


Abstract
18F-fluorocholine is a specific promising agent for imaging tumor cell proliferation, particularly in prostate cancer, using PET/CT. It is a beneficial tool in the early detection of marrow-based metastases because it excludes distant metastases and evaluates the response to hormone therapy. In addition, 18F-fluorocholine has the potential to differentiate between degenerative and malignant osseous abnormalities because degenerative changes are not choline-avid; however, the agent may accumulate in recent traumatic bony lesions. On the other hand, 18F-NaF PET/CT can indicate increased bone turnover and is generally used in the assessment of primary and secondary osseous malignancies, the evaluation of response to treatment, and the clarification of abnormalities on other imaging modalities or clinical data. 18F-NaF PET/CT is a highly sensitive method in the evaluation of bone metastases from prostate cancer, but it has problematic specificity, mainly because of tracer accumulation in degenerative and inflammatory bone diseases. In summary, 18F-NaF PET/CT is a highly sensitive method, but 18F-fluorocholine PET/CT can detect early bone marrow metastases and provide greater specificity in the detection of bone metastases in patients with prostate cancer. However, the difference seems not to be significant.
Prostate cancer is the second most common malignancy among men and the sixth cause of death from cancer throughout the world. Older age, African-American race, tobacco use, and family history are recognized as some of the risk factors for this cancer (1,2). The widespread use of the prostate-specific antigen in the screening examination has caused a decrease in the number of patients primarily diagnosed with advanced disease and metastases at presentation (3). Tissue biopsy confirms the final diagnosis in suspected cases (4). Although prostate cancer grows slowly, it potentially can invade the nearby organs or metastasize distantly, most commonly to the axial skeleton (5,6). Extensive distant metastases make the prognosis poor (1,6). Therefore, early diagnosis and treatment are essential in this group of cancer patients.
Diverse imaging modalities, including nuclear medicine methods, are used for staging and restaging prostate cancer. PET/CT is a tool that has become increasingly available during the past decade; it uses positron-emitting radiopharmaceuticals for imaging most malignancies and has the unique capability of merging the biologic information from PET with the anatomic data from CT in a single examination. Various PET radiotracers have been examined in the evaluation of prostate cancer according to increased glucose metabolism (18F-FDG), amino acid transportation and synthesis of proteins (11C-methionine), synthesis of fatty acids (11C-acetate), cellular phospholipid membrane proliferation (11C- and 18F-choline), expression of androgen receptors (16β-18F-fluoro-5α-dihydrotestosterone), depiction of prostate-specific membrane antigen (68Ga), and osteoblastic activity of osseous metastatic lesions (18F-NaF) (7).
This article reviews the value of 18F-NaF PET/CT and 18F-fluorocholine PET/CT in the assessment of bone metastases in prostate cancer.
18F-FLUOROCHOLINE PET/CT
Choline is a quaternary ammonium base and a precursor of phospholipids such as phosphatidylcholine (lecithin), which is integrated into the cell membrane during cell proliferation, an event that is augmented in malignant tissues such as prostate cancer. Likewise, an upregulation of choline kinase enhances the intracellular transport of choline to build up new membranes in prostatic cancerous cells (8–10). Hence, choline uptake is considered to be a marker of cell proliferation, particularly in malignancies. This characteristic led to the innovation of labeling choline with positron emitters such as 18F and 11C and using them in the evaluation of prostate cancer (11–17).
Radiolabeled choline is physiologically distributed in the liver, spleen, pancreas, and other exocrine glands and excreted in urine (18,19). Urinary excretion is a limitation for 18F-fluorocholine in assessing pelvic organs such as the prostate gland, but it can be compensated for by early dynamic imaging and coregistration with a CT scan (20,21). Although degenerative joint disease normally does not show abnormally increased 18F-fluorocholine uptake, recent trauma and fractures may demonstrate 18F-fluorocholine avidity (22).
A metaanalysis by Shen et al. (23) of 27 studies compared the diagnostic performance of 11C- and 18F-choline PET/CT, MRI, bone SPECT, and bone scintigraphy for detecting bone metastases in patients with prostate cancer. On a per-patient basis, the pooled sensitivities of 11C- and 18F-choline PET/CT, MRI, and bone scintigraphy were 91%, 97%, and 79%, respectively, and the pooled specificities were 99%, 95%, and 82%, respectively. On a per-lesion basis, the pooled sensitivities of 11C- and 18F-choline PET/CT, bone SPECT, and bone scintigraphy were 84%, 90%, and 59%, respectively, and the pooled specificities were 93%, 85%, and 75%, respectively. This metaanalysis indicated that MRI was better than 11C- and 18F-choline PET/CT and bone scintigraphy on a per-patient basis. On a per-lesion basis, 11C- and 18F-choline PET/CT were clearly better than bone SPECT and bone scintigraphy.
18F-FDG, the most readily available PET tracer, showed limited value in the assessment of prostate cancer patients. In a study comparing the value of 18F-fluorocholine with that of 18F-FDG and conventional imaging (whole-body bone scanning and contrast-enhanced CT of suspected lesions) in 16 prostate cancer patients, Beauregard et al. (24) reported that 18F-fluorocholine PET/CT had a per-patient sensitivity of 100% for the detection of bone metastases, versus 67% for 18F-FDG PET/CT and conventional imaging.
A review of the medical literature shows that investigators recognize 18F-fluorocholine PET/CT as a beneficial tool for staging intermediate- to high-risk prostate carcinomas. A prospective study by our group showed that 18F-fluorocholine PET/CT could be a useful modality for evaluating patients who are at a high risk for extracapsular spread of prostate cancer and for excluding distant metastases before prostate surgery. The study revealed a 20% upstaging among the high-risk patients, and the management of 15% of all enrolled patients was changed on the basis of PET/CT findings (9).
Another study by our group reconfirmed the previous data and revealed that skeletal uptake of 18F-fluorocholine was a strong predictor of bone metastases, particularly in patients who did not undergo antiandrogen therapy (25,26).
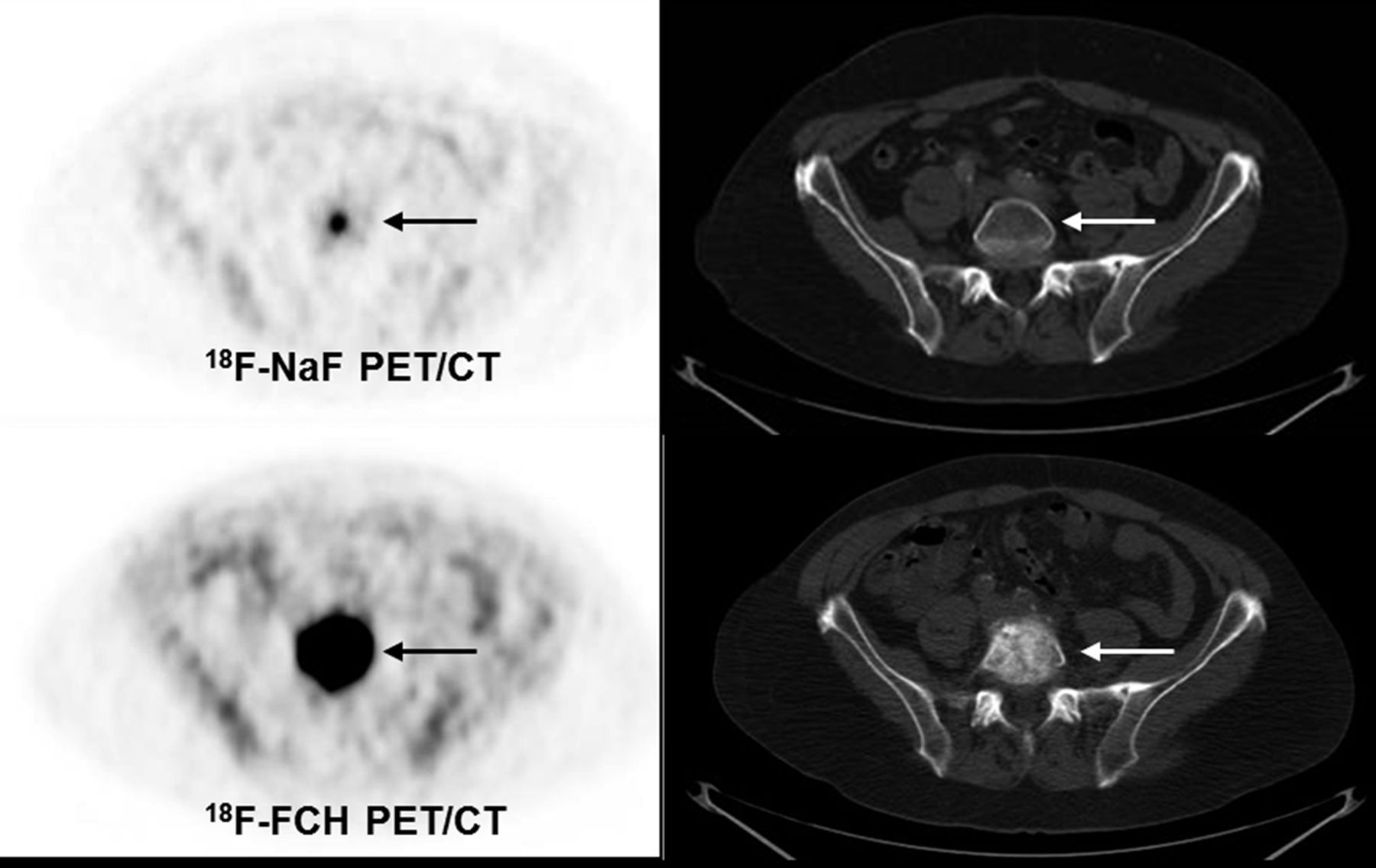
To investigate the role of 18F-fluorocholine PET/CT in detecting bone metastases in prostate cancer patients, our group prospectively examined 70 patients in a study that revealed a promising role for this modality in detecting early bone metastasis, finding a sensitivity, specificity, and accuracy of 79%, 97%, and 84%, respectively (Fig. 1). Interestingly, the metastatic lesions could be categorized into 3 groups: bone marrow involvement (positive on 18F-fluorocholine PET, negative on CT), typically osteoblastic but less often osteoclastic lesions (positive on 18F-fluorocholine PET, positive on CT), and densely sclerotic lesions (negative on 18F-fluorocholine PET, positive on CT). Also, a cutoff value of 825 Hounsfield units has been determined; all lesions with a higher value demonstrated no metabolic uptake of 18F-fluorocholine, a finding that may be the result of therapy-induced death of cancerous cells (22).
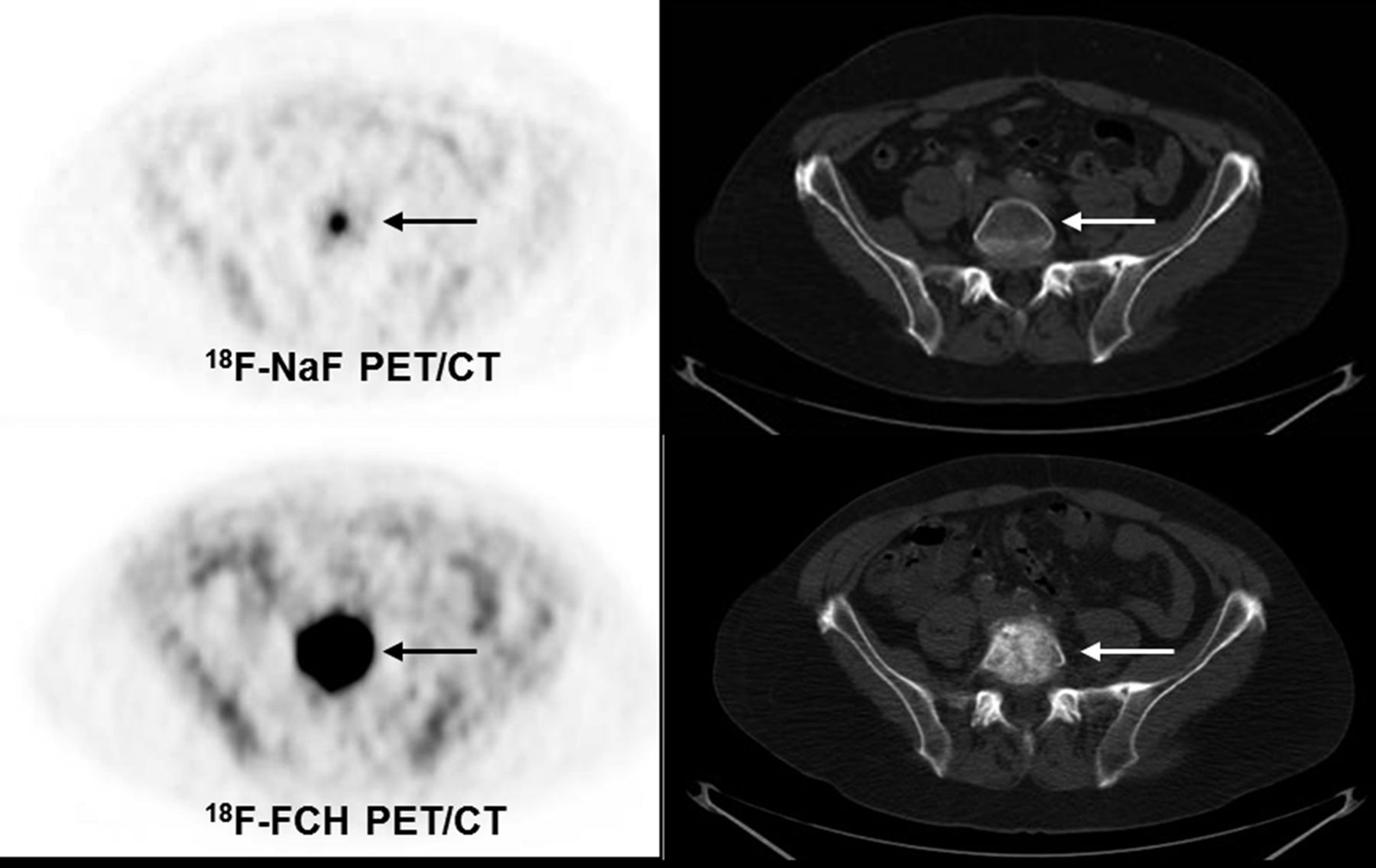
Follow-up 18F-fluorocholine (FCH) PET images of high-risk prostate cancer patient. Suspiciously increased tracer uptake on lumbar spine (upper row left, arrow) without any morphologic change on CT (upper row right, arrow) is suggestive of bone marrow metastasis. Follow-up 18F-fluorocholine scan shows significantly increased tracer uptake on lumbar spine, suggestive of disease progression (lower row left, arrow) corresponding to suspicious sclerotic changes on CT (lower row right, arrow).
In a systematic literature review, Bauman et al. (27) found that 18F-fluorocholine PET/CT was considered useful in staging primary and recurrent prostate cancer and in guiding prostate biopsy and radiotherapy. They emphasized the potential of combining whole-body imaging and pelvic imaging to assess distant metastases in a single session, which is the unique advantage of 18F-fluorocholine PET/CT over other staging modalities.
Because uptake of 18F-fluorocholine by cancer cells is inversely correlated with response to hormone therapy, 18F-fluorocholine PET/CT is likely potent in monitoring the response to such therapy (28).
It is noteworthy that in recurrent prostate cancer, particularly in patients who have undergone hormone therapy, the presence of mild to moderate nonhomogeneous reactive bone marrow uptake of 18F-fluorocholine may cause uncertainty in image interpretation. To solve the problem, a dual-time imaging protocol is applied. Increasing tracer uptake and SUVs on delayed images (i.e., 90–120 min after tracer injection) is an important clue in differentiating malignant from nonmalignant lesions (22).
18F-FLUOROCHOLINE PET/MRI
Recently, hybrid 18F-fluorocholine PET/MRI has been introduced as a promising modality in evaluating prostate cancer. Wetter et al. (29) showed that using simultaneous 18F-fluorocholine PET and MRI makes it possible to fuse MRI diffusion-weighted images and PET with high-resolution T2-weighted prostate images to quantitatively measure molecular and metabolic markers of prostate malignancy in a single study. In a separate research project, Wetter et al. (30) measured the apparent diffusion coefficient and SUV in patients with prostate cancer to differentiate benign from malignant lesions. They concluded that both parameters differ significantly between malignant and intact tissues, without any significant correlation between them, perhaps because each represents a different aspect of tumor biology. However, another study by those authors (31) revealed a significant inverse correlation between SUV and apparent diffusion coefficient in osseous metastases (P = 0.02).
SUVmax and SUVmean may be significantly lower in 18F-fluorocholine PET/MRI than in 18F-fluorocholine PET/CT, possibly because of differences in the attenuation correction techniques used. Furthermore, the biodistribution and biokinetics of 18F-fluorocholine may differ among subsequent examinations and in different organ systems (32).
In a study by Samarin et al. (33) comparing the value of PET/MRI and PET/CT in the assessment of bone metastases in various cancers, the authors concluded that PET/MRI offers higher interpreter confidence and improves conspicuity in bone metastases. However, the overall detection rate was not different. The highest possible clinical impact of PET/MRI appears to be in patients with limited, early bone metastatic disease (33).
In summary, although PET/MRI may offer higher lesion conspicuity and diagnostic confidence than PET/CT in the assessment of bone lesions in oncology patients, the two modalities seem to be of equal value for identifying patients with bone metastases (34).
18F-NAF PET/CT
Approximately 4 decades ago, 18F-NaF was used to image the skeleton at a time when no commercial PET scanners were in use. However, its short half-life and high energy (511 keV) were two flaws at that time, which notably limited its application. After decades and the widespread use of PET/CT scanners, 18F agents were revitalized for both research and clinical imaging (7).
There are several indications for 18F-NaF PET/CT, including assessment of primary and secondary osseous malignancies, evaluation of response to treatment, and clarification of clinical data or abnormalities on other imaging modalities (35). Review of the correlated sensitivity and specificity of 18F-NaF PET/CT in the medical literature shows varying results. Although Even-Sapir et al. (35) calculated a sensitivity and specificity of 100%, Poulsen et al. (36) reported a sensitivity of 93% and an unexpected specificity of 54%, most likely because of the high number of false-positive lesions associated with degenerative or inflammatory changes in older patients, who made up the population of that study.
Similar to other 18F-labeled radiopharmaceuticals, 18F-NaF is produced by a cyclotron and has an approximate half-life of 110 min. Physiologically, it shows osteoblastic activity by attaching to sites of new bone formation. The uptake mechanism of 18F-NaF, much like 99mTc-methylene diphosphonate, is by chemisorption to hydroxyapatite, with resultant conversion to fluoroapatite and a hydroxyl group (37):
Two major parameters that determine the 18F-NaF uptake are regional blood flow and osteoblastic activity (30). With a suggested adult dose of 1.5–3.7 MBq/kg (maximum, 370 MBq) and a first-pass clearance of nearly 100% (38,39), about 50% of the administered dose is taken up in the osseous structures, 30% diffuses in red blood cells, and the remainder is eliminated in urine within 6 h of injection (40). Therefore, when preparing a patient for a conventional whole-body bone scan with the urinary bladder as the target organ, hydration with at least a half-liter of water before and after imaging and frequent voiding are strongly recommended to reduce radiation exposure as much as possible (39,40).
In comparison with conventional bone scintigraphy, 18F-NaF PET/CT is more sensitive and specific for the detection of osseous metastases from prostate cancer. In a comparative study by Even-Sapir et al. (35), the calculated sensitivity and specificity for planar bone scintigraphy were 70% and 57%, respectively, compared with 100% and 100% for 18F-NaF PET/CT. However, because of the mechanism of action and uptake, and because of nonspecific characteristics, increased uptake is seen in degenerative changes (36). Therefore, one of the key points in the interpretation of 18F-NaF PET/CT studies is to consider this issue, correlate the PET findings with morphologic changes on CT, and ascertain that the uptake is not associated with the end plates or joint surfaces. Hence, correlation of functional findings on 18F-NaF PET with anatomic information on CT improves the specificity of this modality (41). Similar to the weaknesses of other PET studies, small metastatic lesions may show no uptake; that shortcoming should be kept in mind at the time of interpretation, particularly when reviewing the spine (42,43).
In addition, the value of 18F-NaF PET/CT in the detection of early bone marrow metastases is unclear. Some studies have reported that 18F-NaF PET/CT is also a sensitive modality for the detection of lytic and early marrow-based metastases (44). In a study by our group, 10 metastatic bone marrow lesions that were detected by 18F-fluorocholine PET/CT were negative on 18F-NaF PET/CT (45). Therefore, positive findings on 18F-NaF PET without corresponding morphologic changes on CT might reflect an early phase of sclerotic activity—microsclerosis—without visible morphologic changes. The explanation for positive 18F-NaF PET findings without sclerotic changes on CT might also be a reactive osteoblastic activity that accompanies lytic lesions and malignant marrow deposits and that is reflected by the increased uptake of 18F-NaF in the periphery of the lesions (45).
Another role of 18F-NaF PET/CT is the assessment of response to treatment in patients with metastatic prostate cancer (46). However, interim studies should be reported with caution because the flare phenomenon may cause overinterpretation of the disease. In a recent study, Kairemo and Joensuu (47) demonstrated that the flare phenomenon has been seen in 3 of 6 patients who underwent interim 18F-NaF PET/CT after the first cycle of 223Ra-dichloride treatment. The authors suggested that monitoring the therapy response by 18F-NaF PET/CT might provide better information after the treatment is completed.
In summary, considering the increased availability of PET/CT systems and the lower cost of PET tracers, we believe that in the near future 18F-NaF PET/CT will replace 99mTc- methylene diphosphonate conventional whole-body bone scintigraphy for assessing bone metastases in prostate cancer (42).
COMPARISON OF 18F-NAF WITH 18F-FLUOROCHOLINE PET/CT
Several investigations have compared 18F-NaF PET/CT with 18F-fluorocholine PET/CT in the detection of osseous metastases from prostate cancer. Langsteger et al. (48) prospectively evaluated 40 patients with prostate cancer using both modalities and found a patient-based sensitivity of 91% versus 91%, specificity of 89% versus 83%, and accuracy of 90% versus 88% for 18F-fluorocholine and 18F-NaF PET/CT, respectively. However, no significant difference was noted between the diagnostic accuracy of the two modalities. Also, no significant difference was shown in site-based performance among patients referred for initial staging; however, in patients with a recurrence, 18F-fluorocholine PET/CT revealed a higher specificity (96% vs. 91%; P = 0.02) but a comparable sensitivity of 89%. Finally, those authors concluded that in patients with recurrent prostate cancer, 18F-fluorocholine PET/CT, if available, is preferred (48).
Our group compared the value of 18F-NaF and 18F-fluorocholine PET/CT in prostate cancer patients with skeletal metastases and found that 18F-fluorocholine PET/CT may localize the bone marrow metastatic lesions earlier than 18F-NaF PET/CT (45). In the same study, we also examined the intensity of malignant versus benign bone lesions detected on 18F-NaF PET/CT using semiquantitative analysis by SUV. We found that it is not possible to differentiate benign from malignant lesions at SUV levels lower than 45. However, an interesting finding was that all lesions with SUV levels greater than 45 were malignant. Also, 19 malignant bone lesions (16%) detected by 18F-NaF PET/CT showed no significant morphologic changes on CT. This might be caused by early phases of sclerotic activity (i.e., microsclerosis) having no visible morphologic changes on CT. In conclusion, both 18F-fluorocholine PET/CT and 18F-NaF PET/CT showed nearly the same accuracy (85% vs. 86%) for the detection of bone metastases in prostate cancer patients. 18F-NaF PET/CT was more sensitive (Fig. 2).

Comparison of 18F-NaF PET and 18F-fluorocholine (FCH) PET images in prostate cancer patient (prostate-specific antigen level, 72.0 ng/mL; Gleason score, 8) after hormone therapy (1-d interval between 2 studies). 18F-NaF PET image (A) shows markedly more lesions than 18F-fluorocholine PET image (B).
We also noted that hormone therapy may be associated with increasing bone mineralization and sclerotic activity in malignant lesions, which may cause discrepancies between 18F-fluorocholine and 18F-NaF PET/CT (e.g., 18F-fluorocholine–negative and 18F-NaF–positive densely sclerotic lesions) (Figs. 3 and 4).

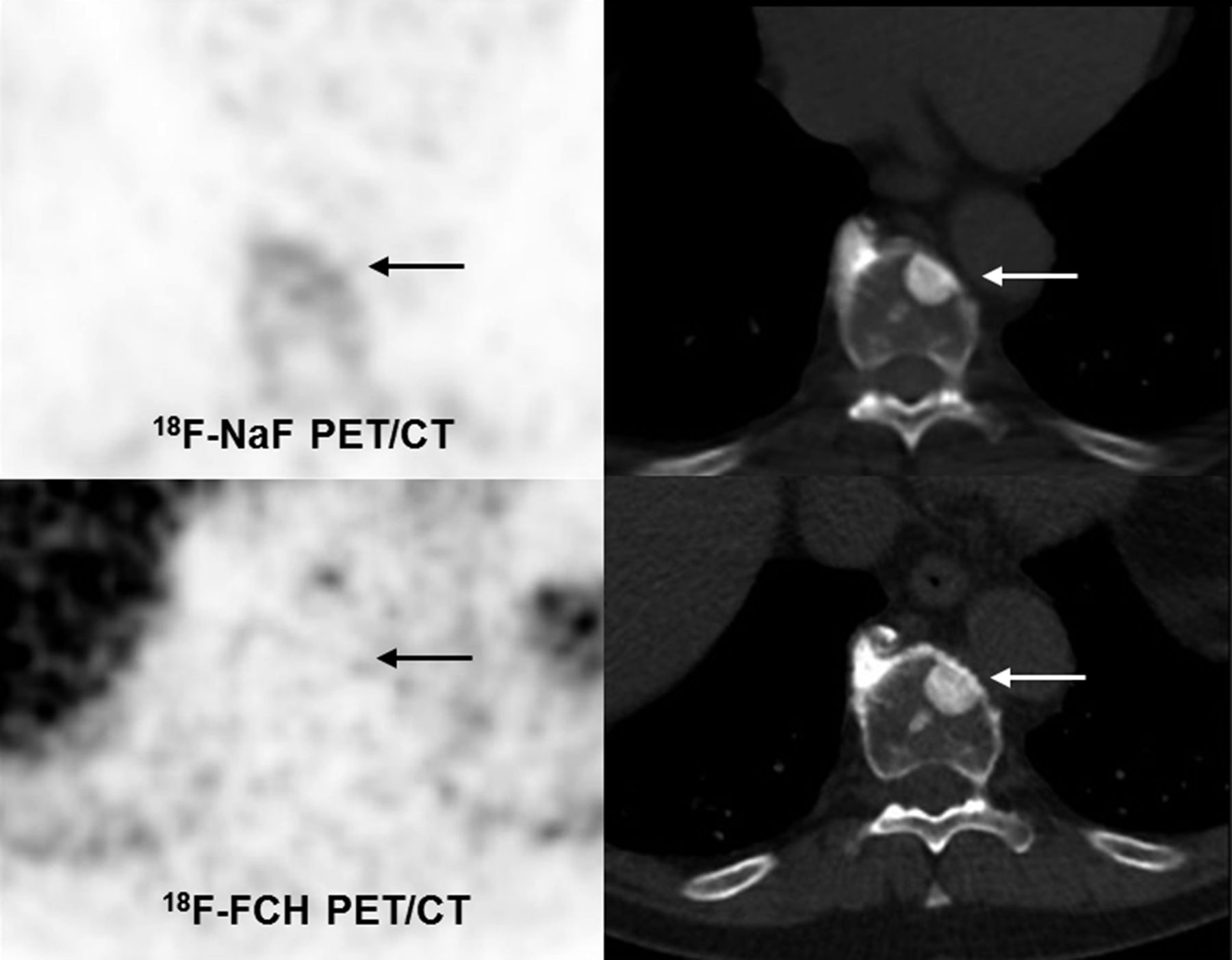
Comparison of 18F-fluorocholine (FCH) and 18F-NaF images in high-risk prostate cancer patient after hormone therapy. 18F-NaF PET image shows significantly increased tracer uptake on thoracic spine (upper row left, arrow) corresponding to highly suspicious, densely sclerotic lesion on CT (upper and lower rows right, arrow). 18F-fluorocholine shows only faint uptake on sclerotic lesion (lower row left, arrow).

Comparison of 18F-fluorocholine (FCH) and 18F-NaF PET/CT images in prostate cancer patient (prostate-specific antigen level, 7.3 ng/mL; Gleason score, 7). 18F-NaF PET scan shows increased tracer uptake on thoracic spine (upper row left, arrow) corresponding to suspicious sclerotic lesion on CT (upper and lower rows right, arrows). 18F-fluorocholine image shows only faint uptake on rim of sclerotic lesion (lower row left, arrow).
More investigations are warranted to define whether such 18F-fluorocholine–negative lesions are truly nonviable bone metastases or whether the phenomenon is caused by the limited sensitivity of 18F-fluorocholine PET/CT when detecting densely sclerotic lesions secondary to diminished malignant cells or reduced perfusion. Until then, we suggest further evaluation with 18F-NaF PET/CT in patients with non–18F-fluorocholine-avid suggestive sclerotic bone lesions in this group of patients (45). However, with respect to therapy response, 18F-NaF PET/CT may also be negative in highly dense sclerotic lesions (Fig. 5).
18F-NaF PET/CT and 18F-fluorocholine (FCH) PET/CT images in intermediate-risk prostate cancer patient after radiation therapy on vertebral spine (T10). Negative 18F-NaF and 18F-fluorocholine PET images (upper and lower rows left, arrow) correspond to sclerotic lesion on CT (upper and lower rows right, arrow) and are suggestive of nonviable bone metastasis after radiotherapy.
Wondergem et al. (49) reviewed 13 articles and calculated lesion-based sensitivity and specificity of approximately 84% and 98%, respectively, for 18F-fluorocholine PET/CT and approximately 89% and 91%, respectively, for 18F-NaF PET/CT. Also, a patient-based sensitivity and specificity of approximately 85% and 97%, respectively, for 18F-fluorocholine PET/CT and approximately 87% and 80%, respectively, for 18F-NaF PET/CT were calculated. But overall, no significant difference was seen between the sensitivity and specificity of 18F-fluorocholine and 18F-NaF PET/CT in detecting metastatic bone disease. Those authors also recommended that these 2 modalities should be considered an alternative to conventional whole-body bone scintigraphy (49).
CONCLUSION
Because of the promising role of PET/CT and its advantages in the evaluation of osseous metastatic disease from prostate cancer, it will most likely replace conventional whole-body bone scintigraphy in the near future. However, no significant difference has been detected in sensitivity and specificity between 18F-NaF and 18F-fluorocholine PET/CT in the assessment of bone metastases. 18F-fluorocholine PET/CT seems to be the superior modality for detecting bone marrow metastases, although the interpretation of 18F-fluorocholine–negative, 18F-NaF–positive densely sclerotic lesions is problematic. More investigations may be warranted to determine whether such lesions are truly nonviable bone metastases after treatment and also to determine whether the phenomenon is caused by the limited sensitivity of 18F-fluorocholine PET/CT for detecting metastatic bony lesions with high density secondary to fewer malignant cells or reduced perfusion.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 14, 2016.
- Accepted for publication May 1, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}