


Abstract
When thyroid tissues exhibited concentrations of therapeutic 131I that appeared to be less than that predicted by data from the preceding diagnostic 131I, the phenomenon was called stunning. We hypothesized that stunning arose from the early effects of the therapeutic dose of 131I and that the initial uptake of 131I, observed within the first day, was not impaired by the diagnostic dose. Methods: The hypothesis was tested by 2 types of studies. In each type, the fractional concentrations of 131I in residual neck thyroid tissues of patients with papillary thyroid carcinoma were quantified. In the first study, fractional concentrations of diagnostic and therapeutic 131I were measured at 2 d, a time when stunning has been observed, and expressed as ratios of radioactivity: therapeutic/diagnostic (Rx/Dx). Three different doses of diagnostic 131I were prescribed to assess a dose response. In the second study, patients were prospectively recruited and tested to record disappearances of radioactivity from thyroid tissues. Diagnostic doses were 1.0 mCi (37 MBq) in all; therapeutic doses were 150 and 30 mCi (5,550 and 1,110 MBq), each to half of the patients. The disappearance curves were extrapolated to the period between 0 and 1 d, an interval when maximum uptake of ingested 131I would be expected. The fractional concentrations of 131I at 2 d and at 0–1 d were compared in terms of Rx/Dx ratios to assess changes at each time point. Results: In the first study, after diagnostic doses of 2, 1, and 0.5 mCi (74, 37, and 18.5 MBq), mean 2-d Rx/Dx values in 24, 29, and 17 patients were 0.35, 0.50, and 0.46 (P = 0.087). Of all patients, 74% exhibited Rx/Dx <0.6. In the second study, 6 of 10 patients exhibited disappearance curves of 131I in which Rx/Dx was <0.6 at 2 d; 5 of the 6 had Rx/Dx values >0.97 at the 0- to 1-d point. In 1 patient the Rx/Dx was 0.54 at 2 d and 0.66 at the earlier time point. The other 4 patients had disappearance curves in which Rx/Dx values were >1.0 throughout or were above 0.6 and did not greatly change. Conclusion: Two days after the administration of 131I, the mean fractional concentration of radioactivity in thyroid tissues after a therapeutic dose is <60% of the diagnostic dose in most patients, but no correlation of Rx/Dx with the mCi in the diagnostic dose was seen. In 5 of 6 patients in whom the Rx/Dx at 2 d was <0.6, the maximum fractional concentrations of therapeutic and diagnostic 131I (i.e., the tissue uptakes during the first day) were similar; this pattern was most apparent after therapies with 150 mCi. These results support the hypothesis that “stunning” of thyroid tissues, often observable by 2 d, is primarily the consequence of early destructive effects from therapeutic 131I.
After total thyroidectomy, patients with well-differentiated thyroid carcinoma often manifest residual thyroid tissue(s) that are displayed by 131I scintigraphy. In some patients, the images of these thyroid tissues made a few days after therapeutic doses of 131I (usually >100 mCi or >3.7 GBq) appear to be less obvious than the images made before treatment with diagnostic doses of 131I (2–10 mCi or 74–370 MBq). This phenomenon has been attributed to stunning, an impairment of function of the tissues induced by the diagnostic 131I (1). Concern for stunning has led some physicians to prescribe treatments of 131I without prior diagnostic imaging in hopes of increasing the therapeutic effect (2,3).
There is an alternative explanation for some of the observed discrepancies between diagnostic and therapeutic images. We hypothesized that a relatively small diagnostic dose would not cause stunning, but that treatment doses of 131I would produce destructive effects that increased the rate of 131I loss from the tissue, and that this enhanced loss would be observable after an interval as brief as 2 d. In this case, differences in fractional concentrations of diagnostic and therapeutic 131I should be unrelated to the amount of diagnostic dose, and maximum uptakes of diagnostic and therapeutic 131I should be similar. This hypothesis was tested by 2 types of studies that quantified fractional concentrations of 131I in residual neck thyroid tissues of patients with papillary thyroid carcinoma.
MATERIALS AND METHODS
Patients
All patients were seen in the Nuclear Medicine Thyroid Clinic after a standard total thyroidectomy for well-differentiated papillary thyroid carcinoma at the University of Michigan Health System. Two types of studies were designed to test the hypothesis. In each study, concentrations of 131I in thyroid tissues were expressed as ratios: therapeutic/diagnostic (Rx/Dx). In the first study, a possible dose response to increasing doses of diagnostic 131I was sought by calculating Rx/Dx at 2 d. In the second study, disappearances of radioactivity from thyroid tissues over time were recorded, and the Rx/Dx values at the times of near-maximum 131I uptakes were determined. In each study, the patients were evaluated 5–6 wk after thyroid hormone deprivation, and each exhibited residual thyroid tissue in the neck by scintigraphy. Most were seen for initial postoperative imaging with 131I after total thyroidectomy; 3 patients who received 2 mCi (74 MBq) of diagnostic 131I in the first study had received prior 131I therapy.
Each patient in both studies was clearly hypothyroid, thyroid-stimulating hormone (TSH) >30 mU/L. Serum TSH concentrations were measured in the University of Michigan Laboratories, and values in the 150 mU/L range had a coefficient of variation of 3.6%. By visual inspection of the images, each exhibited sufficient tissue in the thyroid bed region for quantification. It was not possible to determine if thyroid bed tissue contained carcinoma. Treatments were given within 4 h of completion of the last diagnostic images. All doses of 131I were carrier free and ingested in liquid form. Patients were instructed to follow a low-iodine diet (4) for 1 wk before and until 1 d after treatment with 131I. Thyroxine therapy was initiated 1 d after treatment.
Quantification of Data
For both studies, in addition to whole-body scanning, conjugate images were made of the neck and chest for quantification of radioactivity in thyroid tissues. Dual-head cameras with high-energy, parallel-hole collimators produced the images in a 128 × 128 matrix. The cameras were Siemens Body Scan (first study) and Siemens E.CAM (second study). Some images were magnified 1.5× to make them more reproducible over time. The energy window was 30%, 15% above and below 360 keV. Rectangular regions of interest (ROIs) were drawn around observable thyroid tissue in the neck and around an area in the neck devoid of 131I-concentrating tissues for background; the ROIs were drawn so as to be reproducible over at least 7 d. Linearity of camera responses was assessed by measurements of a 131I source twice a week and by 99mTc source daily; drifts in response were always <10% even over many months. Tissue activity was expressed as the geometric mean (after background subtraction) divided by the administered dose of 131I to give a fractional concentration: counts per minute per mCi (cpm/mCi and equivalent to cpm/37 MBq). Patients whose images showed pixel saturation or observable dead time (found only in the first study) were excluded.
For diagnostic doses of 2, 1, and 0.5 mCi (74, 37, and 18.5 MBq), the periods of acquisition of data were 10, 20, and 40 min, respectively, thereby giving equal information densities (total counts from a ROI) when using different doses. Therapeutic data were acquired over 5 min.
These studies were approved by the University of Michigan Institutional Review Board for Medical Studies.
First Study.
Patients were evaluated in 3 groups divided according to the prescribed (±10%) diagnostic dose of 131I:
2 mCi (standard dose at the time) given from September 1993 through November 1995 (24 patients);
1 mCi (new standard dose) given from December 1995 through July 1998 (29 patients); and
0.5 mCi (patients recruited under a research protocol) given from August 1998 through June 1999 (17 patients).
A measurement of radioactivity in patients was made 44–48 h after administration of diagnostic and of therapeutic 131I. Data are expressed in terms of cpm/mCi and as a ratio of therapeutic/diagnostic results (Rx/Dx).
Second Study.
Ten patients were recruited prospectively. For diagnostic imaging, each patient received 1 ± 0.1 mCi (37 ± 3.7 MBq) of 131I. The initial protocol called for acquisition of data on a daily basis for 7 d after both the diagnostic and the treatment doses. However, recruitment of patients became almost impossible when prospective individuals learned that hypothyroidism and a low-iodine diet were to be prolonged by a week. Therefore, only 3 patients had diagnostic data acquired for >2 d. Nevertheless, the hypothesis could still be tested with the more limited diagnostic information by making the reasonable assumption that the near-maximum uptakes of radioiodine are between 6 and 24 h after ingestion. Five patients received about 150 mCi (5,550 MBq) and 5 were treated with about 30 mCi (1,110 MBq). Decisions for treatment were made by the physician-therapist; the smaller dose was prescribed when persisting carcinoma appeared unlikely. In patients receiving treatments in the range of 150 mCi, the retention of radioactivity at 1 d was too high to enable accurate measurements; for these subjects, data acquisition began at day 2.
The cpm/mCi in the thyroid tissues were expressed on semilogarithmic plots, and a curve of radioactivity disappearance was inscribed for each of diagnostic and therapeutic 131I. Assuming insignificant impairment of the potential maximum uptakes by radiation injury, the curves of the diagnostic and therapeutic doses should cross (Rx/Dx = 1) between 6 and 24 h. Extrapolations to 0 time are for reference only.
When monoexponential extrapolation appeared to give poor fits of data, curves were stripped (5) to give biexponential components (a pattern that may be seen when the disappearance of radioactivity is acted on by a second factor), and the sum of the first and second components was then extrapolated. Previous experience and the results from subjects 1–3 gave evidence that disappearance of diagnostic 131I was monoexponential.
Serum TSH was remeasured on the final day of testing to compare with the value at the outset. Serum thyroglobulin was assayed by the immunochemiluminescence in the University of Michigan Clinical Laboratory. Uptakes as percentage of the diagnostic 131I were measured at 1 d by a scintillation probe positioned 50 cm from the neck; a lead shield over the neck enabled assessment of background radioactivity.
Body retention of radioactivity in the patients was assessed at 2 d using the scintillation probe as previously described (6).
Statistics
Statistical analyses were by ANOVA and by least-square correlations made on Microsoft Excel.
RESULTS
First Study
Descriptions of patients in this study are given in Table 1. The means of Rx/Dx (in terms of cpm/mCi) for the groups receiving diagnostic doses of 2, 1, and 0.5 mCi (74, 37, and 18.5 MBq) were 0.35, 0.50, and 0.46, respectively. The means of Rx/Dx in each group demonstrate that, as a fraction of the dose, therapeutic 131I is substantially less than diagnostic 131I in thyroid tissues. However, there is no statistical difference by ANOVA among the 3 groups and no clear trend toward lower values with increasing doses of diagnostic 131I. The mean Rx/Dx of 0.35 in the 2.0-mCi group is somewhat lower than that in the other 2 groups, but the patients in the 2.0-mCi group also received somewhat higher treatment doses of 131I. The ranges of Rx/Dx were broad, but 74% of all values were <0.6. This level of Rx/Dx was arbitrarily adopted, because it is likely that when the relative radioactivity (in thyroid tissues compared with background) on therapeutic images is <60% of that on diagnostic images, there will be an appearance of stunning.
First Study: 131I in Residual Neck Tissues at 2 Days
Second Study
Data for the 10 patients, numbered according to chronologic assessment, are given in Table 2. The carcinomas were classified as stage I by TNM (7) and MACIS (8) systems for all but patient 8, who exhibited lung metastases on CT and scintigraphy. In each patient the residual tissue in the thyroid bed region was appraised; in patient 8, cervical node metastases were apparent on images and were evaluated separately.
Second Study: Patient Data
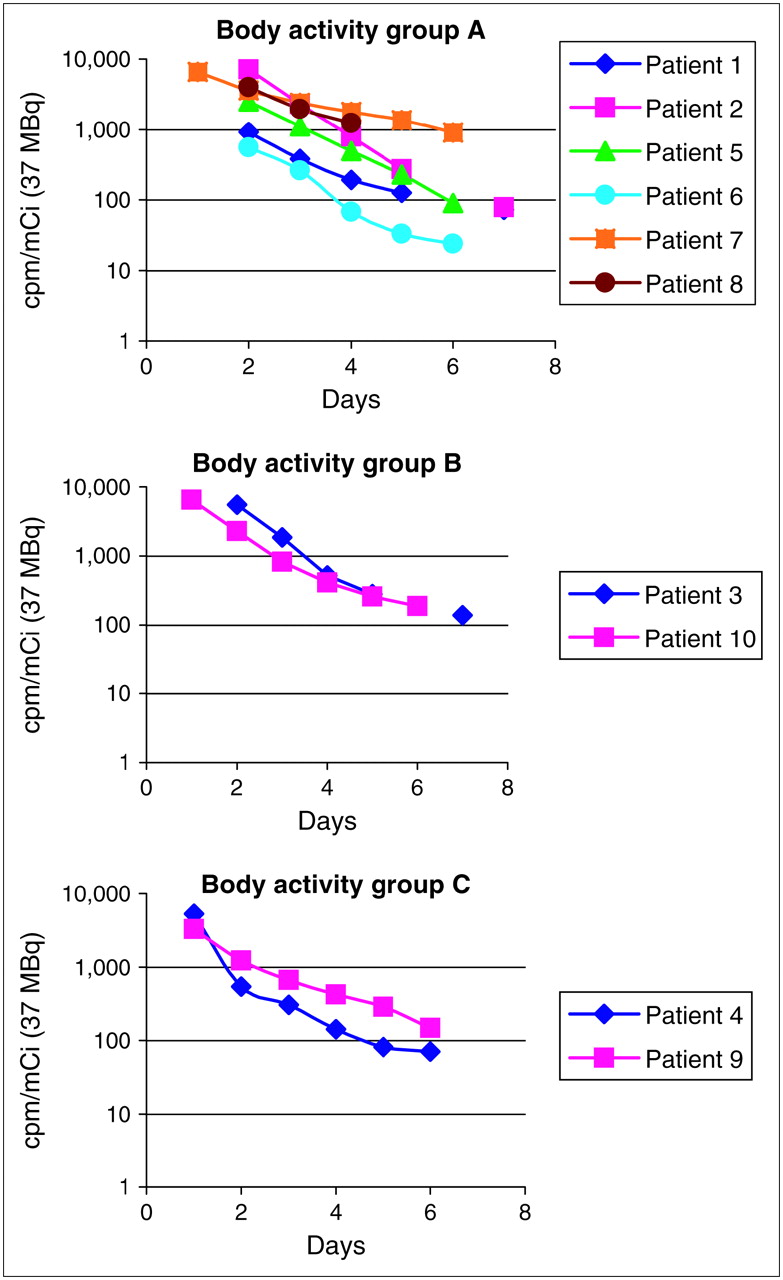
The hypothesis was tested again by comparing the fractional concentrations of 131I (cpm/mCi) as reflected in the ratio Rx/Dx. In 6 patients (1, 2, 5–8; designated group A) (Fig. 1; Table 2), the Rx/Dx values at 2 d were <0.6 (range, 0.12–0.54). During the first day, when ingested 131I is likely to be concentrated maximally in thyroid tissues, Rx/Dx was ≥0.94 in 5 of the 6 patients; 4 of the 5 had received the larger treatment, 150 mCi. In the sixth patient, patient 7, the highest Rx/Dx was only 0.66 (Fig. 1; Table 2).

131I disappearance from thyroid tissues over time (see text for descriptions of patterns). Group A: patients 1, 2, and 5–8 in whom Rx/Dx was <0.6 at 2 d. During the first day Rx/Dx was near unity in all but patient 7; group B: patients 3 and 10 in whom Rx/Dx was >0.6 at 2 d and in whom Rx/Dx values changed modestly over time; and group C: patients 4 and 9 in whom Rx/Dx levels were >1.0 at 2 d. For each subject the diagnostic dose was 1 mCi (37 MBq); therapeutic dose is expressed on each graphic plot. In patients 1, 2, and 4–6, the first and second components of therapeutic disappearance of 131I are inscribed and designated k1 and k2, respectively.
Patients 3 and 10 (designated group B) exhibited different disappearance curves (Fig. 1; Table 2). In patient 3, the Rx/Dx was moderately low at 2 d, 0.75, and was 0.89 earlier, indicating little Rx/Dx change and modest differences between Rx and Dx. In patient 10, the Rx/Dx value at 2 d, 0.82, was actually higher than the earlier values, giving an unusual pattern of 131I disappearance from the tissue. In patients 4 and 9 (designated group C), the Rx/Dx levels at 2 d were >1.0 and higher at earlier times.
Thus, of 10 patients, only one, patient 7, inscribed a pattern that could reflect a substantial impairment of uptake of 131I by thyroid tissue. In patients 1, 2, 5, 6, and 8, the patterns are consistent with an injury to thyroid tissue by the therapeutic 131I that is apparent by 2 d.
Patterns of diagnostic 131I disappearance from thyroid tissues in terms of cpm/mCi were monoexponential (r2 = 0.97–0.99) in patients 1–3 and assumed to be monoexponential (for extrapolation) in the other subjects. Patterns of disappearance of therapeutic 131I appeared in 3 forms (Fig. 1): monoexponential in patients 3, 8, and 10 (in each r2 >0.975); biexponential in patients 1, 2, and 4–6 (early exponential r2 ≥0.975 except that in patients 2 and 6, for whom an outlier point was excluded); and unusual pattern of late acceleration in patients 7 and 9.
In patients in group A, the pattern of uptakes, derived from extrapolation, were similar for Dx and Rx, but the accelerated disappearance of Rx was most obvious in patients 1, 2, 5, and 8, who received the 150-mCi treatment (Fig. 1).
In patient 8, the patterns of disappearance of 131I from tissue in the thyroid bed (probably largely nonmalignant) and from the metastases in cervical lymph nodes were similar.
The ratio of TSH levels, end/outset, in the subjects was 0.87 ± 0.16 (Table 2), and in 2 subjects there was a slight increase in TSH at the end of study. It seems unlikely that the modest changes in TSH stimulation of tissues, from beginning to end, played a significant role in the disappearance patterns of therapeutic 131I.
Patterns of disappearances of therapeutic 131I from the bodies of the patients are shown for groups A, B, and C in Figure 2. There was no apparent difference among the groups. In addition, no differences were found between patients receiving 30 and 150 mCi (not shown).
Disappearance of therapeutic 131I from bodies of patients over time. Composites are of groups A, B, and C (Fig. 1).
Only 6 patients have thus far returned for follow-up imaging; the effectiveness of the treatment doses in scintigraphic ablation of residual thyroid tissues cannot yet be determined.
DISCUSSION
Results of Studies
Our patients with well-differentiated papillary thyroid carcinoma received 131I both for diagnostic imaging and for treatment aimed at residual thyroid tissue in the neck. In the first study, 3 different diagnostic doses were administered. Two days after administration of 131I, there was a marked reduction in fractional radioactivity of the therapy doses compared with the diagnostic doses: Rx/Dx ≤50%; and 74% of all had Rx/Dx ratios of <0.6. Such reductions could have resulted from stunning of the tissue by the diagnostic dose, but there was no correlation between the Rx/Dx and the amount of diagnostic dose. This pattern could also have resulted from an injury effect induced by the treatment dose that was apparent by 2 d. The wide range in Rx/Dx values may have been the consequence of differing therapeutic doses and, more importantly, differing absorbed radiation doses in the tissues.
In the second study, the Rx/Dx ratios in thyroid tissues at 2 d were <0.6 in 6 of the patients, approximately the same proportion observed in the first study. In 5 of the 6, the Rx/Dx values, obtained by extrapolation to near the times of maximum concentrations of 131I, were ≥0.94, indicating no impairment of uptake. Four of the 5 were treated with 150 mCi; their patterns of 131I disappearance from thyroid tissues showed the most striking changes during the period from the time at which maximum uptake was extrapolated from 2 d. One of the 6 exhibited a pattern that could have been a manifestation of reduced uptake of therapeutic 131I. The other 4 patients had patterns of disappearance of therapeutic 131I that did not demonstrate substantial, if any, impairment of the extrapolated early uptake, but also did not portray a great decline in Rx/Dx at day 2. Therefore, it would seem that the diagnostic dose had little effect on the therapeutic dose in 9 of 10 patients.
In patient 8, the disappearance of radioactivity from nodal metastases was similar to that from tissue in the thyroid bed; this therapeutic effect then is seen in malignant as well as benign thyroid residuals.
Patterns of disappearance of therapeutic 131I varied and seemed to fall into 3 groups: monoexponential, biexponential, and unusual. The administered doses of therapy, 30 and 150 mCi, did not correlate with the different patterns. Biexponential disappearance may be the consequence of 2 superimposed factors: the basic loss of 131I seen after diagnostic doses and an injury-enhanced loss from the treatment dose. The cause of the other 2 patterns is unknown but may relate to differing effects from the absorbed doses of radiation—that is, gray (Gy), effects that cannot be determined without accurate measurements of tissue volumes. In fact, the absorbed dose is the principal factor in determining the effects of radiation on tissues.
It is possible that the diagnostic doses incur effects not seen on the early uptake but only on the disappearance of subsequent 131I. Such a limited effect seems unlikely. A diagnostic radionuclide that deposits less damaging radiation than 1 mCi (37 MBq) of 131I, such as 123I in 10 mCi (370 MBq) or more, would seem to be a preferable diagnostic agent. However, in our experience, the logistics of obtaining sufficient 123I for a study to be interposed on a standard pattern of clinical care made such a protocol impractical. The acquisition of more data points would have improved the accuracy of results, but the nature of this human study precluded more measurements, including those at 24 h after 150 mCi (5.6 GBq) where there were concerns for radiation exposure to personnel and camera dead time. Near-maximum uptakes are approximations. In addition, the maximum uptake of ingested 131I in thyroid tissues may vary among individuals and especially among hypothyroid patients in whom gastrointestinal activity is slowed; maximum uptakes could occur at or near 24 h as suggested in the curves of patient 5. Early injury from therapeutic radiation could reduce the potential maximum uptake, but we assumed that this would impose an insignificant effect on our approximations.
Literature Comparisons
Evidence for stunning by a diagnostic dose of 131I has been developed by 3 methods. Diagnostic images were usually made from 2–10 mCi (74–370 MBq) of 131I, and therapies were 30–200 mCi (111–7,400 MBq), but most were >100 mCi (>3,700 MBq).
Scintigraphic.
Images of therapeutic doses of 131I have been interpreted as showing less radioactivity (compared with background) in thyroid tissues than in the preceding images made with diagnostic doses. On evaluation of scintigraphic images, 2 groups reported substantial proportions of patients who exhibited stunning: in 77% (1) and 74% (9). Others reported stunning rates of 1.4% (10), 19% (11), and 21% (12). Even allowing for the differences in the diagnostic doses of 131I and the intervals of time from dose to imaging in these studies, the variations in results are still difficult to reconcile. Some discrepancies can be laid to the subjective nature of image interpretation, the techniques of enhancing images, and the marked differences in counting rates emanating from diagnostic and therapeutic doses. Our results indicate that treatments will reduce 131I in tissues, and this effect is often, but not invariably, apparent by 2 d. In these circumstances, it is probable that many images of the therapeutic doses would differ from those of the diagnostic doses, but it may take more than a 40% difference to be readily appreciated on visual inspections that rely heavily on differences in target and background radioactivity.
Rate of Ablation of Residual Tissues.
In groups of patients treated with 131I, complete disappearance of scintigraphic evidence of residual thyroid tissue on images (ablation) was the index of response. In only one publication was ablation observed less frequently in patients who received treatment preceded by diagnostic imaging than in patients who were treated without diagnostic imaging: 50% and 76%, respectively (13). Others described overall ablation rates of 65%–91% but no significant differences between groups (11,14,15). If the changes in thyroid tissues were primarily from the absorbed radiation imparted by treatments, differences in ablation rates would depend on other difficult-to-control factors, such as volumes of tissue, concentrations of 131I per gram of tissue, and effective half-lives. These multiple variables make for uncertainty when interpreting ablation results.
Quantified Uptakes or Effective Half-Lives.
Radioactivity was measured in ROIs of individual thyroid tissues at 2 d after diagnostic doses of 0.5–5.0 mCi (18.5–185 MBq) and after therapies averaging 100 mCi (3,700 MBq). The fractional uptakes of 131I after therapy averaged 50% of those after diagnosis (16). In another report, 131I emanating from the necks of patients was counted at 3 d after treatment (120 mCi or 4,440 MBq) and diagnosis (2 mCi or 74 MBq). Mean thyroid uptakes expressed as a ratio, therapy/diagnosis, were 30%, and the ratio of mean effective half-lives was 75% (17). The results in these 2 investigations are in keeping with our hypothesis.
In each of 6 subjects, 131I was measured in ROIs to give 24-h uptakes and effective half-lives, each of which was made sequentially under 3 different circumstances: after diagnostic 2 mCi (74 MBq) following recombinant TSH; after diagnostic 2 mCi (74 MBq) during hypothyroidism; and after therapeutic 80–110 mCi (2,960–4,070 MBq). Data from the 3 types of measurements showed a progressive decline in the uptakes. There was also a progressive decline in the effective half lives of 131I (18). The decline from the second to the third measurement (diagnosis to therapy) is consistent with our results, but the decrements from the first to second diagnostic measurements do not support our hypothesis. However, the reproducibility of the initial assays—that is, uptake and retention after stimulation by recombinant TSH—was not provided, and, in this circumstance, the effective half-lives in 6 of 12 lesions were 8 d, signifying a most unusual pattern where there is no biologic loss of 131I.
In 12 patients thyroid tissue uptake of 123I was assessed at 2 h, and, after an intervening 5 mCi (185 MBq) of 131I, was remeasured; there was a significant decline in mean uptakes of 123I from 3.8% ± 1.5% to 2.0% ± 0.7% (19). This suggests stunning of uptake by the diagnostic dose of 131I, but 2-h uptakes are subject to several variables, and, in another cohort of 28 patients, the basal uptakes of 123I were more varied: 4.4% ± 3.1%. The results do not make an entirely convincing case for stunning, but 5 mCi (185 MBq) may impart sufficient ionizing radiation to reduce subsequent uptakes in thyroid tissues by stunning.
In patients with thyroid cancer and hyperthyroidism, thyroid tissue uptakes were measured by a scintillation probe 3 d after 111–178 MBq (3.0–4.8 mCi) of diagnostic 131I on 2 occasions within 1 wk. In 6 of the 7 patients, the second uptake was reduced to <60% of the first uptake (20). It is possible that combined doses of >6 mCi (>222 MBq) delivered sufficient energy to cause injury and produce the changes observed 3 d after the second dose.
When patients with benign thyroid disease were treated twice with 15 mCi (555 MBq) within an interval of 4 d, the second uptake was reduced to 68% of the first uptake, but the effective half-life measured over 5 d was unchanged (21). A dose of 131I, such as 15 mCi, could be sufficient to impair the iodide-concentrating power of thyroid tissue at the time of the second 15 mCi. Concentration of 131I from the second treatment then would be expected to start at a lower uptake level, and the effective half-life of the 131I would also begin at a lower point, but, from a similar injury, a disappearance curve may inscribe a similar half-life. Thus, these data may be consistent with our findings following the treatment doses.
The uptake of 125I by porcine thyroid cells in culture was impaired by as little as 3 Gy of absorbed radiation delivered by exposure to131I that had ceased 3 d previously (22). Again, stunning would be expected after sufficient injury from radiation. A concentration of 131I of 0.1 mCi/g (3.7 MBq/g) is expected to deliver about 75 Gy to a human hyperthyroid gland (23), and, if a 50-g gland exhibits a 50% uptake, then 3 Gy would be imparted from 0.40 mCi (14.8 MBq) of administered 131I (24), a dose that seems unlikely to produce substantial injury in vivo. Quantitative differences between results in porcine cell culture and human thyroid tissue would not be unexpected.
Results from a different type of study bear on the subject of stunning. In patients exhibiting residual thyroid tissues, ablation treatments with 131I were followed by increased urinary excretion of iodide as early as 24 h and maximally at 48 h (25). These changes were attributed to early injury of thyroid tissue by the therapies; the observations are consistent with ours.
CONCLUSION
Our results indicate that a major cause of the phenomenon called stunning is the response to injury of thyroid tissue from radiation by treatment doses of 131I. Importantly, injury will be more closely correlated with the absorbed radiation dose than with the administered dose, but measuring the former is beyond the capacity of clinical laboratories. Nevertheless, it appears that diagnostic information can be obtained from administration of 1 mCi (37 MBq) without concern for impairment of effectiveness of the subsequent treatment. Our results do not exclude reduction of uptakes, true stunning, from diagnostic doses of 131I greater than 1 mCi. It is not known how much 131I in a diagnostic dose is likely to reduce subsequent uptakes, but 6 mCi (222 MBq), a dose that has been therapeutically effective for some patients with hyperthyroidism (23), may produce sufficient injury to incur such stunning.
One set of experiments will not provide definitive answers to vexing questions such as stunning. However, our data bring new evidence to bear and provide a potent argument against stunning as originally described.
Acknowledgments
This research was supported by the General Clinical Research Center at the University of Michigan (National Institutes of Health grant MO1-RR00042). The authors are indebted to Dr. Barry Shulkin for suggestions on data acquisition to James Carey for information on curve analysis. Dr. Robert Koeppe provided invaluable advice on data modeling. Carol Kruise greatly aided the preparation of the manuscript.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 8, 2005.
- Accepted for publication March 13, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline for Nuclear Medicine Evaluation and Therapy of Differentiated Thyroid Cancer: Abbreviated Version
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Thyroid Cancer in Children
- Radiation-Induced Thyroid Stunning: Differential Effects of 123I, 131I, 99mTc, and 211At on Iodide Transport and NIS mRNA Expression in Cultured Thyroid Cells
- Down-regulation of the Sodium/Iodide Symporter Explains 131I-Induced Thyroid Stunning
- Reply: Re: The So-Called Stunning of Thyroid Tissue
- Re: The So-Called Stunning of Thyroid Tissue
- Reply: Stunning Effect
- Stunning Effect
- Thyroid Stunning Revisited