


Article Figures & Data
Figures
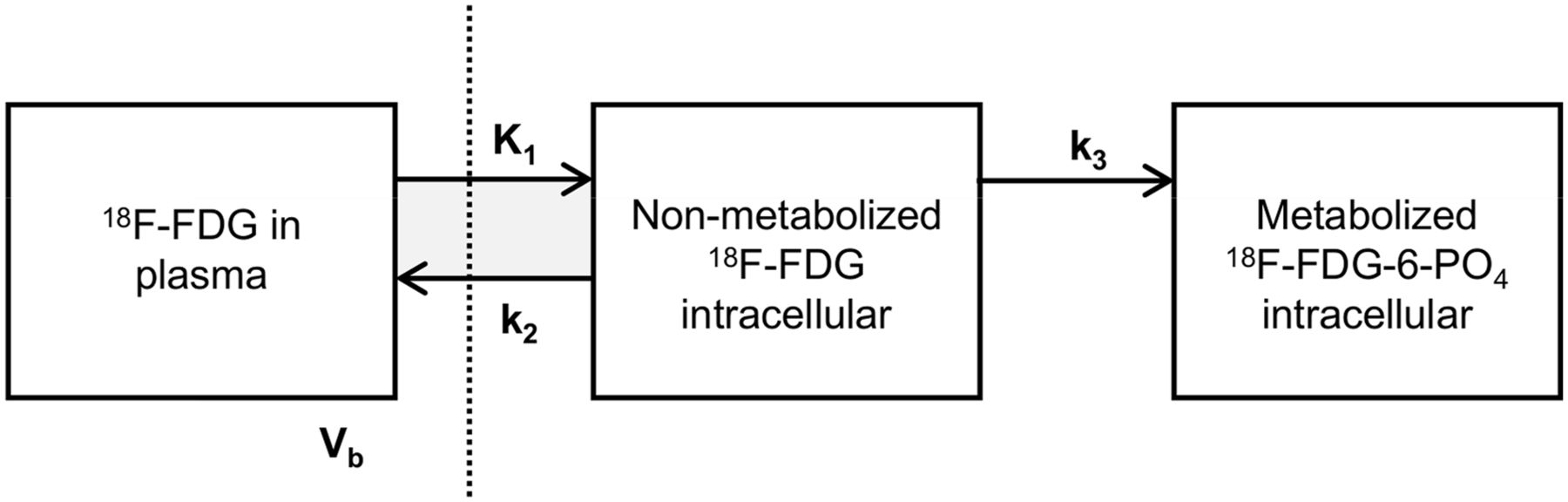
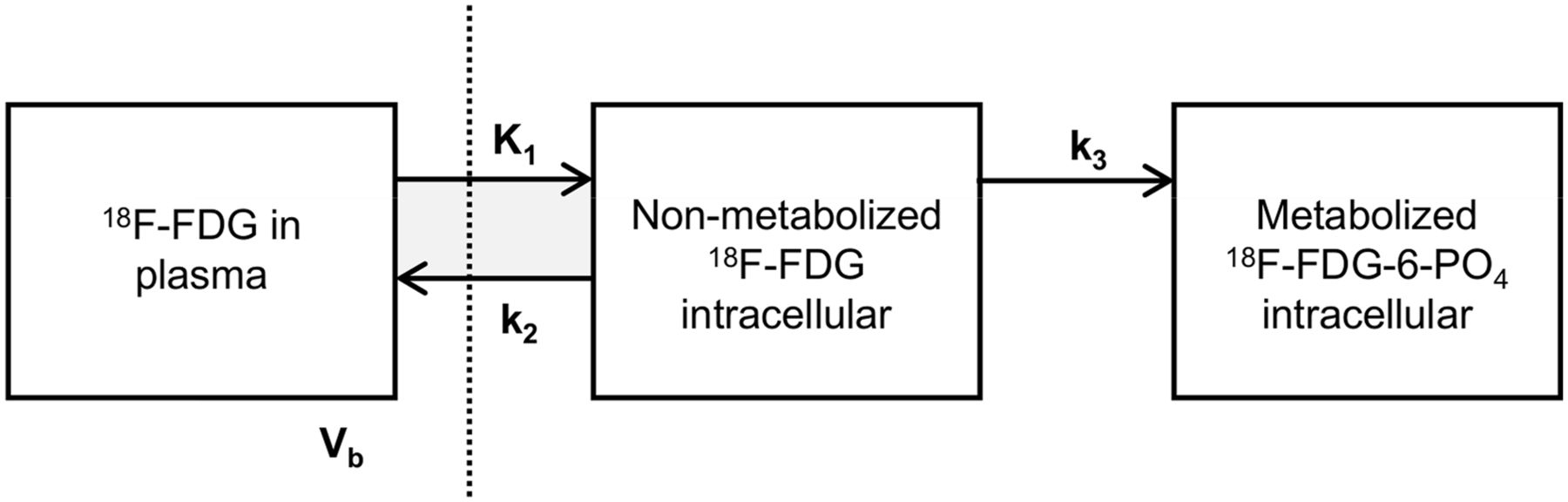
- FIGURE 1.
Irreversible 2-tissue-compartment model for 18F-FDG metabolism. Measured PET signal is combination of intracellular activity concentration of free 18F-FDG (nonmetabolized 18F-FDG in tissue), intracellular activity concentration of 18F-FDG-6-phosphate (metabolized 18F-FDG-6-PO4 in tissue), and fraction of activity concentration of 18F-FDG in blood plasma (Vb). By using dynamic PET/CT, pharmacokinetic rate-constants K1 and k2 (rate constants of transport of 18F-FDG into and out of tumor cell by glucose transporters, in mL/g/min), k3 (rate constant of cytoplasmic phosphorylation of 18F-FDG by hexokinase, per minute), and Vb (in milliliters of blood per milliliter of tumor) can be determined using nonlinear least-squares regression of dynamic PET/CT data. Vertical dashed line represents cell membrane
- FIGURE 2.
Dynamic 18F-FDG PET/CT results in patient 24, with primary sporadic PPGL in left adrenal. (A) Parametric image of MRglc from dynamic 18F-FDG PET scan. (B) Static 18F-FDG PET/CT scan. (C) CT scan. (D) Image-derived input function and tumor time–activity curve. (E) Patlak plot. Slope of Patlak plot equals influx constant Ki
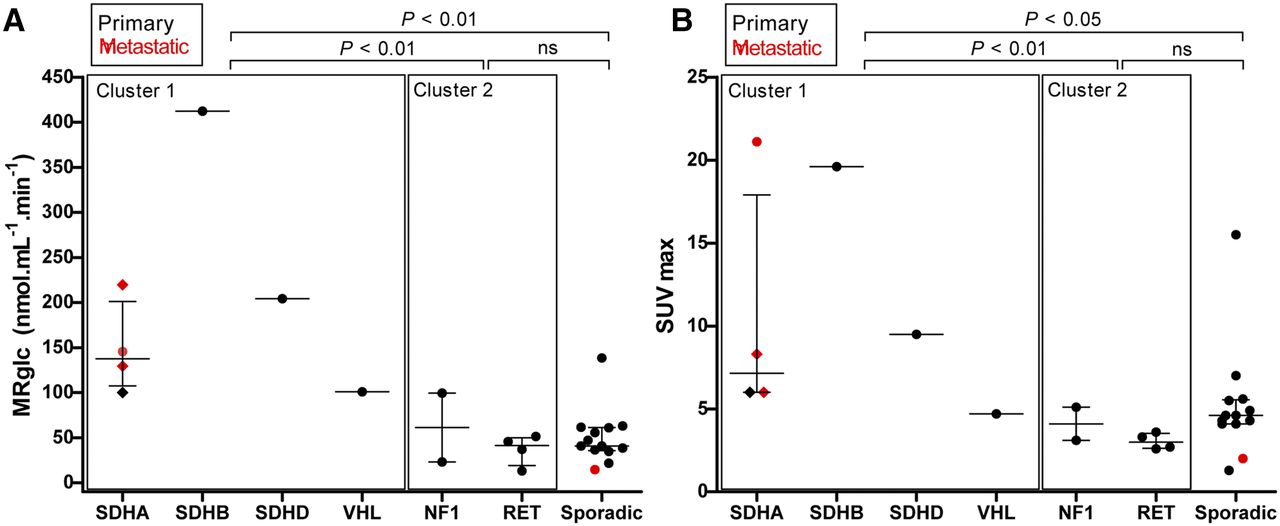
- FIGURE 3.
Scatterplots showing MRglc (A) and 18F-FDG SUVmax (B) in PPGLs across different genotypes. Horizontal bar represents median and interquartile range. Diamonds represent 3 different tumor locations in same patient (patient 7, Table 1). All SUVs are normalized for body weight and decay. P values are from Kruskal–Wallis with Dunn post hoc testing, and groups are compared as indicated. ns = not significant.
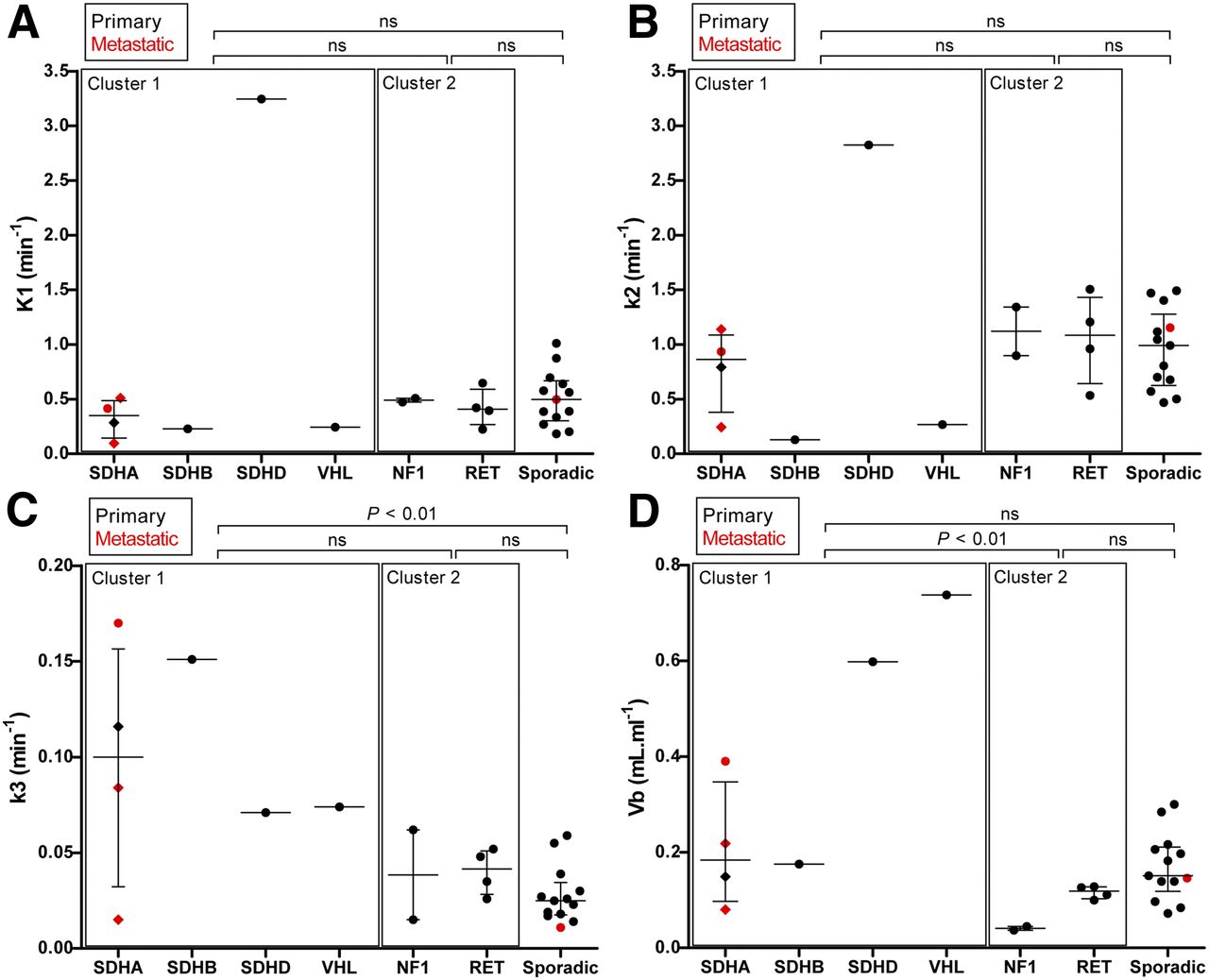
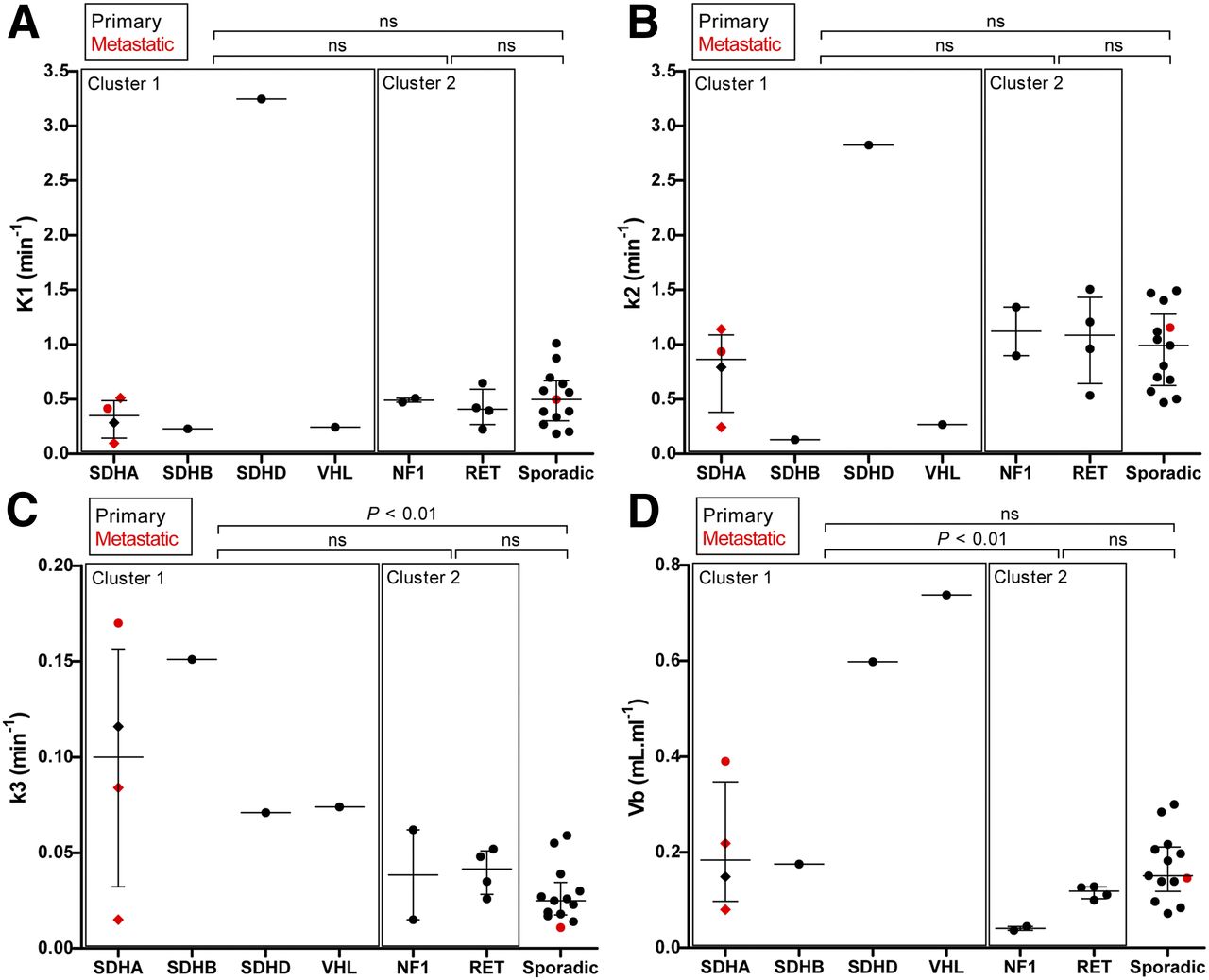
- FIGURE 4.
Pharmacokinetic rate-constants (K1, k2, and k3) and blood volume fraction (Vb) in PPGLs across different genotypes. Horizontal bar represents median and interquartile range (IQR). Diamonds represent 3 different tumor locations in same patient (patient 7). P values are from Kruskal–Wallis with Dunn post hoc testing, and groups are compared as indicated. ns = not significant.
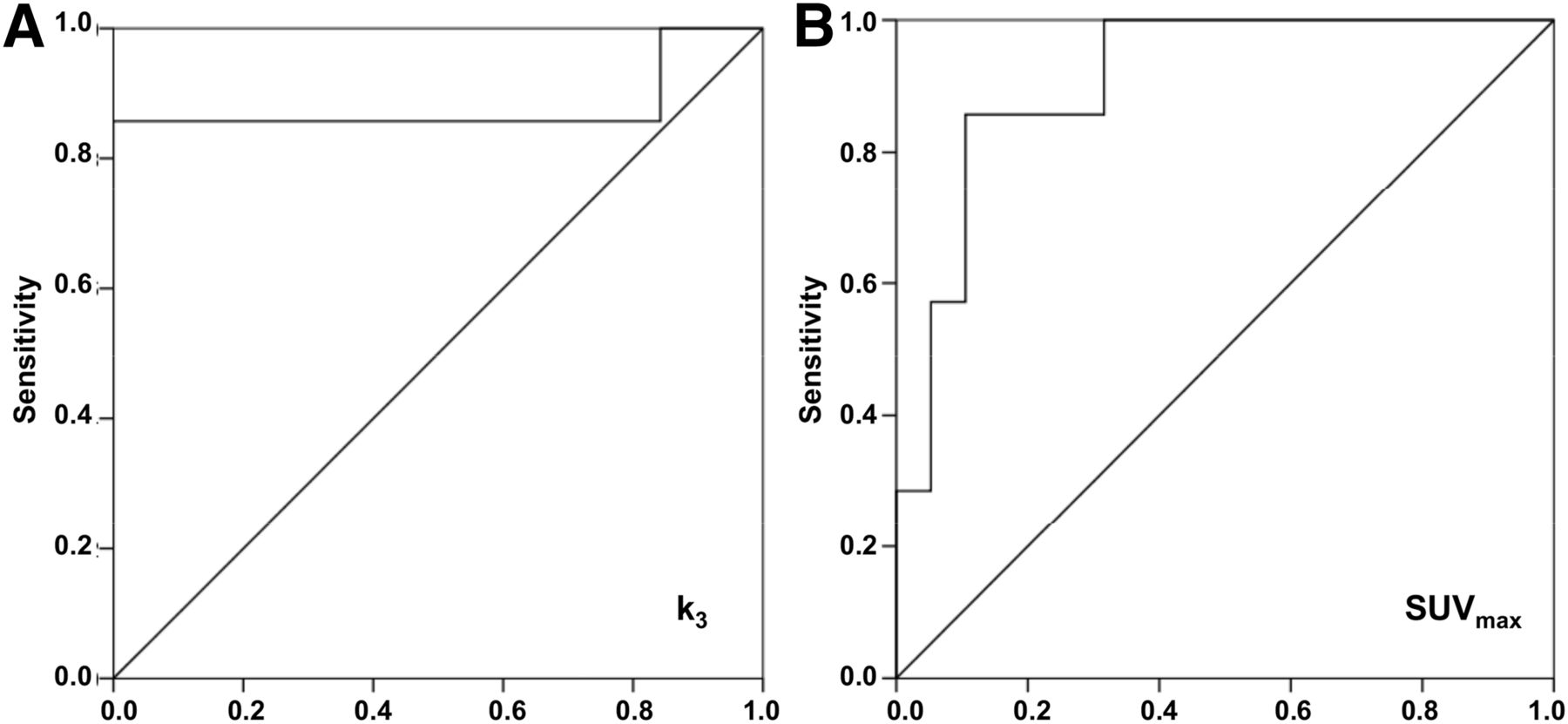
- FIGURE 5.
Receiver-operating-characteristic curve for pharmacokinetic rate-constant k3 (A) and SUVmax (B). This curve was constructed from k3 and SUVmax of cluster 1 tumors vs. other (cluster 2 and sporadic) tumors in patients with PPGL. Diagonal line represents line of no discrimination.



Tables
Patient no. Sex Genotype Age (y) Tumor location Status Maximum tumor diameter (cm) Biochemical phenotype 1 M NF1 66 LA Primary 1.2 E + NE 2 F NF1 31 LA Primary 4.0 E + NE 3 F RET 62 LA Primary 3.4 E + NE 4 F RET 20 RA Primary 3.5 E + NE 5 M RET 35 RA Primary 2.1 E + NE 6 M RET 70 LA Primary 3.0 E 7 F SDHA 63 LA Primary NA NE + DA EA (thoracic spine) Metastatic NA NE + DA EA (paraaortic lymph node) Metastatic NA NE + DA 8 M SDHA 35 EA (retroaortic lymph node) Metastatic NA DA 9 M SDHB 46 EA (dorsolateral bladder) Recurrent NA NE + DA 10 M SDHD 64 RA Primary 1.5 NE + DA 11 M VHL 48 RA Primary 2.2 NE 12 F Sporadic 55 LA Primary 11.0 E + NE 13 F Sporadic 34 RA Primary 5.0 E + NE 14 M Sporadic 51 EA (retrocaval lymph node) Metastatic 2.0 NE 15 F Sporadic 33 LA Primary 4.0 E + NE 16 F Sporadic 56 EA (paraaortic lymph node) Primary 1.4 NE 17 M Sporadic 66 LA Primary 1.8 E 18 M Sporadic 85 RA Primary NA NE 19 M Sporadic 55 LA Primary 3.5 E + NE 20 M Sporadic 43 LA Primary 10.0 E + NE 21 F Sporadic 73 LA Primary 12.5 NE + DA 22 F Sporadic 55 RA Primary 1.5 E 23 M Sporadic 64 RA Primary 5.0 E + NE 24 F Sporadic 55 LA Primary 6.0 E + NE LA = left adrenal; RA = right adrenal; EA = extraadrenal; NA = not available; E = epinephrine; NE = norepinephrine; DA = dopamine.
Parameter All tumor lesions (n = 26) Primary tumors (n = 22) Metastases (n = 4) MRglc (nmol⋅mL−1⋅min−1) 53.6 (13.2–412.4) 49.4 (13.2–412.4) 137.6 (14.6–219.8) SUVmax (g⋅cm−3) 4.7 (1.3–21.1) 4.6 (1.3–19.6) 7.1 (2.0–21.1) K1 (mL⋅g−1⋅min−1) 0.42 (0.10–3.25) 0.41 (0.18–3.25) 0.46 (0.96–0.51) k2 (min−1) 0.95 (0.13–2.82) 0.93 (0.13–2.83) 1.04 (0.24–1.15) k3 (min−1) 0.032 (0.011–0.170) 0.032 (0.014–0.151) 0.049 (0.011–0.170) Vb (mL⋅mL−1) 0.148 (0.037–0.738) 0.144 (0.037–0.738) 0.182 (0.080–0.390) Data are median followed by range in parentheses. No significant differences were observed between 2 groups (Mann–Whitney U test).
Rate constant Hereditary cluster 1 tumors (SDHx, VHL) (n = 7) Hereditary cluster 2 tumors (RET, NF1) (n = 6) Sporadic tumors (n = 13) K1 (mL⋅g−1⋅min−1) 0.28 (0.10–3.25) 0.44 (0.23–0.65) 0.50 (0.18–1.01) k2 (min−1) 0.79 (0.13–2.82) 1.08 (0.54–1.50) 0.99 (0.47–1.49) k3 (min−1) 0.084 (0.015–0.170)* 0.041 (0.015–0.062) 0.025 (0.011–0.059) Vb (mL⋅mL−1) 0.219 (0.080–0.738)† 0.105 (0.037–0.128) 0.151 (0.072–0.300)
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.