


Abstract
Clinical PET studies using 18F-THK5351 have demonstrated significant tracer retention in sites susceptible to tau burden in Alzheimer disease (AD). However, the in vivo PET signal to reflect tau aggregates remains controversial. Methods: We examined the spatial pattern of tracer binding, amyloid-β, tau, and gliosis in an autopsy-confirmed AD patient who underwent 18F-THK5351 and 11C-Pittsburgh compound B PET before death. Results: Regional in vivo 18F-THK5351 retention was significantly correlated with the density of tau aggregates in the neocortex and monoamine oxidase-B in the whole brain, but not correlated with that of insoluble amyloid-β. Furthermore, significant association was observed between the density of tau aggregates, monoamine oxidase-B, and glial fibrillary acidic protein, suggesting that neocortical tau would strongly influence the formation of reactive astrocytes. Conclusion: 18F-THK5351 PET may have limited utility as a biomarker of tau pathology in AD; however, it could be used to monitor the neuroinflammatory processes in the living brain.
In vivo imaging of tau pathology would provide new insights into the pathogenesis of several neurodegenerative diseases, including Alzheimer disease (AD) (1,2). Recent efforts to develop tau-specific PET radiopharmaceuticals produced several promising candidates, including quinoline derivatives designed to detect tau aggregates (1,3,4). Clinical PET studies have demonstrated elevated tracer retention predominantly in the temporal cortex in patients with AD. Despite this evidence, the binding specificity of tau-targeting PET radiopharmaceuticals has yet to be determined. For example, 18F-THK5351 demonstrates significant tracer binding in the basal ganglia, in which tau pathology is not prominent in AD (Fig. 1). Furthermore, a recent human blocking study demonstrated substantial reduction of 18F-THK5351 retention after the administration of monoamine oxidase-B (MAO-B) inhibitor selegiline (5).

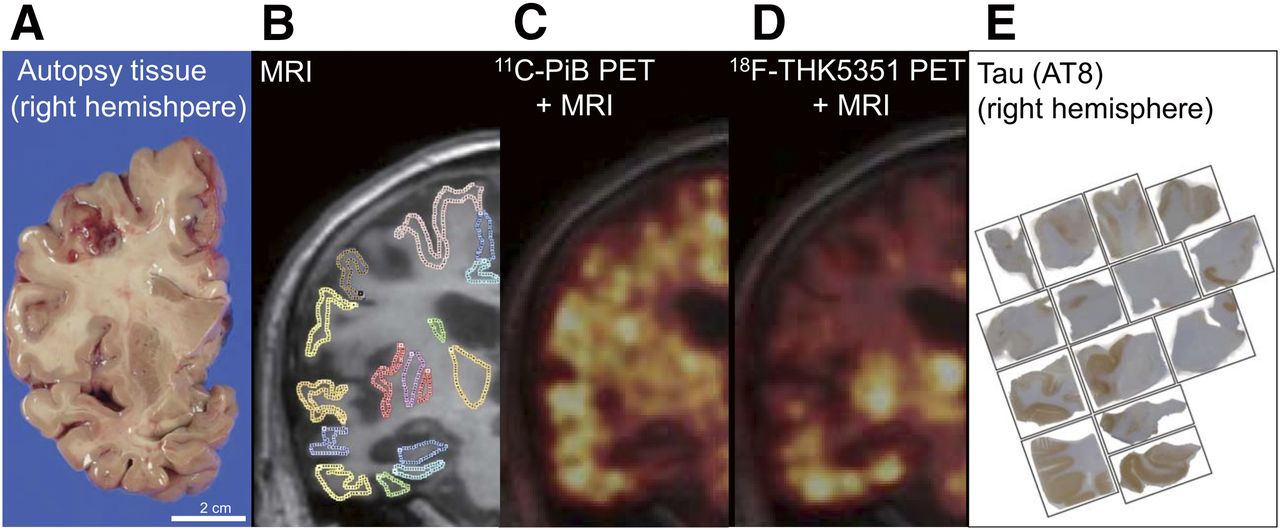
Images from coronal brain sections of autopsy tissue from right hemisphere (A), MRI with regions of interest (B), coregistered 11C-PiB PET scan (C), coregistered 18F-THK5351 PET scan (D), and tissue sections immunostained by anti-tau antibody (AT8) (E) in an AD patient (81-y-old man, Mini Mental State Examination Score 16 at PET scans).
In this study, we examined the imaging data of the brain from an autopsy-confirmed AD patient who underwent 18F-THK5351 and 11C-Pittsburgh compound B (11C-PiB) PET scans before death, to determine the correlation of antemortem in vivo THK5351 and PiB binding with quantitative measurements of neuropathologic substrates in the same brain regions of this patient.
MATERIALS AND METHODS
Participants
The study was approved by the Ethics Committee of the Tohoku University Graduate School of Medicine. Informed consent for neuroimaging and brain autopsy was obtained. The patient was an 81-y-old male with a 7-y history of progressive memory impairment and cognitive decline with delusion. He was clinically diagnosed with AD 3 y after the first symptoms appeared. 18F-THK5351 and 11C-PiB PET scans were performed 216 d and 600 d before death, respectively. At the time of the 18F-THK-5351 PET scan, his Mini Mental State Examination and ADAS-cog (Alzheimer's Disease Assessment Scale-Cognitive Subscale) scores were 10 and 48.3, respectively. At autopsy, his brain weight was 1,230 g. Brain atrophy was observed in the amygdala; hippocampus; parahippocampal gyrus; and the frontal, temporal, and parietal cortices on gross examination. Atherosclerosis was also observed in the basilar artery, left internal carotid artery, and left middle cerebral artery. In this case, amyloid-β (Aβ) Thal phase was 5, Braak stage was VI, and the neuritic plaque score was frequent (A3, B3, C3) (6). Lewy pathology was also present in the amygdala and entorhinal cortex. However, TDP-43 inclusions were absent, although severe neuronal loss was observed in the hippocampus.
Image Acquisition
PET imaging was performed using an Eminence STARGATE PET scanner (Shimadzu). After intravenous injection of 18F-THK5351 (185 MBq) or 11C-PiB (296 MBq), dynamic PET images were obtained for 60 min (18F-THK5351) or 70 min (11C-PiB) with the patient’s eyes closed. T1-weighted MR images were obtained with a SIGNA 1.5-T machine (GE Healthcare) using a previously described method (4). SUV images of 18F-THK5351 (40–60 min after injection) and 11C-PiB (50–70 min after injection) were obtained by normalizing tissue radioactivity concentration by injected dose and body weight. The regional SUV–to–cerebellar cortex SUV ratio (SUVR) was used as an index of tracer retention. PET images were coregistered on MR images using SPM12 software (SPM12; Wellcome Department of Imaging Neuroscience, UCL). Regions of interest were drawn on the coregistered MR image using PMOD software (version 3.7; PMOD Technologies GmbH).
In Vivo–In Vitro Correlation Analyses
Neuropathologic diagnostic analysis was performed on sections from the fixed left hemisphere. Frozen tissue blocks were sampled from the approximately 2-cm-thick coronal tissue slab of the right hemisphere. Frozen tissues were sectioned from the 14 blocks using a cryostat for autoradiography and immunohistochemistry. In vitro autoradiography was performed using the same protocol as previously described except for frozen sections (4). Coregistered MR and PET images of the right hemisphere were oriented along the coronal plane. The corresponding regions of interest were drawn on the MR image (Fig. 1), and then transformed onto the coregistered 18F-THK5351 and 11C-PiB PET images. Frozen tissue samples from the corresponding regions were homogenized in phosphate-buffered saline and used for biochemical analyses and binding assays as previously described (4).
Statistical Analysis
Spearman rank correlation coefficients were calculated to examine the association between radiotracer binding, histopathology, and biochemical data. Statistical significance was defined at a P value of less than 0.05. This analysis was performed using GraphPad Prism software (GraphPad).
RESULTS
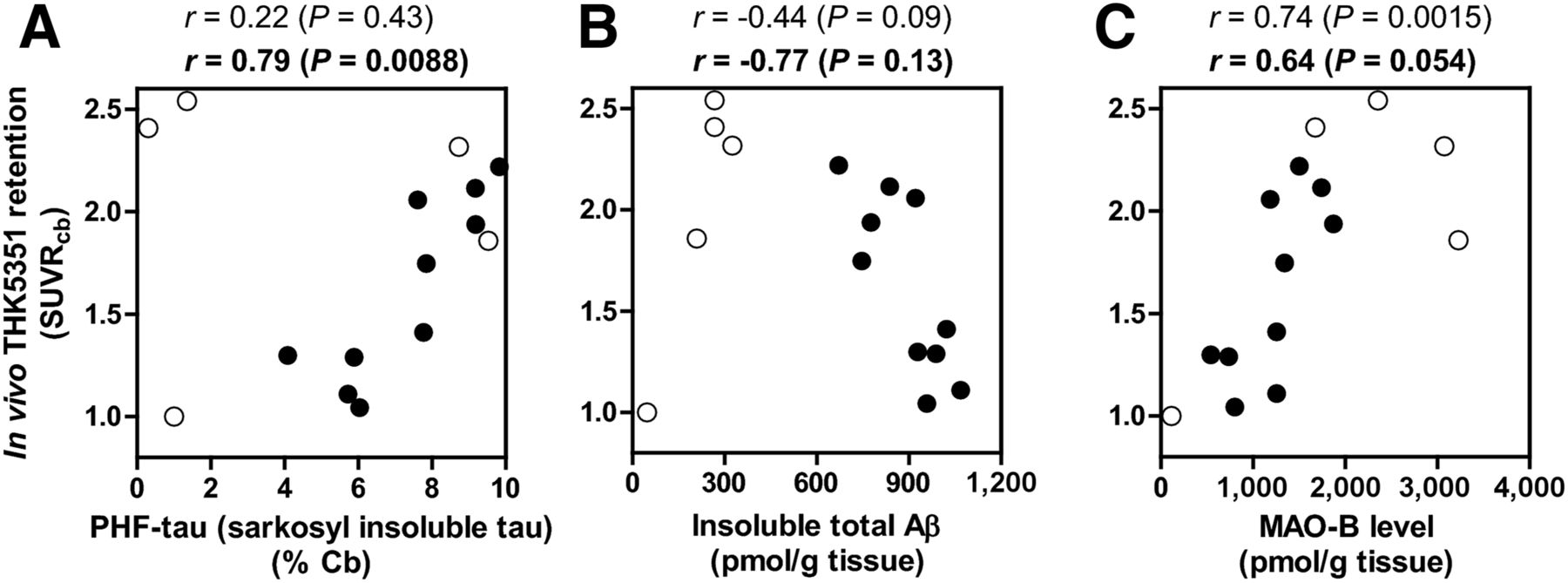
In autoradiography, 3H-THK5351 binding was substantially reduced in the presence of MAO-B inhibitor lazabemide, whereas 3H-THK5351 binding in AD brains remained detectable and was consistent with the distribution of tau deposits (Fig. 2). There was a strong correlation between in vivo THK5351 binding and tau immunohistochemistry in the neocortex (r = 0.96, P < 0.0001) (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). A similar correlation was also found between in vivo THK5351 binding and argyrophilic neurofibrillary pathology detected by Gallyas–Braak staining (r = 0.89, P < 0.0001). However, the significance of these correlations was diminished when subcortical regions were included in this analysis. A significant correlation was additionally observed between in vivo THK5351 retention and in vitro 3H-THK5351 binding in postmortem brain sections (r = 0.54, P = 0.03). There was no correlation between in vivo THK5351 binding and Aβ plaque load. Biochemical analyses were compatible with those determined by immunohistochemistry. In vivo THK5351 retention in the neocortex was strongly correlated with insoluble paired helical filaments (PHF)-tau level (r = 0.79, P = 0.0088), but not with insoluble Aβ level (Fig. 3). The regional MAO-B level was significantly correlated with in vivo THK5351 retention in the whole brain (r = 0.74, P = 0.0015). In contrast, in vivo PiB binding was significantly correlated with insoluble Aβ (r = 0.55, P = 0.03), but not with PHF-tau and MAO-B levels (Supplemental Fig. 2).
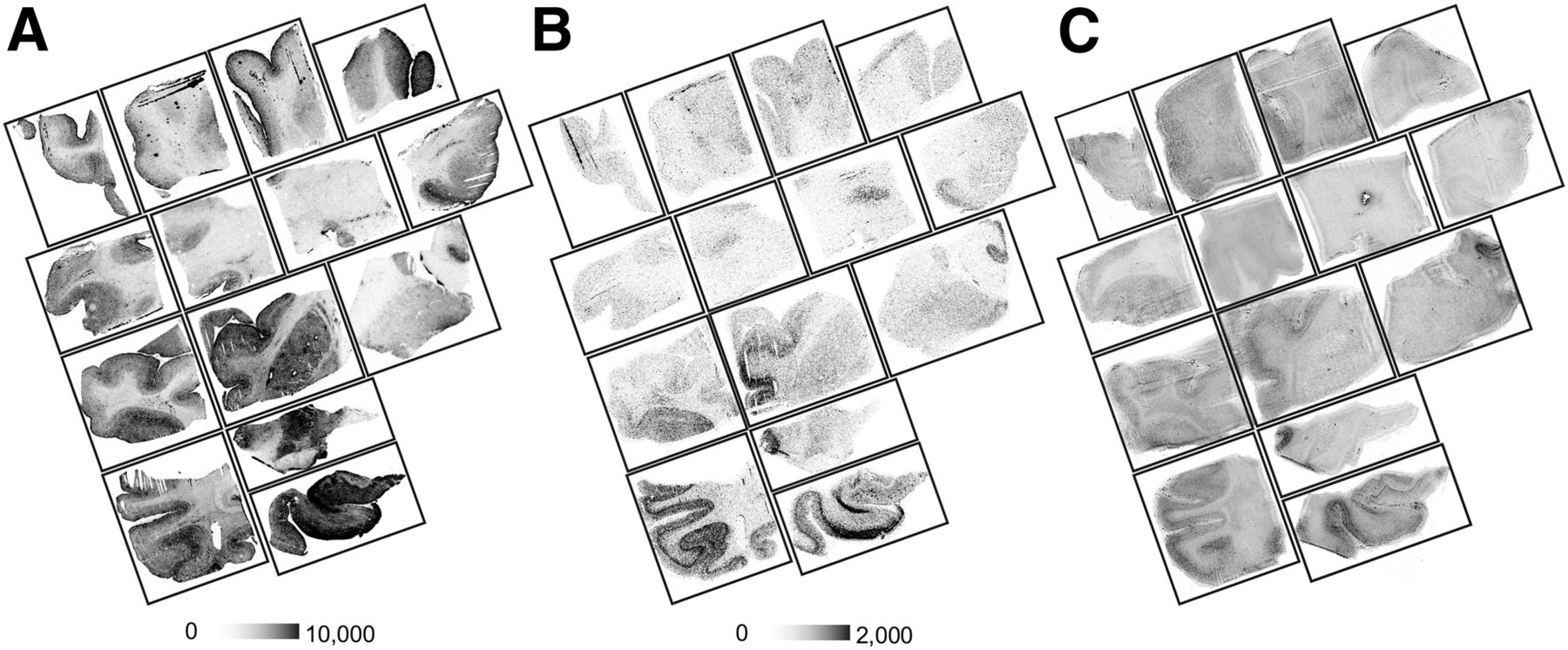
In vitro autoradiograms of 3H-THK5351 in brain sections from a patient with AD (81-y-old man) in absence (A) and presence (B) of MAO-B inhibitor lazabemide. (C) Images of Gallyas-Braak silver staining.

Correlation between antemortem in vivo 18F-THK5351 PET SUVRs on PET scans with biochemical postmortem quantification of sarkosyl-insoluble tau (T46) (A), insoluble total Aβ (B), and MAO-B (C) in corresponding 15 regions from frozen right hemisphere. Correlation coefficients and P values in whole brain (regular) and neocortex (bold) are shown at the top of each graph. ● = neocortical area; ○ = other brain areas.
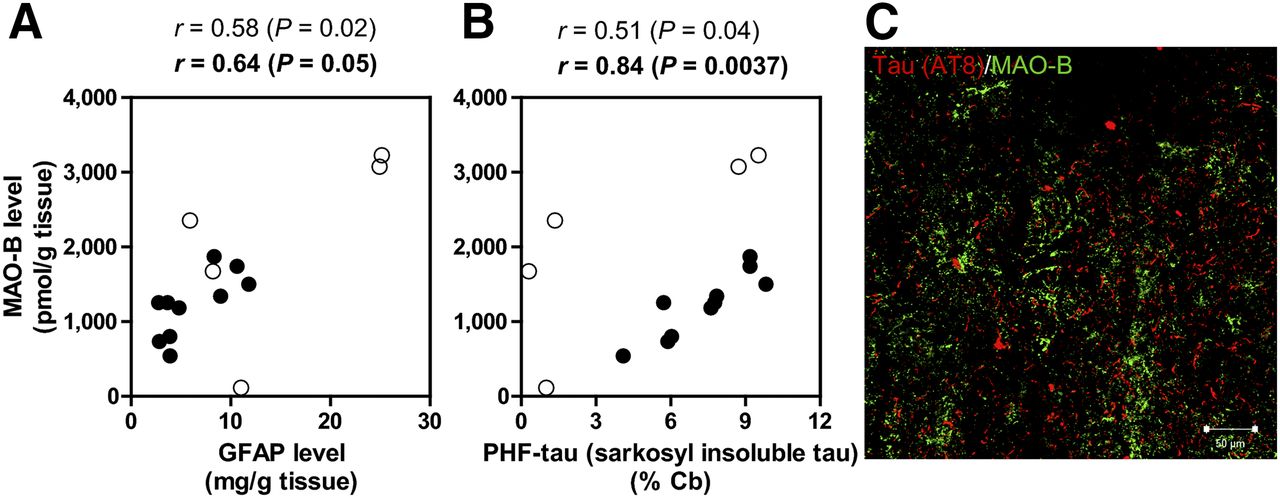
As demonstrated in previous studies, MAO-B is abundant in astrocytes. In fact, regional MAO-B levels were positively correlated with glial fibrillary acidic protein (GFAP) levels in this patient (Fig. 4A). The spatial distribution of PHF-tau in the neocortex of this AD patient was very similar to that of MAO-B (Fig. 4B). Double staining showed no colocalization between tau and MAO-B (Fig. 4C), indicating that these 2 proteins were separately located in neurons and astrocytes.
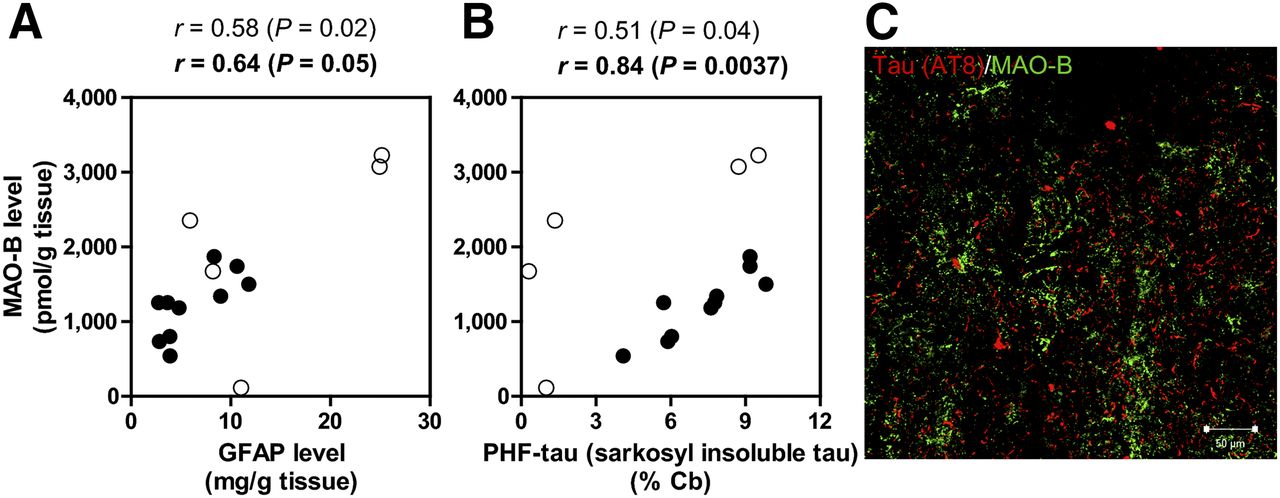
Correlation of MAO-B with GFAP (A) and PHF-tau (B) levels. Immunofluorescence double staining image of AT8 and MAO-B. (C) Correlation coefficients and P values in whole brain (regular) and neocortex (bold) are shown at the top of each graph. ● = neocortical area; ○ = other brain areas.
DISCUSSION
Clinical PET studies using putative tau-specific tracers have demonstrated significant tracer retention in sites susceptible to tau burden in AD patients (1,2). However, recent studies have also suggested the potential contribution of off-target tracer binding to PET images. In the present study, we examined correlations between in vivo tracer binding and neuropathologic substrates in postmortem brain tissues from an AD patient who underwent 18F-THK5351 and 11C-PiB PET before death.
In our imaging-pathology correlation analysis, in vivo cortical 18F-THK5351 retention correlated with PHF-tau and MAO-B, but not with Aβ, in postmortem AD brains. In the autoradiography of AD brain sections, the specific binding of 3H-THK5351 in the neocortex remained even in the presence of MAO-B inhibitors, and correlated with the density of PHF-tau. Thus, it can be said that THK5351 binding to PHF-tau contributes to in vivo PET signals in patients with AD. However, we also observed that 3H-THK5351 binding was substantially blocked in the presence of a MAO-B inhibitor. This was consistent with recent results from a human blocking study showing that a substantial reduction of 18F-THK5351 retention was observed after the administration of the MAO-B inhibitor selegiline (5). Our data demonstrated that in vivo 18F-THK5351 retention in the neocortex correlated not only with PHF-tau, but also with MAO-B levels in the brain. Collectively, these data suggest that THK5351 binding to MAO-B greatly contributes to in vivo PET signals. Further studies are required to clarify what percentage of the 18F-THK5351 PET signal was derived from MAO-B and PHF-tau.
MAO-B is predominantly expressed in the outer membrane of astrocyte mitochondria, which are widely distributed in human brains. MAO-B levels increase linearly in an age-dependent manner in whole-brain regions during the normal aging processes (7,8). A significant correlation has been observed between GFAP immunoreactivity and MAO-B inhibitor binding in AD brain (9). The present study also demonstrated the significant correlation between MAO-B and GFAP levels in AD brains, indicating that the level of THK5351 binding is likely associated with astrogliosis. Postmortem binding studies with 3H-L-deprenyl and 3H-lazabemide have shown the elevation of MAO-B levels in AD brains (9–11). Furthermore, in vivo PET studies using 11C-l-deprenyl have demonstrated elevated tracer uptake in the brains of AD patients (12,13). A large cross-sectional postmortem study has suggested that astrogliosis increased linearly throughout the disease course and correlated with tau pathology and brain atrophy, but not with amyloid plaques (14). Neuroinflammatory elements such as reactive astrocytes and activated microglia are considered to be secondary processes after Aβ accumulation, although they progress together with tau pathology and contribute to neurodegeneration throughout the course of AD (15). 18F-THK5351 PET can thus be used to track the progression of AD, by detecting both tau and reactive astrocytes.
CONCLUSION
18F-THK5351 PET signal reflects the combination of tau pathology and reactive astrocytes. These findings suggest 18F-THK5351 PET has limited utility for selective detection of tau pathology. However, this tracer has potential utility for the assessment of tau-associated neuroinflammatory changes in AD.
DISCLOSURE
This study was supported by research funds from GE Healthcare; the SEI (Sumitomo Electric Industries, Ltd.) Group CSR Foundation; Health and Labor Sciences Research Grants from the Ministry of Health, Labor, and Welfare of Japan; Grant-in-Aid for Scientific Research (B) (15H04900); Grant-in-Aid for Young Scientists (B) (15K19767); Grant-in-Aid for Scientific Research (B) (25293259); Grant-in-Aid for Scientific Research on Innovative Areas (Brain Protein Aging and Dementia Control) (26117003) from MEXT; and the Japan Research Foundation for Clinical Pharmacology. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 1, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 12, 2017.
- Accepted for publication July 25, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preclinical Characterization of the Tau PET Tracer [18F]SNFT-1: Comparison of Tau PET Tracers
- Preclinical Characterization of the Tau PET Tracer [18F]SNFT-1: Comparison of Tau PET Tracers
- First-in-Humans Evaluation of 18F-SMBT-1, a Novel 18F-Labeled Monoamine Oxidase-B PET Tracer for Imaging Reactive Astrogliosis
- Occipital Tau Deposition and Astrogliosis After Traumatic Brain Injuries in a Kendo Player
- 18F-SMBT-1: A Selective and Reversible PET Tracer for Monoamine Oxidase-B Imaging
- In vivo visualization of propagating {alpha}-synuclein pathologies in mouse and marmoset models by a bimodal imaging probe, C05-05
- Data-driven approaches for Tau-PET imaging biomarkers in Alzheimers disease
- Biomarkers for the diagnosis of Alzheimers disease, dementia Lewy body, frontotemporal dementia and vascular dementia
- Characterization of 3 Novel Tau Radiopharmaceuticals, 11C-RO-963, 11C-RO-643, and 18F-RO-948, in Healthy Controls and in Alzheimer Subjects