


Abstract
To assess whether the patient preparation procedure for 131I scintigraphy could be streamlined, we evaluated the time course of thyroid-stimulating hormone (TSH) elevation after total thyroidectomy or after discontinuation of thyroxine (T4) in patients with thyroid cancer. Methods: The clinical records of 284 patients with well-differentiated thyroid cancer were reviewed. All patients had undergone total thyroidectomy. Two groups of patients were evaluated. The immediate postoperative group consisted of 176 patients who were not given thyroid hormone replacement after surgery because of planned postoperative 131I therapy. The surveillance group consisted of 108 patients in whom T4 replacement was stopped (without triiodothyronine [T3] replacement) in preparation for surveillance whole-body 131I scintigraphy. We recorded the first TSH measurement and number of days after surgery or without thyroid hormone for each patient. Results: In the immediate postoperative group, TSH levels obtained 6–65 d (median, 17 d) after surgery ranged from 18.2 to 194.8 μIU/mL (median, 46.6 μIU/mL). The TSH values exceeded 30 μIU/mL in 89% of patients evaluated at 1–2 wk, in 88% of those evaluated at 2–3 wk, and in 90% of those evaluated after 3 wk. In patients discontinuing T4 (without T3 replacement), TSH levels obtained from 6 to 35 d (median, 20 d) later ranged from 23.4 to 214.5 μIU/mL (median, 61.1 μIU/mL). The TSH levels exceeded 30 μIU/mL in 100% of patients evaluated at 1–2 wk, in 89% of those evaluated at 2–3 wk, and in 96% of those evaluated after 3 wk. Conclusion: In most patients with thyroid cancer being prepared for 131I imaging or therapy, a TSH level exceeding 30 μIU/mL can be achieved by withdrawal of thyroid hormone therapy for 1–3 wk.
Serum thyroid-stimulating hormone (TSH) concentrations in patients with thyroid carcinoma must be elevated before administration of 131I iodide either for diagnostic whole-body scintigraphy or for therapy, to ensure sufficient uptake of 131I in tumor tissue. The optimal TSH concentration is unknown, but a level of ≥30 μIU/mL is generally considered sufficient for both imaging and therapy (1,2).
There are 2 distinct groups of patients in whom TSH elevation is desired: patients who are to undergo 131I ablation of residual thyroid tissue after total thyroidectomy for a newly diagnosed thyroid carcinoma, and patients who undergo thyroid hormone withdrawal in preparation for whole-body 131I scintigraphy for surveillance. Although recombinant human TSH may be administered (without the need for thyroid hormone withdrawal) to prepare patients for whole-body 131I scintigraphy, this approach is not optimal for use in patients in whom a positive imaging result is anticipated. Such patients will typically undergo therapeutic administration of 131I after imaging, and thyroid hormone withdrawal is thus a prerequisite.
After thyroidectomy, it is generally held that circulating thyroid hormone (chiefly thyroxine [T4]) secreted before surgery delays the postoperative TSH response and that maximal TSH values are not reached until approximately 4–6 wk. The classic recommendation has thus been that patients be maintained postoperatively on triiodothyronine (T3) replacement therapy for 4 wk (1,3). T3 is then withheld, with the expectation that a TSH concentration of ≥30 μIU/mL will be achieved in 2 wk, reflecting the shorter biologic half-life of T3 than of T4.
The literature recommends a similar procedure for TSH elevation for follow-up 131I whole-body scintigraphy (and therapy): discontinue T4, substitute T3 for T4 for 4 wk, withdraw T3 for 2 wk, and then determine the serum TSH level (1). If TSH is not elevated to ≥30 μIU/mL, T3 withdrawal is maintained for an additional 1–2 wk until the TSH level exceeds that value. As an alternative, some institutions simply withdraw replacement thyroid hormone therapy for 4–6 wk, but this is said to lead to an unnecessarily long period of symptomatic hypothyroidism.
In our practice, we have not used T3 in any patient. We have relied on discontinuation of T4 replacement therapy and have measured serum TSH sooner than the generally recommended 4–6 wk. The purpose of this retrospective review was to evaluate the time course of TSH elevation in our patients after thyroidectomy or after T4 withdrawal without T3 substitution.
MATERIALS AND METHODS
We retrospectively reviewed the clinical records of patients with well-differentiated thyroid carcinoma treated at our institution between July 1998 and July 2002. The institutional Human Studies Committee approved this review. All patients underwent a total thyroidectomy for well-differentiated thyroid carcinoma and subsequently received postoperative 131I ablation or follow-up 131I scintigraphy. They were prepared for 131I administration by withholding of thyroid hormone replacement postoperatively or simple thyroid hormone withdrawal (without T3 substitution) and had at least 1 TSH measurement. For the purposes of this study, only the first TSH measurement in each patient was considered in the analysis.
The analysis included 284 patients, 72 men and 212 women, ranging in age from 6.8 to 85.4 y (mean, 45.9 y). TSH measurements were performed in routine fashion by licensed clinical laboratories. We had planned to obtain the first TSH measurement within 2–3 wk after surgery or T4 withdrawal. However, because this measurement was not obtained per a rigidly defined protocol, the actual timing of TSH measurements in our routine clinical practice ranged broadly.
Our analysis defined 2 groups of patients. The first group consisted of 176 patients who recently underwent total thyroidectomy without immediate thyroid hormone replacement therapy. These patients had known thyroid carcinoma and were scheduled to undergo postoperative 131I ablation. The second group consisted of 108 patients with a history of previous total thyroidectomy and postoperative 131I therapy for thyroid carcinoma. These patients were evaluated with annual surveillance 131I scintigraphy, and T4 was simply withdrawn in preparation for this test.
RESULTS
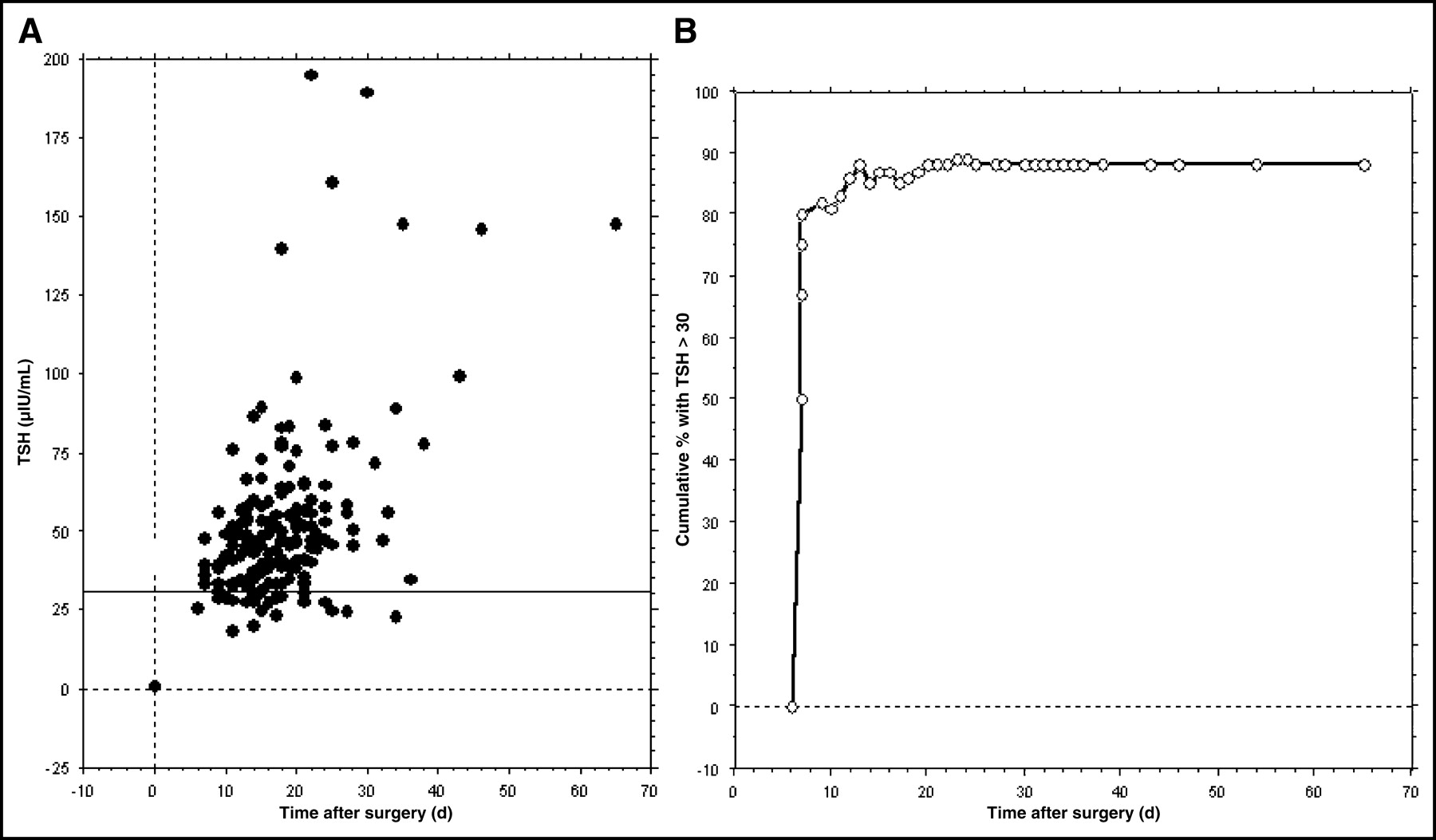
In the immediate postoperative group, the first TSH measurements were obtained 6–65 d (median, 17 d) after surgery, and the values ranged from 18.2 to 194.8 μIU/mL (median, 46.6 μIU/mL). These data are shown in Figure 1A and Table 1. Overall, 89% of initial TSH values exceeded 30 μIU/mL in these patients, as seen in Figure 1B (cumulative frequency). For the 11% of patients with the initial TSH level ≤ 30 μIU/mL, the values ranged from 18.2 to 29.6 μIU/mL (mean, 26.2 μIU/mL).

(A) Scatter plot of first TSH measurements as a function of time after total thyroidectomy (n = 176). (B) Cumulative frequency of TSH concentrations > 30 μIU/mL as a function of time after total thyroidectomy (n = 176).
Postoperative TSH Levels by Time Period
In the group of patients undergoing simple T4 withdrawal in preparation for surveillance scintigraphy, TSH values were obtained 6–35 d (median, 20 d) after discontinuation of T4; the TSH levels ranged from 23.4 to 214.5 μIU/mL (median, 61.1 μIU/mL). These data are shown in Figure 2A and Table 2. Overall, 93% of initial TSH values exceeded 30 μIU/mL in these patients, as demonstrated in Figure 2B (cumulative frequency). For the 7% of patients with an initial TSH level ≤ 30 μIU/mL, the values ranged from 23.4 to 29.1 μIU/mL (mean, 26.2 μIU/mL).

(A) Scatter plot of first TSH measurements as a function of time after abrupt T4 withdrawal (n = 108). (B) Cumulative frequency of TSH concentrations > 30 μIU/mL as a function of time after abrupt T4 withdrawal (n = 108).
TSH Levels by Time After Abrupt T4 Withdrawal
DISCUSSION
The classic protocol that is described in the literature (1,2) and recommended in the practice guidelines of several professional organizations (4–6) for elevation of serum TSH in preparation for 131I therapy or diagnostic imaging requires discontinuation of T4 replacement therapy, use of maintenance T3 therapy for 4 wk, and then discontinuation of T3 for 2–3 wk before TSH values are measured. Acceptance of this method of TSH elevation does not appear to be evidence based, as the literature contains scant data supporting this approach (7,8). Only recently did Liel (9) report on 13 patients who underwent T4 withdrawal and find that the mean interval to reach a TSH of ≥30 μIU/mL was 17 d. Also, Sanchez et al. (10) recently reported the results of a prospective study of 31 patients. In that study, 10 patients were in the immediate postoperative group and 100% achieved a TSH level of >30 μIU/mL within 3 wk. Sanchez et al. also studied 21 patients who discontinued T4; 90% had a TSH level of >30 μIU/mL within 3 wk.
The serum TSH concentration increases exponentially after total thyroidectomy (11) and after thyroid hormone withdrawal (7). Our data indicate that about 90% of patients with TSH values determined 1–3 wk postoperatively or after T4 withdrawal had TSH levels exceeding 30 μIU/mL. Accordingly, our results suggest that preparation of patients for 131I administration can be simpler (thyroid hormone withdrawal alone) and quicker (2–3 wk) than has classically been described.
One presumed advantage of the classic approach is that T3 is metabolized more quickly than T4, such that the hypothyroid state (and TSH elevation) can be achieved more quickly after stopping T3 than after stopping T4. One important limitation of our study is that we did not compare TSH measurements in patients undergoing T3 withdrawal with those in patients undergoing T4 withdrawal. However, our data do demonstrate that sufficient TSH elevation occurred within 1–3 wk in both of our patient groups, and this is the same period that classic protocols recommend for discontinuing T3 substitution therapy.
A major limitation of this study is its retrospective nature. TSH measurements were obtained but not routinely recorded before thyroidectomy. The presence of hypothyroidism in the clinical setting of thyroid cancer is rare (12). Also, baseline TSH measurements were not routinely recorded for the T4 withdrawal group. However, patients in this group were regularly followed clinically with routine TSH measurements, and TSH suppression to ≤0.10 μIU/mL was typical. None were known to be hypothyroid before T4 withdrawal. Unsuppressed TSH measurements were not obtained in accordance with a rigid schedule, but rather per clinical routine, with the initial planned measurement at 2–3 wk. Most patients did not have serial measurements of TSH because of the known exponential rise in TSH after withdrawal. Thus, we did not assess the time course of TSH elevation. In practice, we may repeat the measurement in 1 wk if the initial measurement is sufficiently low (72% of our patients with a TSH of <30 μIU/mL had a value between 25 and 29.9 μIU/mL, and these measurements were not repeated).
All patients in this study underwent a total thyroidectomy. However, the completeness of a total thyroidectomy is well known to be unpredictable (13). The presence of greater amounts of residual thyroid tissue may account for the failure of the TSH concentration to increase to >30 μIU/mL within 2–3 wk in some of our patients.
We did not assess the prevalence of hypothyroid symptoms in our patients while they were not receiving thyroid hormone replacement. Thus, another limitation of our study is that we do not know if such symptoms are more or less frequent with our method than with the classic method of T3 substitution and withdrawal. However, the frequency and severity of symptoms have been shown to correlate with the degree of hypothyroidism (14). We assume that since the degree and the duration of hypothyroidism are comparable in our patients and in patients managed in accordance with the literature recommendations, symptoms of hypothyroidism should not be worse with our methods.
CONCLUSION
An alternative to the classic approach to TSH elevation has been presented. Our method of no thyroid hormone replacement after initial surgery and discontinuation of T4 in preparation for whole-body 131I scintigraphy is less cumbersome than the classic method and appears to sufficiently elevate TSH within an acceptable time frame.
Footnotes
Received Sep. 30, 2003; revision accepted Nov. 17, 2003.
For correspondence or reprints contact: Perry W. Grigsby, MD, Department of Radiation Oncology, Box 8224, Mallinckrodt Institute of Radiology, Washington University School of Medicine, 4921 Parkview Pl., St. Louis, MO 63110.
E-mail: pgrigsby{at}wustl.edu





{kind=link}
{kind=link}