


Abstract
The purpose of this study was to develop a noninvasive imaging test of pancreatic exocrine function. Methods: In this pilot study, 5 healthy volunteers underwent two 60-min dynamic 11C-acetate PET studies, one before and one after intravenous secretin administration. Kinetic analysis of the pancreas was performed using a 1-compartment model and an image-derived input function. From summed images, standardized uptake values were measured from the pancreas and the liver, and the pancreas-to-liver ratio was computed. Results: The baseline k1 and k2 data for all 5 volunteers were consistent. After secretin stimulation, the k1 and k2 significantly increased (paired t test P = 0.046 and P = 0.023, respectively). In the summed PET images, the pancreas-to-liver ratio decreased (P = 0.037). Increased 11C-acetate activity was observed in the duodenum after secretin stimulation consistent with secretin-induced secretion. Conclusion: 11C-acetate PET studies with secretin stimulation show potential as a noninvasive method for assessing pancreatic exocrine function.
Chronic pancreatitis has a high prevalence in developed countries, 25–30 cases per 100,000 people, and an even higher prevalence of approximately 5% in autopsy studies (1,2). The transition from acute pancreatitis, which is the second most common gastrointestinal discharge diagnosis in the United States, to chronic pancreatitis is challenging to identify. Accurate diagnosis of early chronic pancreatitis is difficult with imaging studies such as CT, MR imaging, endoscopic retrograde cholangiopancreatography, or endoscopic ultrasound. Pancreatic volume loss is evident only in the late stages, taking 5–10 y or longer to develop (3). Although imaging and function tests at the early stages of the disease are often negative, early recognition is important to help with accurate diagnosis, reduce disease progression, and prevent unnecessary interventions (4).
A pancreas function test is the most sensitive test described but is not readily performed at most centers (5). The pancreas function test involves passing a tube into the duodenum, injecting a supraphysiologic dose of secretin, and then collecting the pancreatic secretions over an hour to measure the bicarbonate concentration. Secretin is a hormone that stimulates the pancreatic ductal cells to excrete fluid and bicarbonate, and normally, the bicarbonate concentration will double after secretin stimulation in 15 min (6). The pancreas function test is uncomfortable for the patient, expensive, and time-consuming. A shorter-duration endoscopic collection of the pancreatic secretions is an alternative but is less sensitive (7). These current pancreatic function tests are so cumbersome and insensitive that they are essentially obsolete and not being used by most practitioners.
11C-acetate PET was developed first to study oxygen metabolism in the myocardium and is currently applied in oncology for prostate cancer, hepatocellular carcinoma, and brain tumors (8). Intense 11C-acetate uptake is consistently noted in the pancreas, plainly demarcating the organ, and 11C-acetate PET has been used to discriminate between malignant and benign pancreatic diseases (9).
The purpose of this pilot study was to develop a noninvasive and sensitive pancreas function test. Such a test could aid in the diagnosis of early pancreatic dysfunction resulting from chronic pancreatitis. We evaluated 11C-acetate PET in the basal and secretin-stimulated state to determine whether it had potential for this application.
MATERIALS AND METHODS
Five volunteers with no known diseases of the pancreas were studied. The study was approved by the institutional review board at Johns Hopkins University, and all volunteers provided written informed consent. During the volunteers’ first visit, blood was drawn to assess the levels of liver enzymes, pancreatic enzymes, and basic electrolytes. The laboratory values had to be within reference limits.
During the volunteers’ second visit, dynamic 11C-acetate PET studies were performed twice—before and after administration of secretin. All PET data were acquired on a Discovery RX VCT PET/CT system (GE Healthcare) using identical techniques. After a low-dose CT scan for organ localization, 11C-acetate was given intravenously (10 MBq/kg of body weight), and dynamic emission PET was immediately performed over 60 min (6 × 10 s, 6 × 20 s, 6 × 30 s, 6 × 60 s, 11 × 180 s, 3 × 300 s). PET data were acquired in 3-dimensional mode and reconstructed using ordered-subsets expectation maximization (2 iterations, 21 subsets, gaussian filter of 3 mm in full width at half maximum), incorporating corrections for randoms, dead time, scatter, attenuation, and detector normalization. Approximately 120 min after injection of 11C-acetate for the first scan, recombinant human secretin (targeted dose, 0.4 μg/kg) was injected intravenously over 1 min. Approximately 10 min after the secretin injection, the volunteers received a second injection of 11C-acetate and a postsecretin dynamic PET scan was performed.
Kinetic analysis was performed using a 1-compartment model with a blood volume term and an image-derived input function. The pancreas was manually outlined on the baseline scan, and the same volume of interest was manually repositioned for the follow-up study. An image-derived input function was estimated from the aorta using a series of 6-mm-diameter circular regions of interest manually positioned in all but the end slices. Kinetic analysis was restricted to the first 10 min to minimize contamination of the input function at later times due to spill-in from surrounding organs. The uptake rate, k1, and the washout rate, k2, were computed using PMOD software (PMOD Technologies Ltd.).
Standardized uptake values in a 1-cm3 spheric volume of interest, corrected for lean body mass (SULpeak), were measured in the pancreas and liver from the 0- to 60-min summed PET images. The pancreas-to-liver SULpeak ratio was also computed. The SULpeak was measured using XD3 software (Mirada Medical).
RESULTS
The 5 healthy subjects ranged in age from 27 to 34 y (2 men, 3 women), and no abnormality was seen in their baseline metabolic profiles.
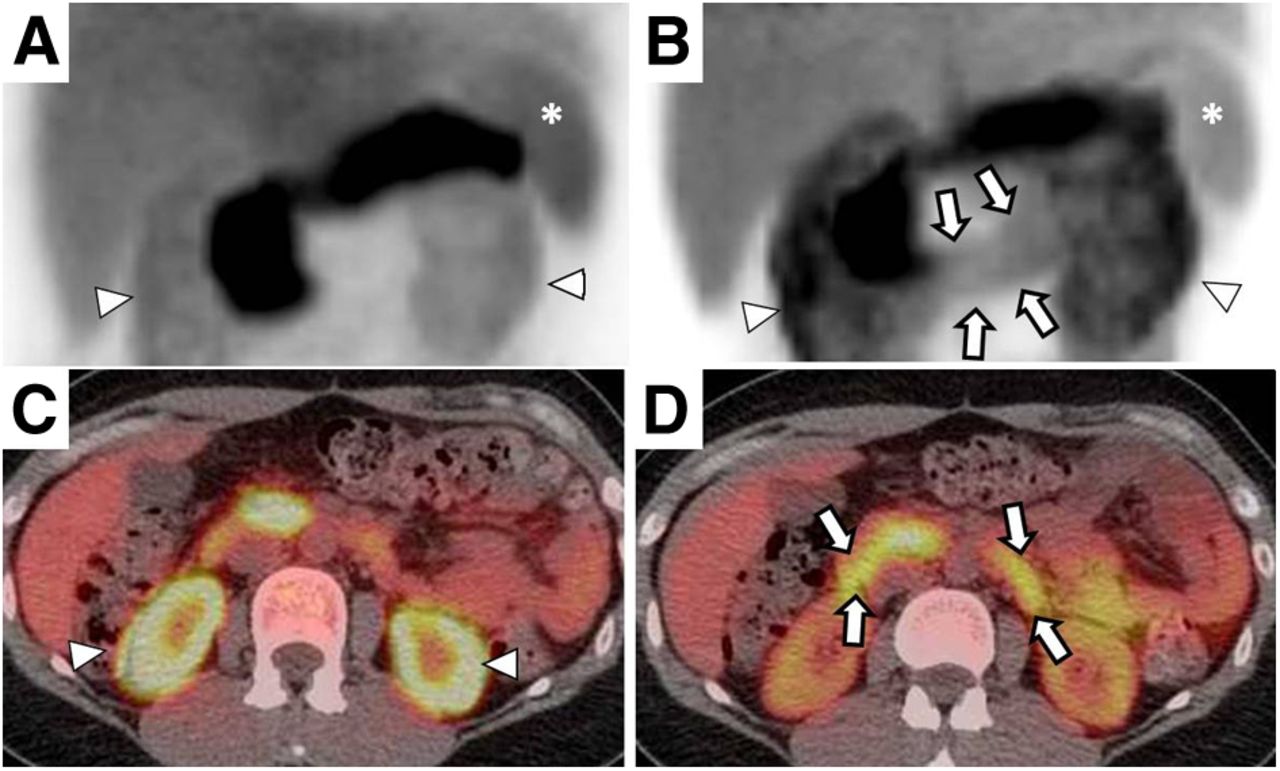
On visual assessment, intense radiotracer uptake was noted in the pancreas in all 5 subjects both at baseline and after secretin stimulation. The summed PET images obtained after secretin stress had an additional shared feature: diffuse duodenal uptake became noticeable in each case after the secretin stress (Fig. 1). Time–activity curves for the pancreas and duodenum are shown in Figure 2.
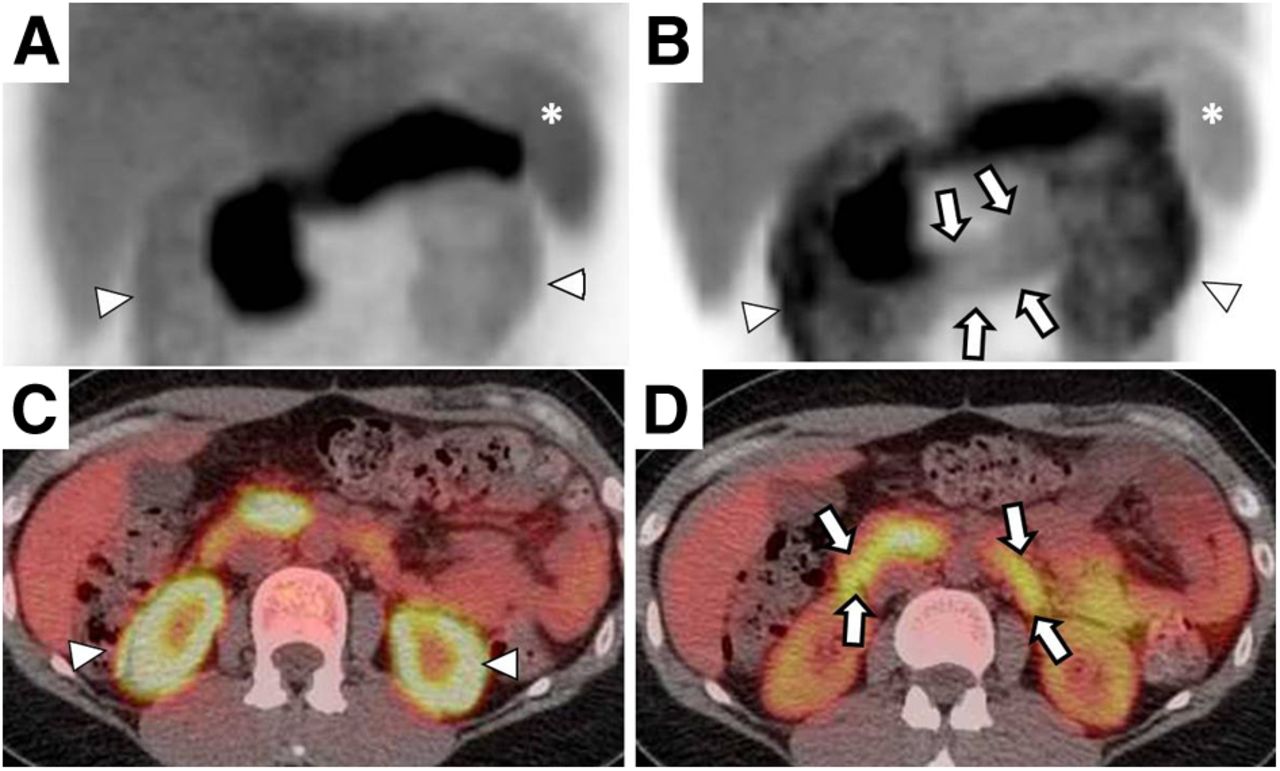
11C-acetate PET images. (A) In maximum-intensity-projection image at baseline, intense radiotracer activity is seen in pancreas. (B) In postsecretin stress image, pancreas is again clearly visualized, and additional activity is newly observed in duodenum (arrows). Kidneys (arrowheads) and spleen (asterisks) are also visualized. (C and D) Axial PET/CT fusion images of different subject before (C) and after (D) secretin stress.

Time–activity curves: changes in SUV over time derived from dynamic 11C-acetate PET studies before and after secretin stimulation in healthy volunteer.
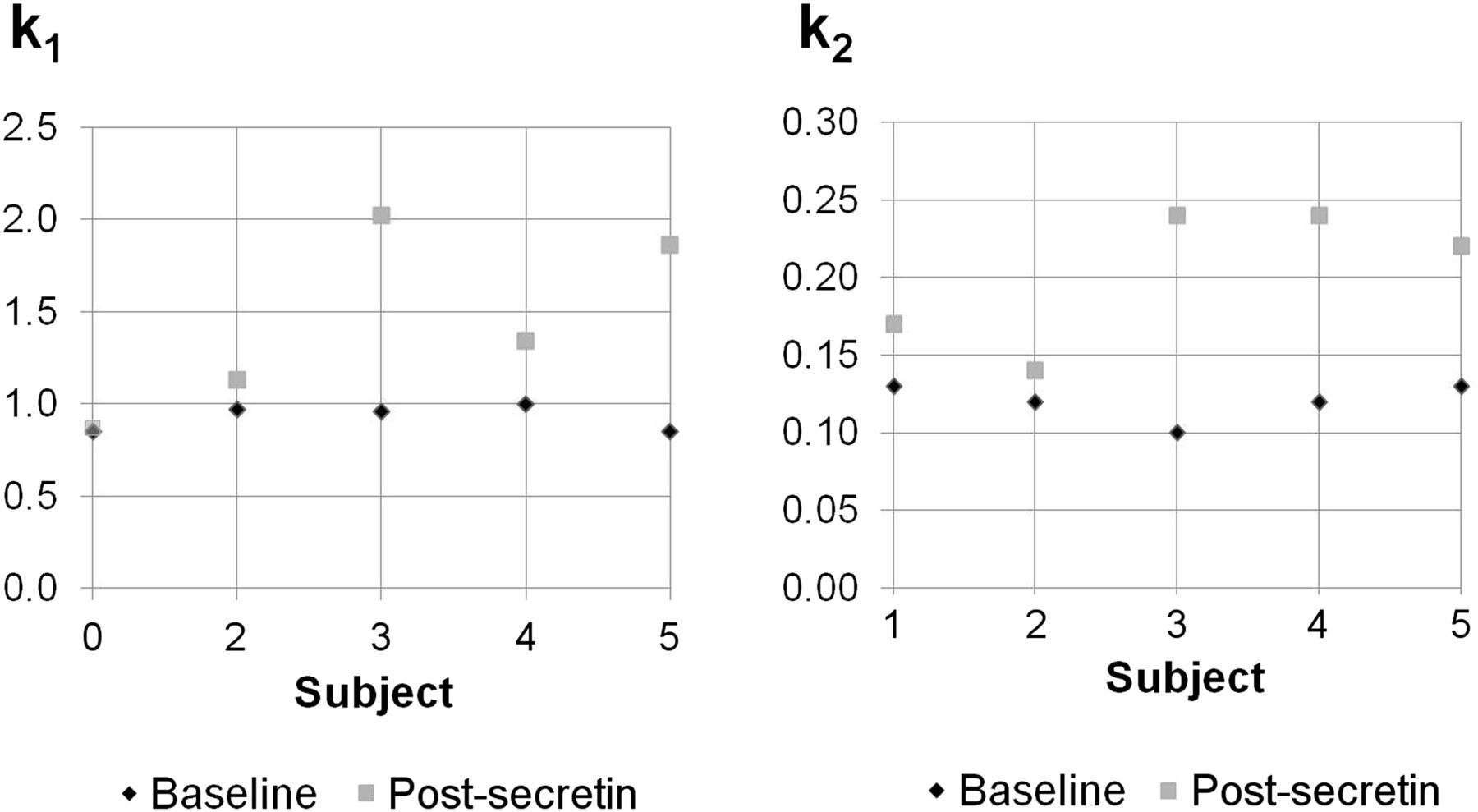
Pancreas k1 and k2 values at baseline and after secretin stimulation are shown with scatterplots (Table 1; Fig. 3). Compared with the kinetics of the baseline dynamic PET image, k1 and k2 were significantly increased after secretin stimulation in the 5 subjects.
k1 and k2 Values from Dynamic 11C-Acetate PET Studies
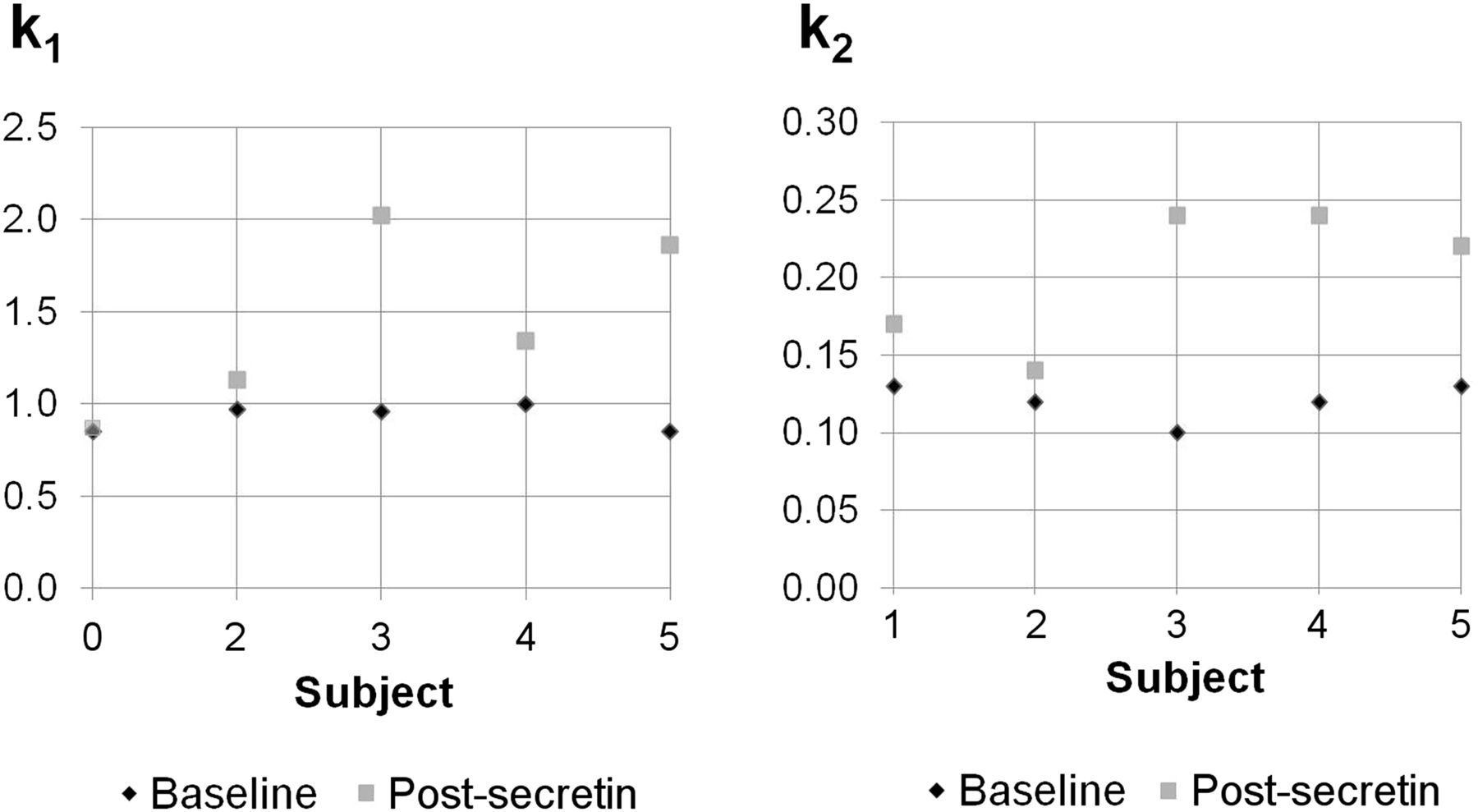
Scatterplots: k1 and k2 values from dynamic 11C-acetate PET studies.
The SULpeaks were measured from the pancreas using the summed PET images, and the pancreas-to-liver SULpeak ratios were computed (Table 2). In all cases, the pancreas-to-liver ratios decreased after secretin stimulation (P = 0.037).
Pancreas-to-Liver SULpeak Ratios from Summed 11C-Acetate PET Studies
DISCUSSION
To our knowledge, this was the first PET study to apply secretin stress to the imaging and quantification of pancreatic exocrine function. The addition of secretin stress is a noninvasive physiologic way to induce the pancreatic ductal cells to produce bicarbonate. The idea of using 11C-acetate to diagnose pancreatic diseases was introduced over 15 y ago (10). 11C-methionine, as a marker of amino acid metabolism in the pancreas, has also been helpful for assessing pancreatic function before and after pancreatectomy (11,12). Another previous study suggested the application of MR cholangiopancreatography using secretin to assess visual changes in the caliber of the pancreatic duct and the amount of pancreatic fluid excreted to the duodenum (13).
Several features were observed after secretin stress in this study: increased k1 and k2 in the pancreas and more prominent duodenal uptake. These findings may be explained by increased perfusion after secretin administration and by the metabolic pathway of 11C-acetate after entry into the pancreas. After β oxidation, the product 11CO2 can enter the bicarbonate pool as H11CO3 and be excreted to the duodenum. When secretin binds to the secretin receptor on pancreatic ductal cells, activated ion channels and exchangers will increase the bicarbonate, water, and electrolyte content of the pancreatic secretion (14,15). Since more bicarbonate is expected to promptly exit the pancreas and enter the duodenum after secretin stimulation, it could be expected that the washout rate of 11C-acetate would increase and the duodenum be better visualized. k1 is often reflective of blood flow, and an increase in blood flow to the pancreas after secretin stimulation might be expected to help meet the metabolic demands of the pancreas. Dynamic MR imaging without and with secretin stimulation was studied in healthy volunteers in a previous study, and the significant increase in pancreas perfusion observed in that study is consistent with our results (16). The greater activity in the duodenum could potentially be related to washout from the first administration, but on the basis of the half-life of 11C and the 2-h delay between the 2 scans, any residual activity would be expected to be negligible.
The k1 and k2 values were consistent in a tight range at baseline in the 5 subjects. The pancreas-to-liver SULpeak ratios observed in this study at baseline were also within the reference range (from 2.1 to 4.5) reported in a 1997 study (10) and suggest that subjects with normal pancreas exocrine function have a stable and narrow range of pancreas-to-liver SULpeak ratios. Note, however, that the distribution of 11C-acetate in the pancreas, liver, and other organs changes rapidly as a function of time. Furthermore, secretin seems to influence the time–activity curves, not only of the pancreas but of other organs including the liver and blood. Tracer kinetic modeling appears to be helpful in understanding these complex dynamic changes.
11C is limited by the short half-life. However, it is feasible, given the widespread distribution of medical cyclotrons, to have 11C tracers used clinically—as evidenced by the global use of 11C-methionine and 11C-choline, which recently received Food and Drug Administration approval in the United States. And although 18F-fluoroacetate has been described (17), further studies are needed to assess whether it is equivalent to 11C acetate in behavior.
In addition to being noninvasive, 11C-acetate PET has the additional advantage of causing only low radiation exposure. The use of 500 MBq of 11C-acetate produces an effective dose of approximately 2.45 mSv (18). A limitation of our study was our small sample size. A future study using 11C-acetate and secretin stress is planned for patients with pancreatic diseases.
CONCLUSION
Dynamic 11C-acetate PET studies before and after secretin stimulation are a promising and innovative, noninvasive approach for assessing basal and stimulated pancreatic exocrine function. Future studies should include both additional control subjects and additional patients with pancreatic diseases.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Judy Buchanan for scientific editing of the manuscript.
Footnotes
Published online May 19, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 9, 2013.
- Accepted for publication March 14, 2014.





{kind=link}
{kind=link}
{kind=link}