


Abstract
Peptide receptor radionuclide therapy (PRRT) may induce long-term toxicity to the bone marrow (BM). The aim of this study was to analyze persistent hematologic dysfunction (PHD) after PRRT with 177Lu-DOTATATE in patients with gastroenteropancreatic neuroendocrine tumors (GEP NETs). Methods: The incidence and course of PHD were analyzed in 274 GEP NET patients from a group of 367 patients with somatostatin receptor–positive tumors. PHD was defined as diagnosis of myelodysplastic syndrome (MDS), acute myeloid leukemia (AML), myeloproliferative neoplasm (MPN), MDS/MPN, or otherwise unexplained cytopenia (for >6 mo). Using data from The Netherlands Cancer Registry, the expected number of hematopoietic neoplasms (MDS, AML, MPN, and MDS/MPN) was calculated and adjusted for sex, age, and follow-up period. The following risk factors were assessed: sex, age over 70 y, bone metastasis, prior chemotherapy, prior external-beam radiotherapy, uptake on the [111In-DTPA0]octreotide scan, tumor load, grade 3–4 hematologic toxicity during treatment, estimated absorbed BM dose, elevated plasma chromogranin A level, baseline blood counts, and renal function. Results: Eleven (4%) of the 274 patients had PHD after treatment with 177Lu-DOTATATE: 8 patients (2.9%) developed a hematopoietic neoplasm (4 MDS, 1 AML, 1 MPN, and 2 MDS/MPN) and 3 patients (1.1%) developed BM failure characterized by cytopenia and BM aplasia. The median latency period at diagnosis (or first suspicion of a PHD) was 41 mo (range, 15–84 mo). The expected number of hematopoietic neoplasms based on The Netherlands Cancer Registry data was 3.0, resulting in a relative risk of 2.7 (95% confidence interval, 0.7–10.0). No risk factors for PHD could be identified for the GEP NET patients, not even bone metastasis or estimated BM dose. Seven patients with PHD developed anemia in combination with a rise in mean corpuscular volume. Conclusion: The prevalence of PHD after PRRT with 177Lu-DOTATATE was 4% in our patient population. The median time at which PHD developed was 41 mo after the first PRRT cycle. The relative risk for developing a hematopoietic neoplasm was 2.7. No risk factors were found for the development of PHD in GEP NET patients.
Peptide receptor radionuclide therapy (PRRT) has been in use for 25 y as second-line therapy in patients with inoperable (metastatic) gastroenteropancreatic (GEP) neuroendocrine tumors (NETs). 111In-radiolabeled somatostatin analogs were used in early studies (1,2). Besides encouraging results regarding symptom relief, the reported number of objective responses was low. Myelodysplastic syndrome (MDS) or leukemia was reported in half the NET patients who received a very high dose (>100 GBq) of [111In-DTPA0]octreotide (OctreoScan; Mallinckrodt). PRRT with 177Lu-DOTATATE results in a better radiologic response rate of 15%–35% (3–6). In general, side effects are mild, although serious hematologic toxicity has been reported, making the bone marrow (BM) the main dose-limiting organ. In 11% of the patients, subacute grade 3–4 hematologic toxicity is observed after PRRT with 177Lu-DOTATATE (7). Also, long-term hematologic toxicity such as acute myeloid leukemia (AML) and MDS was reported in 1%–2% of the patients treated with 177Lu- or 90Y-based PRRT (8–11). To our knowledge, no in-depth report of persistent hematologic dysfunction (PHD) in patients treated with 177Lu-DOTATATE has been published.
The aim of this study was to analyze PHD after PRRT with 177Lu-DOTATATE in GEP NET patients. Incidence, clinical course, and predicting factors were evaluated in a large group of GEP NET patients.
MATERIALS AND METHODS
Patients
In this study, Dutch patients were analyzed who were treated from January 2000 to December 2007. Follow-up data were used up to December 2012 because we expected therapy-related PHDs within 5 y after therapy and because our follow-up protocol changed after December 2012. Only Dutch patients were selected because loss to follow-up was limited in these patients. Only GEP NETs were selected because 177Lu-DOTATATE is indicated for this group of patients.
The inclusion criteria were as follows: patients with somatostatin receptor–positive tumors and baseline tumor uptake on somatostatin receptor scintigraphy with [111In-DTPA0]octreotide, with accumulation in the tumor at least as high as in normal liver tissue; no prior treatment with a radionuclide therapy; a baseline serum hemoglobin level of at least 6 mmol/L; a white blood cell count of at least 2 × 109/L; a platelet count of at least 75 × 109/L; a serum creatinine level of no more than 150 μmol/L or a creatinine clearance of at least 40 mL/min; and a Karnofsky performance status of at least 50.
The intensity of tumor uptake and the extent of tumor burden were scored according to simple scaling systems (3).
This study was part of an ongoing prospectively designed study on patients with neuroendocrine tumors treated with 177Lu-DOTATATE at the Department of Radiology and Nuclear Medicine, Erasmus University Medical Center in Rotterdam. The hospital’s medical ethics committee approved the study. All patients gave written informed consent to participate. All procedures were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Treatment
[DOTA0,Tyr3]octreotate was obtained from BioSynthema. 177LuCl3 was supplied by IDB-Holland, and 177Lu-DOTATATE was prepared locally (12).
Granisetron (3 mg) or ondansetron (8 mg) was injected intravenously 30 min before infusion of 177Lu-DOTATATE. Infusion of amino acids (2.5% arginine and 2.5% lysine, 1 liter) was started 30 min before administration of the radiopharmaceutical and lasted for 4 h. The radiopharmaceutical was coadministered for 30 min using a second pump system. Cycle doses of 1.85 GBq (50 mCi) were given to 1 patient, 3.7 GBq (100 mCi) to 13 patients, 5.6 GBq (150 mCi) to 12 patients, and 7.4 GBq (200 mCi) to the remaining patients, injected over 30 min. The interval between treatments was 6–16 wk. The intended cumulative dose was 29.6 GBq (800 mCi). The median number of therapy cycles was 4 (range, 1–8), with a median cumulative activity of 29.6 GBq (range, 7.4–59.2 GBq). However, the dose was lowered if the calculated kidney dose was higher than 23 Gy. Other reasons for dose reduction or cessation of further therapy were recurrent grade 3 or 4 hematologic toxicity or persistent low blood counts.
Follow-up and Toxicity Assessment
Hematology and liver and kidney function were tested during the 6 wk before the first therapy, at 4 and 6 wk after each therapy cycle, and at follow-up visits. Subacute hematologic toxicity was assessed according to the Common Terminology Criteria for Adverse Events, version 3.0 (13). This version was used because of well-defined grades (1 to 5) for adverse events in platelets, leukocytes, and hemoglobin.
Patients with PHD were defined as having one or more of the following: MDS, AML, myeloproliferative neoplasm (MPN), or MDS/MPN according to the revised World Health Organization 2008 diagnostic criteria (14) or unexplained grade 3–4 hematologic toxicity (>6 mo) in hemoglobin, platelets, or white blood cells (with or without the requirement of multiple blood transfusions).
The latency period was defined as the time from the first treatment with 177Lu-DOTATATE to the date of diagnosis. If no diagnosis was made, the date of the first BM biopsy or aspiration was used. If there was no available BM biopsy or aspiration, the date of diagnosis was replaced by the date when the suspected PHD was noted in the patient’s medical file.
The estimated absorbed BM dose was based on a group-averaged estimated BM dose in 23 patients (7). Therefore, this mean BM dose per administered activity of 0.067 ± 0.007 mGy/MBq (7) was multiplied by the individual cumulative injected activity of 177Lu-DOTATATE.
The Netherlands Cancer Registry
The expected number of patients with hematopoietic neoplasms was calculated using data from The Netherlands Cancer Registry (www.cijfersoverkanker.nl), which is managed by The Netherlands Comprehensive Cancer Organization. Data on incidence, prevalence, survival, mortality, and risk are available on this website. Users can make their own graphs and tables on cancer incidence according to localization, region, sex, and age. Data are available from 1989 to 2016.
The incidence (number of cancers per 100,000 persons per year) of hematopoietic neoplasms was used for 4 categories; MDS, AML, MPN, and MDS/MPN.
Data were categorized by sex and age (in 5-y cohorts). Average incidence rates (per 100,000 residents) of the 4 categories between 2001 and 2011 were calculated. The expected number of cases per category was compiled on the basis of the number of patients and years of follow-up in our study. The expected numbers were adjusted for sex, age, and duration of follow-up.
Statistics
SPSS software (version 19; IBM) was used for statistical analysis. Distributions were examined for normality using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Correlations between distributions were evaluated using the χ2 and unpaired t tests.
PHD was analyzed as a discrete variable. The following baseline variables were included in the analysis: sex, age over 70 y, presence of bone metastases, prior chemotherapy, prior external-beam radiotherapy, uptake on the [111In-DTPA0]octreotide scan, tumor load, grade 3–4 hematologic toxicity during treatment, and plasma chromogranin A level of more than 2,000 μg/L (reference level, <100 μg/L). Continuous variables included in the analysis were baseline hemoglobin level, baseline platelet count, baseline white blood cell count, and estimated absorbed BM dose. The creatinine clearance was estimated with the Cockcroft–Gault formula and evaluated as a continuous variable.
RESULTS
In total, 367 patients with somatostatin receptor–positive tumors were treated, of whom 274 had GEP NETs, 34 had NETs of unknown primary or other location, and 59 had other tumors (supplemental materials; supplemental materials are available at http://jnm.snmjournals.org). The median follow-up time of the 274 patients was 29 mo (range, 0–142 mo). Twenty-six (10%) of the 274 patients had been treated with cytotoxic chemotherapy in the past, and 18 had been treated with external-beam radiation therapy. The full patient characteristics are summarized in Table 1.
Baseline Characteristics of 274 GEP NET Patients
Long-Term Hematologic Toxicity
Eleven of the 274 GEP NET patients (6 women and 5 men) had PHD after treatment with 177Lu-DOTATATE (4%). Eight patients developed a hematopoietic malignancy (4 MDS, 1 AML, 1 MPN, and 2 MDS/MPN), and 3 patients developed BM failure characterized by cytopenia and BM aplasia (Table 2). Two patients with PHD were not analyzed because they did not have GEP NETs: one patient with thyroid carcinoma died 2 wk after a BM biopsy demonstrating BM hypoplasia, and another patient with a NET of unknown primary developed BM failure, which was most likely due to significantly decreased kidney function (glomerular filtration rate < 50 mL/min). The characteristics of the 11 GEP NET patients with PHD are shown in Table 3.
Classification of 11 of 274 GEP NET Patients with PHD after PRRT with 177Lu-DOTATATE
Characteristics of 11 of 274 GEP NET Patients with PHD after PRRT with 177Lu-DOTATATE
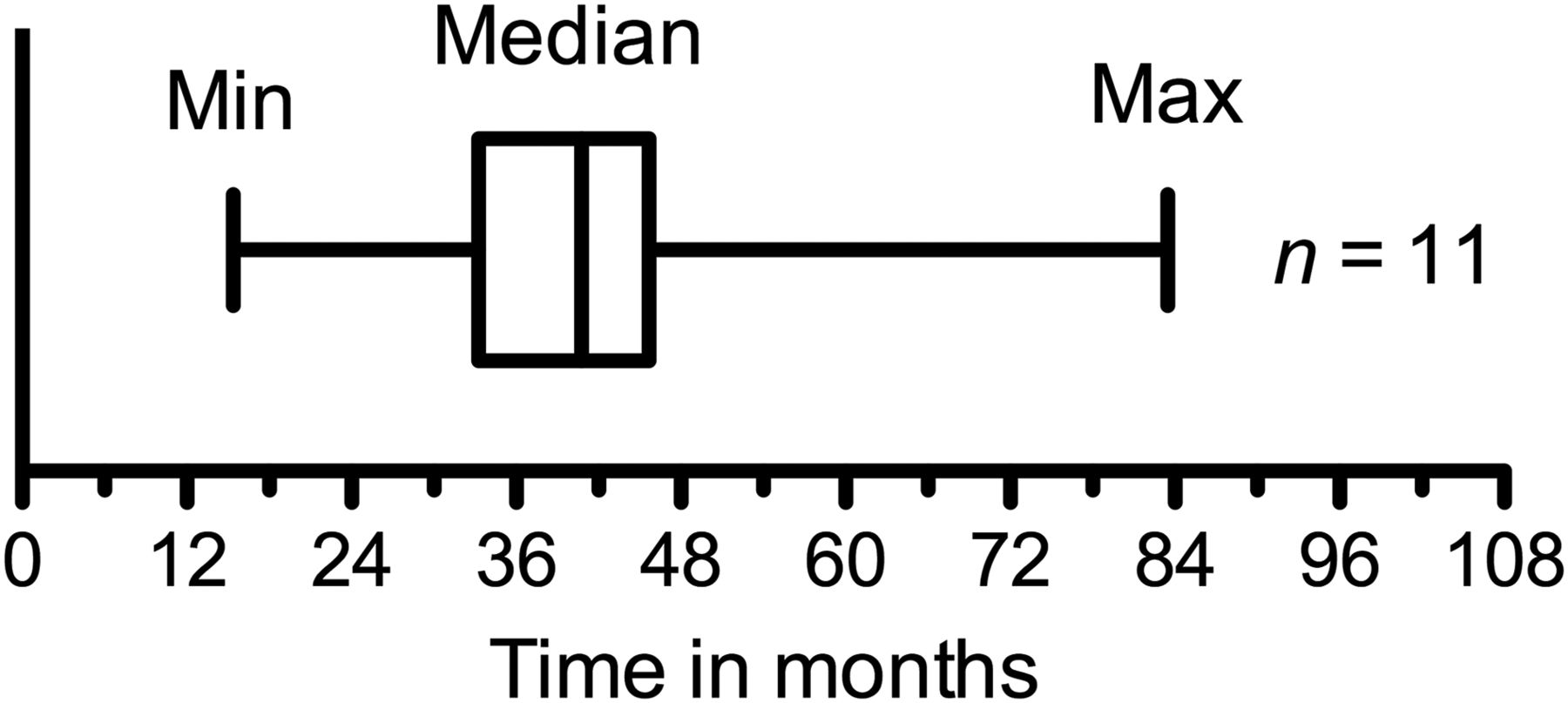
The median latency period from initiation of PRRT to diagnosis of PHD in the 11 of 274 GEP NET patients was 41 mo (range, 15–84 mo) (Fig. 1).
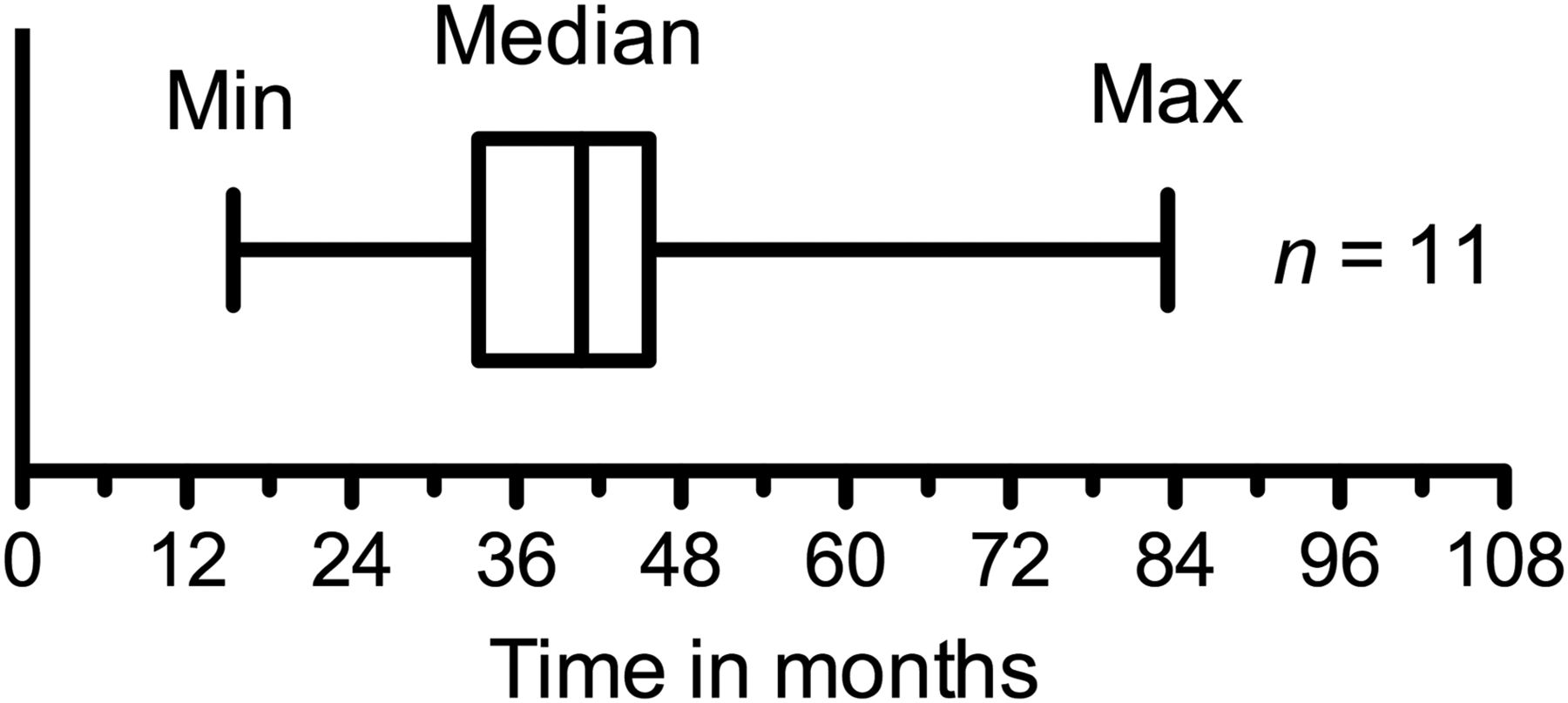
Median latency time in 11 patients with PHD. Latency time (period between first treatment and date of diagnosis) is shown for 11 of 274 GEP NET patients with PHD after PRRT with 177Lu-DOTATATE. Whiskers represent minimum (15 mo) and maximum (84 mo) latency time. Width of box shows interquartile range, and vertical line in box is median (41 mo) latency time.
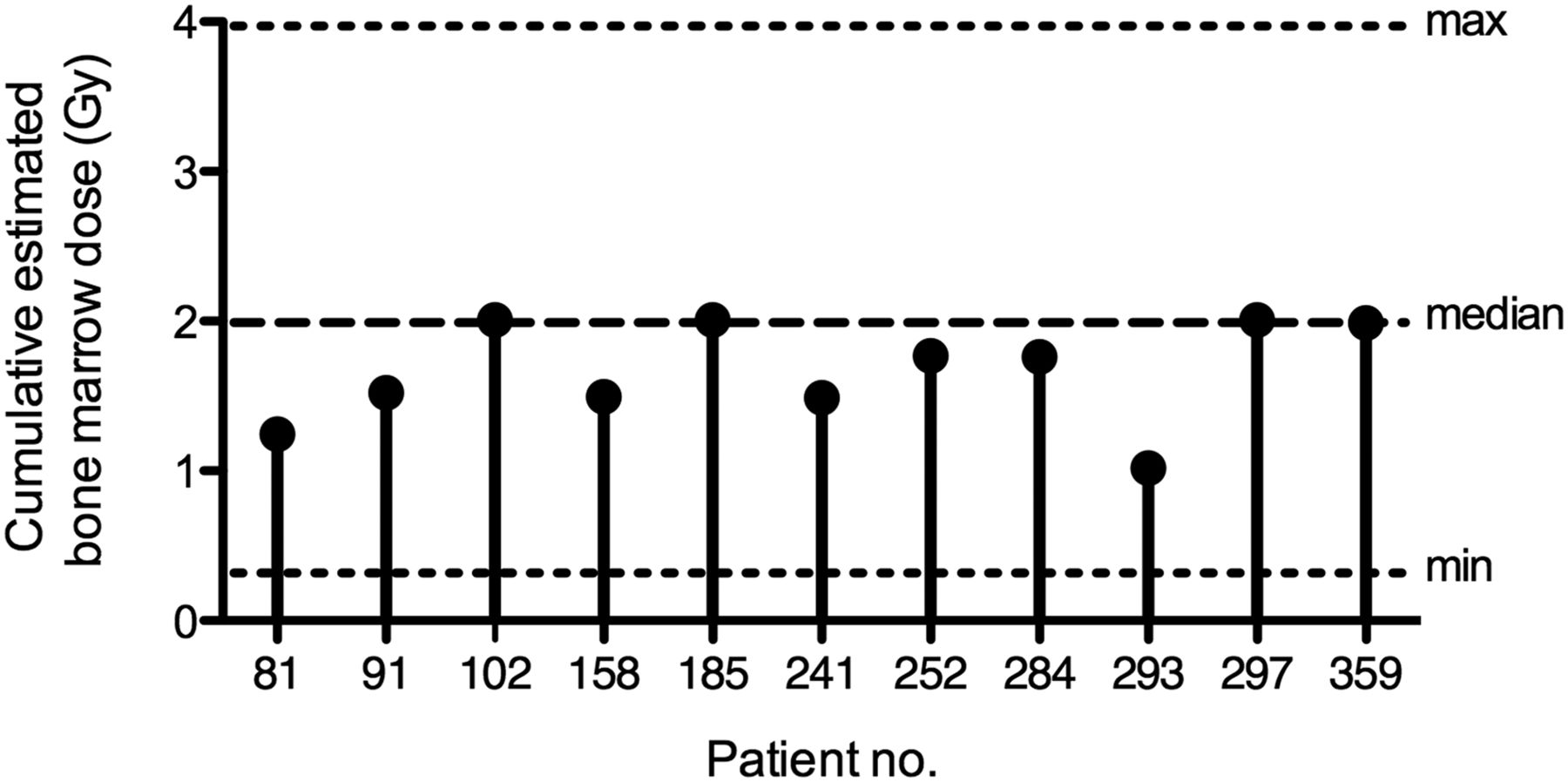
In 5 of the 11 patients, PRRT was interrupted and the planned cumulative activity of 29.6 GBq of 177Lu-DOTATATE was not administered. The median cumulative estimated BM dose was 2.0 Gy (range, 0.2–4.0 Gy) in the 263 patients without PHD and 1.8 Gy (range, 1.0 −2.0 Gy) in the 11 patients with PHD (Fig. 2). Seven of the 11 patients received a BM dose of less than 2.0 Gy.

Estimated BM dose in 11 GEP NET patients with PHD. Spike plot shows cumulative estimated BM dose in 11 GEP NET patients with PHD after PRRT with 177Lu-DOTATATE. Dashed lines indicate median (and range) of estimated BM dose in 263 NET patients without PHD.
In total, 274 GEP NET patients (139 men and 135 women) were analyzed for calculating the expected number of patients with hematopoietic neoplasms. The cumulative follow-up was 1,113 person-years, resulting in an expected number of MDS, AML, MPN, and MDS/MPN cases of 1.10, 1.27, 0.48, and 0.19, respectively, with a total number of 3.0 patients based on The Netherlands Cancer Registry data (Fig. 3) (supplemental materials).

Expected number of patients with hematopoietic neoplasms and type, based on data from The Netherlands Cancer Registry, as well as observed number of patients (of 274 GEP NET patients) with PHD after PRRT with 177Lu-DOTATATE, including 8 patients with hematopoietic neoplasms and 3 with BM failure. Red = MDS; orange = AML; yellow = MPN + MDS/MPN; green = BM failure.
The relative risk is the chance that a hematopoietic neoplasm occurs when exposed to PRRT (8/274), divided by the chance that hematopoietic neoplasms occur when not exposed (3/274). For our study, these numbers were 8 and 3, respectively, of 274 patients, for a relative risk of 2.7 (95% confidence interval, 0.7–10.0). Therefore, patients treated with PRRT had more than a 3 times higher risk of developing hematopoietic neoplasms than patients not treated with PRRT.
Risk Factors and Course
Risk factors were assessed in the 274 GEP NET patients, including the 11 GEP NET patients with PHD. The presence of bone metastases or prior chemotherapy was not more prevalent in NET patients with PHD than in those without PHD. For the other defined risk factors (sex, age over 70 y, prior external-beam radiotherapy, uptake on the [111In-DTPA0]octreotide scan, tumor load, grade 3–4 hematologic toxicity during treatment, estimated absorbed BM dose, elevated plasma chromogranin A level, baseline blood counts, and renal function), no significant differences were found between GEP NET patients with PHD and those without.
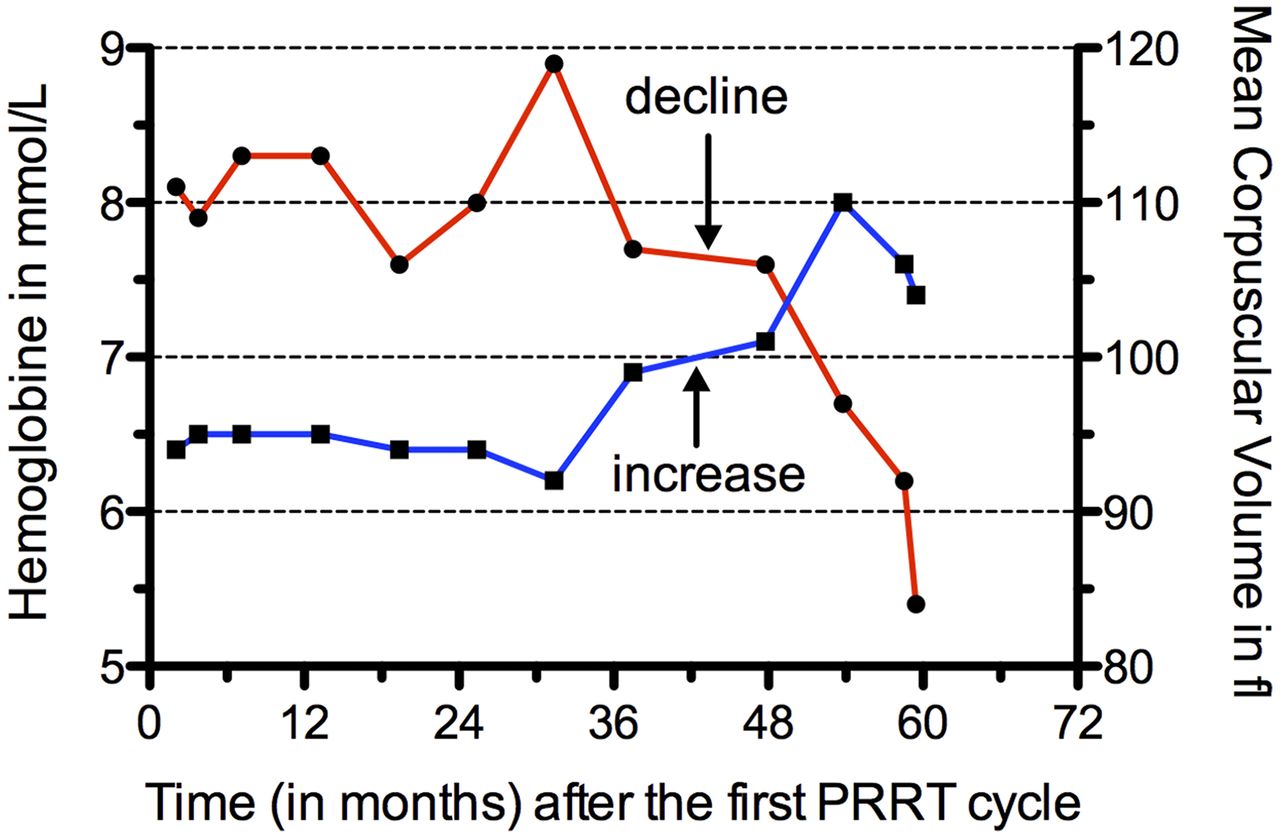
Seven patients with PHD had anemia in combination with an elevated mean corpuscular volume (e.g., patient 185; Fig. 4).

Course of hemoglobin (red) and mean corpuscular volume (blue) in patient 185, diagnosed with MDS/MPN after PRRT with 177Lu-DOTATATE. Time zero is date of last PRRT cycle. Decline in hemoglobin was followed by increase in mean corpuscular volume (arrows).
The incidence of PHD and the expected number of hematopoietic neoplasms were also determined—and the risk assessment performed—in all 367 patients with somatostatin receptor–positive tumors (Table 4).
Analysis of 367 Patients with Somatostatin-Positive Tumors after PRRT with 177Lu-DOTATATE
DISCUSSION
MDS covers a heterogeneous group of myeloid malignancies and occurs in 2–4 individuals per 105 persons per year in the Dutch population (15). AML and related precursor neoplasms occur in 3–4 individuals per 105 persons per year in the European population (16). The incidence of myeloid neoplasms and leukemia is strongly determined by age and sex. Also, exposure to radiation increases the frequency of hematologic malignancies (17).
The total observed incidence of hematopoietic neoplasms after PRRT is a summation of de novo incidence (i.e., without exposure to therapeutic radiation) and therapy-related incidence (i.e., with radiation exposure). The total number of patients with PHD after PRRT was significantly higher than we would anticipate on the basis of the expected number of de novo hematopoietic neoplasms. Our incidence of PRRT-related PHD was 4%; however, this percentage is patient-group–dependent because sex, age, and previous chemotherapeutic treatments influence the incidence of hematopoietic neoplasms. In a large retrospective analysis of a 90Y-DOTATOC phase II trial, only 2 (<1%) of 1,109 patients developed myeloproliferative diseases (10). Considering the number of patients and mean follow-up of 23 mo in this study, one would expect an incidence of more than 2 de novo hematopoietic neoplasms alone. Therefore, the reported number of myeloproliferative events after PRRT in this study does not seem accurate. Bodei et al., in a large retrospective study of 807 NET patients treated with 177Lu- or 90Y-labeled somatostatin analogs, found a 3.3% incidence of MDS and acute leukemia (8). This is in line with our findings. In the same retrospective study of Bodei et al., mean latency times of 45 and 57 mo were reported between the start of PRRT and the development of MDS and leukemia, respectively (8). Our median latency period was 41 mo, which is approximately the same as reported by Bodei et al. (8).
PRRT with 177Lu-DOTATATE has significant similarities to therapy with radioiodine (131I), such as the physical decay characteristics and the human biodistribution in blood and BM. In patients with thyroid cancer treated with 131I, a leukemia incidence of 0.2%–0.3% is observed in comparison to the general population (18,19). In a comprehensive metaanalysis, the pooled relative risk for development of leukemia increased 2.5-fold in patients treated with 131I as compared with thyroid cancer survivors not treated with 131I (20,21). In our study on GEP NET patients treated with 177Lu-DOTATATE, we found a relative risk similar to that of thyroid cancer patients treated with 131I. However, the number of de novo (i.e., expected) MDS and leukemia cases is age-dependent. Therefore, the incidence can vary between studies if the age distributions of the patient populations differ. Also, in radioimmunotherapy, myelosuppression is the primary toxicity and raises concerns about the risk of treatment-related MDS or acute leukemia. In a retrospective study that analyzed patients treated with a 131I-labeled monoclonal antibody (131I-tositumomab), 35 (3.5%) of 995 non-Hodgkin lymphoma patients developed MDS or acute leukemia (22), whereas clinical studies with the 90Y- or 111In-labeled monoclonal antibody (Zevalin; Spectrum Pharmaceuticals, Inc.) reported an incidence of 2.3% for MDS or acute leukemia, and the malignancies were diagnosed 23 mo after radioimmunotherapy (23).
In our study, we did not find a difference in cumulative estimated BM dose between patients with and without PHD, as is in line with the BM dose calculation of Bodei et al. (Fig. 5) (8). However, about half our patients with PHD did not receive the intended cumulative administered activity of 29 GBq of 177Lu-DOTATATE. These patients were also excluded for salvage therapy with 177Lu-DOTATATE, therefore creating a bias in our results. Despite this selection bias, about 30% of our patients received a cumulative injected dose of more than 30 GBq, with an estimated BM dose of more than 2 Gy. However, none of these patients developed PHD. Therefore, the cumulative administered activity of 177Lu-DOTATATE and estimated BM dose are currently not a dominant factor for predicting PHD after PRRT with 177Lu-DOTATATE using our treatment regimen.
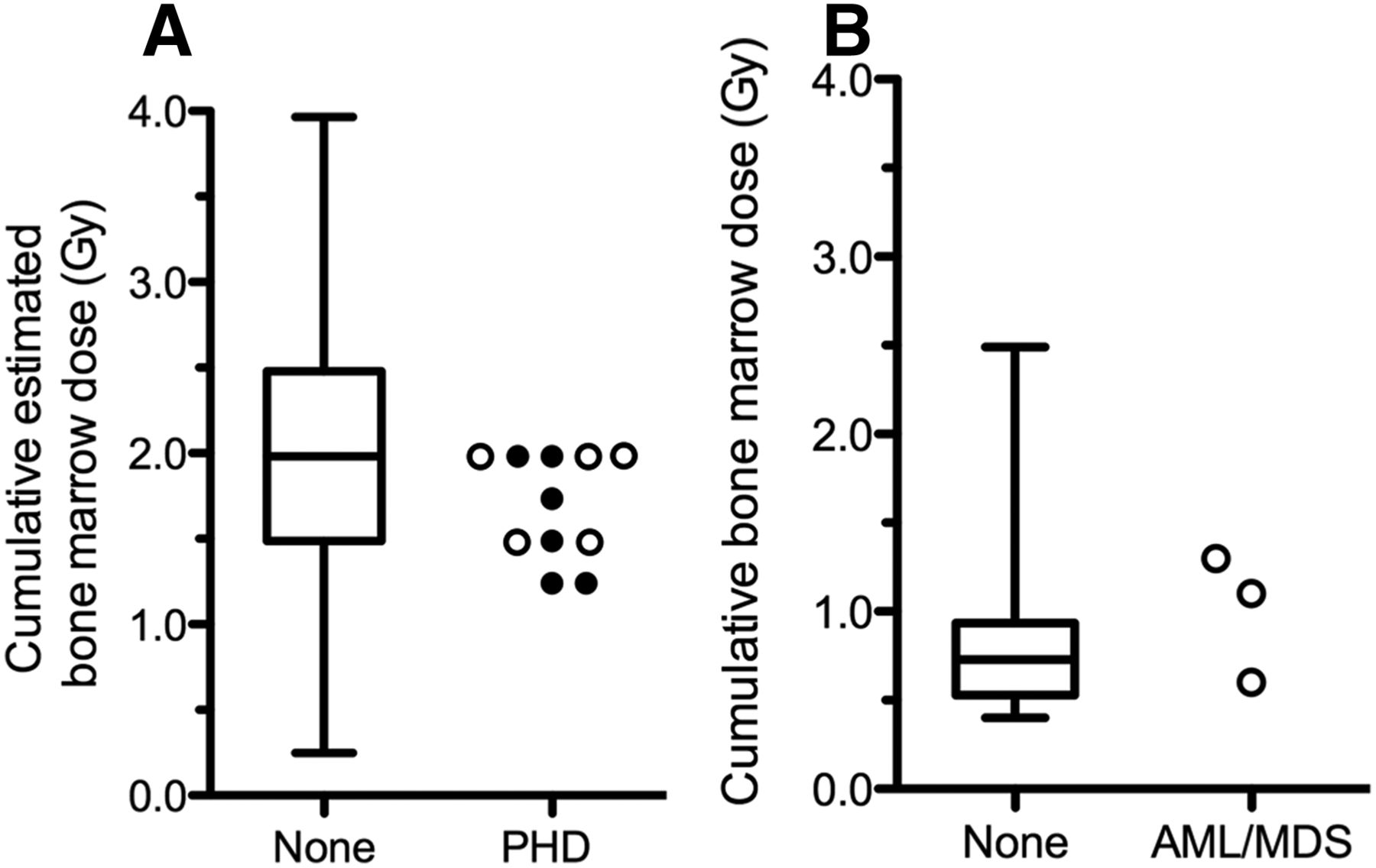
Comparison of PHD and cumulative dose to BM. (A) Cumulative estimated BM dose in 11 patients with PHD (including 5 AML/MDS ○ and 6 other diagnosis ● patients) and 263 patients without PHD. (B) Marrow dose in 3 patients with AML/MDS ○ and 28 patients without AML/MDS. Data for dosimetry analysis in subgroup of 807 patients were adopted from Bodei et al. (8). Whiskers represent minimum and maximum estimated BM dose in grays. Height of box shows interquartile range, and horizontal line in box is median estimated BM dose in grays.
In general, signs and symptoms in patients with MDS are nonspecific. Many patients are asymptomatic at diagnosis and come to the physician’s attention only after abnormalities are found on routine blood work (e.g., anemia, neutropenia, and thrombocytopenia) (24). First, common causes of anemia have to be excluded, such as nutrient deficiencies (iron, folate, and vitamin B12) and anemia secondary to renal failure (25). In our patient group, the red blood cells are the most frequently affected cell line, followed by a reduction in platelets or white blood cells. In more than half our patients, we observed a decrease in hemoglobin combined with a rise in mean corpuscular volume. The decrease in red blood cells reflects the imbalance between their production and their survival, whereas the increased mean corpuscular volume reflects abnormal blood cell production.
In another paper, we have identified several risk factors for subacute hematologic toxicity after PRRT with 177Lu-DOTATATE, such as impaired renal function, low white blood cell count, extensive tumor mass, high tumor uptake on the [111In-DTPA0]octreotide scan, or advanced age (7). As for PHD, Bodei et al. reported the following risk factors associated with MDS and leukemia after PRRT with 177Lu-DOTATATE (8): previous chemotherapy, tumor invasion of the BM, platelet toxicity grade, and other previous myelotoxic therapies. In our study, we could not identify any risk factors for GEP NET patients who develop PHD after PRRT with 177Lu-DOTATATE. However, analysis of all 367 patients with somatostatin receptor–positive tumors demonstrated significantly lower white blood cell counts in patients with PHD (Table 4). Also, a trend was observed in which subacute hematologic toxicity (grade 3–4) during PRRT was more frequent in patients with PHD than in those without.
In a recent study, a high incidence (20%) of MDS/AML after chemotherapy and PRRT with 177Lu-DOTATATE was reported in a small group of patients with metastatic GEP NET (26). A critical response was written about the limited (biased) group of patients in this study (27). The high dose of alkylating chemotherapy was the main contributing factor for development of MDS/AML in these patients. In our study, chemotherapy was not a risk factor, which might be explained by the fact that in our patient population lower doses of previous chemotherapy were given.
CONCLUSION
The prevalence of therapy-related PHD after PRRT with 177Lu-DOTATATE in GEP NET patients was 4%, implying a relative risk of 2.7. The median latency time to disease development was 41 mo.
In the group of GEP NET patients, no risk factors could be identified for the development of therapy-related PHD. Anemia combined with a rise in mean corpuscular volume occurred in half the patients with PHD related to PRRT with 177Lu-DOTATATE.
DISCLOSURE
Dik J. Kwekkeboom and Eric P. Krenning are shareholders and scientific advisors of Advanced Accelerator Applications (Adacap). Wouter W. de Herder receives speaker fees and research support from Ipsen/Novartis. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵† Deceased.
Published online Aug. 3, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 19, 2017.
- Accepted for publication July 7, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Therapy-Related Myeloid Neoplasms After [177Lu]Lu-PSMA Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer: A Case Series
- Limitations of the radiotheranostic concept in neuroendocrine tumors due to lineage-dependent somatostatin receptor expression on hematopoietic stem and progenitor cells
- Elevated Baseline Mean Corpuscular Volume Predicts the Development of Severe Hematologic Toxicity After 177Lu-DOTATATE Therapy
- SPECT/CT Image-Derived Absorbed Dose to Red Marrow Correlates with Hematologic Toxicity in Patients Treated with [177Lu]Lu-DOTATATE
- Rethinking Dosimetry: The Perils of Extrapolated External-Beam Radiotherapy Constraints to Radionuclide Therapy
- Dosimetric Quantities in Neuroendocrine Tumors over Treatment Cycles with 177Lu-DOTATATE
- Bone Marrow Absorbed Doses and Correlations with Hematologic Response During 177Lu-DOTATATE Treatments Are Influenced by Image-Based Dosimetry Method and Presence of Skeletal Metastases
- NANETS/SNMMI Procedure Standard for Somatostatin Receptor-Based Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE
- Safety, Pharmacokinetics, and Dosimetry of a Long-Acting Radiolabeled Somatostatin Analog 177Lu-DOTA-EB-TATE in Patients with Advanced Metastatic Neuroendocrine Tumors