


Visual Abstract

Abstract
Reactive gliosis, characterized by reactive astrocytes and activated microglia, contributes greatly to neurodegeneration throughout the course of Alzheimer disease (AD). Reactive astrocytes overexpress monoamine oxidase B (MAO-B). We characterized the clinical performance of 18F-(S)-(2-methylpyrid-5-yl)-6-[(3-fluoro-2-hydroxy)propoxy]quinoline (18F-SMBT-1), a novel MAO-B PET tracer as a potential surrogate marker of reactive astrogliosis. Methods: Seventy-seven participants—53 who were elderly and cognitively normal, 7 with mild cognitive impairment, 7 with AD, and 10 who were young and cognitively normal—were recruited for the different aspects of the study. Older participants underwent 3-dimensional magnetization-prepared rapid gradient-echo MRI and amyloid-β, tau, and 18F-SMBT-1 PET. To ascertain 18F-SMBT-1 selectivity to MAO-B, 9 participants underwent 2 18F-SMBT-1 scans, before and after receiving 5 mg of selegiline twice daily for 5 d. To compare selectivity, 18F-THK5351 studies were also conducted before and after selegiline. Amyloid-β burden was expressed in centiloids. 18F-SMBT-1 outcomes were expressed as SUV, as well as tissue ratios and binding parameters using the subcortical white matter as a reference region. Results: 18F-SMBT-1 showed robust entry into the brain and reversible binding kinetics, with high tracer retention in basal ganglia, intermediate retention in cortical regions, and the lowest retention in cerebellum and white matter, which tightly follows the known regional brain distribution of MAO-B (R2 = 0.84). More than 85% of 18F-SMBT-1 signal was blocked by selegiline across the brain, and in contrast to 18F-THK5351, no residual cortical activity was observed after the selegiline regimen, indicating high selectivity for MAO-B and low nonspecific binding. 18F-SMBT-1 also captured the known MAO-B increases with age, with an annual rate of change (∼2.6%/y) similar to the in vitro rates of change (∼1.9%/y). Quantitative and semiquantitative measures of 18F-SMBT-1 binding were strongly associated (R2 > 0.94), suggesting that a simplified tissue-ratio approach could be used to generate outcome measures. Conclusion: 18F-SMBT-1 is a highly selective MAO-B tracer, with low nonspecific binding, high entry into the brain, and reversible kinetics. Moreover, 18F-SMBT-1 brain distribution matches the reported in vitro distribution and captures the known MAO-B increases with age, suggesting that 18F-SMBT-1 can potentially be used as a surrogate marker of reactive astrogliosis. Further validation of these findings with 18F-SMBT-1 will require examination of a much larger series, including participants with mild cognitive impairment and AD.
The neuropathologic hallmarks of Alzheimer disease (AD)—neurofibrillary tangles of tau protein and amyloid-β (Aβ) plaques—are accompanied by reactive gliosis, cellular degeneration, and diffuse synaptic and neuronal loss (1).
In recent years, there has been increased interest in the study of astrocytes (2). Astrocytes are the most abundant glial cells in the brain and are involved in several functions critical for the normal functioning and preservation of brain homeostasis (3,4), such as synaptic plasticity and formation of memory (5,6), regulation of γ-aminobutyric acid and glutamatergic neurotransmission (7–9), regulation of cerebral blood flow (10,11), and both Aβ production (12) and Aβ clearance (13). Astrocytes are also essential components of the neuroglial vascular unit, where they play a key neuroprotective role in cerebrovascular disease (10,11). Astrocytes do not constitute a homogeneous population and have been morphologically classified into protoplasmic, fibrous, and interlaminar or by their state: resting or activated (14). Although reactive astrocytes have also been classified as neurotoxic (A1), characterized by the expression of complement fraction 3, and neuroprotective (A2), expressing the S100A10 protein (15,16), reactive astrogliosis constitutes a much more complex spectrum of toxic and protective pathways (2,17), playing a crucial role in the pathophysiology of AD (9,18). Astrogliosis is an early neuroinflammatory event in several neurodegenerative conditions (19) such as AD (7,9,18), making it a target for the in vivo assessment of neuroinflammatory processes and their potential synergistic or independent contribution to the development of AD dementia. In AD, reactive astrogliosis and microgliosis have been observed around both dense-core Aβ plaques and neurofibrillary tangles, and they are believed to contribute greatly to neurodegeneration throughout the course of the disease (18,20). In contrast to microgliosis, which is not detected by imaging at early disease stages (21), reactive astrogliosis occurs early (22), making it a particularly attractive target for understanding its contribution to AD pathogenesis and the development of dementia and, as such, is a potential therapeutic target for AD (23).
Reactive astrocytes overexpress monoamine oxidase B (MAO-B) (24), and molecular neuroimaging studies have used MAO-B tracers such as 11C-l-deprenyl-D2 (11C-DED) as surrogate markers of astrogliosis (22,25–28). Some of these studies have shown that reactive astrogliosis is observed at the prodromal stages in both sporadic and familial AD (22,25). Historically, 11C-DED has been used as a surrogate PET tracer for reactive astrogliosis; however, several issues limit the use of 11C-DED, such as difficulty with quantification due to its irreversible kinetics, the existence of radiolabeled metabolites that can cross the blood–brain barrier and bind to monoamine transporters, poor image quality, and low selectivity for MAO-B (29). More recently another MAO-B tracer, 11C-SL25.1188, with more favorable tracer kinetics than 11C-DED was developed (30,31). 11C-BU99008, a tracer for the imidazoline 2 binding sites, has also been proposed as a surrogate marker of astrogliosis (32–35). Unfortunately, like 11C-DED, these tracers are labeled with 11C, which has a 20-min half-life, preventing widespread clinical or research applications.
Recently, an analog of the PET radiotracer 18F-THK5351, which was developed as a putative tau imaging radiotracer (36) but was later shown to have significant MAO-B binding (37,38), has been found to be highly selective for MAO-B (39). Preclinical assessment showed that 18F-(S)-(2-methylpyrid-5-yl)-6-[(3-fluoro-2-hydroxy)propoxy]quinoline (18F-SMBT-1) binds with high affinity (dissociation constant, 3.5 nM) and selectivity to MAO-B in human brain homogenates (39). Comparison of in vitro 18F-SMBT-1 binding against MAO-B regional activity expressed as relative luminescence showed 18F-SMBT-1 binding to correlate strongly with regional activity of MAO-B in the brain (39). Autoradiography studies showed significantly higher specific binding in the frontal cortex of an AD patient than in a control subject (39). Specific binding of 18F-SMBT-1 was completely displaced after incubation with 1 μM of the selective MAO-B inhibitor lazabemide (39), showing high selectivity and low nonspecific binding. Receptor-binding screening assays showed no significant 18F-SMBT-1 binding to 60 common neurotransmitter receptors, ion channels, and transporters (39). Radiation exposure was extrapolated to be 21.3 μSv/MBq for women and 12.2 μSv/MBq for men (39). Toxicity studies of 18F-SMBT-1 in animals, including acute pharmacology and toxicity at doses 1,000–10,000 times higher than those expected in a PET study, demonstrated no toxic effects related to the drug treatment.
The aim of this first-in-humans study was to characterize 18F-SMBT-1 binding, assessing its relation to age, regional brain distribution, and selectivity for MAO-B. We also examined 18F-SMBT-1 tracer kinetics and explored potential quantification approaches.
MATERIALS AND METHODS
Participants
In total, 77 nonsmoking participants—53 who were elderly and cognitively normal (CN), 7 with mild cognitive impairment (MCI), 7 with AD, and 10 young and CN (YCN)—were recruited for the different aspects of the study. All participants were screened for unstable medical or psychiatric disease and concomitant medication. Participants with known use of antidepressants, cold and flu tablets, or opiate or opioid agonist medication were excluded because of the possibility of interactions with selegiline. For participants with a recognized memory impairment, this information was collected from a next of kin or caregiver. The study protocol was approved by the Austin Health Human Research Ethics Committee, and all participants gave written informed consent.
Image Acquisition
PET scans were acquired on 1 of 2 scanners, a Philips TF64 PET/CT or a Siemens Biograph mCT. A low-dose CT scan was obtained for attenuation correction. Partial-volume correction was not performed in any of the studies.
18F-SMBT-1 PET
18F-SMBT-1 was synthesized in-house in the Department of Molecular Imaging and Therapy, Austin Health, using an ORA Neptis radiosynthesiser. The 18F-SMBT-1 synthesis is detailed in the supplemental materials (available at http://jnm.snmjournals.org). Sixty-nine adults (10 YCN, 49 CN, 6 MCI, and 4 AD) participated in the assessment of 18F-SMBT-1. All were administered 186 ± 6 MBq (range, 177–194 MBq). The average administered mass was 1.0 ± 0.8 μg (range 0.10–2.60 μg). Of the 69, 10 nondemented participants (4 CN and 6 MCI) underwent a 90-min dynamic scan after an intravenous bolus injection of 18F-SMBT-1. The remaining 59 participants (10 YCN, 45 CN, and 4 AD) underwent a 20-min emission scan (4 × 5 min) starting at 60 min after injection of 18F-SMBT-1. A second 18F-SMBT-1 PET scan was acquired for 9 participants (5 CN and 4 AD) after completion of a 5-d regimen of oral selegiline.
Aβ PET
All 67 older adults underwent Aβ PET imaging with 18F-flutemetamol (n = 3), 18F-florbetapir (n = 2), or 18F-NAV4694 (n = 62) to ascertain Aβ status. 18F-NAV4694 and 18F-florbetapir were synthesized in-house in the Department of Molecular Imaging and Therapy, Austin Health, as previously reported (40–42). 18F-flutemetamol was manufactured by Cyclotek Pty Ltd. The 18F-NAV4694 and 18F-florbetapir PET acquisitions consisted of 20-min (4 × 5 min) dynamic scans obtained at 50 min after an intravenous bolus injection of 185 MBq (±10%) of 18F-NAV4694 or 18F-florbetapir. Similarly, the participants who received 18F-flutemetamol also underwent a 20-min (4 × 5 min) PET acquisition starting at 90 min after injection of 185 MBq (±10%) of 18F-flutemetamol. All Aβ imaging results were expressed in centiloids (40,41,43,44).
Tau PET
Nine older adults who were enrolled in the selegiline assessments with 18F-SMBT-1 also underwent tau imaging with either 6-(fluoro-18F)-3-(1H-pyr- rolo[2,3-C]pyridin-1-yl)isoquinolin-5-amine (18F-MK-6240) (n = 7) (45) or 18F-PI2620 (n = 2) (46). Both tau imaging tracers were synthesized in-house in the Department of Molecular Imaging and Therapy, Austin Health, as previously reported (47). The 18F-MK6240 PET acquisition consisted of a 20-min (4 × 5 min) dynamic scan acquired at 90 min after an intravenous bolus injection of 185 MBq (±10%) of 18F-MK6240. The 18F-PI2620 PET acquisition consisted of a 20-min (4 × 5 min) dynamic scan acquired at 80 min after an intravenous bolus injection of 200 MBq (±10%) of 18F-PI2620. All tau imaging results were expressed as SUV ratios (SUVRs) using the cerebellar cortex as a reference region.
18F-THK5351 PET
Eight older adults (4 CN, 1 MCI, and 3 AD) underwent 2 18F-THK5351 PET scans. 18F-THK5351 was synthesized in-house in the Department of Molecular Imaging and Therapy, Austin Health, as previously described (48). Participants received an intravenous bolus injection of 185 MBq (±10%) of 18F-THK5351, and a 30-min emission scan (4 × 5 min) was acquired starting at 50 min after injection. A second 18F-THK5351 PET scan was acquired after completion of a 5-d regimen of oral selegiline.
MRI
Participants were also asked to undergo structural MRI on a 3-T TIM Trio scanner (Siemens Medical Solutions) to obtain high-resolution T1-weighted anatomic magnetization-prepared rapid gradient-echo sequences.
Image Analysis
Aβ and tau PET scans were spatially normalized using CapAIBL (44). The standard centiloid method was applied to determine Aβ burden (43). A centiloid value of more than 20 was selected to determine a high-Aβ (Aβ+) scan (49). A 1.19 SUVR in the temporal composite region (50) was used to discriminate between high tau (tau-positive) and low tau (tau-negative). 18F-THK5351 scans were spatially normalized using CapAIBL and expressed as SUVs. 18F-SMBT-1 PET images were also spatially normalized using CapAIBL. 18F-SMBT-1 PET volumes of interest were sampled to assess tracer selectivity, regional distribution, effect of age, and kinetic analysis. SUV values for the selegiline studies were estimated in 4 composite gray matter volumes of interest: neocortex (comprising frontal cortex, superior parietal lobe, lateral temporal lobe, lateral occipital lobe, anterior and posterior cingulate gyri, and precuneus), mesial temporal lobe (comprising hippocampus, entorhinal cortex, parahippocampus, and amygdala), basal ganglia (comprising caudate nuclei, putamen, globus pallidus, and thalamus), and cerebellar cortex. Several brain regions were evaluated as potential reference tissue, before generation of semiquantitative tissue ratios/SUVRs and graphical analysis of the data. Kinetic analysis was performed using PMOD (PMOD Technologies).
Assessing Tracer Selectivity Using Selegiline
Seventeen volunteers participated in the selegiline study. After a baseline 18F-THK5351 or 18F-SMBT-1 PET scan, the participants were supplied with oral selegiline tablets and instructed to follow a 5-d regimen at the standard therapeutic dose of 10 mg daily (5 mg at breakfast and 5 mg at lunch). At the completion of the regimen, the participants were invited back for a repeat PET scan.
Statistical Analysis
All statistical analyses were performed with JMP Pro (version 16.0; SAS Institute Inc.) for Macintosh (Apple). Data are presented as mean ± SD unless otherwise stated. Groups were compared using paired or unpaired Student t tests. Effect size was measured with Cohen d. Correlations were assessed by Spearman and Pearson correlation coefficients. Changes in tracer retention between pre- and postselegiline 18F-THK5351 studies were expressed as percentage reduction from baseline. Significance was set at a P value of less than 0.05, uncorrected for multiple comparisons.
RESULTS
No significant changes in vital signs or in immediate or delayed adverse events related to the study drug were observed or reported by any of the participants during or after the 18F-SMBT-1 scan.
Tracer Selectivity Studies
The irreversible MAO-B inhibitor selegiline was used to evaluate the selectivity of 18F-SMBT. All participants underwent an Aβ and tau imaging scan, in addition to the 2 18F-SMBT-1 scans before and after selegiline. The same study was repeated with a different cohort of participants using 18F-THK5351 to assess the validity of the selegiline regimen.
Table 1 shows the demographics of both groups. Tracer selectivity was assessed in 17 participants; 8 of them (4 CN, 3 Aβ+ AD, and 1 Aβ+ MCI) underwent assessment with 18F-THK5351, whereas 9 (5 CN and 4 Aβ+ AD) underwent assessment with 18F-SMBT-1.
Demographics of 18F-THK5351 and 18F-SMBT-1 Selectivity Evaluations
For the selectivity study with 18F-THK5351, 8 participants underwent Aβ PET and 2 18F-THK5351 PET scans, one at baseline and one after a 5-d regimen of 5 mg of oral selegiline twice daily. Figure 1A shows Aβ imaging studies performed with 18F-flutemetamol in a CN subject and with 18F-NAV4694 in an AD patient, as well as baseline 18F-THK5351 PET images of the same individuals before and after the selegiline regimen, indicating a variable degree of blockade of the 18F-THK5351. Given that there is a significant reduction in tracer retention in the cerebellar cortex, usually used as a reference region, all images are displayed in SUV units. Importantly, there is residual neocortical signal in the follow-up scan of the Aβ+ AD patient that is likely attributable to tau. Figure 1B shows a variable decrease in baseline 18F-THK5351 signal in the neocortex (∼63% decrease), mesial temporal lobe (∼71% decrease), basal ganglia (∼82% decrease), and cerebellar cortex (∼54% decrease), although there were no significant differences in the degree of signal reduction between CN and AD subjects.

Effect of selegiline on 18F-THK5351 and 18F-SMBT-1. (A) Representative coronal, sagittal, and transaxial PET images in Aβ-negative CN subject (79-y-old man; MMSE, 29) and in Aβ+ AD subject (72-y-old man; MMSE, 24). Aβ imaging studies are expressed in centiloids (top row) and were performed with 18F-flutemetamol or 18F-NAV4694. Baseline 18F-THK5351 PET images (middle row) of same individuals before and after (bottom row) selegiline regimen indicate variable degree of regional blockade of 18F-THK5351, most noticeable in basal ganglia, mesial temporal lobe, and neocortex. Given that there is significant reduction in tracer retention in cerebellar cortex, images are displayed in SUV units. Although in CN participants there is significant reduction of 18F-THK5351 retention throughout brain, in AD patients there is residual cortical retention likely due to 18F-THK5351 binding to tau. (B) Bar graphs showing percentage of selegiline 18F-THK5351 regional blockade in neocortex (∼63% decrease), mesial temporal lobe (∼71% decrease), basal ganglia (∼82% decrease), and cerebellum (∼54% decrease). Reduction of signal was greater in basal ganglia and mesial temporal lobe than in neocortex and cerebellum, although there were no significant differences in degree of signal reduction between CN and AD subjects. (C) Representative coronal, sagittal, and transaxial PET images in Aβ-negative, tau-negative CN subject (78-y-old woman; MMSE, 29) and in Aβ+, tau-positive AD subjects (75-y-old woman; MMSE, 21). Aβ imaging studies performed with 18F-NAV4694 are expressed in centiloids (top row). Second row shows tau imaging studies expressed in SUVR using cerebellar cortex as reference region, performed with either 18F-MK6240 or 18F-PI2620. Baseline 18F-SMBT-1 PET images (third row) of same individuals before and after (bottom row) selegiline regimen indicate high degree of regional blockade of 18F-SMBT-1 across all regions of brain. Images are displayed in SUV units. In contrast to 18F-THK5351 (Fig. 1A), there was no residual cortical retention in CN or AD subjects. (D) Bar graphs showing high percentage of blocking of 18F-SMBT-1 by selegiline, with more than 85% blockade across all regions of brain, indicating selective binding of 18F-SMBT-1 to MAO-B as well as low nonspecific binding. There were no significant differences in degree of signal reduction between regions or between CN and AD subjects. BG = basal ganglia; CB = cerebellum; CL = centiloids; MTL = mesial temporal lobe; NCTX = neocortex.
For the selectivity study with 18F-SMBT-1, 9 participants (5 CN and 4 Aβ+ tau-positive AD) underwent Aβ and tau imaging and 2 18F-SMBT-1 PET scans, one at baseline and one after the same 5-d regimen of 5 mg of oral selegiline twice daily. Figure 1C shows Aβ imaging studies with 18F-NAV4694 and tau imaging studies with 18F-MK6240, using the cerebellar cortex as a reference region, in a CN subject and an AD subject. The 18F-SMBT-1 SUV images before and after the selegiline regimen indicate a very high degree of reduction in 18F-SMBT-1 signal, with no residual activity attributable to Aβ or tau. Figure 1D shows a more than 85% decrease in baseline 18F-SMBT-1 signal in the neocortex, mesial temporal lobe, basal ganglia, and cerebellum, with the same degree of signal reduction in CN and AD subjects. A more detailed brain regional blockade by selegiline is provided in Table 2.
Percentage Reduction in Regional 18F-THK5351 and 18F-SMBT-1 SUV by Selegiline
Regional Brain Distribution of 18F-SMBT-1
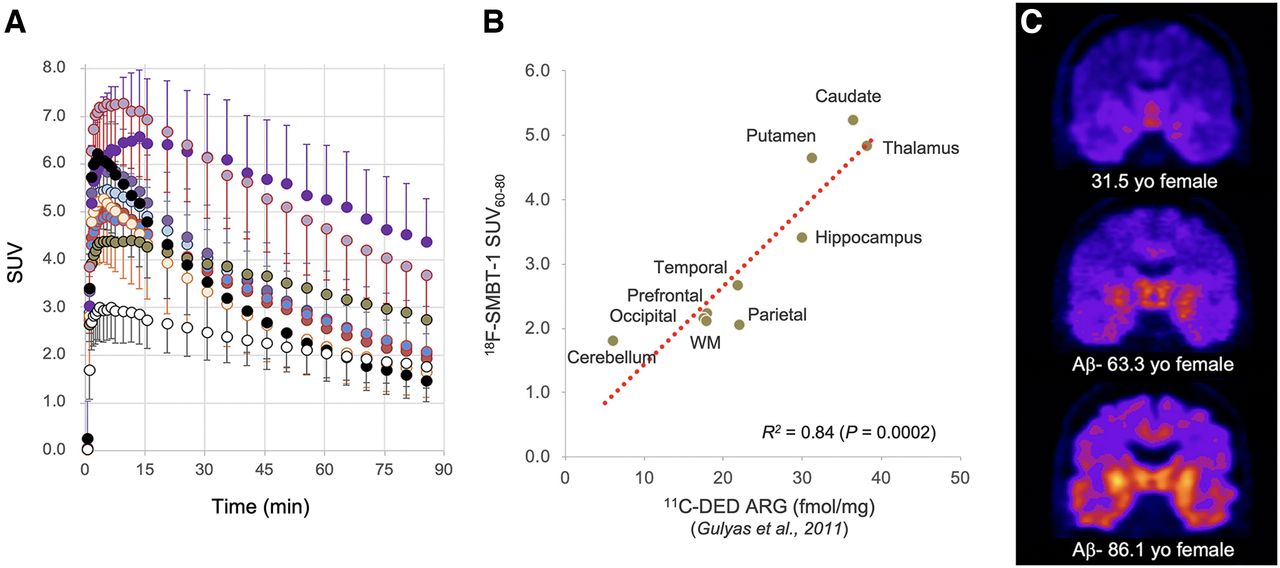
We also assessed the in vivo regional brain distribution of 18F-SMBT-1. Figure 2 shows 18F-SMBT-1 SUV at 60–80 min after injection in 44 low-Aβ (Aβ-negative) CN subjects, against the reported in vitro 11C-DED autoradiography regional concentrations (51). There was a strong correlation (R2 = 0.84, P = 0.0002) between the in vivo regional 18F-SMBT-1 signal and the in vitro concentrations in several regions of the brain.

Regional distribution of MAO-B in brain: correlation between in vitro autoradiography with 11C-DED and 18F-SMBT-1 retention in Aβ-negative CN subjects. There was high correlation (R2 = 0.84) between known in vitro regional distribution of MAO-B in brain (51), expressed in fmol/mg, and regional SMBT-1 retention at 60–80 min after injection. ARG = autoradiography; WM = white matter.
Increase in MAO-B with Age
To further evaluate 18F-SMBT-1, we scanned 10 YCN subjects (5 women, 5 men; 31.3 ± 4.0 y old) (Table 3) to assess whether 18F-SMBT-1 was able to capture the age-related increases of MAO-B in the frontal cortex as previously reported by in vitro studies (52). 18F-SMBT-1 SUV in the frontal cortex of 10 YCN and 44 Aβ-negative tau-negative CN subjects (Fig. 3A) demonstrated a significant age-related increase in MAO-B (R2 = 0.44, P < 0.0001). Figure 3B shows coronal, sagittal, and transaxial images illustrating the age-related regional increases in 18F-SMBT-1 signal in 3 women, whose ages ranged from 31 to 86 y old.
Demographics for Assessment of Effect of Age

Effect of age. (A) 18F-SMBT-1 SUV at 60–80 min after injection in frontal cortex of 10 YCN subjects (5 women, 5 men; 31.3 ± 4.0 y old) and 44 Aβ-negative CN subjects (25 women, 19 men; 76.0 ± 4.8 y old) was able to capture reported age-related increases of MAO-B in frontal cortex as previously reported by in vitro studies (52) and in vivo with PET (62). (B) Coronal, sagittal, and transaxial 18F-SMBT-1 images illustrating age-related regional increases in 18F-SMBT-1 signal in 3 women, whose ages ranged from 31 to 86 y (red circles in A).
18F-SMBT-1 Kinetics
We characterized the in vivo 18F-SMBT-1 kinetics in 10 elderly participants (6 MCI and 4 CN, Table 4). Time–activity curves revealed that 18F-SMBT-1 has robust entry into the brain (SUV, 4–7 at ∼3–5 min after injection) and displays reversible kinetics (Fig. 4A). 18F-SMBT-1 retention was highest in the basal ganglia and thalamus; intermediate in the anterior cingulate, gyrus rectus, and hippocampus; low in neocortical areas; and lowest in the cerebellum and in the subcortical white matter (SWM).
Demographics for Assessing 18F-SMBT-1 Tracer Kinetics

18F-SMBT-1 time–activity and total binding curves. (A) Time–activity curves reveal that 18F-SMBT-1 has robust entry into brain (SUV, 5–7 at ∼5 min after injection) and reversible kinetics. 18F-SMBT-1 clearance was slower in areas of high concentrations of MAO-B, such as basal ganglia and hippocampus, and faster in regions with lower MAO-B concentrations, such as frontal cortex, temporal lobe, and cerebellum. (B) Tissue ratios—using SWM as reference region—over time show SWM SUVR approaching apparent steady state in high binding areas ∼50 min after injection. SWM was more stable reference region across clinical groups and across Aβ status.
Before generating SUVRs over time, we compared the SUVs in several potential reference regions—cerebellum, cerebellar white matter, SWM (53), SWM, and corpus callosum (54)—to be used in a simplified reference tissue model (55). The SUVR generated with the SWM as a reference region had the strongest correlation with the in vitro regional distribution of MAO-B (Table 5) (51).
Correlation Between MAO-B In Vitro Distribution and 18F-SMBT-1 Binding Parameters and Tissue Ratios Generated with Different Reference Regions
SUVRs were shown to approach an apparent steady state in high-binding areas approximately 50 min after injection (Fig. 4B), suggesting the possibility of using a simplified 18F-SMBT-1 imaging protocol with SUVR as the outcome. 18F-SMBT-1 reversible kinetics were further validated by graphical analysis of the 90-min dynamic scans, using the same regions as used for generating SUVRs. 18F-SMBT-1 specific binding measures of distribution volume derived from the noninvasive Logan plot (56), as well as nondisplaceable binding potential estimated using the Ichise multilinear reference tissue model, MRTM (57), showed high correlations with late-scan SUVR (R2 = 0.97 and 0.94 for nondisplaceable binding potential and distribution volume, respectively) and with the known distribution of MAO-B in the human brain (R2 = 0.78 and 0.72 for nondisplaceable binding potential and distribution volume, respectively) (51).
DISCUSSION
To the best of our knowledge, 18F-SMBT-1 represents the first available 18F MAO-B radiotracer to be used in a clinical study. Because preclinical evaluation demonstrated 18F-SMBT-1 to have an in vitro binding profile well suited for an MAO-B PET tracer (39), the study aimed at characterizing the 18F-SMBT-1 binding profile in vivo with PET. The study was divided into 4 main areas or substudies. We first assessed 18F-SMBT-1 selectivity for MAO-B before and after a 5-d regimen of oral selegiline. 18F-SMBT-1 is an analog of the PET radiotracer 18F-THK5351, which was developed as a putative tau imaging radiotracer (39) but was later shown to have significant MAO-B binding (37,38). Therefore, we compared the 18F-SMBT-1 results with studies performed with 18F-THK5351 under the same selegiline regimen. For these studies, given that there is a significant widespread reduction in tracer retention even in regions usually used as an internal reference, all images were displayed in SUV units. In the 18F-THK5351 studies, the degree of blockade by selegiline in gray matter areas was variable, ranging from 54% in the cerebellar cortex to more than 80% in the basal ganglia. Moreover, there was some residual 18F-THK5351 signal in the cortex, likely representing 18F-THK5351 binding to tau. In the 18F-SMBT-1 studies, the degree of blockade by selegiline in gray matter areas was more than 85%, and most importantly, there was no residual cortical signal. There were no significant differences in the degree of signal reduction between CN and AD subjects with either 18F-THK5351 or 18F-SMBT-1. This study also demonstrated the low degree of nonspecific binding with 18F-SMBT-1. This is important because it enables 18F-SMBT-1 to accurately detect incipient early cortical changes in MAO-B concentrations as well as small changes over time. The low nonspecific binding is also evident in the high-contrast images (Fig. 1C) even at 60–80 min after injection. We then assessed the regional brain distribution of 18F-SMBT-1 and compared the results with in vitro autoradiography performed with 11C-DED (51), showing a high correlation between the two. The competition studies with selegiline and the regional distribution studies indicate that 18F-SMBT-1 is a highly selective 18F-labeled MAO-B tracer (7).
18F-SMBT-1 was also able to capture the known increases in MAO-B with age. The estimated yearly signal increase for 18F-SMBT-1 in the frontal cortex is about 2.5%/y, similar to the approximately 1.9%/y estimates from in vitro studies (52).
Finally, we evaluated the tracer kinetic characteristics of 18F-SMBT-1. The time–activity curves showed high initial entry into the brain, followed by clearance of the tracer. Clearance was slower in areas with very high MAO-B concentrations such as the basal ganglia, intermediate in areas with high MAO-B concentrations such as the hippocampus and anterior cingulate gyrus, and faster in cortical areas with low concentrations of MAO-B such as the neocortical areas. The lowest retention was observed in SWM. The reversible binding kinetics suggested that 18F-SMBT-1 binding could be quantified using graphical analysis (56,57) and a simplified reference tissue model (55).
Before embarking on the generation of tissue ratios and graphical analysis of the data, we explored several potential reference regions. We correlated the tissue ratios generated with each of them against the known regional distribution of MAO-B in the brain. SWM SUVR yielded the strongest correlation. Moreover, the SWM was the region least affected by selegiline (Table 2) and one of the least atrophic regions across the AD continuum (58). Graphical analysis outcomes, either multilinear reference tissue model or Logan plot, also generated using the SWM as reference region, correlated strongly with SWM SUVR and with the in vitro brain distribution of MAO-B. The small number of MCI and AD patients precludes drawing any conclusion regarding group differences in the 18F-SMBT-1 signal. A larger sample size of MCI and AD patients, with their corresponding Aβ and tau status, will be required to examine whether 18F-SMBT-1 can capture the reported increases in MAO-B in AD.
Although most of the recently developed specific neuroimaging and biofluid markers of disease have focused on the pathologic hallmarks of AD, such as Aβ plaques and tau tangles, the most prevalent markers identified in genomewide association studies of AD are related to neuroinflammation (59). The introduction of biomarker-based approaches to identifying brain pathology has informed new strategies for the design of preventative clinical trials aimed at preventing the onset of cognitive impairment and dementia. Markers of Aβ and tau pathology and markers of neurodegeneration have been incorporated into a recently proposed biomarker-based framework (60). In view of the advantage of the modular design of the framework, and considering that reactive gliosis is a critical aspect of the neuropathology of AD, the biomarker framework might be expanded to include reactive gliosis.
There are several limitations to the study. There is no validation of the semiquantitative or simplified reference region approach by full kinetic analysis with metabolite-corrected arterial input function. The same applies to the selection of the reference region. Initial semiquantitative and quantitative examinations used the SWM as the reference region. Although SWM was affected significantly less by the selegiline regimen than were the cortical, subcortical, or cerebellar regions (∼60% vs. >85% blockade), the selegiline study clearly indicates that there is substantial specific binding in SWM. This, in principle, would preclude the use of SWM as a reference region. It could be argued that SWM represents a brain region that is not likely to be involved in the early disease process; although there is SWM atrophy in AD, atrophy is more prevalent around mesial temporal lobe structures (58). Another issue to consider is that SWM, stricto sensu, does not truly fulfill the criteria for a reference region (55) given that it has a completely different cellular composition, has about half the regional cerebral blood flow of gray matter, and is likely to have a completely different degree of nonspecific binding. A more appropriate term for it might be internal brain scaling region. The kinetic analysis was performed pooling CN and MCI subjects, with 30% being deemed Aβ+. Probably because of the small numbers, there were no significant kinetic differences between CN and MCI subjects, nor were there significant kinetic differences when comparing Aβ-negative with Aβ+.
CONCLUSION
Our first-in-humans studies confirmed that 18F-SMBT-1 is a selective MAO-B tracer. Although the main goal was to characterize an MAO-B tracer to be used as a surrogate marker of astrogliosis in neurodegenerative conditions, the potential applications of an MAO-B tracer are much wider, extending from neuropsychiatric conditions such as depression (30) to movement disorders (61). In the particular case of assessing astrogliosis, 18F-SMBT-1 will allow a better understanding of the pathophysiology of AD while examining its potential direct or indirect effect over neurodegeneration, cognitive decline, and clinical progression, enabling more accurate staging and prognosis at earlier stages of the disease.
DISCLOSURE
The study was supported in part by National Health Medical Research Council (NHMRC) of Australia grants G1005121 and 19KK0212 from Japan. Yukitsuka Kudo and Nobuyuki Okamura own stock in Clino Ltd., licensing SMBT-1. Ryuichi Harada, Shozo Furumoto, Yukitsuka Kudo, and Nobuyuki Okamura have a patent pending for the technology described in this article. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 18F-SMBT-1 a selective MAO-B tracer?
PERTINENT FINDINGS: A clinical study in 59 elderly and 10 young participants showed that 18F-SMBT-1 is a highly selective MAO-B tracer, with reversible kinetics and low specific signal that follows the known regional distribution of MAO-B in the brain and captures the known increases in MAO-B with age.
IMPLICATIONS FOR PATIENT CARE: 18F-SMBT-1 can be used as a surrogate marker of reactive astrogliosis
ACKNOWLEDGMENTS
We thank the Brain Research Institute for support in acquiring the MRI data. We thank Drs. Chester Mathis, William E. Klunk, Milos Ikonomovic, Oscar Lopez, Ann Cohen, Howard Aizenstein, Scott Mason, Beth Snitz, and Beth Shaaban at the University of Pittsburgh for extremely fruitful discussions around 18F-SMBT-1, MAO-B, and reactive astrogliosis. We thank the participants who took part in the study and their families.
Footnotes
Published online Jan. 27, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 22, 2021.
- Accepted for publication January 14, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}