


Abstract
The impact of prostate-specific membrane antigen (PSMA) PET/CT on management of prostate cancer (PCa) patients with biochemical recurrence (BCR) is well established. However, whether and how PSMA PET/CT affects the management of patients undergoing scans for other clinical indications remains unknown. The goal of this study was to determine the impact of 68Ga-PSMA-11 PET/CT on initial and subsequent management decisions in a cohort of PCa patients referred for various indications (i.e., a basket trial) excluding the 2 main classic indications: BCR and presurgical staging. Methods: This was a prospective study of 197 patients that aimed to determine the impact of 68Ga-PSMA-11 PET/CT on PCa stage and management. The indications for PSMA PET/CT were initial staging of nonsurgical candidates (30 patients) and restaging after definitive treatment (167 patients). The restaging cohort comprised patients restaged with known advanced metastatic disease (n = 103), after androgen deprivation therapy only (n = 16), after surgery and with serum prostate-specific antigen levels lower than 0.2 ng/mL (n = 13), after radiation therapy and not meeting the Phoenix criteria (n = 22), and after other primary local treatments (i.e., high-intensity focused ultrasound, focal laser ablation, cryoablation, hyperthermia, or irreversible electroporation) (n = 13). Patients with BCR and candidates for curative surgery were excluded. Impact on management was assessed using pre- and post-PET questionnaires completed by referring physicians, electronic chart review, or patient telephone calls. Results: PSMA PET/CT changed the disease stage in 135 of 197 (69%) patients (upstaging in 38%, downstaging in 30%, and no change in stage in 32%). Management was affected in 104 of 182 (57%) patients. Specifically, PSMA PET/CT impacted the management of patients who were restaged after radiation therapy without meeting the Phoenix criteria for BCR, after other definitive local treatments, and with advanced metastatic disease in 13 of 18 (72%), 8 of 12 (67%), and 59 of 96 (61%), respectively. Conclusion: PSMA PET/CT has a profound impact on stage and management of PCa patients outside the 2 main classic indications (BCR and presurgical staging) across all examined clinical scenarios.
Prostate-specific membrane antigen (PSMA) PET/CT stages and restages prostate cancer (PCa) with high accuracy (1–3), even at low serum prostate-specific antigen (PSA) levels (3,4). The impact of PSMA PET on the clinical management of PCa patients has been investigated in intermediate- and high-risk disease at initial staging (5–8) and after biochemical recurrence (BCR) (9–15) but not in patients who undergo imaging for other indications. Specifically, the impact on management of patients whose PSA has not risen to or beyond the threshold to define BCR (16,17), those with known metastatic or advanced castration-resistant disease, and those with primary treatments other than surgery or radiation therapy (RT) (i.e., high-intensity focused ultrasound, focal laser ablation, cryoablation, hyperthermia, or irreversible electroporation) is unknown. PSMA PET/CT can also be used to select patients for PSMA-targeted radioligand therapies, as well as for subsequent therapy response evaluations (18).
Here, we report the results of an institutional trial that prospectively evaluated the impact of PSMA PET/CT on the clinical management of PCa patients referred for various indications but ineligible for inclusion in simultaneously accruing trials for patients with BCR (NCT02940262) or patients with intermediate- or high-risk disease before surgery (NCT03368547). On the basis of other studies (10,14), we hypothesized that the proportion of patients whose management is changed as a result of PSMA PET would exceed 40%.
MATERIALS AND METHODS
Study Design and Data Collection
This prospective single-center, open-label, single-arm phase 2 imaging study was approved by the local institutional review board, was registered at clinicaltrials.gov (NCT04050215), and relied on an investigational-new-drug application (130649) for 68Ga-PSMA-11.
The primary objective of the study was to determine the rate of implemented management changes after PSMA PET/CT in a cohort of PCa patients referred for various indications (i.e., a basket trial).
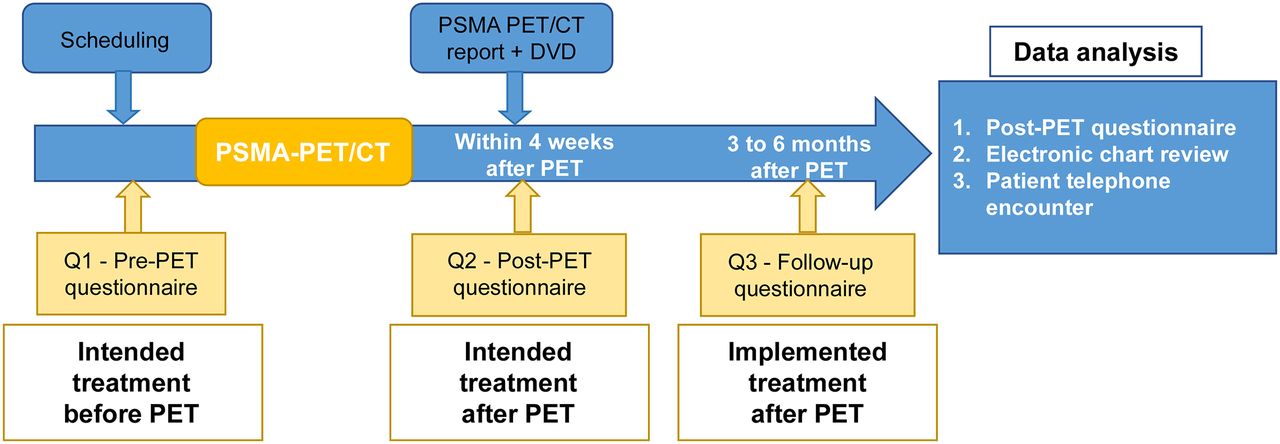
The study design is shown in Figure 1. All referring physicians were asked to complete 3 questionnaires (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). A pre-PET questionnaire and a post-PET questionnaire inquired about the disease stage and intended treatment strategy before and after PSMA PET/CT, respectively. The post-PET questionnaire asked the referring physicians whether any imaging test or diagnostic procedure was avoided or requested after PSMA PET/CT. A follow-up questionnaire determined whether and how the intended management change was altered by PSMA PET/CT and inquired about any other imaging or diagnostic procedures performed within the same time frame. A complete pre-PET questionnaire was required to enroll the patient in the final analysis. The post-PET questionnaire was required within 4 wk, and the follow-up questionnaire was required between 3 and 6 mo after PSMA PET/CT. If the referring physician did not return the post-PET and follow-up questionnaires, the information was derived from a combination of patient chart review and follow-up patient telephone calls.
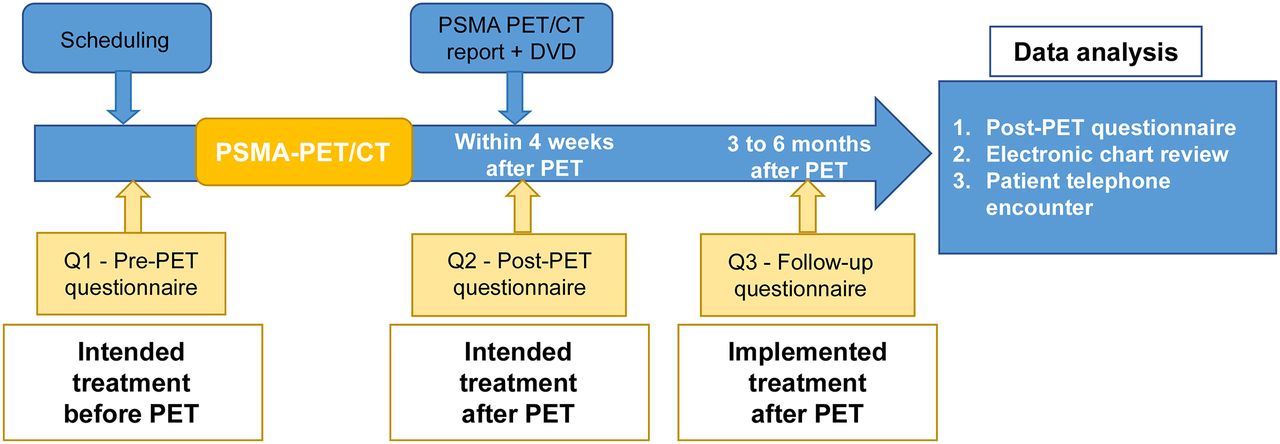
Study design flowchart.
Changes from intended (pre-PET) to implemented (post-PET) management were categorized on the basis of the kind of change or the lack of change in management and stratified by subgroups, as well as changes in staging before and after PSMA PET/CT. Intramodality changes in management were not specifically analyzed. The addition of other imaging or diagnostic procedures within 3–6 mo after PSMA PET/CT was also investigated.
We conducted a post hoc subgroup analysis after stratifying the full cohort by clinical indication, type of initial treatment, and serum PSA level. Changes in stage and detection rate stratified by clinical indication and serum PSA level were assessed. Management change rates across the clinical indication subgroups were compared.
Patients
Patients with histologically proven or strongly suspected PCa (serum PSA level > 50 ng/mL) who required an initial management decision, and patients already treated for PCa (16) and requiring a subsequent treatment decision, were eligible for the study. The latter group included PCa patients with new-onset symptoms or with known metastatic disease, rising PSA level, and negative or inconclusive conventional imaging results; BCR patients who were candidates for salvage therapy; and patients treated medically or with radioligand therapy in whom response to treatment needed to be assessed. Patients eligible for the prospective trials NCT02940262 (post–radical prostatectomy BCR with PSA > 0.2 ng/mL or post-RT BCR with PSA > 2 ng/mL + nadir) and NCT03368547 (initial staging of intermediate- or high-risk disease before intended surgery) were not enrolled in the study. Informed written consent was obtained from all subjects.
The study population included in the final analysis (n = 197) was divided into 6 cohorts for a post hoc subgroup analysis. The first cohort was for initial staging in treatment-naïve patients (castration-sensitive PCa) who were not surgical candidates (n = 30). The second cohort was for restaging after androgen deprivation as primary therapy (n = 16). The third cohort was for restaging after surgery (PSA < 0.2 ng/mL) in castration-sensitive PCa (n = 13). The fourth cohort was for restaging after RT (PSA ≤ 2 ng/mL + nadir) in castration-sensitive PCa (n = 22). The fifth cohort was for restaging after nonconventional primary definitive therapy (i.e., high-intensity focused ultrasound, focal laser ablation, cryoablation, hyperthermia, or irreversible electroporation) in castration-sensitive PCa (n = 13). The sixth cohort was patients with advanced disease (castration-resistant PCa [CRPC]) (n = 103), including patients with known metastatic disease and patients who underwent multiple salvage or second-line therapies.
PSMA PET/CT Image Acquisition and Analysis
68Ga-PSMA-11 PET/CT imaging was performed according to current guidelines, as previously described (18–20). Briefly, 68Ga-PSMA-11 (Glu-NH-CONH-Lys-(Ahx)-[68Ga(HBED-CC)]) was injected 65.5 ± 9.8 min (range, 44–100 min) before image acquisition at a mean activity of 197.95 MBq ± 14.8 (range, 236.8–74 MBq). We acquired images using a 64-detector PET/CT scanner (2007 Biograph 64 TruePoint or 2010 Biograph mCT 64; Siemens). A diagnostic CT scan (200–240 mAs, 120 kV) was performed after administration of oral contrast medium (600 mL of barium sulfate, 2.1% [Readi-Cat 2; Bracco] and intravenous contrast (115 mL of iohexol [Omnipaque; GE Healthcare], 350 mg iodine/mL, injection speed of 2 mL/s, portal venous phase + 80 s after injection) unless contraindicated. The PET image acquisition included a whole-body scan (pelvis to vertex, 2–4 min/bed position depending on the patient weight (21)) and, if deemed necessary by the responsible nuclear medicine physician, a dedicated pelvic scan after voiding (same acquisition time per bed position as used for the whole body). All PET images were reconstructed using correction for attenuation, dead time, random events, and scatter. PET images were reconstructed with an iterative algorithm (ordered-subset expectation maximization) in an axial 168 × 168 matrix on the Biograph 64 TruePoint (2-dimensional, 2 iterations, 8 subsets, 5.0-mm gaussian filter) and in a 200 × 200 matrix on the Biograph mCT 64 (3-dimensional, 2 iterations, 24 subsets, 5.0-mm gaussian filter).
Images were interpreted during clinical rounds by a consensus reading by a board-certified nuclear medicine physician and a board-certified radiologist as routinely done in our clinic.
PSMA PET/CT findings were reported as follows: any focal uptake of 68Ga-PSMA-11 above background level, not associated with physiologic uptake or known pitfalls (19,22), was considered PSMA-positive. Additionally, a PSMA PET–based TNM staging system (Prostate Cancer Molecular Imaging Standardized Evaluation) was used, as done routinely in our clinic (20).
Statistical Analysis
Sample Size Calculation
This study was designed to provide more than 90% power to determine whether the proportion of patients whose management is changed as a result of PSMA PET/CT exceeds 40%, assuming an exact binomial test and a 1-sided α of 0.025. Further, a sample size of 200 patients is expected to produce a margin of error of 6.9% for the proportion of patients with implemented management change, assuming a 2-sided 95% confidence level.
Post Hoc Subgroup Analysis
The planned sample of 200 patients provides 80% power to detect effect sizes between pairs of study arms ranging from 0.59 to 1.12 SD, assuming a 2-sample t test and a 0.05 2-sided significance level.
Descriptive statistics were used to characterize the population and the rates of changes in stage and management for the full cohort and among the subgroups. Quantitative variables were described using means, SDs, and ranges. Categoric variables were summarized using frequencies and percentages. Comparisons between subgroups were performed using 1-way ANOVAs for the quantitative variables and Fisher exact tests for the categoric variables. P values of less than 0.05 were considered statistically significant. Analyses were performed using R, version 3.5.0 (http://www.r-project.org/).
RESULTS
Patient Population and Questionnaires
In total, 234 patients were enrolled between April 2018 and January 2019. Of these, 197 (84%) were included in the final analysis. Thirty-seven patients were excluded because of an incomplete pre-PET questionnaire (n = 14) or because they were lost to follow-up (n = 23).
Patient and subgroup characteristics and are summarized in Table 1. The post-PET questionnaire was available for only 53 of the 197 patients (27%), and the follow-up questionnaire was available for 65 (33%). Because of the low rate of returned post-PET questionnaires and difficulty in recovering the interim information derived from it, data on intended management from the post-PET questionnaire were excluded from the final analysis. Follow-up information was collected from electronic chart review or direct patient contact for 132 of the 197 patients (77%).
Patient Characteristics
Detection Rate and Location of Disease
PSMA PET/CT detection rates varied significantly among subgroups (P < 0.001). The detection rate was 166 of 197 (84%) for the whole cohort. It was lowest in patients restaged after radical prostatectomy with a PSA level of 0.2 ng/dL or less 1/13 (8%), and it ranged from 84% to 100% in the other subgroups (Table 2; Supplemental Fig. 2). Disease location stratified by subgroups is shown in Supplemental Figure 3.
Study Result Summary
Changes in Stage
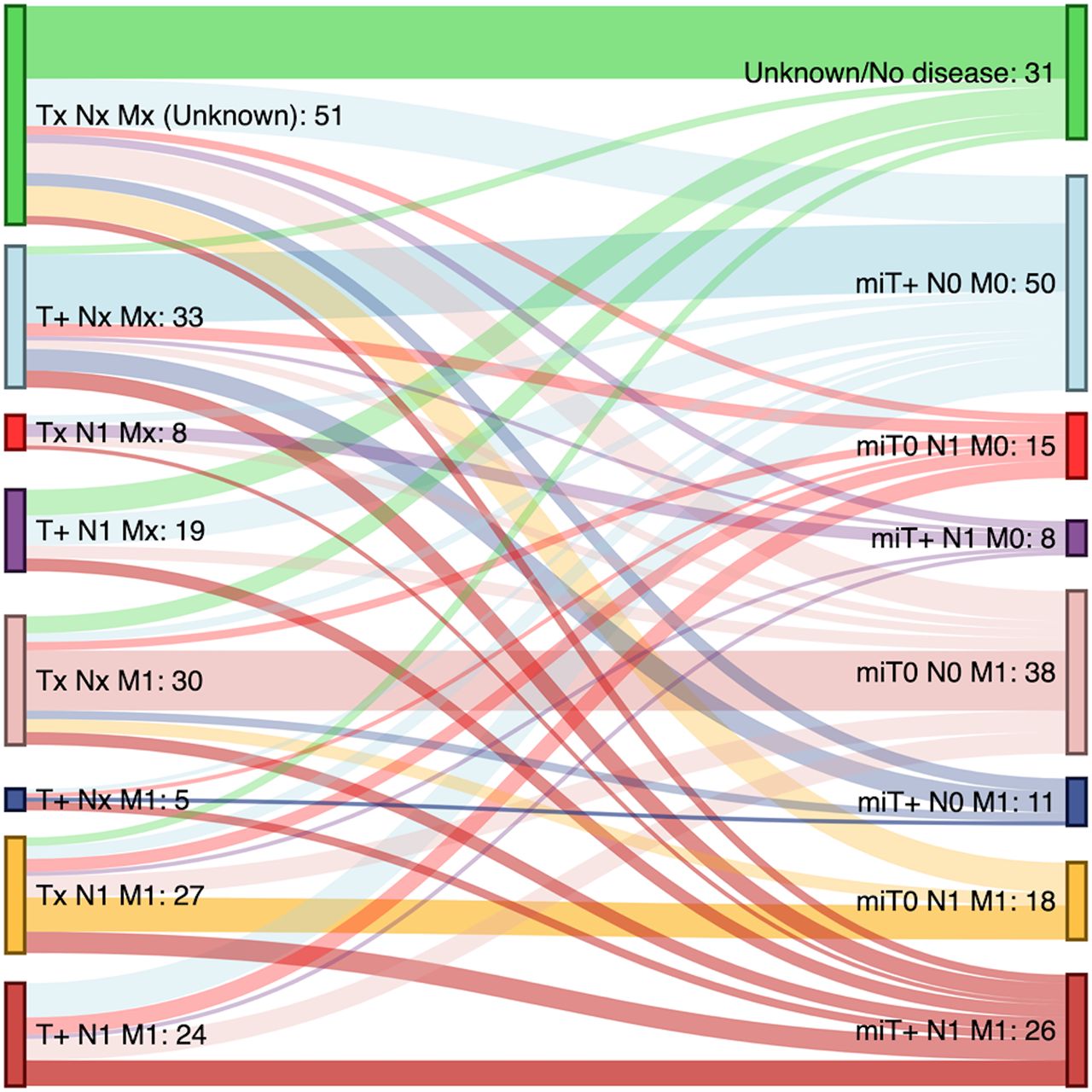
The pre-PET stage as determined by the referring physicians changed after PSMA PET/CT in 135 of the 197 patients (69%) (Table 2; Figs. 2 and 3). PSMA PET/CT upstaged 75 of the 197 patients (38%), downstaged 59 (30%), and had no effect on stage in 63 (32%).
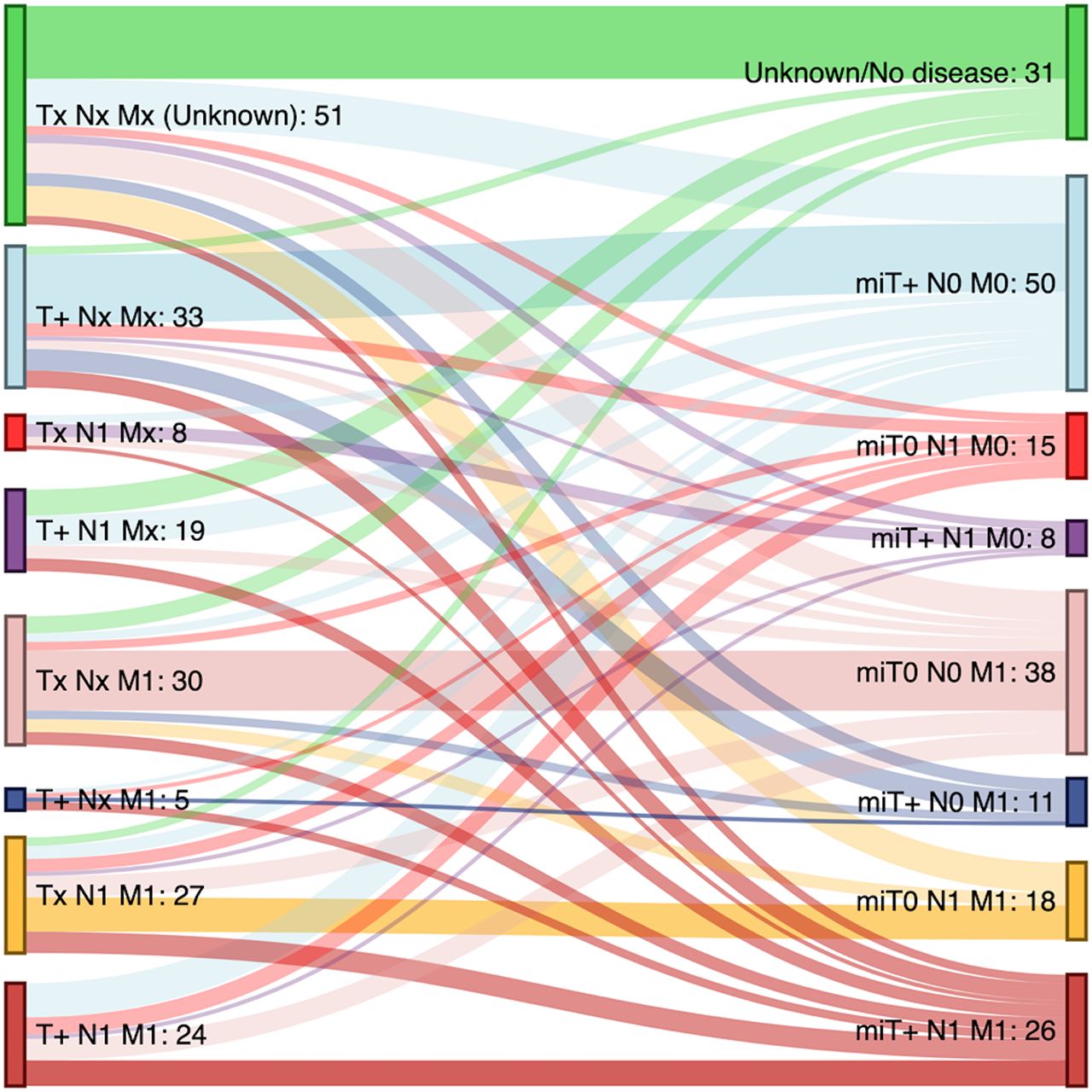
Impact of PSMA PET/CT imaging on staging of PCa. Sankey diagram showing per-patient differences in staging or restaging of disease before (left) and after (right) PSMA PET/CT. Staging of disease before PSMA PET/CT was indicated by referring physician on pre-PET questionnaire, staging after PSMA was based on PSMA PET/CT results (T+ = presence of disease in prostate/prostate bed on PSMA PET/CT; 1 = presence of disease in location on PSMA PET/CT). Sixty-two (31%) patients had no change in staging, and 135 (69%) patients had change in staging. On Sankey diagram, each color of vertical bars indicates same TNM or molecular imaging TNM staging, color of flow reflects color of destination, and darker color in each flow indicates no changes in stage.

Changes in stage of disease before and after PSMA PET/CT stratified by subgroup.
Rates of stage changes did not differ significantly among subgroups (P = 0.081). The post-RT restaging cohort had the highest rates of stage change (19/22 [86%]) and upstaging (13/22 [69%]). However, PSMA PET/CT also changed the stage frequently in the other subgroups (ranging from 67% to 81%). As expected, the lowest impact on stage occurred in the postsurgery subgroup with serum PSA levels of 0.2 ng/mL or less (5/13 patients, 38%, all downstaged) (Fig. 3).
Changes in Management
Change-in-management data were available in 182 of the 197 patients (92% of the full cohort) (Table 2). Management was changed by the PSMA PET/CT findings in 104 of 182 patients (57%) but was not affected in 78 (43%) (Fig. 4; Supplemental Table 1).

Impact of PSMA PET/CT imaging on management stratified by clinical indication. Both focal and systemic treatments are intended with or without androgen deprivation therapy (ADT). ADT as monotherapy was considered systemic treatment. AS = active surveillance.
Rates of management changes did not differ significantly among subgroups (P = 0.183). The subgroups for restaging after RT (13/18 [72%]) and restaging after other definitive treatment (8/12 [67%]) experienced the most frequent management changes. The subgroups for restaging after androgen deprivation therapy, restaging after surgery, and restaging with advanced disease had management changes in 6 of 15 (40%), 6 of 13 (46%), and 59 of 96 (61%) patients, respectively. Management changes occurred in 12 of 28 (43%) treatment-naïve patients (Supplemental Table 1).
The most common changes in management in the full cohort were conversion from systemic to focal treatment (29/182 patients [16%]) and changes in focal treatments (19/182 patients [10%]). A detailed analysis of management changes stratified by stage change is shown in Supplemental Figure 4. An example of the impact on management is shown in Supplemental Figure 5.
Imaging and Other Diagnostic Procedures
No additional imaging or diagnostic procedure was performed within 3–6 mo after PSMA PET/CT in 128 of the 197 patients (64%), whereas MRI was performed in 36 (18%), PET with PSMA or different radiotracer in 16 (8%), CT in 12 (6%), biopsy in 13 (6%), and bone scanning in 9 (4%).
DISCUSSION
The impact of PSMA PET/CT on therapeutic decisions has been reported comprehensively for PCa patients with BCR (9–15) and those who underwent presurgical staging (5–8). Here, we prospectively studied the impact of 68Ga-PSMA-11 PET/CT on the stage and management of PCa patients with other clinical indications. We stratified the analysis on the basis of clinical indications to evaluate how PSMA PET/CT impacts the management of PCa patients in different clinical scenarios. The primary endpoint of the study was met, with a 57% (>40%) rate of management change in the entire cohort (14). This finding confirms the impact of PSMA PET/CT on clinical decisions beyond the 2 main classic indications: BCR and presurgical staging.
Patients restaged after RT who did not meet the Phoenix criteria for BCR (PSA ≤ 2 ng/mL + nadir) (16) seem to be those who benefit most from PSMA PET/CT. PSMA PET/CT detected PCa recurrence in 86% of these patients who were not supposed to have BCR per definition. In this cohort, we found the highest rates of change in stage and management (86% and 72%, respectively). Our findings suggest that recurrence after RT may need to be redefined and that this cohort may benefit from PSMA PET imaging.
In patients restaged after other nonconventional definitive treatments, the PSMA PET/CT detection rate was 100% and impacted management in 67% of patients. Excepting one who underwent active surveillance, all received focal lesion treatment identified by PSMA PET/CT.
In patients restaged with advanced or metastatic disease, PSMA PET/CT had a high detection rate (84%) and impacted management in 61%. Because of the heterogeneity of the cohort, a wide range of management changes was induced by PSMA PET/CT. Consistent with other reports, management changed most frequently from intended systemic to implemented focal treatment (10,13,14). This finding highlights that high lesion detection rates can lead to focal (metastasis-targeted) treatment. Whether this approach will affect patient outcomes needs to be determined in future prospective studies.
Detection rates were lowest (1/13 patients [8%]) in patients restaged after definitive surgery who had serum PSA levels of 0.2 ng/mL or less. The impact on patient stage was also lowest in this group (38%), but changes in management still occurred in 6 of 13 (46%) of these patients. Despite the small size of the subgroup (only 13 subjects), these findings suggest that this population with an early stage of disease and a very low tumor burden may not benefit from the current imaging techniques.
In the 2 subgroups of patients who did not undergo definitive treatment, that is, treatment-naïve patients at initial staging who were not surgical candidates and those who underwent androgen deprivation therapy as first-line monotherapy after PCa diagnosis, PSMA PET/CT had a detection rate of 100% and induced changes in stage in 67% and 81% of patients, respectively. However, changes in management occurred less frequently in these 2 subgroups than in all others (43% and 40%, respectively). This finding may be explained by the limited treatment options in these cohorts. The primary tumor had not been treated, and most patients were scheduled to undergo a definitive focal treatment after the scan. After PSMA PET/CT, the treatment plan either remained the same (no changes in focal therapy in most cases) or there was a change in focal treatment (Fig. 4).
Müller et al. (13) found that metastasis-targeted treatments in patients with BCR with PSMA PET/CT–positive lesions resulted in a complete biochemical response in 45% of patients within 6 mo after PSMA PET/CT. Since a large proportion of the patients involved in our study were not treated in our hospital, we could not assess the clinical impact of PSMA PET/CT on patient outcome. Also, whether the PSMA PET/CT–induced management changes translate into survival benefits remains unknown. Prospective studies with long-term follow-up are required to answer this question.
The low rate of returned postscan questionnaires is a major limitation of this study. Patients were referred from multiple outside institutions, and physicians’ interest in sending back paperwork decreased dramatically after the scan. With only 27% of post-PET questionnaires available, we were not able to include in the analysis the postscan intended management (intended management can be obtained only prospectively). Late follow-up questionnaires were returned for only 33% of patients. We were able to overcome this limitation by determining the final implemented management through electronic chart review or patient telephone calls for 132 of the 197 (77%) patients. The critical information that must be obtained prospectively is the prescan intended management, which was systematically obtained for all included patients. However, we acknowledge that telephone calls with patients are not a reliable source of medical information and do not allow a detailed analysis of intramodality changes, (i.e., changes in the radiation field, surgical approach, or androgen deprivation therapy regimen). Therefore, these cases were considered as “no change in focal or systemic therapy,” but they still indicate changes attributable to information derived from PSMA PET/CT. The lack of information on how PSMA PET/CT altered specific intramodality treatment represents a limitation of our study because it underestimates the reported changes in management. This issue needs to be further addressed by dedicated prospective studies of each treatment modality.
Another limitation of the study is the lack of histopathologic validation of the PSMA-positive lesions. Obtaining a firm reference standard in recurrent PCa is a well-known challenge, even in prospective studies. Thus, false-positive findings cannot be ruled out. However assessing PSMA PET/CT diagnostic performance was not the aim of this study. Of note, high positive predictive values for PSMA PET (>85%) were reported in a metaanalysis that included only patients with BCR with histopathologic verification (23) and in a prospective multicenter phase 3 trial (3).
Despite the differences in stage and management changes that were observed among subgroups, they did not reach statistical significance. Although the heterogeneity of the population is a strength of our basket study, dividing the full cohort into 6 subgroups reduced the size of the subcohorts. The initial sample size calculation was not powered to evaluate differences in rates of change between indications. Because some subgroups were small, changes in management should be interpreted with caution. Therefore, the results need to be further explored in larger prospective trials for each of the subpopulations and clinical indications.
One final limitation of the study is that some of our patients had varying conventional imaging and diagnostic procedures performed before—and in 36% of cases after—the protocol PSMA PET/CT; the postprotocol procedures may have affected patient management.
CONCLUSION
PSMA PET/CT significantly impacted the stage and management of PCa patients across all relevant clinical scenarios, beyond the 2 main classic applications in BCR and presurgical staging. Further prospective studies need to determine whether these changes in management ultimately result in improved patient outcomes.
DISCLOSURE
This was an investigator-initiated trial with institutional academic funding (Ahmanson Translational Theranostics Division, Department of Molecular and Medical Pharmacology, UCLA). Jeremie Calais was the recipient of a grant from the Philippe Foundation Inc. and from the Fondation ARC pour la recherche sur le cancer (grant SAE20160604150), received personal fees from Progenics Pharmaceuticals and RadioMedix, and is a consultant for Blue Earth Diagnostics outside the submitted work. Johannes Czernin was the recipient of a grant from the U.S. Department of Energy (DE SC0012353), from the Prostate Cancer Foundation (2019 and 2017 Challenge Award, 17CHAL02), and from the Johnson Comprehensive Cancer Center National Institutes of Health–National Cancer Institute Cancer Center (support grant P30 CA016042). He is a founder and board member and holds equity in Sofie Biosciences and Trethera Therapeutics and serves on the medical advisory board of Actinium outside the submitted work. Wolfgang P. Fendler was the recipient of a scholarship from the German Research Foundation (Deutsche Forschungsgemeinschaft grant) and is a consultant for Endocyte and Ipsen. He received personal fees from RadioMedix outside the submitted work. Mattias Eiber was supported by the SFB 824 (DFG Sonderforschungsbereich 824, project B11) from the Deutsche Forschungsgemeinschaft and received grants from ABX Advanced Biochemical Compounds and Blue Earth Diagnostics. He is a consultant for Janssen, received personal fees from Progenics Pharmaceuticals, and has a patent rhPSMA issued outside the submitted work. Matthew B. Rettig received research grants from Novartis, Johnson and Johnson, Merck, Astellas, Medivation, and Progenics. He is a consultant for Constellation Pharmaceuticals and a member of the speakers bureau for Johnson and Johnson and Bayer. Amar U. Kishan received personal fees from ViewRay, Inc., Varian Medical Systems, Inc., and Janssen Pharmaceuticals outside the submitted work. Nicholas Nickols received research support from Janssen, Varian, and Progenics. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does PSMA PET/CT have an impact on the clinical management of PCa patients referred for indications other than BCR or presurgical staging?
PERTINENT FINDINGS: This prospective single-center, open-label, single-arm phase 2 imaging trial showed that PSMA PET/CT significantly impacts the stage and management of PCa patients across all relevant clinical scenarios.
IMPLICATIONS FOR PATIENT CARE: The results of this study demonstrate that PSMA PET/CT can be used in PCa patients in a wide variety of clinical settings other than BCR and presurgical staging, significantly impacting clinical staging and management.
Acknowledgments
We thank all the patients and their referring physicians, whose willingness to participate made this study possible. We thank the whole staff team of the UCLA Nuclear Medicine and Theranostics Division, whose hard work made this study possible.
Footnotes
Guest editor: Todd Peterson, Vanderbilt University.
Published online Jan. 10, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 1, 2019.
- Accepted for publication December 17, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Factors That Influence Repeat 68Ga-PSMA-11 PET/CT Scan Positivity in Patients with Recurrent Prostate Cancer Under Observation After a Negative 68Ga-PSMA-11 PET/CT Scan: A Single-Center Retrospective Study
- Single Chelator-Minibody Theranostic Agents for 89Zr PET Imaging and 177Lu Radiopharmaceutical Therapy of PSMA-Expressing Prostate Cancer
- Impact of 68Ga-FAPI PET/CT on Staging and Oncologic Management in a Cohort of 226 Patients with Various Cancers
- Delayed Imaging Improves Lesion Detectability in [99mTc]Tc-PSMA-I&S SPECT/CT in Recurrent Prostate Cancer
- Staging Prostate Cancer with 68Ga-PSMA-11 PET/CT in the Elderly: Is Preimaging Biopsy Imperative?
- 177Lu-PSMA Therapy
- 18F-rhPSMA-7 PET for the Detection of Biochemical Recurrence of Prostate Cancer After Curative-Intent Radiation Therapy: A Bicentric Retrospective Study
- Assessing the Correlation Between 68Ga-PSMA-11 Renal PET Parameters and Renal Function Tests
- Renal Cortical Scarring: 68Ga-PSMA-11 PET Versus 99mTc-DMSA Scanning in a Case of Pyelonephritis
- Diagnostic Performance and Clinical Impact of 68Ga-PSMA-11 PET/CT Imaging in Early Relapsed Prostate Cancer After Radical Therapy: A Prospective Multicenter Study (IAEA-PSMA Study)
- A Phase II, Open-Label Study to Assess Safety and Management Change Using 68Ga-THP PSMA PET/CT in Patients with High-Risk Primary Prostate Cancer or Biochemical Recurrence After Radical Treatment: The PRONOUNCED Study
- Detection Efficacy of 18F-rhPSMA-7.3 PET/CT and Impact on Management in Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy and Before Potential Salvage Treatment
- Reply: PSMA-Targeted Therapeutics: A Tale About Law and Economics
- Identification of PCWG3 Target Populations Is More Accurate and Reproducible with PSMA PET Than with Conventional Imaging: A Multicenter Retrospective Study
- Renal Cortical 68Ga-PSMA-11 PET and 99mTc-DMSA Images
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy