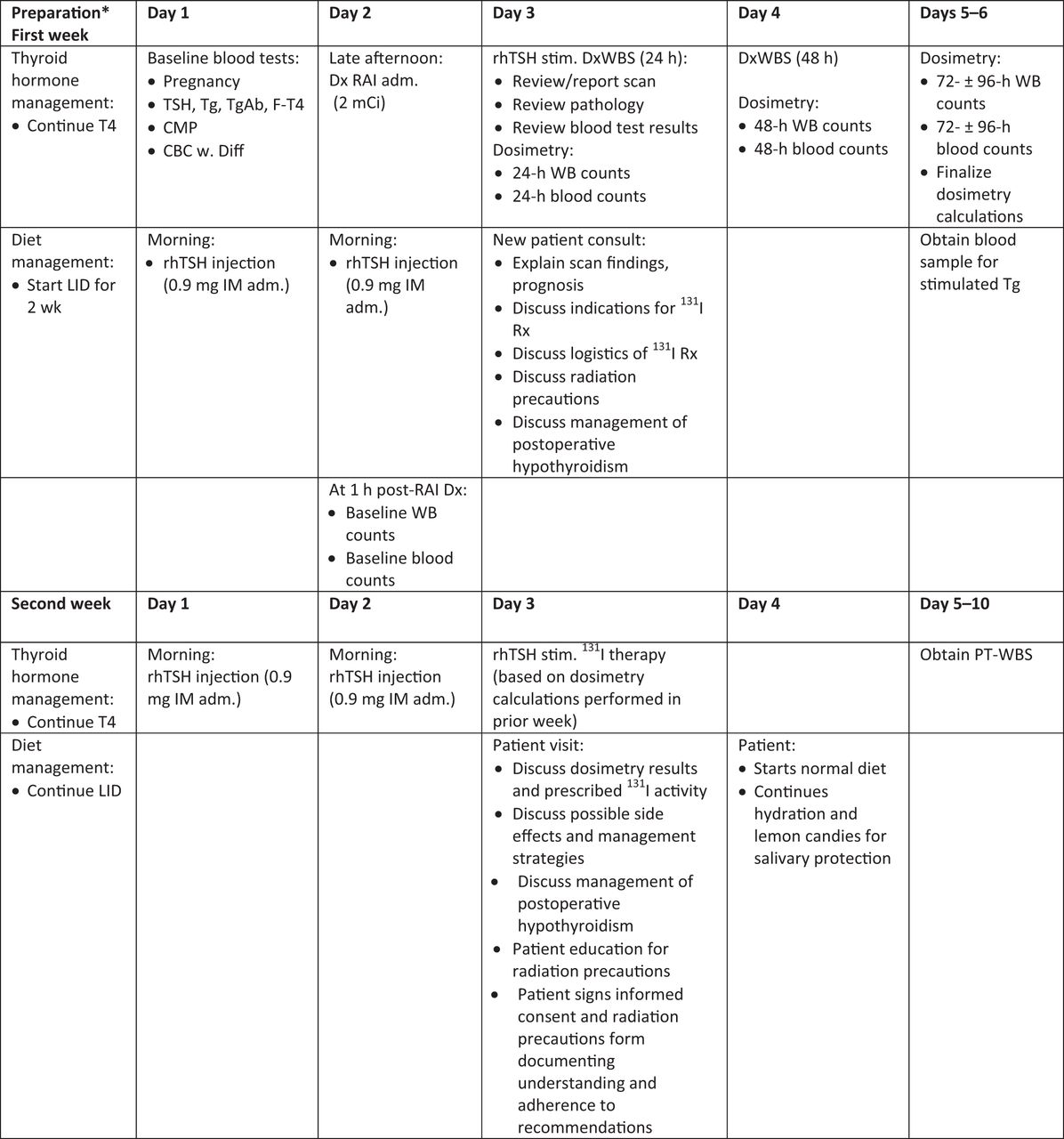
Sample protocol for 131I theranostics with dosimetry after rhTSH-stimulation. *Initial consultation is recommended to discuss preparation protocol with patient and family and explain logistics and expectations of 131I therapy and radiation precautions. RAI = radioiodine; T4 = levothyroxine; CMP = comprehensive metabolic panel; CBC = complete blood count; Dx RAI adm. = diagnostic radioiodine activity administration; DxWBS = diagnostic radioiodine whole-body scan; RAI Rx = 131I therapy; PT-WBS = posttherapy 131I whole-body scan; THW = stimulation protocol by thyroid hormone withdrawal; rhTSH = recombinant human TSH; LID = 2 wk of low-iodine diet; TSH = thyroid stimulating hormone; F-T4 = free thyroxine; Tg = thyroglobulin.
G. Risk-Based Management Followed by Posttherapy 131I Scans with Diagnostic Intent
The risk-based approach is generally used for thyroid remnant ablation and for adjuvant 131I treatment. Empiric activity selection is the most commonly used approach in advanced DTC, in which the nuclear medicine physician chooses an activity based on convention, availability, experience with various imaging modalities, and patient-related parameters. With this therapeutic approach patients are most commonly given activities of 1.1 GBq (30 mCi), 1.85 GBq (50 mCi), 3.7GBq (100 mCi), 5.6 GBq (150 mCi), or 7.4 GBq (200 mCi) (91). Although there are theoretical disadvantages of this approach compared to dosimetric strategy in the treatment of locoregional and metastatic disease, no recommendation can be made for the superiority of 1 method of 131I application over another. However, it is essential to emphasize that the MTA can be exceeded in patients undergoing empiric 131I therapy escalation for treatment of advanced DTC, which may cause acute dose-related toxicities. Likewise, patients may be undertreated with this conventional therapeutic approach (92). (The full discussion on the limitations of the empiric approach as compared to the dosimetric strategy for treatment of metastatic DTC is available online in the full version of the guideline.)
Administration of empiric 131I activities of ≤3.7 GBq (≤100 mCi) is generally not recommended for treatment of locoregionally advanced and/or distant metastatic DTC, as these patients require escalation of 131I therapeutic activity and an individualized treatment approach. Particularly in the setting of diffuse iodine-avid distant metastatic disease, the attending physician or managing medical team should consider either performing dosimetry or referring the patient to a site that performs dosimetry-guided 131I therapy, for 2 reasons: (1) to identify those patients who would have a higher likelihood of side effects if ≥5.6–7.4 GBq (150–200 mCi) 131I therapeutic activity is administered; and/or (2) to administer the highest safe 131I therapeutic activity (MTA) for maximizing tumor radiation absorbed dose. Current evidence suggests that dosimetry-based high-activity 131I therapy in patients with advanced DTC may be more effective in improving outcomes and survival (93,94).
Each 131I therapy should be followed by 131I PT-WBS. Distinct advantages are offered by postsurgery 131I activity administration for all risk stratification categories and irrespective of postoperative Tg levels, confirming the role of PT-WBS for early detection and treatment of locoregional and distant metastatic disease. Park et al. (55) demonstrated in a large cohort of 824 DTC patients who underwent 131I therapy after T4 withdrawal protocol that 52 (6.3%) had functioning metastases identified on PT-WBS scans despite stimulated Tg ≤ 2 ng/mL in the absence of interfering anti-Tg antibodies (TgAbs). A low stimulated Tg ≤ 2 ng/mL did not exclude the presence of distant metastases, because in this group 7 patients (13.5%) had pulmonary and osseous metastases, whereas the remaining 45 (86.5%) had cervical/mediastinal lymph nodal metastases. In a recent study by Campenni et al. (95) in 570 low- and low-intermediate–risk DTC patients (pT1–pT3) PT-WBS scans with SPECT/CT demonstrated metastases in 82 patients (14.4%), of whom 73 (90.2%) had postsurgical nonstimulated Tg ≤ 1 ng/mL; furthermore, in 44 patients (54%) stimulated Tg remained ≤ 1 ng/mL, despite the presence of metastases on PT-WBS scans. Therefore, postsurgical nonstimulated Tg levels cannot be used independently in deciding whether to pursue therapeutic 131I administration, mainly in patients assigned as low-risk based solely on surgical pathology information. The body of published evidence regarding the outcome of postoperative 131I ablation in low-risk patients (which in current terminology would encompass both remnant ablation and adjuvant treatment) demonstrates that these patients can be fully reassured by a complete treatment response and would not require Tg stimulation testing or periodic neck US examinations during long-term follow-up (96). In fact, cohorts in which all patients, including those at low risk with nonmetastasized, nonmicrocarcinoma disease, received 131I therapy after surgery demonstrated that life expectancy is normal for >85% of patients; only patients with stage IV disease at diagnosis have a reduction in life expectancy (97,98). We are not aware of similar data available for individualized or more restrictive 131I prescription strategies.
In conclusion, postoperative Tg levels are helpful in identifying high-risk patients who require higher 131I activity but cannot be used for ruling out 131I therapy. Omission of the procedure exposes the patients to the risk of late diagnosis of residual disease (99,100). Finally, early reassurance and more reliable follow-up are only possible when patients had received total thyroidectomy followed by postoperative 131I therapy.
H. Determining the Prescribed Therapeutic 131I Activity
Current practice guidelines recommend routine 131I adjuvant therapy for patients with intermediate to high risk of recurrence (although there are some differences concerning intermediate-risk disease) and avoiding routine 131I therapy for patients with a small (≤1 cm) intrathyroidal DTC and no evidence of locoregional or distant metastatic spread (6,91). However, 131I therapy for other low-risk DTC patients (i.e., pT1b–T2) remains controversial. The various iterations of the ATA guidelines advised against the systematic use of 131I in these patients (6), whereas in 2008 the European Association of Nuclear Medicine (EANM) suggested that 131I therapy is helpful, citing the lack of prospective data showing that surveillance without ablation is noninferior to 131I administration (101). Indeed, ATA, EANM, SNMMI, and the European Thyroid Association recently published a joint statement acknowledging the absence of high-quality evidence either for or against the postoperative use of 131I in low-risk patients (20).
The decision for 131I therapy and the prescribed 131I activity depend on the goal of 131I therapy as determined by estimated risk for persistent/recurrent disease. Table 3 lists suggested 131I treatment activities in the context of therapeutic intent:
Suggested Framework for 131I Therapy
Thyroid remnant ablation in low-risk patients is typically performed with low 131I activity (e.g., 1.1–1.85 GBq [30–50 mCi]), based on the preponderance of published evidence demonstrating equal effectiveness as compared with higher 131I activities, with lower rates of adverse events (102–138). The Federal Drug Administration (FDA) approved the used of rhTSH (Thyrogen®; Genzyme Corp., Cambridge, MA) in combination with 3.7 GBq (100 mCi) 131I for remnant ablation in December 2007 (68,139,140).
Adjuvant 131I therapy is performed with 1.85–3.7 GBq (50–100 mCi), with some institutions extending this range to 5.6 GBq (150 mCi); there are no comparison data regarding the effectiveness of 3.7 GBq (100 mCi) vs. 5.6 GBq (150 mCi) for adjuvant treatment, although current guidelines advise that the risk for 131I toxicity increases with therapeutic activity escalation (141).
Treatment of known disease is performed with 3.7–5.6 GBq (100–150 mCi) for small-volume locoregional disease and 5.6–7.4 GBq (150–200 mCi) 131I for treatment of advanced locoregional disease and/or small-volume distant metastatic disease. Identification of iodine-avid diffuse metastatic disease may lead to escalation of prescribed therapeutic 131I activity to ≥7.4 GBq (200 mCi), guided by dosimetry calculations (73,142,143).
A special circumstance is presented by the use of 131I therapy (3.7 GBq [100 mCi]) for ablation of a remaining thyroid lobe after lobectomy/hemithyroidectomy as an alternative to completion thyroidectomy (144–146). Current guidelines propose lobectomy for patients deemed as at low risk for recurrence; however, if the pathology demonstrates a higher risk tumor, then completion thyroidectomy with resection of the contralateral thyroid lobe is recommended, with the goal of facilitating postoperative 131I therapy and long-term surveillance. Therapeutic 131I administration as a substitute for completion thyroidectomy is not recommended routinely (6). However, it can be used to eliminate the residual thyroid lobe in highly selected cases, such as patients who had experienced complications during initial surgery (e.g., recurrent laryngeal nerve paralysis), for whom completion thyroidectomy is contraindicated due to other comorbidities, or for patients who decline additional surgery. There are limited data regarding the long-term outcomes of this approach. The data suggest similar clinical outcomes, with a slightly higher proportion of patients with persistently detectable Tg. In a randomized controlled equivalence trial of 136 low-risk DTC patients treated with lobectomy, which compared low vs. high 131I activities in achieving successful ablation of the remaining lobe, the remnant ablation success rate was significantly higher (75% success rate) using 3.7 GBq (100 mCi) as compared with 1.1 GBq (30 mCi) (54% ablation success rate). Mild-to-moderate short-term neck pain was more frequently reported in the high-activity group (66%) than in the low-activity group (51%). Prednisone treatment for neck pain was used more frequently in the high-activity group (36%) than in the low-activity group (147).
I. Dosimetry-Guided 131I Therapy
There are 2 approaches for individualization of 131I therapy based on dosimetry calculations: (1) blood or bone marrow dosimetry–based methods, primarily targeting safety; and (2) lesion dosimetry–based methods, primarily targeting efficacy. Of these, the classic blood-based method is more widely used and permits calculation of the MTA that can be administered to an individual patient without risk of severe hematopoietic toxicity. (The complete online version of the guideline contains a detailed discussion of blood- and lesion-based dosimetry methods.)
J. Radioiodine Toxicity: Acute and Chronic Side Effects of Radioiodine Therapy and Possible Risk of Subsequent Primary Malignancies
Therapeutic 131I administration carries a risk for acute and chronic side effects and a small risk of possible subsequent primary malignancies. (The complete online version of the guideline contains a detailed discussion of these risks.)
V. THYROID HORMONE THERAPY AND SURVEILLANCE STRATEGY
After 131I therapy patients receive T4 therapy with the goal of TSH suppression, depending on patients’ risk stratification (0.1–0.3 mU/L for patients with regional metastases and <0.1 mU/L for patients with distant metastases) (6). A recent consensus statement by the American, British, and European thyroid associations recommends that T4/T3 therapy should be considered under specific circumstances and for selected patients, especially hypothyroid patients without residual thyroid function and those with persistent symptoms of impaired well-being and cognitive dysfunction despite adequate T4 doses (148).
Serum Tg measurement is employed for monitoring DTC status after primary therapy. However, the usefulness of following Tg is limited in patients who have TgAbs because the serum Tg levels can be underestimated when using immunometric assays (52). In these patients the trend of TgAb levels over time can serve as a surrogate tumor marker (29). Immune memory in patients with a background of thyroid autoimmune disease accounts for the slow decline of TgAb levels after initial DTC treatment, and levels should be interpreted with caution for at least 6 mo after 131I therapy (51). During long-term surveillance the TSH suppression target is adjusted, taking into consideration the outcome of primary therapy according to dynamic risk restratification. In patients with a structural incomplete response serum TSH is maintained <0.1 mIU/L indefinitely, while target values of 0.5–2 and 0.1–0.5 mIU/L are adopted in low- to intermediate-risk and in high-risk patients, respectively, with excellent response. Finally, TSH target values of 0.1–0.5 mIU/L are also suggested when post-therapy Tg remains detectable with evidence of structural disease (6).
VI. RESPONSE ASSESSMENT AFTER PRIMARY THERAPY
Dynamic risk restratification consists of reassignment of recurrence risk based on response to initial treatment, which is predictive of long-term clinical outcomes (6). This is performed during the first 2 y of follow-up after initial therapy (total thyroidectomy followed by 131I therapy) and involves basal and stimulated Tg testing and imaging reevaluation. US is a reliable method for detection of locoregional persistent or recurrent DTC (i.e., thyroid bed and cervical lymph nodes). However, the probability of false-positive results leading to unnecessary and expensive additional procedures is far from negligible. Accordingly, the use of US should be limited (particularly in low-risk DTC) and, in the absence of TgAbs, reserved only for patients with unstimulated serum Tg levels ≥1 ng/mL (96). US-guided FNA biopsy with Tg determination in the fluid aspirate is used for Dx confirmation of residual disease in suspicious-appearing cervical lymph nodes identified on anatomic imaging.
In combination with Tg measurement, follow-up DxWBS are helpful for therapy response evaluation and to identify patients with suspected non-iodine–avid metastatic disease (based on elevated basal and/or stimulated Tg and negative WBS), which will prompt further investigation with 18F-FDG PET/CT and/or Dx CT scan for localizing structural persistent disease (73,149,150).
Response to Therapy in DTC Patients: Dynamic Risk Stratification Criteria (Modified from [6])
The combination of Tg, US, and follow-up DxWBS performed at 1–2 y after primary therapy is used to restratify the risk of recurrence according to patient response to initial therapy for more accurately predicting long-term clinical outcomes. Risk restratification criteria are summarized in Table 4 (6).
In patients with excellent response to therapy the risk of disease recurrence is 1%–4%, which for intermediate-risk patients (whose initial risk for recurrence is estimated at 36%–43%) and for high-risk patients (whose initial risk for recurrence is estimated at 68%–70%) represents a major change in risk when CR to therapy is achieved. The clinical outcomes in patients with biochemical incomplete response are usually good: ∼60% have no evidence of disease over long-term follow-up, 20% continue to have persistently abnormal Tg values without structural correlates, and only 20% develop structurally identifiable disease over 5–10-y follow-up. Patients with biochemical indeterminate response generally do well: in 80%–90% of patients the nonspecific biochemical findings either remain stable or resolve over time with T4 suppression therapy alone; however, up to 20% of these patients will eventually develop functional or structural evidence of disease progression and require additional therapies. Patients with structural incomplete response require multidisciplinary management tailored to their disease status (e.g., regional vs. distant metastases, iodine-avid vs. non-iodine–avid disease) (6). Depending on the results of such additional treatment patients may be restratified according to the criteria above.
Importantly, dynamic risk restratification has been validated only in patients treated with complete thyroid ablation (i.e., [near-] total thyroidectomy and postoperative 131I therapy). Evidence is not available for patients treated with lobectomy alone or with thyroidectomy without postoperative 131I therapy (151). After thyroidectomy, Tg levels are influenced by the amount of thyroid tissue remnant and the TSH level at the time of Tg measurement. Even if decreasing Tg levels may be reassuring, it is difficult to provide general interpretation criteria for serum Tg in such cases. Furthermore, measuring Tg is essentially useless after lobectomy, because Tg levels will not depend on the presence or absence of tumor but rather on the mass of remaining thyroid tissue, current iodine status, and TSH concentration (152). Park et al. (153) followed 208 low-risk PTC patients postlobectomy over a median of 6.9 y. The levels of Tg and Tg/TSH ratio and the proportions of patients in whom serum Tg levels increased by ≥50% or ≥100% over baseline measurement did not differ significantly in patients with or without recurrence (153).
VII. THERAPY OF ADVANCED DISEASE
Distant metastases develop in about 10% of DTC patients, commonly in lungs and less frequently in bone, brain, liver, and skin, and are the main cause of significant symptoms and death (i.e., overall mortality of 65% at 5 y and 75% at 10 y) (154). Younger patients and those with single-organ metastases and low disease burden have the best outcomes (60). The mainstay of metastatic disease treatment is TSH suppression and repeated courses of 131I treatment as long as the disease remains iodine-avid (155). About two-thirds of patients have radioiodine-avid distant metastases, and >40% of these will achieve remission after 131I treatments (60). However, a minority of DTC cases lose the ability to concentrate iodine in sufficient quantities to allow therapeutically effective radiation absorbed doses to DTC lesions (i.e., radioiodine-refractory DTC). Determining when a patient will no longer respond to 131I therapy can be challenging, and all factors impacting the patient’s specific clinical situation (such as age, tumor histology, initial stage, radioiodine residual avidity, and 18F-FDG avidity) should be carefully considered (156). Definitions of radioiodine-refractory DTC have been proposed by several authors (157–160), followed by updated classifications of radioiodine-refractory disease (20,156,161,162). Classification of a patient as radioiodine refractory is very important and consequential. If one classifies a patient as radioiodine refractory when, in fact, the patient may respond to a 131I therapy, then that patient has lost the potential benefit of an effective 131I therapy in a situation with limited therapeutic options. However, if patients receive 131I therapy without benefit, not only may they experience unnecessary side effects from an ineffective therapy, but a potentially beneficial alternative therapy is delayed.
The criterion with the best predictive value that a patient has radioiodine-refractory disease and will not respond to another 131I treatment is progression after a short time interval after administration of a maximum safe 131I therapeutic activity. All other criteria have varying degrees of likelihood that the patient is radioiodine refractory and should be cautiously considered, understanding their limitations (161). Although exact likelihood ratios cannot be given here for the various criteria that have been used in the past, Figure 5 presents an example of the spectrum of relatively low-to-high likelihoods of 3 criteria for predicting that a patient’s metastatic DTC is radioiodine refractory. Nevertheless, the time from 131I treatment to progression (i.e., progression-free survival [PFS]) after optimized 131I treatment is 1 of the most important criteria for predicting radioiodine-refractory DTC. Although in the past disease progression was considered in and of itself indicative of 131I treatment failure (6), progression must be considered in light of many factors (Table 5), including length of PFS and amount of 131I activity administered. Caveats guiding classification of a patient’s metastatic DTC as radioiodine refractory are also noted in Table 6. Additional management options to be considered prior to classifying a patient’s metastatic DTC as radioiodine refractory are presented in Table 7.

Likelihood of radioiodine-refractory differentiated thyroid cancer.
Additional Considerations Before Assignment of Radioiodine-Refractory Disease Status (161)
Caveats Regarding Criteria for Radioiodine-Refractory Metastatic Differentiated Thyroid Cancer (Adapted from [161])
Additional Options Prior to Radioiodine Refractory Classification
Despite a negative DxWBS, administration of 131I therapy should still be considered for obtaining a PT-WBS, which is more sensitive for detectig metastatic disease with reduced (but not absent) 131I-concentrating capacity. Although absence of uptake on a PT-WBS is a stronger indicator of radioiodine-refractory disease, it is not a definitive imaging biomarker for tumor NIS expression in the setting of progressive metastatic disease. Several authors have shown that the timing of a PT-WBS scan after therapeutic 131I administration (e.g., 3–4 d versus 5–7 d) can make the difference in interpretation between a negative and positive PT-WBS (80,81,83,84,163). Additional options to be considered before classifying a patient’s DTC as radioiodine refractory are: (1) refer the patient to a site that performs radioiodine dosimetry and/or frequently manages aggressive and progressive DTC; or (2) help selected patients explore eligibility for participating in a research study offering “resensitizing” or “redifferentiating” agents to determine if radioiodine uptake can be reestablished or increased for a potential 131I therapy (164–167).
Focally targeted treatment (i.e., resection, vertebroplasty, external-beam radiation therapy, and thermal ablation) can provide local control, provide symptomatic relief, and delay initiation of systemic therapy. These therapies can be used with concurrent 131I or other systemic therapies when targeting progression in a single lesion and may enable continued overall disease control (168). Treatment with bisphosphonates or denosumab can delay time to skeletal related events (169). However, caution is necessary if using biphosphonates, as there is a risk for osteonecrosis of the jaw, especially in patients treated with intravenous bisphosphonates. Therefore, it is important to evaluate dental health before initiation of such therapy and avoid dental procedures during the therapy (170). In cases of confirmed systemic progression of radioiodine-refractory disease, intravenous chemotherapy with doxorubicin was traditionally used, but a partial response was obtained only in a small minority of patients. More recently “targeted” therapies, including multikinase inhibitors (MKIs) (e.g., sorafenib and lenvatinib), have been approved for patients with advanced radioiodine-refractory DTC. These drugs have been shown to induce periods of PFS (rarely remission). However, they do not increase cancer-specific survival and may be associated with significant side effects, such as hypertension, diarrhea, hand/foot skin reactions, rash, fatigue, mucositis, loss of appetite, and weight loss (154). It remains unclear which patients will benefit from MKIs in terms of an increase in quality-adjusted life years and optimal time to start therapy, especially in asymptomatic patients. As a rule, molecular-targeted therapies should be started in patients with progression of measurable lesions (as defined radiologically by the Response Evaluation Criteria in Solid Tumors [RECIST]) over the previous 12 mo, taking into consideration tumor burden, disease sites, symptoms, and risk of local complications (171). In the setting of clinical trials involving redifferentiation strategy, molecular tumor analysis can direct therapy (e.g., BRAFV600E + → dabrafenib [± trametinib, vemurafenib; BRAF– → trametinib]). Furthermore, identification of NTRK RET fusion could also direct therapy toward selective inhibitors (e.g., selpercatinib).
The biologic mechanisms implicated in radioiodine refractoriness involve gain-of-function mutations in the MAPK-signaling pathway, resulting in reduced NIS and other iodine-metabolizing gene expression. Experimental data showed that MAPK-signaling pathway inhibition using MEK or BRAF inhibitors may restore radioiodine avidity. Subsequent clinical studies demonstrated that mutation-guided treatment using selective MEK inhibitors (selumetinib, trametinib), BRAF inhibitors (dabrafenib, vemurafenib), or a combination of BRAF inhibitor and MEK inhibitor is feasible and represents a promising strategy to redifferentiate radioiodine-refractory DTC, thereby permitting reapplication of 131I therapy. Preliminary data obtained on a small clinical series of 13 patients demonstrated restoration of 131I avidity in 62% of patients who subsequently received 131I treatment (median activity, 7.6 GBq [204.4 mCi]; range, 5.5–9.4 GBq [150–253 mCi]), resulting in durable disease control (median duration >1 y) while not receiving chronic, expensive MKI therapy (165). 131I therapy remains the only known cure for metastatic radioidine-sensitive DTC, and the use of a redifferentiating strategy to permit additional 131I treatment for patients with radioiodine-refractory metastatic disease represents a promising therapeutic approach while minimizing exposure to kinase inhibitor therapy.
A. 18F-FDG PET/CT Imaging for Thyroid Cancer
Advances in molecular Dx imaging and the clinical availability of PET/CT systems produced a paradigm shift in the management of thyroid cancer by allowing characterization of tumor biology based on variable uptake patterns of radioiodine and 18F-FDG in metastatic lesions. Feine et al. (172,173) described the “flip-flop” phenomenon as opposite radiotracer uptake patterns on radioiodine scintigraphy and 18FDG-PET/CT imaging, recognizing 4 patterns of variable radioiodine/FDG uptake in metastatic disease. Type I is characterized by negative 131I/positive FDG uptake and is the most commonly encountered pattern in patients with elevated Tg and negative scintigraphy (i.e., Tg+/scan–), which is found in ∼46% cases. Type II is characterized by positive 131I/negative FDG uptake and represents the most favorable context for therapeutic 131I administration. Type III consists of a combination of type I and II patterns recognized in different metastatic lesions within the same patient due to varying biologic behavior in metastatic foci. Type IV is characterized by uptake of both 131I and 18FDG within the same metastatic lesions. The flip-flop phenomenon is not a constant for DTC metastases but rather a variable marker of tumor biology. A prospective study of 122 postthyroidectomy patients with established metastatic DTC who were imaged with both DxWBS and 18FDG-PET/CT showed a general correlation of FDG avidity with lack of iodine avidity; however, the correlation coefficient was only 0.62. For the selected SUVmax cutoff value of 4.0, the authors calculated a sensitivity of 75.3% and specificity of 56.7% for identification of non-iodine–avid metastatic disease (174). Hence, the decision on whether to perform 131I therapy should not be based on 18F-FDG PET/CT alone. The most common application of PET/CT imaging in DTC is for evaluation of patients with elevated Tg and negative DxWBS (i.e., Tg+/scan–) (175).
B. Management Algorithm for Patients with Elevated Tg and Negative DxWBS (Tg+/Scan–)
Although this is frequently seen as 1 syndrome (called TENIS syndrome [Tg elevation, negative iodine scintigraphy]), in fact it represents a wide spectrum of clinical situations (discussed in more detail in the online complete version of the guideline).
Devising a treatment plan may be facilitated by following 4 steps:
Step 1: Rule out false-negative DxWBS and false-positive Tg levels: To evaluate for false-negative DxWBS, the interpreting physician needs to consider: (1) screening for a history of recent iodine load, such as recent administration of radiologic contrast agents or ingestion of kelp, as well as administration of amiodarone, even months to years earlier; (2) confirming compliance with LID as demonstrated by low urinary iodine levels (e.g., spot urine iodine level, spot urine I/Cr, or 24-h urine iodine collection); (3) ascertaining adequate TSH elevation, which is especially important with preparation by THW; (4) excluding heterophilic antibody interference on Tg measurement (prevalence 0.4%–1%) (176); (5) confirming correct radiopharmaceutical administration (reviewing documents for appropriate isotope and prescribed activity and reviewing the scan images themselves for inappropriate distribution of radioactivity); (6) confirming technical scan parameters (collimator type, peaking of energy window, table speed for planar scan, time interval for stop position for SPECT acquisition, etc). Although one may assume that all radioiodine scans are performed equally, they are not, and assessment of the quality of the scan is important to minimize false-negative radioiodine scans (177).
Step 2: Perform dynamic risk restratification: If the patient has a low risk for disease recurrence, active surveillance is appropriate and may include: (1) physical exam; (2) Tg, TgAb, and TSH testing; and (3) US of the thyroid bed and neck. However, nonradioiodine imaging is indicated when the patient has an intermediate or higher risk for disease recurrence. Other factors noted in Table 8 are relevant to consider.
Factors Considered for Management of Elevated Tg and Negative DxWBS (Tg+/Scan–) Patients
Step 3: Obtain nonradioiodine imaging: Nonradioiodine imaging studies for metastatic DTC have been divided into 3 tiers: primary, secondary, and tertiary. The primary tier includes: (1) neck US; (2) 18F-FDG PET/CT imaging; and/or (3) CT of the neck, chest, abdomen, and pelvis. These studies can be performed sequentially; however, whenever possible, integrated PET/CT imaging is preferable because it provides both functional and anatomic information. The secondary tier includes: (1) brain MRI; (2) bone scanning (using 99mTc-methylene disphosphonate [99mTc-MDP] or 18F-sodium fluoride PET/CT [18F-NaF PET/CT]); and (3) mitochondrial imaging (e.g., 99mTc-sestamibi, 201Tl, or 99mTc-tetrofosmin). These studies should primarily be reserved for patients in whom the first tier did not reveal metastatic lesions. In the context of advanced DTC, brain MRI is recommended, because patients may have brain metastases in the absence of neurologic signs or symptoms and 18F-FDG PET is not reliable in the brain due to high brain glucose metabolism. Although DTC osseous metastases are typically osteolytic and highly vascularized, bone metastases can occasionally be detected on 99mTc-MDP bone scintigraphy or 18F-NaF PET/CT when 18F-FDG PET/CT is negative. Although widespread implementation of 18F-FDG PET/CT imaging for evaluation of Tg+/scan– patients replaced routine use of mitochondrial imaging, the different uptake mechanisms of 99mTc-sestamibi and 18F-FDG in neoplastic cells provides the rationale for selected use of 99mTc-sestamibi in difficult patients with suspected metastatic disease not identified by other conventional imaging modalities (e.g., negative 131I WBS, US, 18F-FDG PET/CT, and CT) (79,178). The tertiary tier includes somatostatin receptor (SSR) imaging with radiolabeled somatostatin analogs (e.g., 99mTc-depreotide, 99mTc-EDDA/HYNIC-Tyr3-octreotide [Tektrotyd], 111In-octreotide, and 68Ga-DOTATATE/TOC/NOC). A substantial percentage of aggressive histologic variants of DTC (e.g., Hürthle cell, tall cell, insular variants) associated with locoregionally advanced and/or metastatic DTC exhibit cellular expression of SSR, which can be found independently of glucose transporter overexpression (i.e., in patients with negative 18F-FDG PET/CT imaging) (79). SSR PET imaging also often provides complementary information in 18F-FDG+ patients and appears to be especially promising in poorly differentiated and oxyphilic subtypes (i.e., Hürthle cell) metastatic DTC (179,180). Peptide-receptor radionuclide therapy using radiolabeled somatostatin analogues has shown promise for treatment of 131I-refractory metastatic DTC, with a demonstrated objective response rate of 20%–60% tumor reduction as determined by radiologic measurements (RECIST) (181–183). For the future, some promise is shown in individual cases employing 68Ga–prostate-specific membrane antigen imaging.
Step 4: Customize management to the location and number of the metastases: Once 1 or multiple metastatic sites are identified, one must decide whether tissue biopsy for histologic examination and mutational profile characterization is needed. Focally directed therapy needs to be considered for management of unifocal or oligometastatic disease (e.g., surgical resection, external-beam radiation therapy, alcohol injection, radiofrequency ablation, cryotherapy, embolization, and/or radioisotope embolization). 131I therapy should be considered if doubt is still present regarding 131I refractory status. Systemic and/or combined therapy is recommended for multifocal or widespread metastases.
C. 18F-FDG PET/CT Imaging for Prognosis of Metastatic DTC
Approximately 15%–20% of patients with metastatic DTC and most patients with Hürthle cell thyroid cancer are refractory to radioiodine, and OS for these patients ranges between 2.5 and 4.5 y (60,158,184). The prognosis of metastatic DTC is variable, with 2 distinct phenotypes identified: indolent and aggressive (185,186). Patients with iodine-avid metastatic DTC tend to have more favorable prognoses, with 10-y survival >90%, whereas non-iodine–avid metastatic DTC has a dire 10-y survival of 10% (187). On a molecular level, this is largely driven by genetic patterns, with specific mutations associated with aggressiveness of thyroid cancer disease (188). Two studies demonstrated suboptimal predictive value of staging, including the widely used TNM system (189,190). Tg doubling time (Tg-DT) has been identified as a prognostic factor, with Tg-DT < 1 y portending poor prognosis and Tg-DT > 2 y signifying good prognosis (191). However, Tg-DT cannot be calculated in the presence of TgAbs, which invalidate Tg measurements, and it cannot inform regarding the metabolic phenotype and spatial distribution of metastatic lesions. There is a large variability in survival time for patients with metastatic DTC, ranging from 1 to 30 y (186). The lack of accurate survival estimates for the individual patient has important implications for treatment decisions, especially regarding initiation of targeted MKI therapies (192,193). Due to the toxicity profiles of these medications, current National Comprehenisve Cancer Network guidelines advocate active surveillance as standard of care in metastatic disease until evidence of symptomatic or clinically progressive disease as outlined by RECIST (194,195).
18F-FDG PET/CT imaging is particularly useful not only for identification and localization of non-iodine–avid metastases but also for predicting the course of disease as aggressive or indolent. 18F-FDG PET/CT has demonstrated prognostic value for survival in metastatic DTC (196), predicting a survival disadvantage for patients with positive PET compared with those with negative PET results (184,197). Robbins et al. (184) demonstrated that in patients with metastatic DTC a positive 18F-FDG PET/CT scan result predicted a 7-fold increased risk of mortality compared with patients who had negative FDG scans.
18F-FDG PET/CT metabolic parameters can help define the volume and biologic variations of metastatic tumor burden. Specifically, metabolic tumor volume (MTV) and total glycolytic activity (also referred to as total lesion glycolysis [TLG]) have been proposed as imaging biomarkers for prognosis in human solid tumors (198). Robbins et al. (184) demonstrated that total FDG tumor volume and lesional SUVmax correlate with survival. Wang et al. (196) noted that an FDG volume >125 mL was associated with worse survival. The metabolic parameters of MTV and TLG obtained with 18F-FDG PET/CT have been used as surrogate markers for tumor burden and biologic aggressiveness for prognosis of OS and PFS in non-iodine–avid metastatic DTC. Higher-than-median MTV and TLG values were associated with worse OS and PFS, with a median OS of only 3.5 y for patients with radioiodine-refractory metastatic DTC (199). This information can be used to guide more rapid implementation of newer therapeutic agents for radioiodine-refractory metastatic DTC and enrollment in clinical trials.
VIII. CONCLUSION
DTC is the most common endocrine malignancy, with a rising incidence for the last 30 y. The standard of care for DTC patients is multidisciplinary and involves a risk-stratified approach integrating information from surgical histopathology, genetic markers, postoperative Tg levels, and anatomic/functional imaging studies. Early identification of residual nodal and/or distant metastases is particularly relevant for successful 131I therapy of metastatic disease, because patients who achieve a CR have considerably higher survival rates than patients with structural incomplete responses. Integration of Dx radioiodine scintigraphy in the management algorithm of patients with thyroid cancer should be considered, and further multidiciplinary collaborative studies to assess patient-relevant outcome measures (disease-specific survival, recurrence rates, and PFS) need to be performed.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.↵
- 139.
- 140.
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.
In this issue





{kind=link}
{kind=link}
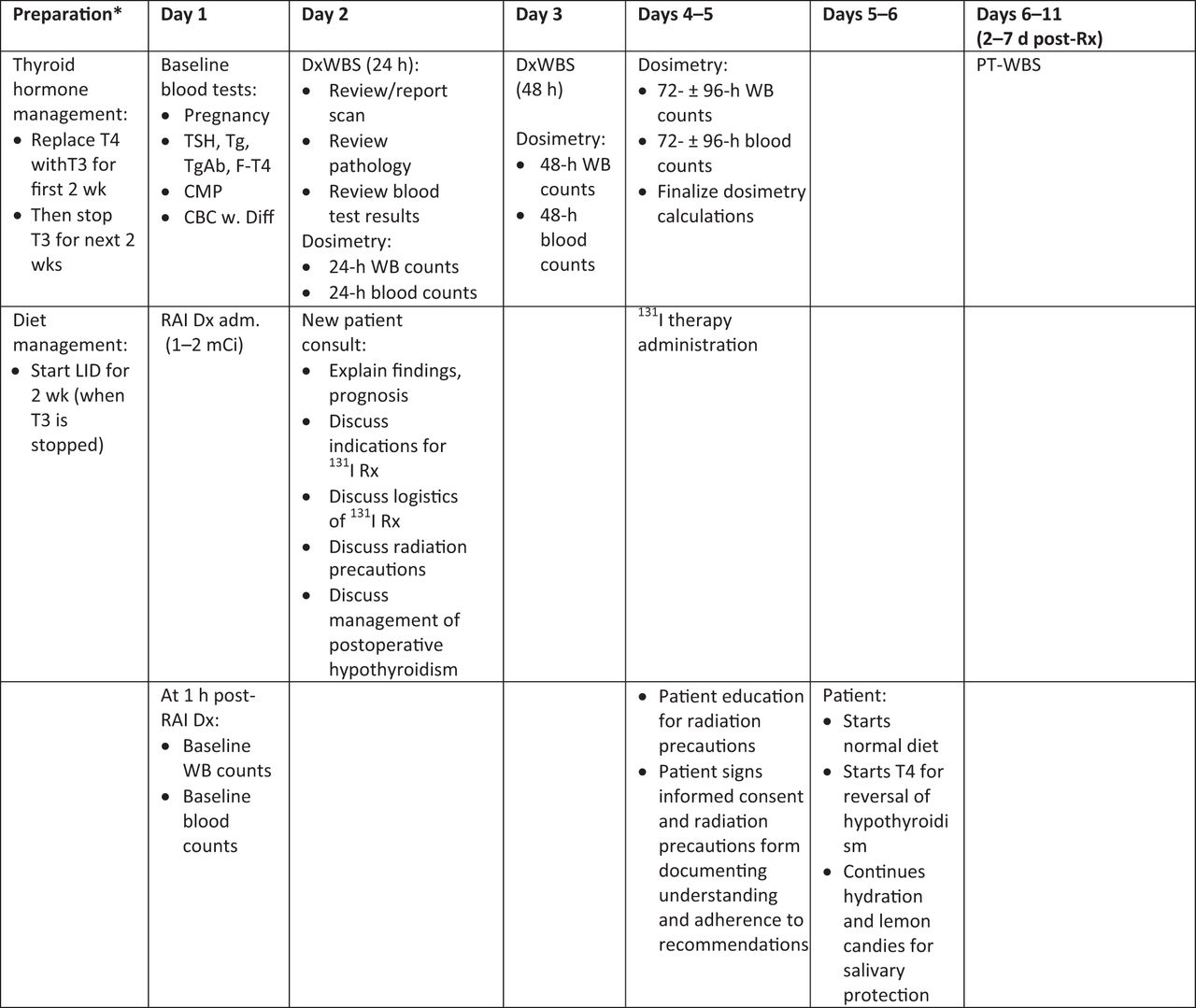{kind=link}
{kind=link}
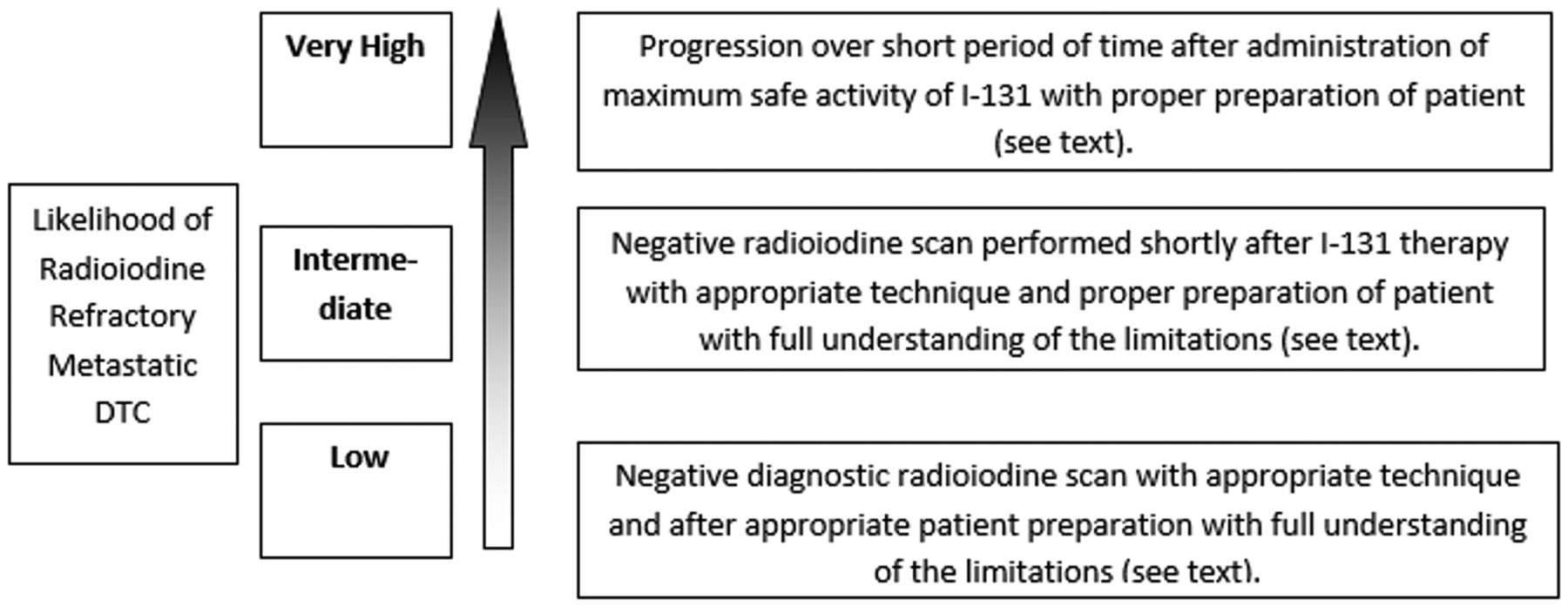{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.