


Abstract
The aim of this review is to report on the value of 11C-choline PET imaging as a diagnostic procedure for metastasis-directed therapies. Furthermore, the role of 11C-choline PET/CT as a diagnostic tool for monitoring castration-resistant prostate cancer patients treated with systematic therapy is assessed. Finally, the role of 11C-choline PET/CT in the prediction of survival in both castration-resistant prostate cancer patients and hormone-naïve patients is investigated.
- 11C-choline PET/CT
- salvage radiotherapy
- salvage lymph node dissection
- PET-guided therapies
- metastasis-directed therapies
Prostate cancer (PCa) is the most common solid neoplasm in men (1,2). Although primary treatment of clinically localized PCa is associated with excellent oncologic results, up to 50% of patients treated with radical prostatectomy (RP) or external-beam radiotherapy experience biochemical recurrence (BCR) during follow-up (3–7). Several tools for evaluating clinical and pathologic parameters, such as prostate-specific antigen (PSA) level, PSA doubling time, PSA velocity, pathologic Gleason score, pathologic stage, and lymph node invasion, are available for assessment of the probability that a patient harbors local versus systemic recurrence after RP or external-beam radiotherapy (8–10). With these parameters, differentiation of the site of recurrence is not possible; they may allow for only an estimation of the probability of local or distant disease. As a consequence, clinicians are currently not able to target individualized salvage therapies in accordance with the information provided by these tools only. Therefore, patients are generally referred for salvage radiotherapy (S-RT) to the prostate bed when local relapse is suspected and for systemic androgen deprivation therapy (ADT) when systemic relapse is suspected (2).
Metastasis-directed therapies might play a role in the management of patients with suspected relapse (11,12) if an imaging modality that could accurately identify the number and site(s) of metastases were available. 11C-choline PET/CT has been proven to be a better diagnostic tool for restaging in patients with PCa after BCR than conventional imaging (10,13). Choline may be labeled with 18F or 11C. The first has a half-life of 110 min, whereas the second has a half-life of 20 min and can be used only in centers with an on-site cyclotron. The main difference in physiologic biodistribution between 18F-choline and 11C-choline is that the former is excreted by the kidneys and the latter is not.
If 11C-choline PET/CT were capable of differentiating limited, potentially curable disease from metastatic disease, it could have an important role if metastasis-directed therapies could be performed in accordance with the PET results (14). Several studies (11,12) on the role of 11C-choline PET/CT in metastasis-directed therapies—such as S-RT or salvage pelvic lymph node dissection (S-PLND), performed in accordance with the 11C-choline PET/CT results—have been published; these studies had promising results in terms of BCR-free survival and ADT-free survival. Furthermore, in daily practice, 11C-choline PET/CT had a valuable clinical impact on patient management. In 3 different patient series, 11C-choline PET/CT led to a change in the decision-making process in approximately 50% of cases (15–17). Moreover, 11C-choline PET/CT was recently proposed as a diagnostic tool for monitoring castration-resistant PCa (CRPC) patients treated with chemotherapy (18) and new ADT (19,20). The main drawback of 11C-choline PET/CT is the relatively low sensitivity in patients with low PSA levels at the time of imaging (13,21,22). In these patients, promising results have been obtained with novel agents such as 68Ga-labeled prostate-specific membrane antigen analogs (23,24).
The aim of this review is to report on the value of 11C-choline PET imaging as a diagnostic procedure for metastasis-directed therapies. Furthermore, the role of 11C-choline PET/CT as a diagnostic tool for monitoring CRPC patients treated with systematic therapy is assessed. Finally, the role of 11C-choline PET/CT as a predictor of survival in both CRPC patients and hormone-naïve patients is investigated.
USE OF CHOLINE PET/CT TO GUIDE METASTASIS-DIRECTED S-RT
The efficacy of S-RT for treating recurrent PCa in patients with BCR and suspected local relapse has already been established in the literature (14,25,26). The optimal timing (to obtain the best chance of cure) for S-RT would be when the tumor burden is low, that is, when PSA first reaches a detectable level during BCR (14,25,26). Disease-free survival rates at 6 y after S-RT were reported to be 40% in patients with PSA levels of less than 0.5 ng/mL before treatment and 18% in patients with PSA levels of greater than 1.5 ng/mL (14). Nonetheless, most patients treated with S-RT will experience disease progression after treatment (14,25,26). For this reason, efforts to exclude the presence of metastases not included in the planned target volume should be made.
Recently, Castellucci et al. (27) used 11C-choline PET/CT to investigate a cohort of 605 recurrent PC patients (PSA range, 0.2–2 ng/mL) who were scheduled to receive S-RT in the prostatic bed. With an overall rate of detection of 28.7%, 11C-choline PET/CT detected disease limited to the pelvis in 13.7% of patients and extrapelvic disease in 14.7% of patients. PSA, PSA kinetics, and ongoing ADT were predictors of positive scan results. 11C-choline PET/CT performance increased in patients with a PSA doubling time of less than 6 mo (47%) and in patients receiving ongoing ADT (46%). As a consequence, the authors proposed the use of 11C-choline PET/CT in patients suitable for receiving S-RT, particularly patients with fast PSA kinetics or increasing PSA levels despite ongoing ADT, given the high probability of the detection of positive findings outside the pelvis. 11C-choline PET/CT might lead to better stratification of patients suitable for receiving S-RT, leading to the exclusion of patients because of the presence of distant metastases or to the performance of S-RT in an extended planned target volume because of the presence of positive locoregional lymph nodes.
Souvatzoglou et al. (28) investigated a cohort of 37 patients who had BCR after RP and were referred for S-RT to the prostatic bed in accordance with their risk factors. In 13% of the patients, 11C-choline PET/CT revealed positive iliac lymph nodes. In this patient population, the planned target volume was significantly changed in accordance with the 11C-choline PET/CT findings; S-RT was performed in an extended planned target volume including 11C-choline PET/CT–positive lymph nodes. In the overall population, the disease-free survival rate was 56%, whereas in patients treated with metastasis-directed S-RT, the disease-free survival rate was 80%. Similar results were reported by Würschmidt et al. (29) for recurrent PCa in 19 patients treated with intensity-modulated radiotherapy for BCR after RP. A standard dose was delivered to the prostatic bed with a boost (65 Gy) for 18F-choline PET/CT–positive lymph nodes. After 28 mo of follow-up, they reported an overall survival rate of 94%, a BCR-free survival rate of 49%, and a distant disease–free survival rate of 75%. The authors concluded that 18F-choline PET/CT could be helpful in dose escalation for PCa, allowing a boost of the dose to metastatic lymph node regions when metastasis-directed S-RT is used. The main limitation of those 2 works (28,29) is the limited number of patients enrolled.
Picchio et al. (30) investigated the use of 11C-choline PET/CT for planning and monitoring helical tomotherapy in 83 patients with recurrent PCa, with a simultaneous integrated boost only in patients with PET-positive lymph nodes. Despite the short follow-up proposed (mean, 83 d; range, 16–365 days), the authors observed an early biochemical partial response in 70% of cases. Incerti et al. (31) recently studied a cohort of 68 patients who had BCR after radical therapy and were treated with helical tomotherapy in accordance with the pathologic 11C-choline lymph node uptake. The 24-mo overall survival, locoregional relapse–free survival, clinical relapse–free survival, and BCR-free survival rates were 87%, 91%, 51%, and 40%, respectively.
Whether metastasis-directed therapy performed in accordance with 11C-choline PET/CT results could delay the administration of ADT has not yet been determined. ADT is the treatment of choice for BCR, and it is also administrated as an adjuvant treatment after S-RT. Nevertheless, ADT causes incontrovertible side effects. Furthermore, patients with hormonal blockade sooner or later will progress to a CRPC condition (32). Recently, Berkovic et al. (33) investigated whether repeated stereotactic body radiotherapy of oligometastatic disease could defer the initiation of ADT in patients with low-volume metastases. They enrolled 24 PCa patients who had BCR after radical therapy and 1–3 synchronous metastases (bone or lymph node) assessed by 18F-choline PET/CT. Patients were treated with repeated stereotactic body radiotherapy, and the ADT-free survival was defined as the time interval between the first day of stereotactic body radiotherapy and the initiation of ADT. The authors concluded that repeated salvage stereotactic body radiotherapy was feasible, was well tolerated, and deferred palliative ADT for a median of 38 mo in patients with limited bone or lymph node PCa metastases (Figs. 1 and 2).
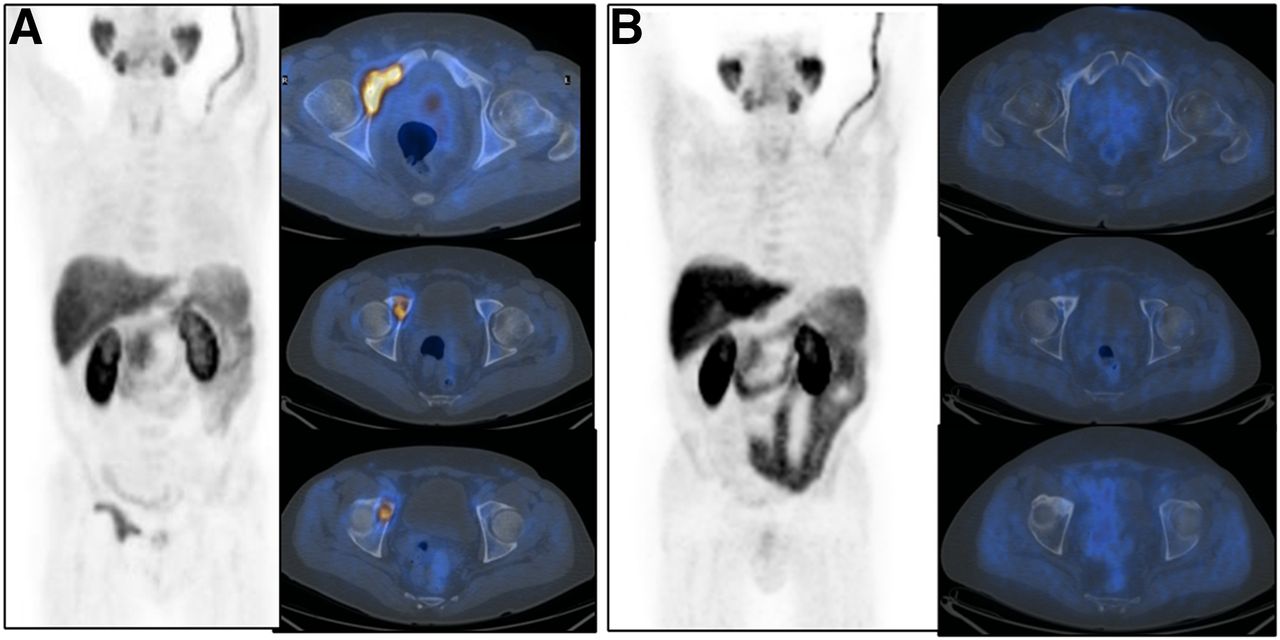
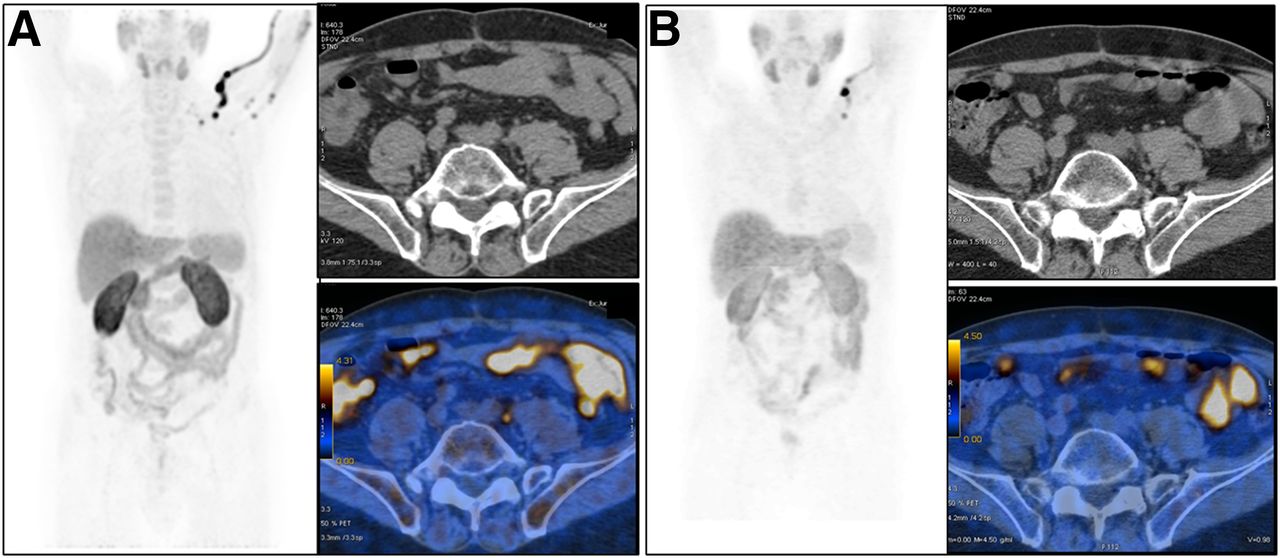
66-y-old patient with Gleason score of 4 + 4 and pT3aN0(0/12)Mx cancer. Initial PSA was 8 ng/mL. Patient was treated with RP. BCR (PSA, 0.4 ng/mL; PSA doubling time, 6 mo) occurred 12 mo after RP. (A) 11C-choline PET/CT (maximum-intensity-projection [MIP], CT, and fused images) showed single left common iliac lymph node (SUVmax, 4; diameter, 8 mm). Metastasis-directed S-RT was subsequently performed; PSA nadir was 0.08 ng/mL. (B) 11C-choline PET/CT performed 3 mo after S-RT (MIP, CT, and fused images) showed complete metabolic response.
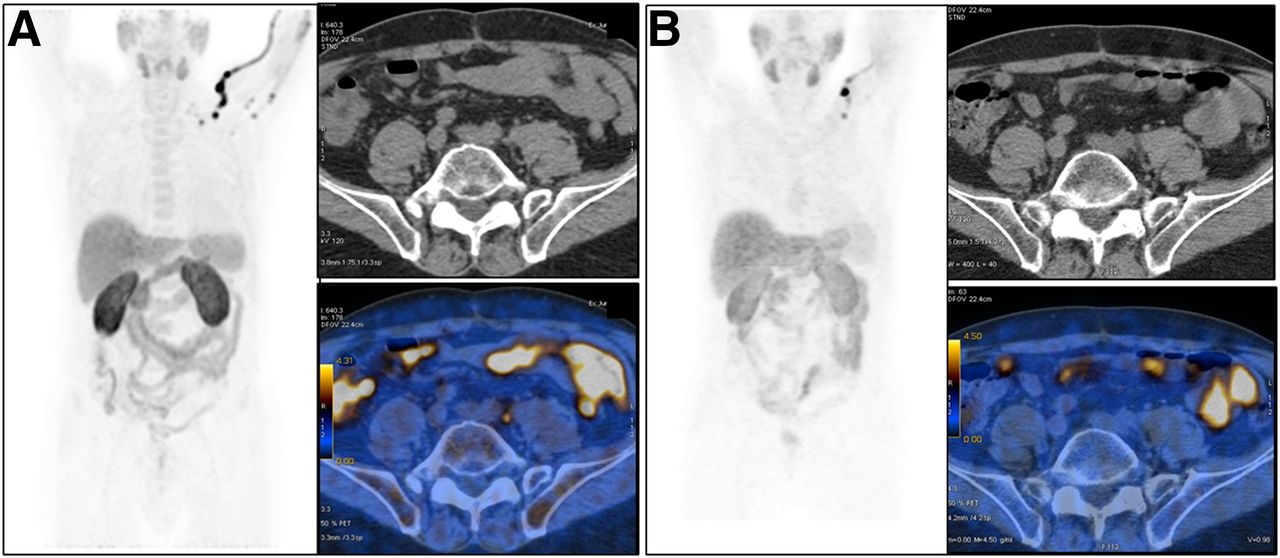
70-y-old patient with Gleason score of 4 + 4 and pT3aN1(2/15)Mx cancer. Initial PSA was 21 ng/mL. Patient was treated with RP. BCR (PSA, 11 ng/mL; PSA doubling time, 4.1 mo) occurred 10 mo after external-beam radiotherapy (EBRT). (A) 11C-choline PET/CT (maximum-intensity-projection [MIP] and fused images) showed single osteoblastic lesion involving right ilium and pubis bones (SUVmax, 10). (B) Patient was referred for metastasis-directed EBRT; PSA response (PSA, 0.4 ng/mL) after treatment was confirmed by 11C-choline PET/CT performed 3 mo after EBRT (MIP and fused images).
In conclusion,11C-choline PET/CT is a valuable tool for selecting patients suitable for image-guided S-RT, particularly in the early phase of BCR. However,11C-choline PET/CT still has low sensitivity, and in some cases, small, undetectable lesions could be left out of the field of irradiation. As a consequence, some authors have suggested irradiation of areas that have 11C-choline PET/CT–positive findings with a boost in addition to a standard dose to the closest lymphatic chains.
USE OF CHOLINE PET/CT TO GUIDE METASTASIS-DIRECTED SALVAGE LYMPH NODE DISSECTION
Patients experiencing lymph node relapse after RP are considered to be affected by systemic disease; consequently, palliative therapies are generally the treatment of choice. However, patients with lymph node relapse showed more favorable outcomes than patients with bone or visceral metastases after radical treatment (34). On the basis of these data, PET metastasis–directed therapies, such as S-PLND, have been proposed for patients with lymph node relapse.
In that scenario, as recently reported by Kitajima et al. (35), 11C-choline PET/CT performance was better than that of MRI in pelvic lymph node metastasis detection, regardless of PSA levels (MRI: sensitivity, 64%; specificity, 85%; accuracy, 70%; 11C-choline PET: sensitivity, 90%; specificity, 100%; accuracy, 92.9%). Rinnab et al. (36) reported on the usefulness of 11C-choline PET/CT for metastasis-directed pelvic/retroperitoneal lymph node dissection in a cohort of 15 patients who had BCR treated with open S-PLND. The authors reported a positive predictive value for 11C-choline PET/CT of 53% and good compliance with the treatment. The efficacy of 11C-choline PET/CT–guided S-PLND was further investigated by Rigatti et al. (37). They reported a biochemical response after S-PLND in 57% of patients (41/72), with BCR-free survival rates at 3 and 5 y of 27.5% and 10.3%, respectively. The main predictive factors were a PSA level of less than 4 ng/mL at the time of 11C-choline PET/CT, a time to biochemical relapse of less than 24 mo, and negative lymph nodes at the time of RP. The 5-y clinical recurrence-free survival rate was lower for patients with retroperitoneal nodal uptake than for patients with only positive pelvic lymph nodes (11% vs. 53%). Updated results for that series were recently published (11); clinical recurrence– and cancer-specific mortality–free survival rates of 38% and 81%, respectively, after 8 y of follow-up were reported. The PSA level at the time of 11C-choline PET/CT, a biochemical response, and PET-positive retroperitoneal lymph nodes were predictors of an earlier clinical relapse.
Tilki et al. (38) studied 56 PCa patients who had BCR after RP. After 18F-choline PET/CT, all patients underwent bilateral pelvic or retroperitoneal lymphadenectomy (1,149 lymph nodes removed). 18F-choline PET/CT findings were compared with histologic results. A per-patient analysis yielded a specificity of 85.7% for 18F-choline PET/CT. However, in a lesion-based analysis, 18F-choline PET/CT sensitivity, specificity, positive predictive value, and negative predictive value were 39.7%, 95.8%, 75.7%, and 83.0%, respectively. A site-based analysis yielded a sensitivity, specificity, positive predictive value, and negative predictive value of 68.4%, 73.3%, 81.3%, and 57.9%, respectively. The authors concluded that positive 18F-choline PET/CT findings correctly predicted the presence of lymph node metastases in most patients but did not allow for a precise localization of all metastatic lymph nodes.
Passoni et al. (39) confirmed the data of Tilki et al. (38). They studied 46 patients who had BCR after RP and a single PET-positive lymph node. All patients underwent pelvic or retroperitoneal lymph node dissection. Overall, 30 patients (65%) had positive lymph nodes at pathologic examination. 11C-choline PET/CT results were confirmed in 16 patients (35%) who had pathologically confirmed metastases in the same lymphatic region as seen on 11C-choline PET/CT. The overall positive predictive values of 11C-choline PET/CT were 34.8% and 23.9% when exact concordance was defined on the basis of the lymphatic drainage site and the single positive lymph node, respectively.
Karnes et al. (40) obtained encouraging results for 52 patients treated with S-PLND. After a median follow-up of 20 mo, 57.7% of the patients (30/52) had a PSA level of less than 0.2 ng/mL, 75% (39/52) were free of systemic progression, and 96.2% were alive.
Despite some criticism in the past, S-PLND in patients with few lymph nodes positive on 11C-choline PET/CT is now considered the treatment of choice (41). However, this approach should be reserved for a population with good performance status, long life expectancy, and limited disease (preferably in the pelvis). With these criteria, good results were obtained in a long-term follow-up study (39). The benefits of S-PLND are prolonged overall survival and delayed administration of ADT. Clinicians should consider the risk of overtreatment and the fact that this approach is not curative for the patient. Finally, given the lack of a control group, the benefits for patients of PET-based treatment versus non–PET-based S-PLND cannot be assessed.
USE OF CHOLINE PET/CT TO ASSESS RESPONSE TO SYSTEMIC THERAPIES
Patients with PCa may develop resistance to ADT during BCR, and consequently, the hormonal blockade loses its protective effect on tumor cell growth (32). The condition of CRPC, particularly in the presence of proven metastatic spread (mCRPC), is associated with a median overall survival of 2–3 y (42). At this stage, palliation is the main target of any treatment. Many palliative therapies, including systemic chemotherapy (e.g., docetaxel and cabazitaxel) and recently developed antiandrogenic therapies (e.g., abiraterone and enzalutamide), are available (43,44). A consensus about the optimal timing and type of treatments has not been reached yet. The main drawback is the lack of accuracy of biochemical markers (including PSA and PSA kinetics) for predicting the response to therapy in mCRPC (2,45). In this scenario, a diagnostic procedure capable of evaluating tumor burden before therapy (i.e., evaluating the presence and the site or sites of visceral or bone metastases) could provide key information for choosing the most appropriate treatment strategy.
Another limitation for clinicians is the lack of reliable factors predicting the response to therapy (45). The most common treatment strategy proposed for mCRPC patients is docetaxel as the first line of chemotherapy (42). Recently, Ceci et al. (18) investigated the role of 11C-choline PET/CT for evaluating the response to docetaxel in a cohort of 61 mCRPC patients. The authors compared the radiologic response evaluated with 11C-choline PET/CT with the PSA response. The progression of disease was defined as the appearance of a new PET-positive lesion, whereas the PSA response was defined as a decrease in the PSA level of greater than or equal to 50% after chemotherapy. The radiologic progression of disease was observed in 44% of patients with a PSA response. Furthermore, a higher tumor burden (expressed as >10 PET-positive bone lesions before docetaxel treatment) was significantly associated with an increased probability of the progression of disease.
In recent years, patients who developed CRPC were offered a new generation of ADT (such as abiraterone and enzalutamide), with good results in terms of biochemical response and pharmacologic effects (43,44). De Giorgi et al. (19,46) assessed the usefulness of 18F-choline PET/CT for evaluating the early response to treatment with abiraterone and enzalutamide in mCRPC patients. The authors concluded that a radiologic response, as assessed with 18F-choline PET/CT, was associated with more favorable overall survival than a PSA response of greater than or equal to 50% alone. Maines et al. (20) evaluated the role of 18F-choline PET/CT in monitoring the response to enzalutamide in 30 mCRPC patients. The authors observed that SUVmax measured by PET before enzalutamide treatment was significantly related to BCR-free survival, radiologic progression–free survival, and overall survival. However, only a few data about this topic have been published. In addition, there is still no consensus regarding the criteria that should be used to evaluate the response to treatment with 18F-choline PET/CT, because both EORTC and RECIST 1.1 have many limitations when applied to patients with mCRPC (Figs. 3 and 4).
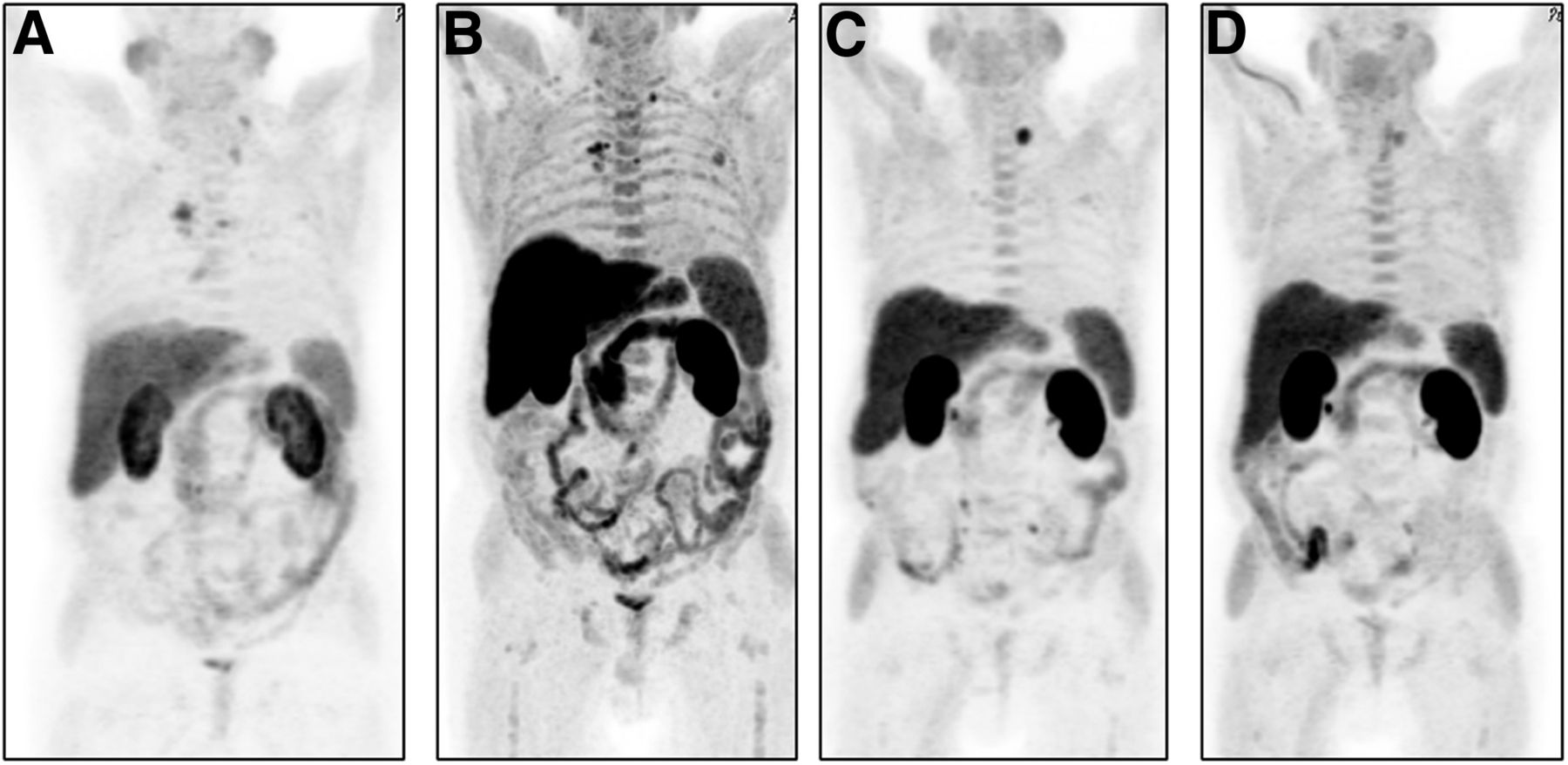
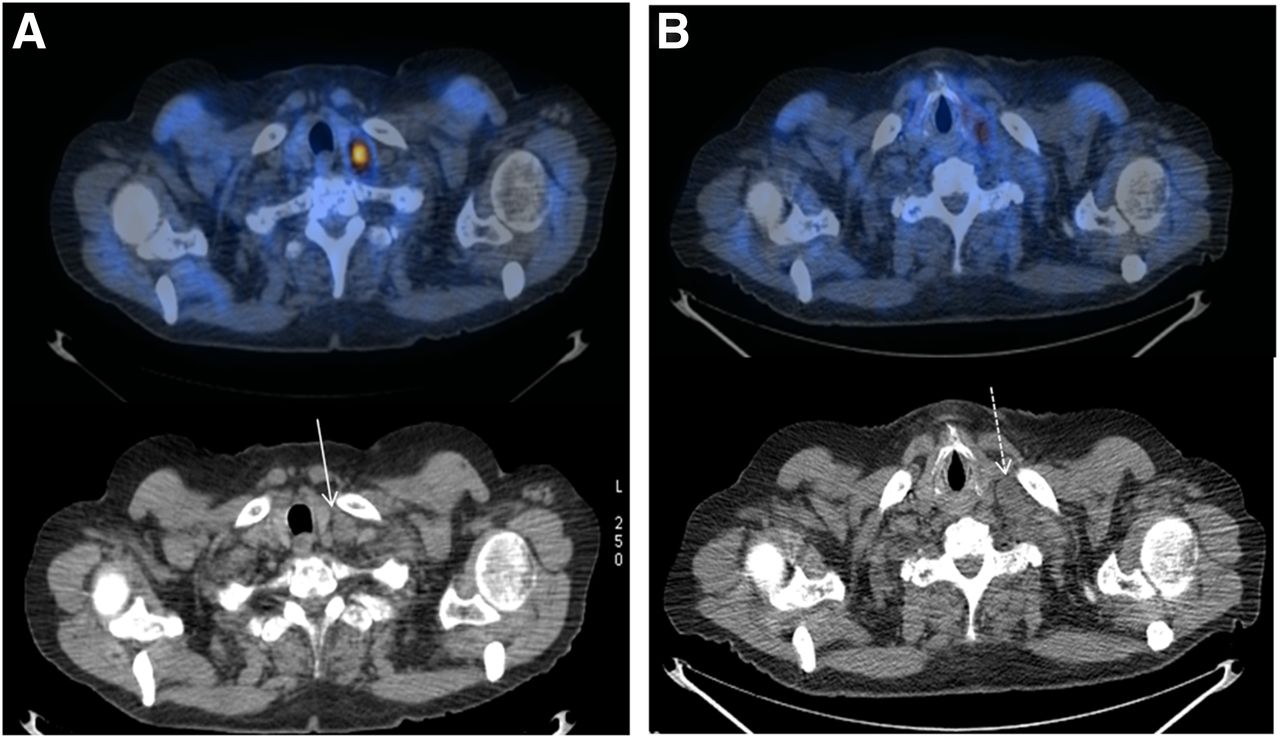
62-y-old patient with Gleason score of 4 + 4 and pT3b N1(8/24)Mx cancer. Initial PSA was 18 ng/mL. Patient was treated with RP. BCR occurred 8 mo after RP, and ADT was administered. After 26 mo, patient developed CRPC (PSA, 14 ng/mL; PSA doubling time, 3.2 mo). (A) 11C-choline PET/CT (maximum-intensity-projection [MIP] images) showed positive lymph nodes in paratracheal region and left supraclavicular lymph node, and docetaxel was administered. (B) Subsequent 11C-choline PET/CT (MIP images) showed progression of disease (in mediastinal lymph nodes and third left rib) despite PSA response (PSA, 10 ng/mL). Patient was given abiraterone; PSA response occurred after 6 mo (PSA, 4 ng/mL). (C) 11C-choline PET/CT (MIP images) showed response of mediastinal lymph nodes and rib but increased uptake in supraclavicular lymph node. (D) Patient was given metastasis-directed external-beam radiotherapy; PSA response (PSA, 1 ng/mL) and partial response on 11C-choline PET/CT (MIP images) occurred.
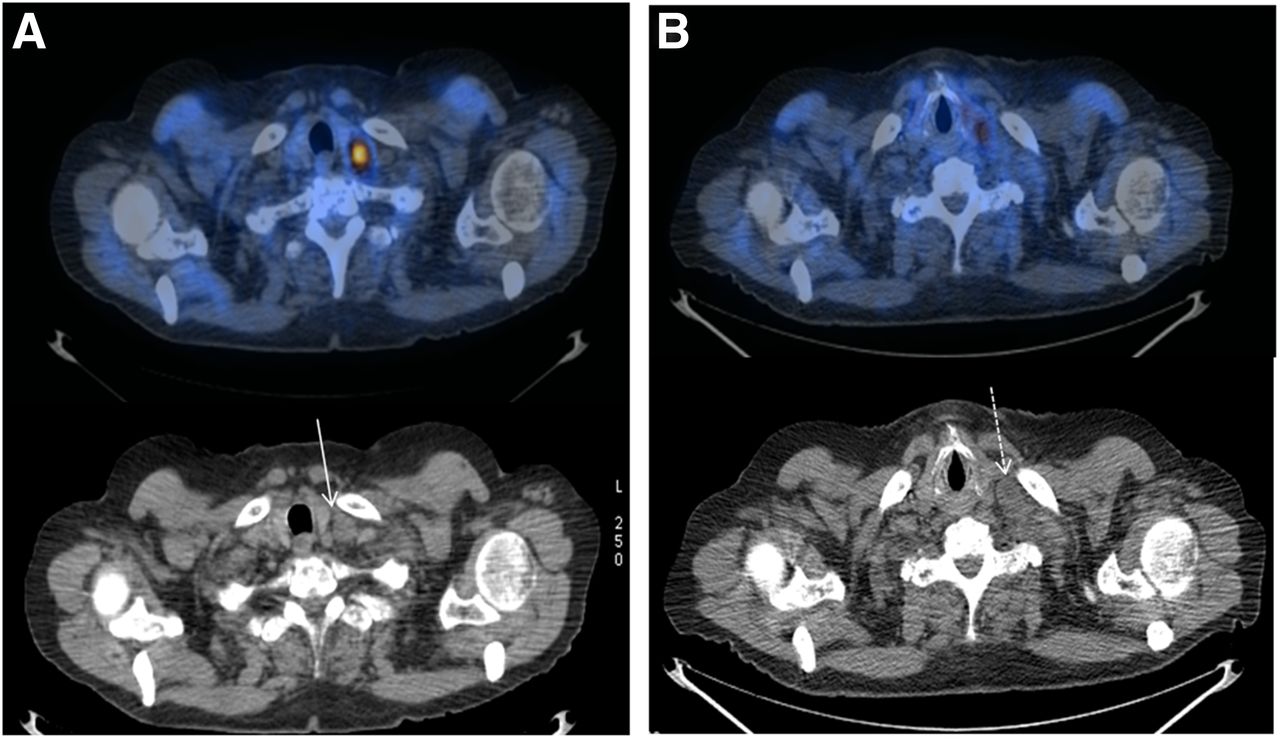
Additional images of same patient as in Figure 3. (A) Fused images of left supraclavicular lymph node before metastasis-directed external-beam radiotherapy (EBRT). (B) Fused images of left supraclavicular lymph node after metastasis-directed EBRT. 11C-choline uptake decreased after EBRT, but necrotic component of node enlarged after EBRT (arrows).
PROGNOSTIC VALUE OF CHOLINE PET/CT
The use of 11C-choline PET/CT as a prognostic factor in patients experiencing BCR was recently explored by Giovacchini et al. with 2 large cohorts of patients (47,48). In the first study (47), 195 PCa patients with BCR after RP were retrospectively enrolled to evaluate whether 11C-choline PET/CT performed during ADT could predict PCa-specific survival. The median follow-up after 11C-choline PET/CT was 4.5 y, whereas the 11C-choline PET/CT detection rate was 57%. The median PCa-specific survival was statistically significantly different: 16.4 y in patients with negative 11C-choline PET/CT results and 11.2 y in patients with positive 11C-choline PET/CT results. In the second study (48), 302 hormone-naïve PCa patients with BCR after RP were evaluated. The median follow-up after 11C-choline PET/CT was 7.2 y, whereas the 11C-choline PET/CT detection rate was 33%. The 15-y PCa-specific survival probability was statistically significantly different: 42.4% in patients with positive 11C-choline PET/CT results and 95.5% in patients with negative 11C-choline PET/CT results. Given these findings, it seems that positive 11C-choline PET/CT results could predict PCa-specific survival if performed during BCR in either hormone-naïve patients or patients treated with ADT. These data indicate why 11C-choline PET/CT should be more widely used in the follow-up of PCa patients receiving metastasis-directed therapies.
Kwee et al. (49) investigated the prognostic significance of the metabolically active tumor volume measured with 18F-fluorocholine PET/CT in 30 CRPC patients. Statistical analysis demonstrated significant differences in survival between groups stratified by median net metabolically active tumor volume.
The lack of predictive factors is one of the main limitations for clinicians in choosing the proper systemic therapies (8). Few attempts have been made to assess whether 11C-choline PET/CT could be a reliable method for predicting the response to treatment. It seems from the studies described here that at least for CRPC, measurement of the extent of disease before treatment with 11C-choline PET/CT could be a reliable way to predict the response to treatment.
CONCLUSION
Despite some limitations due to the suboptimal sensitivity of 11C-choline PET/CT in patients with BCR and low PSA levels, the use of this imaging procedure to guide metastasis-directed therapies (S-RT and S-PLND) in patients with oligometastatic recurrent PCa is increasing. 11C-choline PET/CT could lead to better patient stratification, allowing the selection of patients with a low tumor burden and tailored therapy instead of palliative treatment, with benefits in terms of BCR-free survival and ADT-free survival. Furthermore, 11C-choline PET/CT should be suggested for monitoring patients treated with systemic therapies (chemotherapy and ADT) to assess the eventual radiologic progression of disease, given that the radiologic response assessed with 11C-choline PET/CT was associated with a more favorable outcome. Finally,11C-choline PET/CT should be more widely used for restaging PCa, given that positive 11C-choline PET/CT results could predict PCa-specific survival in either hormone-naïve or CRPC patients.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 2, 2016.
- Accepted for publication July 5, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}