


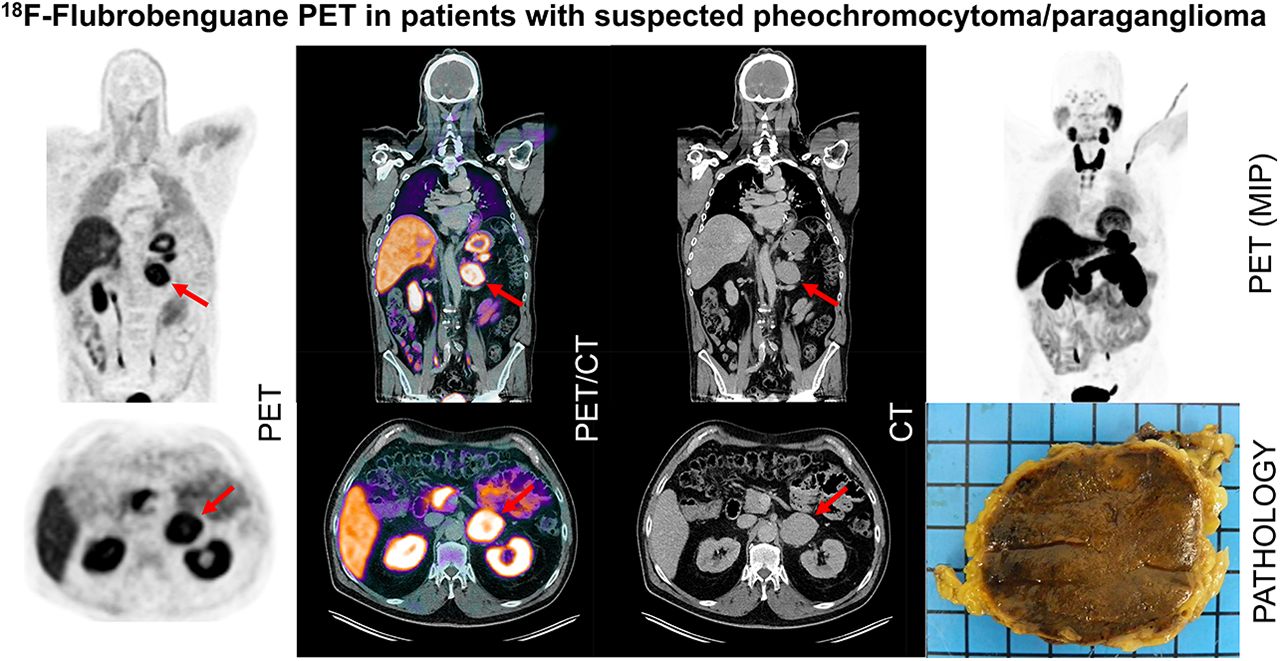
Visual Abstract
Abstract
Pheochromocytomas and paragangliomas are a rare tumor entity originating from adrenomedullary chromaffin cells in the adrenal medulla or in sympathetic, paravertebral ganglia outside the medulla. Small lesions are especially difficult to detect by conventional CT or MRI and even by SPECT with the currently available radiotracers (e.g., metaiodobenzylguanidine [MIBG]). The novel PET radiotracer 18F-flubrobenguane could change the diagnostic paradigm in suspected pheochromocytomas and paragangliomas because of its homology with MIBG and the general advantages of PET imaging. The aim of this retrospective analysis was to evaluate 18F-flubrobenguane in pheochromocytomas and paragangliomas and to investigate the biodistribution in patients. Methods: Twenty-three patients with suspected pheochromocytoma or paraganglioma underwent PET/CT or PET/MRI at 63 ± 24 min after injection of 256 ± 33 MBq of 18F-flubrobenguane. The SUVmean and SUVmax of organs were measured with spheric volumes of interest. Threshold-segmented volumes of interest were used to measure the SUVmean or SUVmax of the tumor lesions. One reader evaluated all cross-sectional imaging datasets (CT or MRI) separately, as well as the PET hybrid datasets, and reported the lesion number and size. The diagnostic certainty for a positive lesion was scored on a 3-point scale. Results: 18F-flubrobenguane showed a reproducible, stable biodistribution, with the highest SUVmax and SUVmean being in the thyroid gland (30.3 ± 2.2 and 22.5 ± 1.6, respectively), pancreas (12.2 ± 0.8 and 9.5 ± 0.7, respectively), and tumor lesions (16.8 ± 1.7 and 10.1 ± 1.1, respectively) and the lowest SUVmax and SUVmean being in muscle (1.1 ± 0.06 and 0.7 ± 0.04, respectively) and the lung (2.5 ± 0.17 and 1.85 ± 0.13, respectively). In a subgroup analysis, a significantly higher average SUVmean was seen for both pheochromocytoma and paraganglioma than for healthy adrenal glands (11.9 ± 2.0 vs. 9.9 ± 1.5 vs. 3.7 ± 0.2, respectively). In total, 47 lesions were detected. The reader reported more and smaller lesions with higher certainty in PET hybrid imaging than in conventional imaging; however, statistical significance was not reached. Of the 23 (23/47, 49%) lesions smaller than 1 cm, 61% (14/23) were found on hybrid imaging only. Conclusion: Our preliminary data suggest 18F-flubrobenguane PET to be a new, effective staging tool for patients with suspected pheochromocytoma or paraganglioma. Major advantages are the fast acquisition and high spatial resolution of PET imaging and the intense uptake in tumor lesions, facilitating detection. Further studies are warranted to define the role of 18F-flubrobenguane PET, particularly in comparison to standard diagnostic procedures such as MRI or 123I-MIBG SPECT/CT.
Pheochromocytomas are rare, catecholamine-producing tumors originating from chromaffin cells in the adrenal medulla or in sympathetic, paravertebral ganglia outside the medulla (the latter are usually referred to as paragangliomas) (1,2). Sympathetic paragangliomas may be located in the pelvis, the abdomen, or the thorax. About 80%–85% of pheochromocytomas arise from the adrenal medulla, whereas 15%–20% originate from extraadrenal chromaffin tissue (1). Pheochromocytomas and paragangliomas may occur in the context of genetic disorders (3–5). Furthermore, pheochromocytomas may be bilateral in more than 10% of cases or may even be multifocal (particularly in familial pheochromocytoma syndromes) (1,6). Malignancy is relatively rare in adrenal pheochromocytomas (≤5%) but is quite common in paragangliomas (≤33%) (1,7). There is no genetic or histologic marker that definitely indicates malignancy in these tumors; for this reason, malignancy is defined in the World Health Organization classification as being the occurrence of metastasis (8). Surgery is generally recommended as the primary treatment, with curative intent (2). These facts illustrate the immense importance of noninvasive assessment of the disease before surgery.
CT is recommended as the primary imaging modality because of a high sensitivity of about 90%, whereas MRI is recommended in special situations only (e.g., paragangliomas of the head and neck, contrast medium allergy, or young patients) (2,9,10). Both CT and MRI have low specificity. In contrast, iodine-labeled (123I- or 131I) metaiodobenzylguanidine (MIBG) scintigraphy and SPECT imaging demonstrate a high specificity ranging from 70% to 100% at an acceptable sensitivity (56%–88%) for both pheochromocytomas and paragangliomas (2). However, PET is usually preferred over SPECT because of the higher sensitivity and higher spatial resolution of the former, often resulting in higher diagnostic accuracy (11). Also, PET allows for truly quantitative imaging, facilitating response assessment (11), and has shorter acquisition times.
The available PET tracers for the assessment of pheochromocytoma or paraganglioma are 18F-FDG, somatostatin receptor targeting tracers such as 68Ga-DOTATATE, and rarely used PET tracers such as 11C-hydroxyephedrine, 18F-fluorodopa, 18F-fluorodopamine, or 124I-MIBG. However, these radiotracers have disadvantages such as a long half-life and high cost (124I), the need for an onsite cyclotron (11C), a complex radiosynthesis (18F-fluorodopa and 18F-fluorodopamine), or a low specificity for pheochromocytoma and paraganglioma (somatostatin receptor targeting tracers) (12–14). N-[3-bromo-4-(3-18F-fluoro-propoxy)-benzyl]-guanidine (18F-flubrobenguane, formerly known as LMI1195) is a novel, 18F-labeled radiotracer that has a high homology with MIBG and can visualize norepinephrine transporters with a high affinity and specificity (15). This radiotracer has been evaluated successfully in a MENX tumor model, a rat model with bilateral pheochromocytomas (16). In humans, this radiotracer has been evaluated in healthy volunteers for biodistribution and radiation dosimetry studies and in a recent case report of a 74-y-old man with heart failure who underwent 18F-flubrobenguane and 11C-hydroxyephedrine PET (17,18). The aim of this retrospective analysis was to evaluate 18F-flubrobenguane in patients with suspected pheochromocytoma or paraganglioma.
MATERIALS AND METHODS
Radiotracer Synthesis
18F-flubrobenguane was synthesized as previously described (15).
Briefly, the synthesis was performed using a brosylate precursor and a 1-step no-carrier-added 18F displacement reaction with high-performance liquid chromatography purification. Radiochemical purity was at least 95% in all performed syntheses, and specificity was more than 130 GBq/μmol. The radiotracer was formulated in an 8% ethanol/saline solution.
All patients gave written informed consent for the procedure as a legal requirement for 18F-flubrobenguane PET/CT or PET/MRI on a compassionate-use basis. All reported investigations were conducted in accordance with the Helsinki Declaration and with national regulations. The retrospective analysis was approved by the local Ethics Committee (permit 142/20 S-KH). The administration of 18F-flubrobenguane complied with the German Medicinal Products Act, AMG §13 2b, and the responsible regulatory body (Government of Upper Bavaria).
Patient Population and Imaging Protocol
Twenty-three patients with clinically suspected or a history of pheochromocytoma or paraganglioma underwent whole-body (head to mid thigh) PET/CT (Biograph mCT) or PET/MRI (Biograph mMR) between August 2016 and November 2018 (Table 1). Fifteen patients underwent at least one other imaging modality before 18F-flubrobenguane PET (CT, 8; MRI, 9), including 4 patients whose medical history showed that they had undergone 123I-MIBG SPECT/CT. In total, 26 PET scans (24 PET/CT, 2 PET/MRI [3 patients were scanned twice]) were performed after injection of a mean activity of 256 ± 33 (range, 183–307 MBq). The PET acquisition was started after 63 ± 24 min (range, 43–143 min). In PET/CT, a diagnostic CT scan in the portal venous phase was performed (Imeron 300 [iomeprol 300 mg iodine/mL, Bracco Imaging Deutschland, Konstanz, Germany] at 1.5 mL/kg of body weight). In PET/MRI, the following sequences were acquired: T1-weighted volumetric interpolated breath-hold examination (VIBE) Dixon (for attenuation correction purposes), axial and coronal T2-weighted half-Fourier-acquired single-shot turbo spin echo (skull to mid thigh), axial diffusion-weighted imaging, axial T1-weighted VIBE with contrast dynamics, and axial T1-weighted in-phase/opposed-phase, axial T1-weighted VIBE fat saturated (all upper abdomen). For contrast-enhanced MRI, a 0.2-mL dose of gadoterate meglumine (Dotarem [Guerbet], 0.5 mmol/mL) per kilogram of body weight was injected.
Patient Characteristics and Scan Details
Quantitative and Qualitative Image Analysis
The biodistribution of 18F-flubrobenguane was quantified by SUVmean and SUVmax corrected for body weight (19). Spheric volumes of interest 1 cm in diameter (salivary glands, thyroid, myocardium, stomach, and pancreas) and 2 cm in diameter (bladder, liver, spleen, kidney, muscle, aortic lumen, and lungs) were placed inside the organs’ parenchyma. SUVmean and SUVmax for tumor lesions were measured by circular, 3-dimensional regions of interest at a 40% isocontour around the lesions using Syngo.via software (Siemens Healthcare).
Imaging data of the hybrid PET/CT or combined PET/MRI were read separately against the respective cross-section imaging dataset only by a dual board-certified radiologist and nuclear medicine physician. Lesion size and number were reported, and the diagnostic certainty for positive lesions was rated using the categories “possible,” “probable,” or “consistent with.”
Additionally, in the 4 subjects who underwent both 123I-MIBG SPECT/CT and 18F-flubrobenguane PET/CT, imaging datasets were compared visually for divergent findings.
Histopathology
Thirteen patients (13/23, 57%) underwent surgery and subsequent histopathologic analysis of the tumor lesions. Eleven of those had a positive finding (11/13, 85%): 2 patients had proven paraganglioma (2/11, 18%) and 9 patients had pheochromocytoma (9/11, 82%). In 2 patients (2/13, 15%), an adrenal adenoma was diagnosed.
Statistics
Data are reported as mean ± SEM, and all statistical analysis was performed with Prism, version 8.4.2 (GraphPad Software). To compare groups, the Student t test was applied, or ANOVA was applied if more than 2 groups were compared and data were normally distributed. The Mann–Whitney test was performed for nonparametric data. Differences were considered statistically significant at P values of less than 0.05.
RESULTS
Quantitative Analysis of Biodistribution and Tumor Lesions
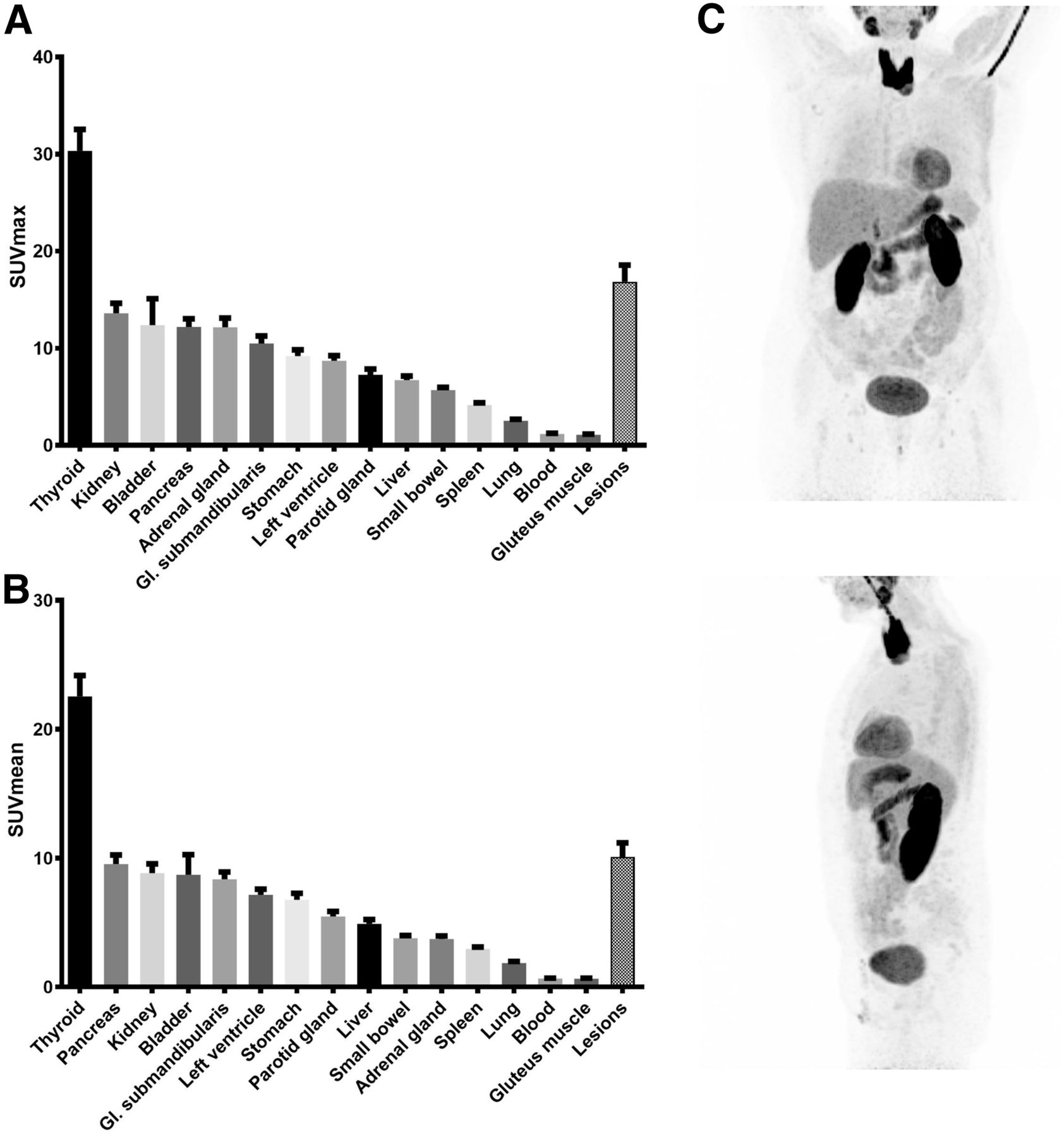
18F-flubrobenguane showed stable and reproducible biodistribution in healthy organs. The highest SUVmean was in the thyroid glands (22.5 ± 1.6), pancreas (9.5 ± 0.7), and kidneys (8.8 ± 0.7), the last of these being due to the excretion pathway of the radiotracer. Accordingly, high uptake in the urinary bladder was observed (8.7 ± 1.5). SUVmean was lowest in the lungs (1.85 ± 0.13), muscles (0.7 ± 0.04), and blood pool (0.65 ± 0.03).
Lesions suspected of being pheochromocytoma or paraganglioma had very intense uptake (SUVmean, 10.1 ± 1.1) that was significantly higher than uptake in liver parenchyma and healthy adrenal glands (4.9 ± 0.3 and 3.7 ± 0.24, respectively; P < 0.0001). SUVmax was 16.8 ± 1.7 versus 6.7 ± 0.4 versus 12.2 ± 0.95, respectively; P < 0.01) (Figs. 1 and 2A). Uptake in pheochromocytoma and paraganglioma was relatively similar (SUVmean, 11.9 ± 2.0 vs. 9.9 ± 1.5, respectively [P = 0.44]; SUVmax, 19.0 ± 3.0 vs. 16.8 ± 2.1, respectively [P = 0.55]). When pheochromocytoma and paraganglioma were evaluated separately, tracer uptake was significantly higher than in healthy adrenal glands (SUVmean, 11.9 ± 2.0 vs. 9.9 ± 1.5 vs. 3.7 ± 0.2, respectively [P < 0.01]; SUVmax, 19.0 ± 3.0 vs. 16.8 ± 2.1 vs. 12.2 ± 0.95 [P < 0.05]) (Fig. 2.).
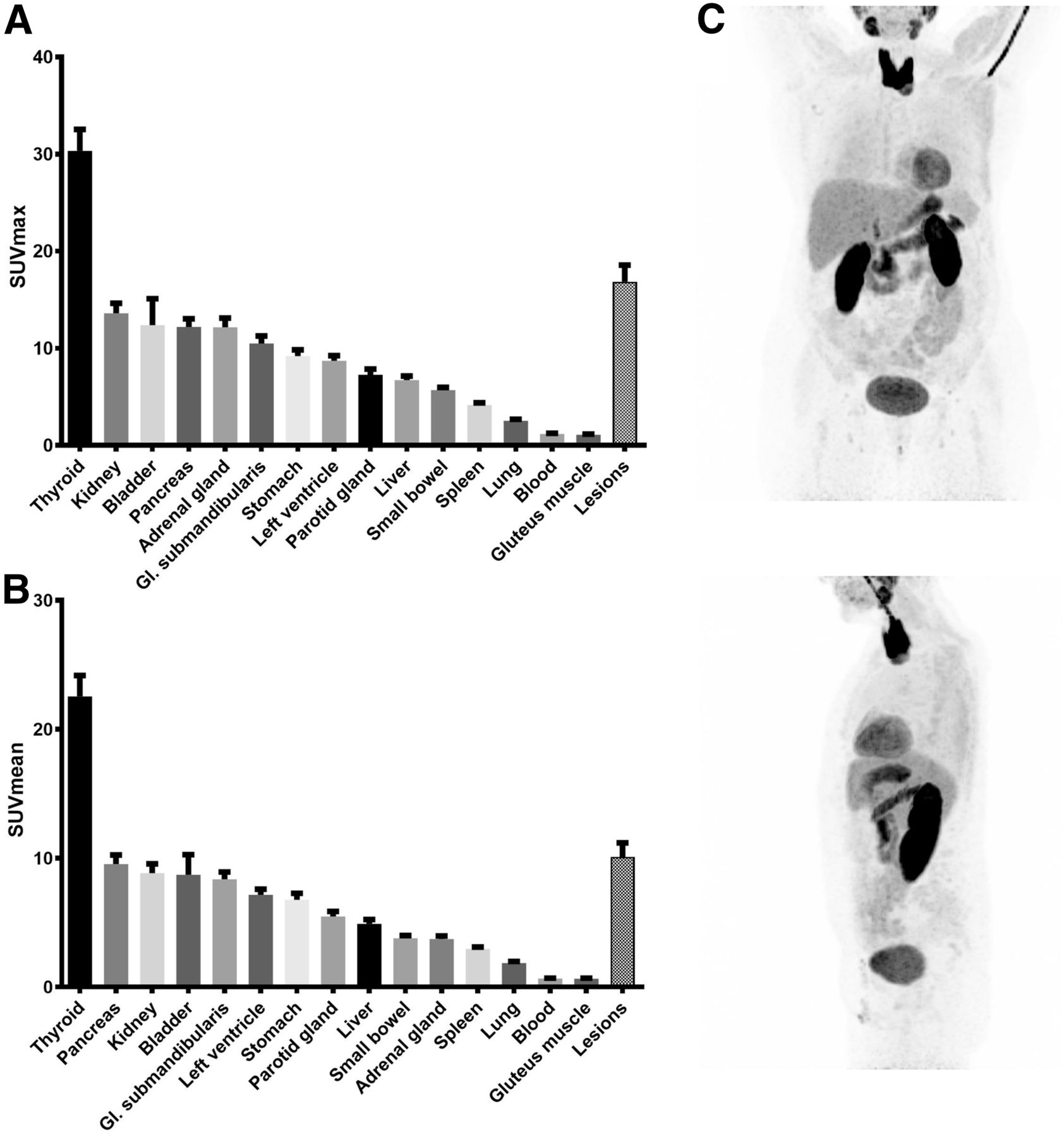
(A and B) SUVmax (A) and SUVmean (B) of 18F-flubrobenguane in organs. Highest uptake is in thyroid, pancreas, and pheochromocytoma and paraganglioma lesions. Lowest uptake is in muscle, lung, and blood pool (aortic lumen). (C) Maximum-intensity projection of negative PET scan. Gl. = glandula.

SUVmax and SUVmean of pheochromocytoma and paraganglioma lesions, liver, and adrenal glands. (A) SUVmean was significantly higher in all lesions than in liver parenchyma and adrenal glands and was significantly higher in liver parenchyma than in normal adrenal glands. (B) SUVmax was significantly higher in lesions and healthy adrenal glands than in liver parenchyma. (C and D) SUVmean (C) and SUVmax (D) were significantly higher in paraganglioma and pheochromocytoma than in healthy adrenal glands and liver. *P < 0.05. **P < 0.01. ****P < 0.0001. PGL = paraganglioma; PHEO = pheochromocytoma.
Lesion Detection and Certainty
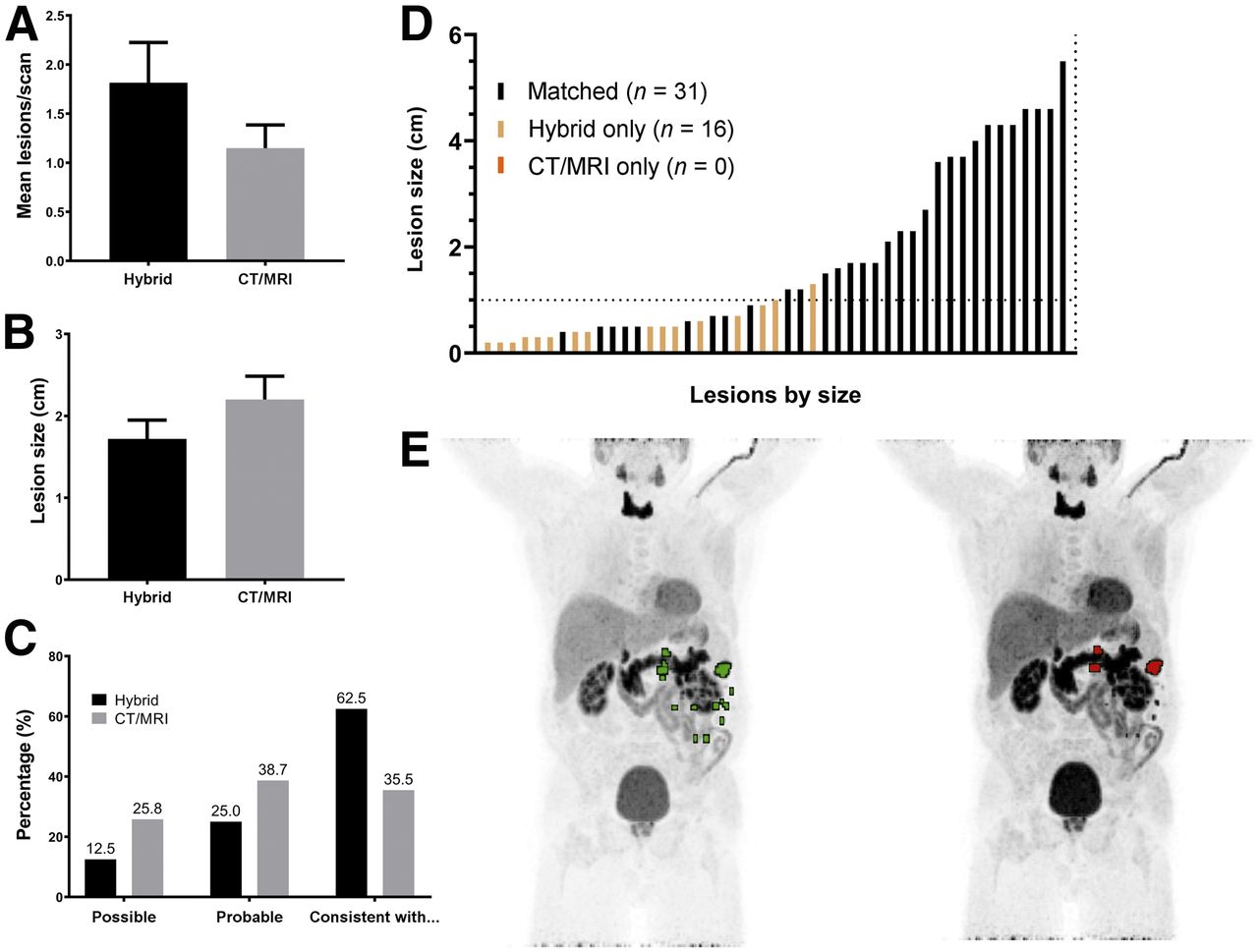
In total, 47 lesions were detected on hybrid PET/CT or PET/MRI. No statistically significant difference in number of lesions or lesion size was present. Still, a clearly higher number of lesions (1.8 ± 0.4 vs. 1.1 ± 0.2, P = 0.24) was reported for hybrid imaging than for CT or MRI (Fig. 3A). Especially, a smaller mean lesion size was reported for 18F-flubrobenguane PET/CT or PET/MRI (1.7 ± 0.2 cm vs. 2.2 ± 0.3 cm, P = 0.10) (Fig. 3B). In addition, diagnostic certainty about positive lesions was superior for 18F-flubrobenguane hybrid imaging, with 62.5% of lesions rated as “consistent with,” 25.0% rated as “probable,” and 12.5% rated as “possible,” compared with 35.5%, 38.7%, and 25.8%, respectively, for CT or MRI alone (Fig. 3C).

Separate and combined reading of 18F-flubrobenguane PET hybrid imaging and CT or MRI. (A and B) There was no significant difference in number of lesions per scan (A) or lesion size (B) in either reading. (C) Reader certainty was higher for hybrid imaging. In total, 47 lesions were detected. (D) Most lesions were found on CT or MRI and on hybrid imaging (matched; n = 31). No lesion was detected on CT or MRI alone (n = 0), but several lesions were detected on hybrid imaging alone (n = 16). An increased number of smaller lesions were detected by hybrid imaging. (E) Representative maximum-intensity projections of patient with multiple lesions. On left are lesions reported on hybrid imaging (green); on right, lesions reported on CT or MRI alone (red).
Interestingly, of the 47 lesions detected in total, 31 (66%) were found both on cross-sectional imaging alone and on PET hybrid imaging, whereas 16 (34%) were found on hybrid imaging only. No lesions were seen only on cross-sectional imaging. Of note, 61% (14/23) of the 23 (23/47, 49%) lesions smaller than 1 cm were found on hybrid imaging only, whereas 92% (22/24) of the lesions larger than 1 cm were also detected on cross-sectional imaging (Fig. 3D).
Case Examples
Figure 4 depicts the 18F-flubrobenguane PET/CT images of 2 patients. First, a 50-y-old man was referred because of an unclear lesion on conventional imaging in the left adrenal gland and a history of hypertension. 18F-flubrobenguane PET/CT showed only mild tracer uptake, and surgical resection diagnosed an aldosterone-producing adenoma (Fig. 4A). In the other patient, a 57-y-old man with an elevated concentration of metanephrine in the plasma, a contrast-enhancing, centrally hypodense lesion with intense 18F-flubrobenguane uptake was detected in the right adrenal gland and suspected of representing pheochromocytoma. Subsequent surgical resection and histopathology verified the imaging results. Correspondence was seen between the necrotic area within the tumor, which showed no uptake, and intense tracer uptake in the vital surrounding area (Fig. 4B). In our cohort, only 2 individuals were diagnosed with an adrenal adenoma after surgical resection; the adenomas and the healthy adrenal glands of these patients had a similar SUVmean (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org).
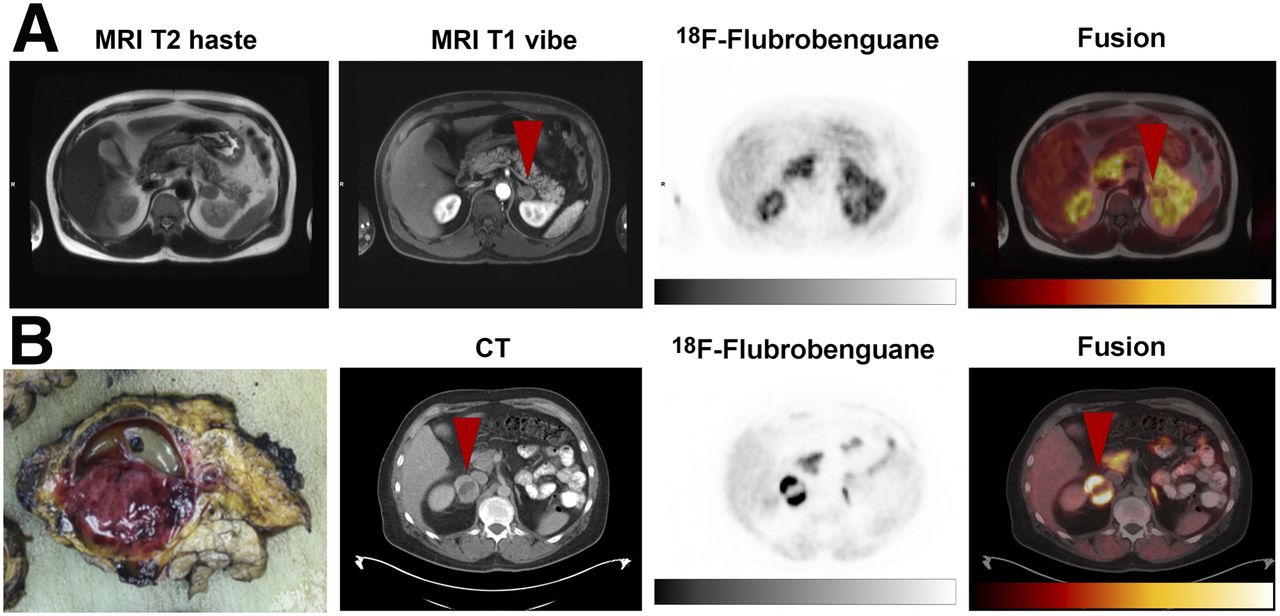
Case examples of adrenal adenoma and pheochromocytoma. (A) A 50-y-old man with hypertension and unclear lesion in left adrenal gland. 18F-flubrobenguane PET/CT showed only mild tracer uptake (arrowheads), and surgical resection diagnosed aldosterone-producing adenoma. (B) A 57-y-old man with pathologically elevated metanephrine concentration in plasma. Pheochromocytoma (arrowheads) was detected in right adrenal gland on 18F-flubrobenguane PET/CT by increased tracer uptake in lesion but focal lack of uptake in central necrotic tissue, as was verified after surgical resection. haste = half-Fourier-acquired single-shot turbo spin echo.
In a third patient, who was 38 y old and had recurrent pheochromocytoma after multiple resections, 123I-MIBG SPECT/CT was performed for suspected recurrence (Supplemental Fig. 2). The scan revealed suspected paravertebral lesions close to the left kidney. In a follow-up scan with 18F-flubrobenguane PET/CT 6 mo later, 2 small lesions with intense 18F-flubrobenguane uptake, which were not detectable on 123I-MIBG SPECT/CT, could be identified in the pelvis. In another follow-up 18F-flubrobenguane PET/CT scan 14 mo after the SPECT/CT, lesions were still detectable and overall stable disease was reported. Since a stable condition was previously reported over several years by means of annual 123I MIBG SPECT/CT examinations, progressive disease appeared very unlikely and the reason for the additional lesions most likely lay in the superiority of 18F-flubrobenguane PET over 123I SPECT. However, this single case does not allow general conclusions on a comparison of the 2 tracers and imaging modalities.
DISCUSSION
In the present retrospective study, a novel 18F-labeled PET radiotracer, 18F-flubrobenguane, targeting the norepinephrine transporter was evaluated in 23 patients with clinical suspicion of, or a history of, pheochromocytoma or paraganglioma. The results demonstrated a favorable biodistribution, with pheochromocytomas and paragangliomas having intense uptake clearly above the level in the normal adrenal glands and surrounding liver tissue. Furthermore, hybrid 18F-flubrobenguane PET/CT or PET/MRI led to greater diagnostic certainty than morphologic imaging with CT or MRI alone. Particularly, lesions smaller than 1 cm were more often found to be suggestive of pheochromocytoma or paraganglioma with 18F-flubrobenguane PET than with morphologic imaging alone.
Although various PET tracers are already available for the assessment of pheochromocytomas or paragangliomas, such as 11C-hydroxyephedrine, 18F-fluorodopa, 18F-fluorodopamine, or 124I MIBG, these tracers have not found their way into clinical routine because of various disadvantages such as a short half-life or complex radiosynthesis. Accordingly, in the clinical setting, 123I- or 131I-MIBG SPECT/CT, 18F-FDG, or somatostatin receptor–targeted imaging (e.g., 68Ga-DOTATATE) are usually used, all of which demonstrate a rather low sensitivity or specificity. Previously published data favor 68Ga-DOTATATE over 18F-FDG because of a higher lesion-to-background contrast than, and a similar detection rate to, 123I-MIBG SPECT/CT. However, the somatostatin receptor is not a specific target of pheochromocytoma and paraganglioma (13,20,21).
Because of its broad availability, iodine-labeled MIBG is the most applied radiotracer for pheochromocytoma and paraganglioma SPECT/CT. MIBG is a guanethidine analog with structural similarities to norepinephrine (22) and is often used for imaging of adrenal neoplasms (especially pheochromocytoma, paraganglioma, and neuroblastoma). For imaging purposes, the radionuclide 123I has advantages over 131I, imposing a lower radiation burden on the patient and having superior image quality and higher sensitivity and specificity (23–25). On the downside, MIBG SPECT/CT has lower image quality and low tracer-to-background ratios, no quantitative capability, and often a need for multiple acquisition time points (4 and 24 h after injection), resulting in only limited patient comfort and compliance. Consequently, there is a yet-unmet clinical need for feasible PET tracers not just for primary staging and diagnosis but for assessment of therapy response and follow-up examinations.
In the last couple of years, 18F-flubrobenguane has gained more attention, especially for cardiac sympathetic innervation imaging, and its application (mostly in small animals) has been thoroughly described (15–18,26–29). These findings underline the potential clinical application of this tracer. Further, the first in vivo studies showed that 18F-flubrobenguane is a suitable PET tracer for pheochromocytoma in a MENX model and therefore interesting for clinical applications (16).
PET imaging has multiple major advantages over 123I- or 131I-MIBG SPECT, such as better imaging quality, faster acquisitions at a single time point at a comparable effective dose, and the possibility of true quantification (17,30). With these advantages in view, 18F-flubrobenguane combines both PET imaging and a MIBG analog, which might allow an evaluation of therapy response or progressive disease on follow-up examinations superior to that possible with previous methods (31–33).
To our knowledge, this work was the first to evaluate 18F-flubrobenguane as a diagnostic tool in patients with suspected pheochromocytoma or paraganglioma. Because of the relatively small cohort of subjects, the scope of this work did not include an evaluation of the diagnostic accuracy (e.g., sensitivity and specificity) of this new diagnostic modality; rather, the work assessed its principal applicability in this patient population. All patients with histopathologically proven pheochromocytoma or paraganglioma were judged positive on 18F-flubrobenguane PET, indicating high potential for further clinical assessment.
We showed that 18F-flubrobenguane is a suitable PET tracer in pheochromocytomas and paragangliomas, with excellent imaging quality and a high tracer-to-background ratio. Significantly higher tracer uptake was seen in tumor lesions than in healthy adrenal glands and liver parenchyma, making it easier for readers to discriminate pathologic tracer uptake in the adrenal from the liver parenchyma or the contralateral normal adrenal gland. Additionally, our limited reader data hint that 18F-flubrobenguane PET hybrid imaging can be beneficial in detecting smaller tumor lesions with greater certainty than is possible with conventional imaging. Of course, this possibility needs to be validated in larger cohorts or even prospective trials.
Further studies are warranted to investigate the performance of 18F-flubrobenguane in larger clinical trials, particularly with a head-to-head comparison to 123I-MIBG SPECT and conventional imaging such as MRI and CT, which could result in a change in diagnostic management.
There are several limitations to this retrospective analysis. First, we investigated a small and heterogeneous patient cohort that included patients with suspected or recurrent paraganglioma or pheochromocytoma. Further, in only slightly more than half of the cohort was histopathologic validation possible. In cases without histopathologic results, no defined reference standard was available. This is an inherent problem in negative diagnostic test results and could be solved by follow-up examinations. Consequently, we omitted calculation of sensitivity and specificity. Future—preferably prospective—studies need to investigate whether 18F-flubrobenguane PET really has additional value over established examinations such as CT, MRI, or 123I MIBG SPECT, since this question cannot be answered conclusively in the present retrospective study using a clinical patient group in a real-life scenario.
CONCLUSION
The 18F-labeled catecholamine analog 18F-flubrobenguane represents a promising radiotracer for the detection and staging of pheochromocytomas and paragangliomas. 18F-flubrobenguane provides a stable and reproducible biodistribution with high uptake in tumor lesions. The relatively fast acquisition time and excellent image quality on PET are advantageous for pheochromocytoma and paraganglioma staging, and further applications in other tumor entities (e.g., neuroblastoma) should be investigated as well. Nonetheless, because there have been no thorough comparisons of this novel tracer to other established diagnostic methods (e.g., 123I- or 131I-MIBG SPECT/CT or MRI), its clinical benefits need to be evaluated in larger clinical trials.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is the novel sympathetic nerve imaging tracer 18F-flubrobenguane suitable for the evaluation of patients with suspected pheochromocytoma or paraganglioma?
PERTINENT FINDINGS: In 23 patients with suspected pheochromocytoma or paraganglioma, 47 lesions were detected. When 18F-flubrobenguane PET/CT was compared with conventional imaging, more and smaller lesions were described, without reaching statistical significance. A significantly higher tracer accumulation was found in pheochromocytoma or paraganglioma than in the healthy adrenal gland.
IMPLICATIONS FOR PATIENT CARE: 18F-flubrobenguane PET is a promising imaging modality in patients with suspected pheochromocytoma and paraganglioma and should be investigated in larger studies.
Footnotes
Published online Aug. 28, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 27, 2020.
- Accepted for publication July 20, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}