


Abstract
1762
Objectives: Enhanced time-of-flight (TOF) timing resolution with silicon photomultiplier array (SiPM) technology coupled with point response function (PRF) and regularized reconstructions (RR) are creating a new generation of PET scanners with unprecedented signal-to-noise characteristics. Commercial options for some of these scanners allow for 3, 4, or 5 detector ring configurations with substantially different sensitivities. Although sensitivities associated with 4 or 5-ring systems (20-25 cm axial field of view (FOV)) allow for unprecedented throughput opportunities, 3-ring systems with advanced reconstructions may provide an affordable entry into the high-performance world of SiPM PET/CT. The objective of this work is to compare clinical image quality (noise and SUVmax measurements) of 15 clinical oncology patients acquired on both a clinical 3-ring and 4-ring SiPM array PET/CT system reconstructed with standard and advanced reconstructions.
Methods: 15 oncology subjects were injected with FDG and imaged on a 4-ring PET/CT system for 4 min. per bed position using list mode acquisition. Subsequently, a detector ring was removed, the scanner was fully recalibrated, and 14 subjects returned for a follow-up 4 min. per bed position list mode acquisition on the 3-ring system. Paired injected doses were within ± 5% and uptake times within ± 2 min. of original scan. For both the 3 and 4-ring systems, the list mode data was replayed to simulate 1, 2, 3, and 4 minutes per bed position acquisitions. Images were reconstructed using a 3D OSEM reconstruction with TOF, a PRF, and a RR, resulting in 12 image sets per subject per scanner configuration. To characterize noise properties, 7 30mm spherical VOIs were placed in uniform regions of the liver. SUVmean and standard deviation (SD) of voxels were calculated. The 7 coefficient of variations (SD/SUVmean, COV) were averaged to generate a single metric representative of image noise. COVs were calculated as a function of acquisition time and reconstruction approach to quantitatively determine at what min/bed position a 3-ring system matched the noise characteristics of a 4-ring system, and to what extent advanced reconstructions could compensate. Those subjects with positive clinical FDG scans (n=7) each had up to 5 positive index lesions assessed for SUVmax (n=18 lesions total) for each reconstruction as a metric for image signal.
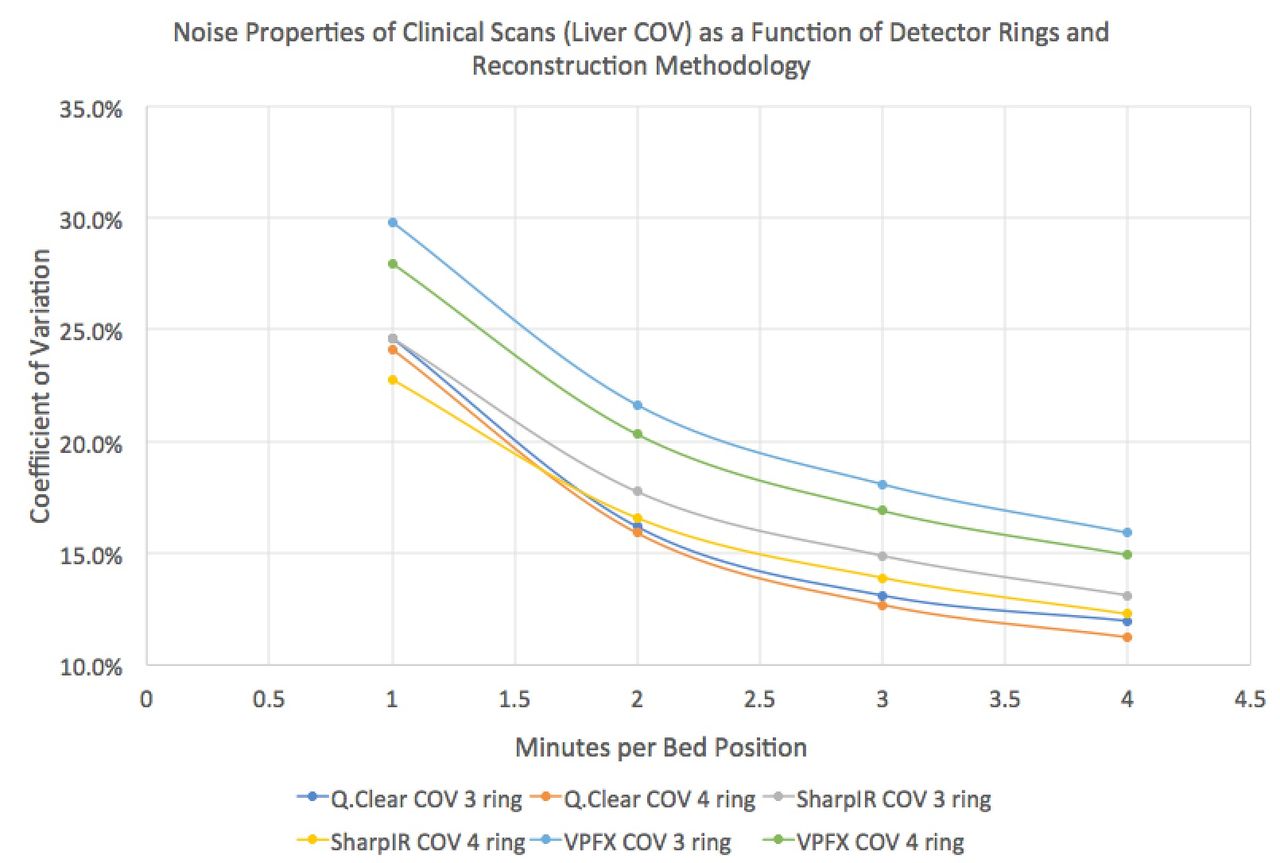
Results: Under no conditions were 1 min scans of acceptable image quality. All images on both systems collected for more than 3 minutes were, subjectively, of excellent quality. COVs in the liver for the 3 and 4-ring scanner systems several reconstructions are plotted as a function of min. per bed position in the figure below. Adding approximately 30 seconds per bed position to an OSEM or PRF reconstruction on a 3-ring system results in comparable image noise characteristics to a 4-ring system. However, the limited axial FOV of the 3-ring system requires approximately 1.5x more bed positions for similar coverage. Total scan time, therefore, is substantially higher to achieve identical image quality. RR, however, has virtually identical COV properties on the 3 and 4-ring systems, suggesting successful noise suppression; however, the 1.5X time penalty remains. PRF reconstructions appear to buy 1 minute per bed position for similar COV characteristics. A 3-ring system equipped with RR at 2:40 seconds per bed position results in a COV superior to a 4-ring system operating with OSEM and TOF at 4 minutes per bed position (identical total scan times). PRF reconstructions also boosted SUVmax values 14±7%, and RR an additional 12±9%, adding additional lesion conspicuity.
Conclusions: Expected noise penalties associated with a 3-ring SiPM array PET/CT scanner vs. a 4-ring system have been characterized on 14 FDG oncology studies. Advanced reconstructions substantially improve noise properties and lesion conspicuity that result in excellent image quality on both 3 and 4-ring SiPM systems.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.