


Article Figures & Data
Figures
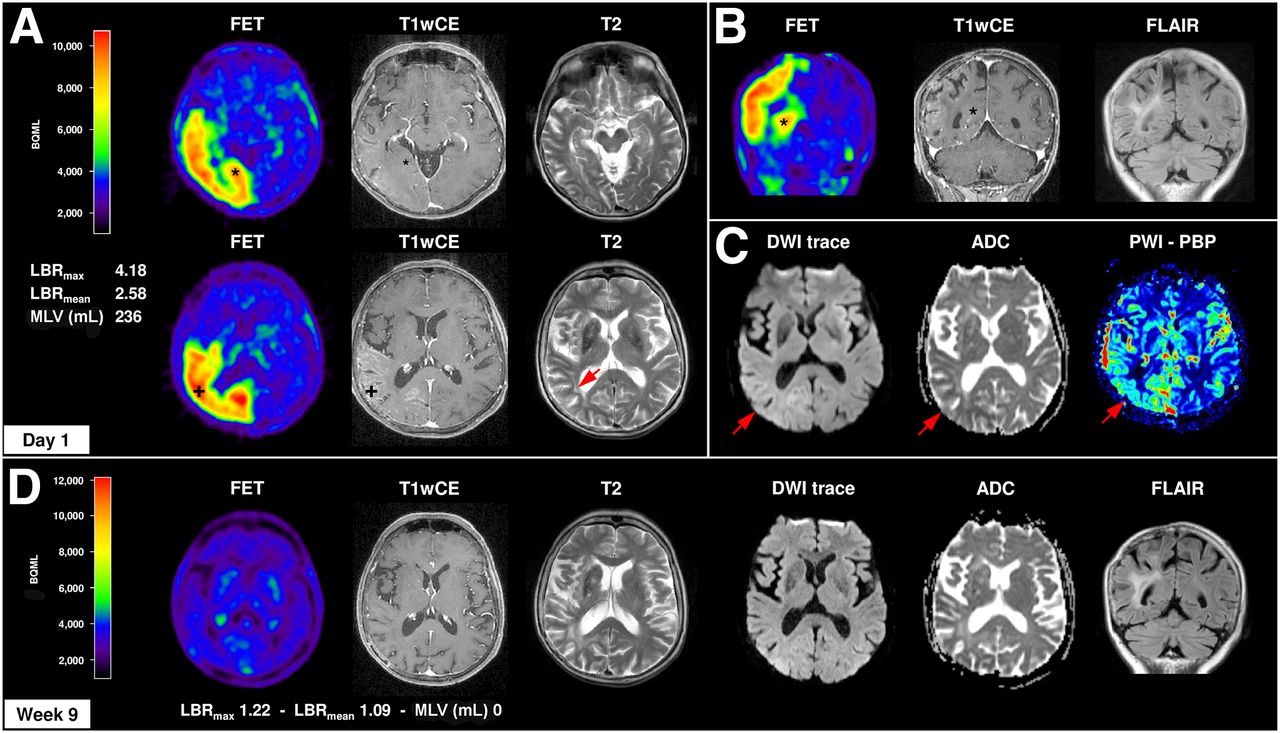
- FIGURE 1.
Structural and metabolic changes in MRI and 18F-FET PET in focal SE. Case 1 represents a 64-y-old woman with clinically stable right frontal anaplastic astrocytoma WHO III without residual tumor. In 2011, she developed a series of treatment-refractory motor SPS and a focal SE of left arm and leg, followed by a severe and prolonged postictal left hemiparesis for 4 wk. (A–C) MRI/18F-FET PET was performed simultaneously with motor SPS and revealed a distinct increased and extended cortical 18F-FET uptake right temporo–parieto–occipital (LBRmax, 4.18; LBRmean, 2.58) associated with cortical vasogenic (T2/FLAIR hyperintensity) and cytotoxic (diffusion-restriction in DWI + low ADC values) edema, contrast enhancement (T1wCE, BBB leakage), and hyperperfusion (PWI-PBP, baseline at peak map). 18F-FET uptake was observed independently from BBB disruption in cortex with (*) and without (+) contrast enhancement in T1wCE. (D) Nine weeks after seizure onset and antiepileptic treatment, structural and metabolic MRI and 18F-FET PET signal alterations completely resolved, except for slight cortical atrophy in T1 and T2/FLAIR. In 2014, same patient again developed treatment-resistant series of motoric SPS with prolonged postictal hemiparesis for 4 wk with similar morphologic and metabolic changes in MRI/18F-FET PET (LBRmax 4.02, LBRmean 2.50) (not shown).
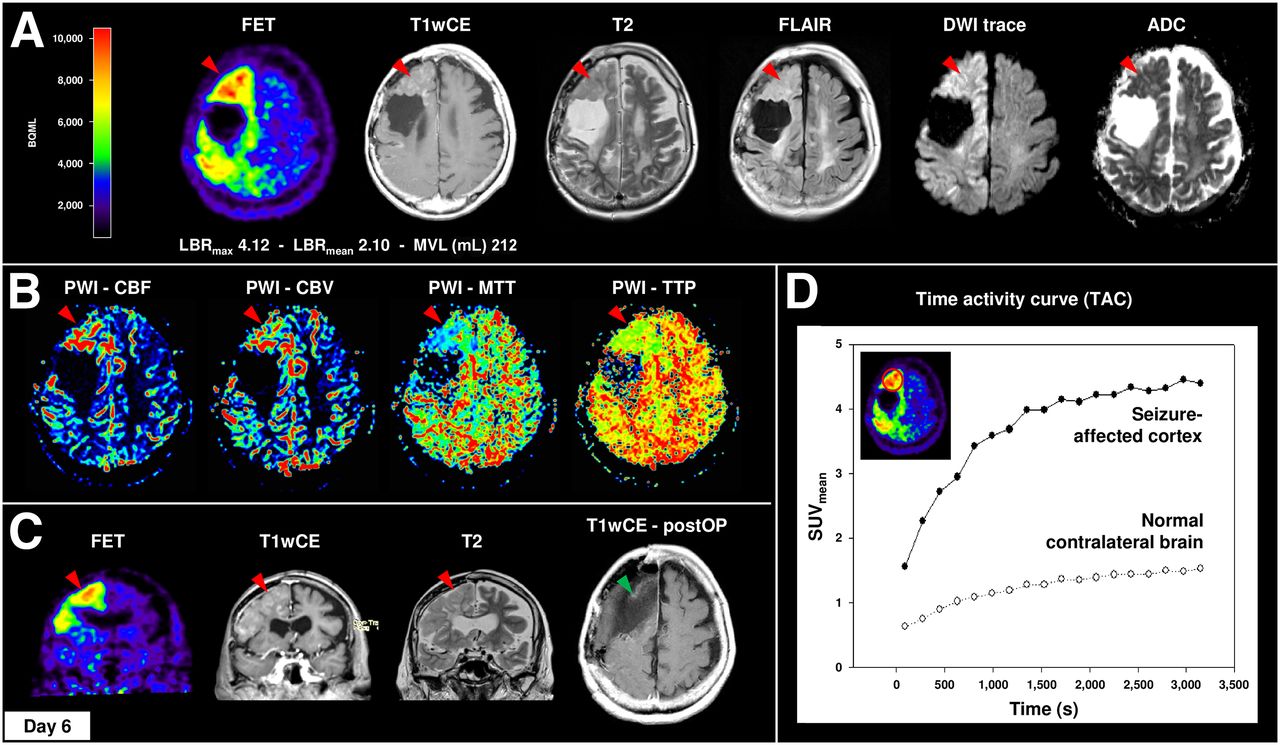
- FIGURE 2.
Widespread 18F-FET uptake, vasogenic and cytotoxic edema, contrast enhancement, and hyperperfusion with strict gyral pattern during nonconvulsive SE. Case 3 demonstrates a 66-y-old woman with clinically stable right frontal oligodendroglioma WHO II without residual tumor. In 2014, the patient presented with repeated CPS followed by treatment-resistant nonconvulsive SE. 18F-FET PET revealed distinct elevated cortical 18F-FET uptake of right hemisphere with frontal and parietal accentuation (LBRmax, 4.42; LBRmean, 2.45), corresponding to cortical contrast enhancement in T1wCE, marked gyral vasogenic (T2/FLAIR, cortical swelling), and cytotoxic (DWI/ADC) edema (A) and cortical hyperperfusion in DSC-PWI (B). (C) Clinical deterioration in combination with MRI and 18F-FET PET imaging was interpreted as tumor recurrence. Therefore, patient underwent subtotal frontal lobe resection without any histologic evidence of tumor progression. (D) Additional 18F-FET kinetic analysis of right frontal lesion and normal contralateral brain demonstrated SUVmean time–activity course curve pattern with continuously increasing 18F-FET uptake without washout. CBF = cerebral blood flow; CBV = cerebral blood volume; MTT = mean transit time; TTP = time to peak.
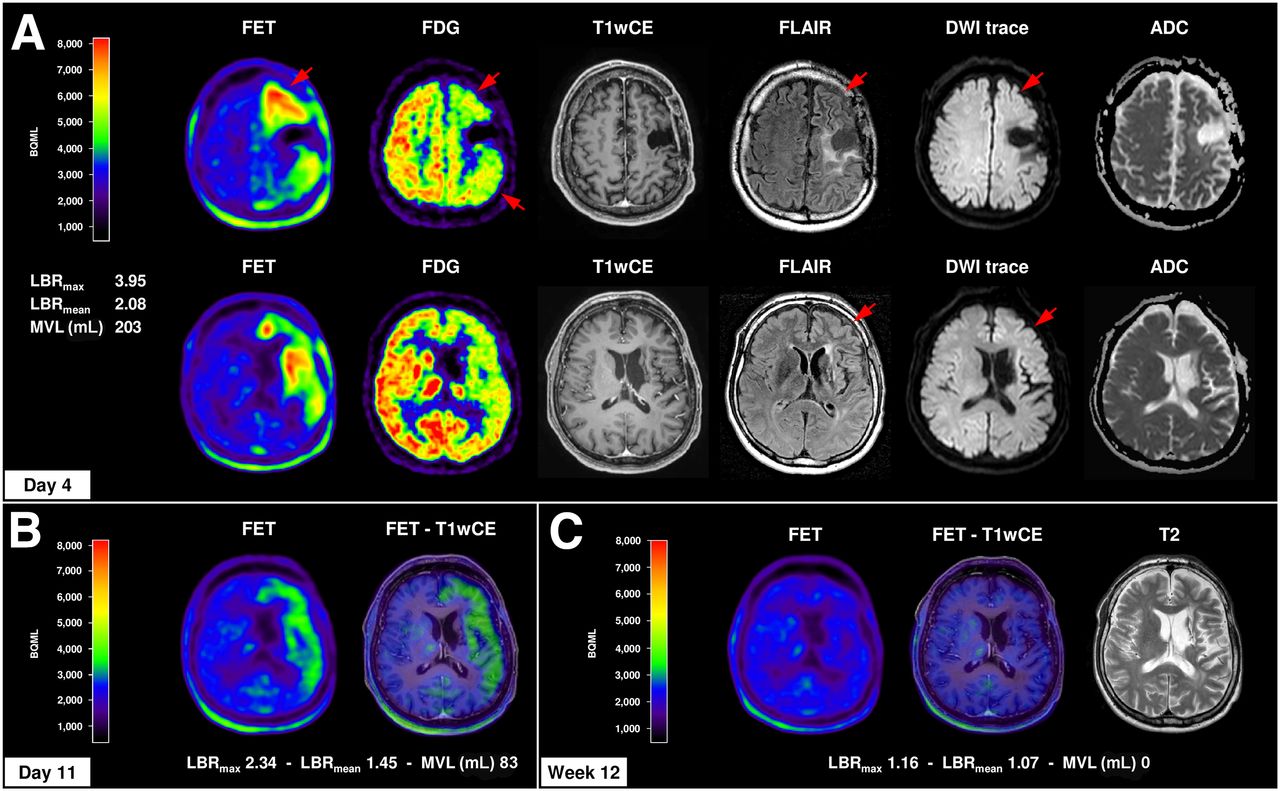
- FIGURE 3.
Cortical amino cid metabolism in 18F-FET PET in course of prolonged postictal episode. Case 4 demonstrates 44-y-old man with clinically stable anaplastic astrocytoma WHO III without any residual tumor over years who presented with TCS followed by severe and prolonged postictal symptoms (global aphasia, right-sided hemiplegia, and hemineglect) over 8 wk. (A) MRI (day 1) and 18F-FET PET (day 4) showed distinct increased and extended cortical 18F-FET uptake of left brain hemisphere (LBRmax, 3.95; LBRmean, 2.08) with frontal and temporal accentuation, corresponding to slight cortical vasogenic and cytotoxic edema (T2/FLAIR, DWI/ADC) without contrast enhancement (T1wCE). EEG monitoring, 18F-FDG PET (glucose hypometabolism, red arrows), and 99mTc-HMPAO SPECT (hypoperfusion, only written medical report available), however, revealed no evidence of SE. (B) For 18F-FET PET 11 d after symptom onset and 7 d after first 18F-FET PET, slight regression of cortical 18F-FET uptake (LBRmax, 2.34; LBRmean, 1.45) was observed. (C) Patient slowly recovered within 8 wk after seizure onset. 18F-FET PET and MRI 12 wk after symptom onset demonstrated complete recovery of cortical 18F-FET uptake and brain edema; only residual cortical atrophy in T1 and T2/FLAIR sequences remained.
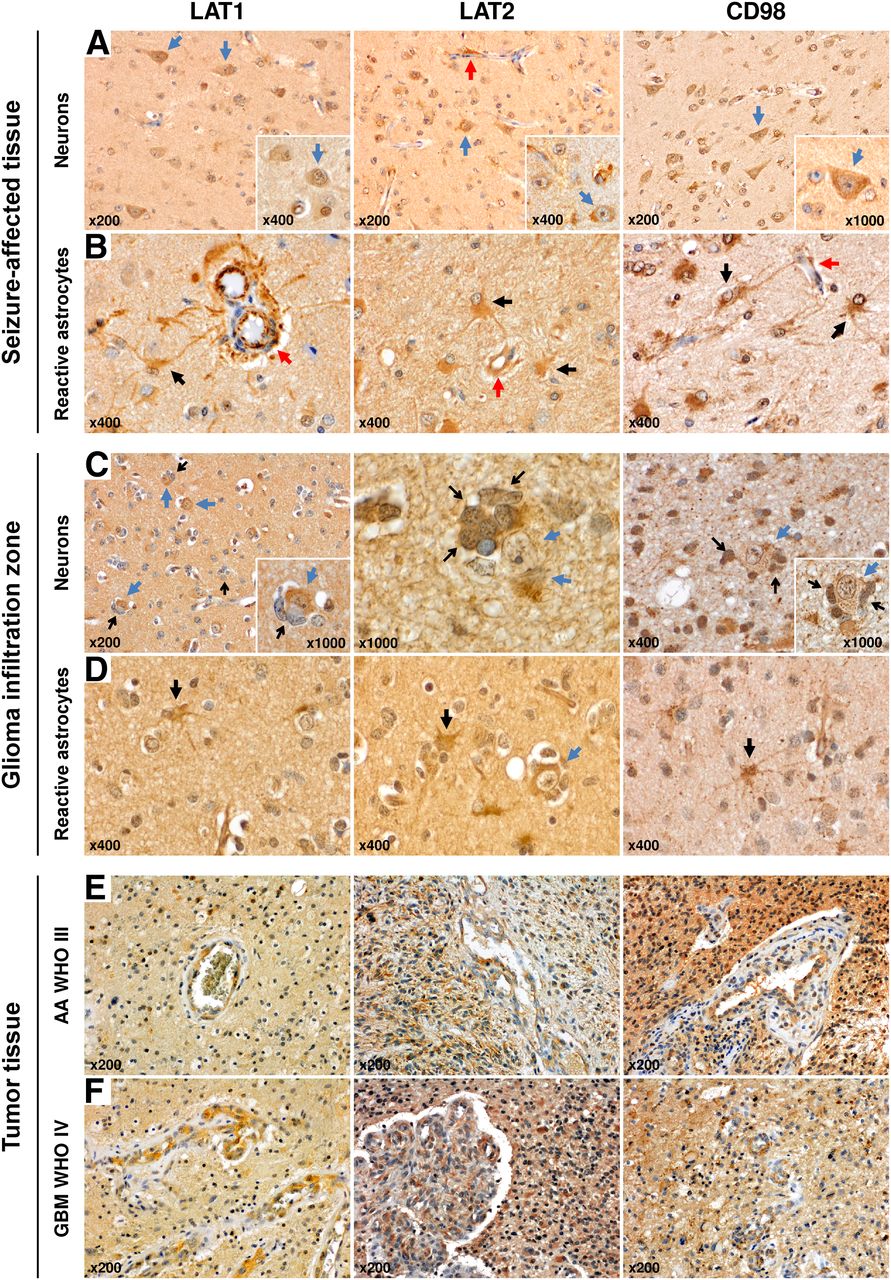
- FIGURE 4.
LAT1, LAT2, and CD98 protein expression pattern in seizure-affected and glioma tissue. (A) LAT1, LAT2, and CD98 showed strong and widespread expression in neurons of seizure-affected cortex obtained from patient with nonconvulsive SE and subtotal frontal lobe resection (case 3; Fig. 2; blue arrow, neuron; red arrow, vessel). (B) LAT1, LAT2, and CD98 were also detected in brain endothelial cells and reactive astrocytes (astrocyte–endothelium interaction as part of BBB; red arrow, vessel; black arrow, reactive astrocyte). Overall, LAT1, LAT2, and CD98 expression from neurons was more frequent than that from reactive astrocytes as reactive astrocytosis was only focally represented. (C) Within infiltration zone of astrocytoma WHO grade II cortical neurons revealed pronounced staining of LAT1/LAT2/CD98, in particular when glioma cells directly interact with neurons (tumor cells as satellites of neurons; blue arrow, neuron; open black arrow, satellitosis by tumor cells). (D) In addition, sporadic LAT1/LAT2/CD98-positive reactive astrocytes were observed within tumor infiltration zone. In comparison, tumor cells and tumor endothelium of anaplastic astrocytoma WHO grade III (E) and glioblastoma WHO grade IV (F) were also strongly positive for LAT1, LAT2, and CD98 expression.




Tables
Case Center Age (y) Sex Diagnosis Tumor localization Treatment Disease status Seizure disorder before 1 + 2* F 64 F AA (1989) Right frontal SU, RA, CT 1989 SD, no residual tumor Yes (motor SPS, TCS) 3 R 66 F O (1985) Right frontal SU, RA, PCV 1985 SD, no residual tumor Yes (motor SPS) 4 S 44 M A (1991) Left frontotemporal SU 1991, 1996, 1997 SD, no residual tumor Yes (TCS) OA (1996) RA/BCNU 1997 AOA (1997) 5 R 54 M A (2014) Left frontoparietal SU, TMZ 2014 PD of residual tumor Yes (motor SPS) 6 S 68 F O (2004) Right frontal SU 2004 SD, residual tumor Yes (motor SPS, TCS) AO (2011) SU, RA/TMZ 05/2011 CCNU 11/2011 7 R 51 M GBM (2013) Right frontal SU 2013 ID of GBM Yes (CPS, TCS) 8 R 29 F A (2012) Right frontoparietal SU 2012, TMZ 2012–2013 PD of residual tumor Yes (motor/sensory SPS, TCS) sGBM (2015) SU + RA/TMZ 2015 9 R 45 M AO (2012) Right frontotemporal SU, RA/TMZ 2012 SD, residual tumor No PC 2014 BEV/CCNU 2014–2015 10 R 76 F Nonconvulsive SE caused by septic encephalopathy (6/2013) Anticonvulsive treatment No recovery Yes (nonconvulsive SE 4/2013) 11 S 66 F Embolic cerebral ischemia (2011) Anticonvulsive treatment Seizure-free after 1 d No ↵* Patient presented with same clinical symptoms and EEG findings according to SE in 2011 and 2014. At both time points combined MRI and 18F-FET PET imaging was available.
F = Freiburg, Germany; R = Regensburg, Germany; S = Salzburg, Austria; O = oligodendroglioma WHO II; A = astrocytoma WHO II; OA = oligoastrocytoma WHO II; AA = anaplastic astrocytoma WHO III; AOA = anaplastic oligoastrocytoma WHO III; AO = anaplastic oligodendroglioma WHO III; GBM = glioblastoma WHO IV (s, secondary); SU = surgery; RA = radiotherapy; TMZ = temozolomide; BCNU = carmustine; CCNU = lomustine; PC = procarbazine + CCNU; PCV = procarbazine + CCNU + vincristine; BEV = bevacizumab; SD = stable disease; PD = progressive disease; ID = initial diagnosis.
- TABLE 2
Overview on Seizure Activity, EEG Findings, MRI, and 18F-FET PET Imaging and Disease Course of Study Population
Cases 1 and 2 Findings TR serial motor SPS and focal SE, prolonged PH (2011)** TR serial motor SPS and focal SE, prolonged PH (2014)** Case 3: serial CPS followed by nonconvulsive SE, prolonged PS Case 4: TCS followed by prolonged PS Case 10: serial CPS followed by nonconvulsive SE (septic encephalopathy) Case 5: daily (5–10) motor SPS followed by focal motor SE Case 6: repeated motor SPS, secondarily TCS followed by focal acoustic SE Case 11: TCS with PH Case 7: repeated CPS and 1 secondarily TCS Case 8: daily (1–3) sensory SPS Case 9: daily (1–2) CPS EEG SA SA SE SA SE SE ED, SA ED, SA ED, SA NA SA MRI Hem+ R R R L L L R R R R R Lobe+ P, T, O P, T, O F, P, T F, P, T P, T, O F F, P F F F F T1wCE† + + + – – – – – – – – T2/FLAIR† ++ ++ ++ ++ ++ ++ + + + – – DWI/ADC† ++ ++ ++ ++ ++ ++ ++ ++ + – – PWI† ++ ++ ++ NA NA ++ NA NA NA NA – 18F-FET PET* LBRmax 4.18 4.02 4.42 3.95 2.47 2.63 1.83 1.81 1.78 1.75 1.69 LBRmean 2.58 2.50 2.45 2.08 1.68 1.71 1.46 1.42 1.54 1.57 1.43 MLV 236 271 212 203 76 26 19 23 8 16 12 Uptake extension‡ +++ +++ +++ +++ +++ ++ ++ + + + + Epi-PET duration§ Sim Sim 6 d 4 d 5 d 7 d 5 d 3 d 5 d Sim Sim Disease course Biopsy/surgery¶ BIEPI – SUEPI – – – SUEPI – SUTU SUTU – Symptom duration║ 4 w 4 w NA 8 w NR 2 w 1 w 1 d 1 d – – 18F-FET PET preinvestigation (-) and follow-up (+) +9w +12 w NA +11 d, +12 w NA NA –4 w NA +8 w –10 w +10 w 18F-FET reversibility Yes Yes – Yes – – Yes – Yes Yes Yes LBRmax 1.22 1.24 2.34, 1.16 1.18 1.20 1.23 1.19 LBRmean 1.09 1.11 1.45, 1.07 1.09 1.07 1.10 1.12 MLV 0 0 83, 0 0 0 0 0 ↵* Evaluation of structural and metabolic cortical changes in MRI and 18F-FET PET; +Tumor localization ([L] left, [R] right and [F] frontal, [P] parietal, [T] temporal, [O] occipital); †Visual assessment of cortical MRI changes ([–] no, [+] weak, [++] strong); ‡Visual assessment of cortical 18F-FET uptake extension ([+] focal [1 lobe and ≤ 5 cm], [++] enlarged [1 lobe and > 5 cm], [+++] widespread [more than 1 lobe]); §Time period between seizure onset or last EEG finding and 18F-FET PET in (d) days or simultaneous (sim); ¶SUTU, surgery due to tumor progression; SUEPI/BIEPI, surgery/biopsy due to false-positive tumor diagnosis in MRI/PET; –No surgery/biopsy; ║Time period between seizure onset and complete recovery or adequate seizure control ([d] days, [w] weeks); **Patient presented with identical clinical symptoms and EEG findings in 2011 and 2014 and was evaluated twice.
ED = epileptic discharges; Hem = hemisphere; LBR = lesion-to-brain ratio; MLV = metabolic lesion volume (mL); NA = not assessed or available; NR = not recovered; PH = postictal hemiparesis; PS = postictal symptoms; SA = slow activity; Sim = simultaneous; TR = treatment-resistant.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comprehensive Update and Review of Clinical and Imaging Features of SMART Syndrome
- Comprehensive Update and Review of Clinical and Imaging Features of SMART Syndrome
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Early Treatment Response Assessment Using 18F-FET PET Compared with Contrast-Enhanced MRI in Glioma Patients After Adjuvant Temozolomide Chemotherapy