


Abstract
In this article, we will first describe the metabolic fate of 11C-acetate; then discuss its biodistribution in health and disease; and subsequently focus on its key clinical applications, the detection and localization of prostate cancer tissue in patients with primary or recurrent disease. Finally, we will discuss the potential role of 11C-acetate in the context of other prostate cancer imaging probes and non–radionuclide-based imaging approaches.
Identifying those primary prostate cancers that require aggressive interventions and localizing the origin of biochemical recurrence remain important yet still elusive clinical needs. Molecular imaging provides a diverse portfolio of PET probes for phenotyping and localizing prostate cancer tissue, including peptide and hormone receptor ligands and small molecules for metabolic phenotyping. The best use of these probes as diagnostic, predictive, and intermediate endpoint biomarkers within the framework of other available diagnostic tools has yet to be determined.
11C-acetate was originally used for PET measurements of myocardial oxidative metabolism because acetate enters the Krebs cycle after conversion to acetyl coenzyme A (CoA) to meet cellular energy demands (1–4). However, acetate has a diverse metabolic fate because it is also a substrate for lipid and cholesterol synthesis (5–7). Therefore, its increased cellular uptake reflects the increased membrane lipid demands of proliferating tissues.
The biology and clinical role of probing membrane lipid synthesis with 11C- and 18F-choline are discussed extensively elsewhere in this supplement. Suffice it to say that choline has its own transporter, and the rate-limiting enzyme in its synthetic (Kennedy) pathway (8) is choline kinase. Yet both acetate and choline are incorporated into membrane phospholipids in cancer cells and thus are likely to reflect the same process—that is, the increased demand for these lipids in cancers with increased cell turnover.
BIOLOGIC CORRELATES OF 11C-ACETATE IN PROSTATE CANCER
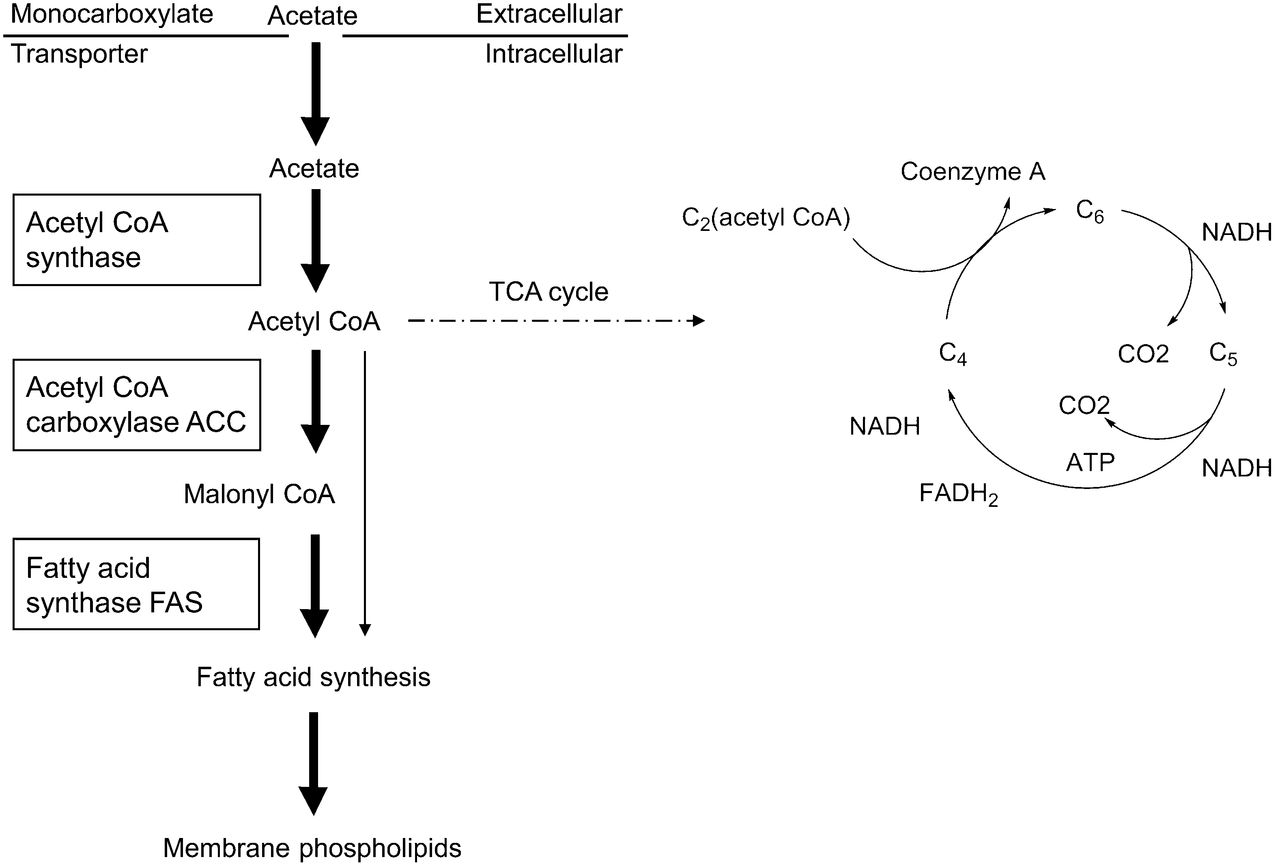
Acetate is an important substrate in the energy metabolism of cells. As an essential intermediate in catabolic and biosynthetic processes, its intracellular fate is diverse. On one hand, it is transported into tissues via the monocarboxylate transporter and is further metabolized to CO2 via the tricarboxylic acid cycle. This metabolic pathway has been exploited for imaging and quantifying myocardial oxidative metabolism (9–13). However, acetate use in cancer cells is governed predominantly by another metabolic process (Fig. 1). Cancer cells have an increased requirement for cell membrane lipids. In fact, acetate is the only carbon source for fatty acid and cholesterol synthesis. The rate-limiting enzyme in this pathway is fatty acid synthase (FAS). Its increased expression promotes de novo fatty acid synthesis from CoA, malonyl-CoA, and nicotinamide adenine dinucleotide phosphate in normal and abnormal tissues and meets the increased demand for membrane lipids (7,14,15). Overexpression of FAS correlates with prostate cancer aggressiveness (16) and high Gleason scores (17).

Fatty acid synthesis from acetate. Acetate is transported across cell membranes via monocarboxylate transporter and converted to acetyl CoA. It is then further metabolized by acetyl CoA carboxylase to malonyl CoA. FAS—the rate-limiting enzyme in fatty acid synthesis and 11C-acetate metabolism—further processes both acetyl CoA and malonyl CoA for fatty acid synthesis. Fatty acids are incorporated as phospholipids into cell membranes. ACC = acetyl-CoA carboxylase; ATP = adenosine triphosphate; FADH2 = reduced form of flavin adenine dinucleotide; NADH = nicotinamide adenine dinucleotide hydrate; TCA = tricarboxylic acid.
In support of the notion that FAS is the rate-limiting enzyme, in vitro studies have shown that cellular 11C-acetate uptake can be blocked with inhibitors of FAS and acetyl-CoA carboxylase (18). 11C-acetate uptake may therefore serve as a biomarker of FAS activity and thus of an important metabolic process in cancer, namely the increased lipid synthesis required for maintaining cell membrane integrity. 11C-acetate uptake may also serve as a pharmacodynamic biomarker of interventions targeting lipid synthesis in cancer.
11C-ACETATE BIODISTRIBUTION AND DOSIMETRY
The first synthesis of 11C-acetate dates back to 1943, when Buchanan et al. (19) labeled acetic, propionic, and butyric acids with 11C to determine contributions to liver glycogen synthesis. Subsequent synthesis approaches resulted in initial human biodistribution studies using an Anger camera (20). High-quality tomographic images of the human heart were first acquired by Pike et al. (21) in 1982, who used a scanner based on the design by Hoffman and Phelps (22).
The earliest reports on 11C-acetate imaging in cancer date back to 1995, when Shreve et al. (23) reported different tracer kinetics among normal myocardium, normal renal parenchyma, and renal cancer tissue. Myocardial and normal renal tissue showed rapid washout consistent with predominant oxidation to CO2 via the tricarboxylic acid cycle. In contrast, tracer was retained in tumor tissue, probably because of the use of 11C-acetate as an important substrate for the generation of membrane lipids.
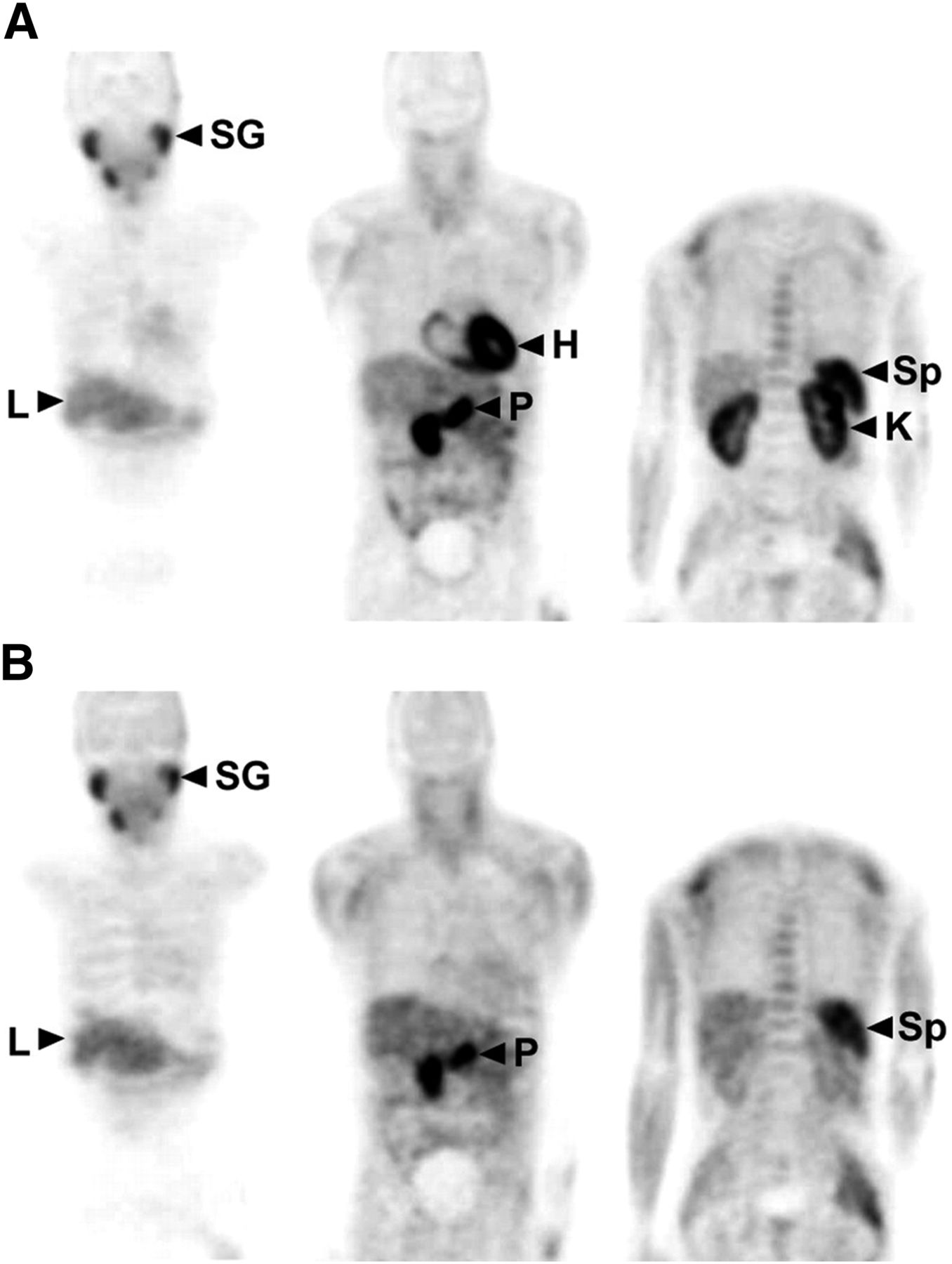
Systematic biodistribution and dosimetry studies (Fig. 2) were conducted by Seltzer et al. (24). They demonstrated early tracer accumulation in the myocardium, kidneys, pancreas, spleen, and bone marrow. In an advantage for prostate imaging, urinary bladder activity was notably absent because of the active reabsorption of 11C-acetate in the proximal convoluted tubule. Pancreas, kidneys, spleen, heart, and liver received the highest organ doses. The consistently high tracer uptake in the pancreas was recently exploited for secretin testing of the pancreatic exocrine function (25). The effective whole-body dose was low, at 0.0049 mSv/MBq. The same authors developed a model to describe acetate kinetics in prostate cancer (Fig. 3) (26).
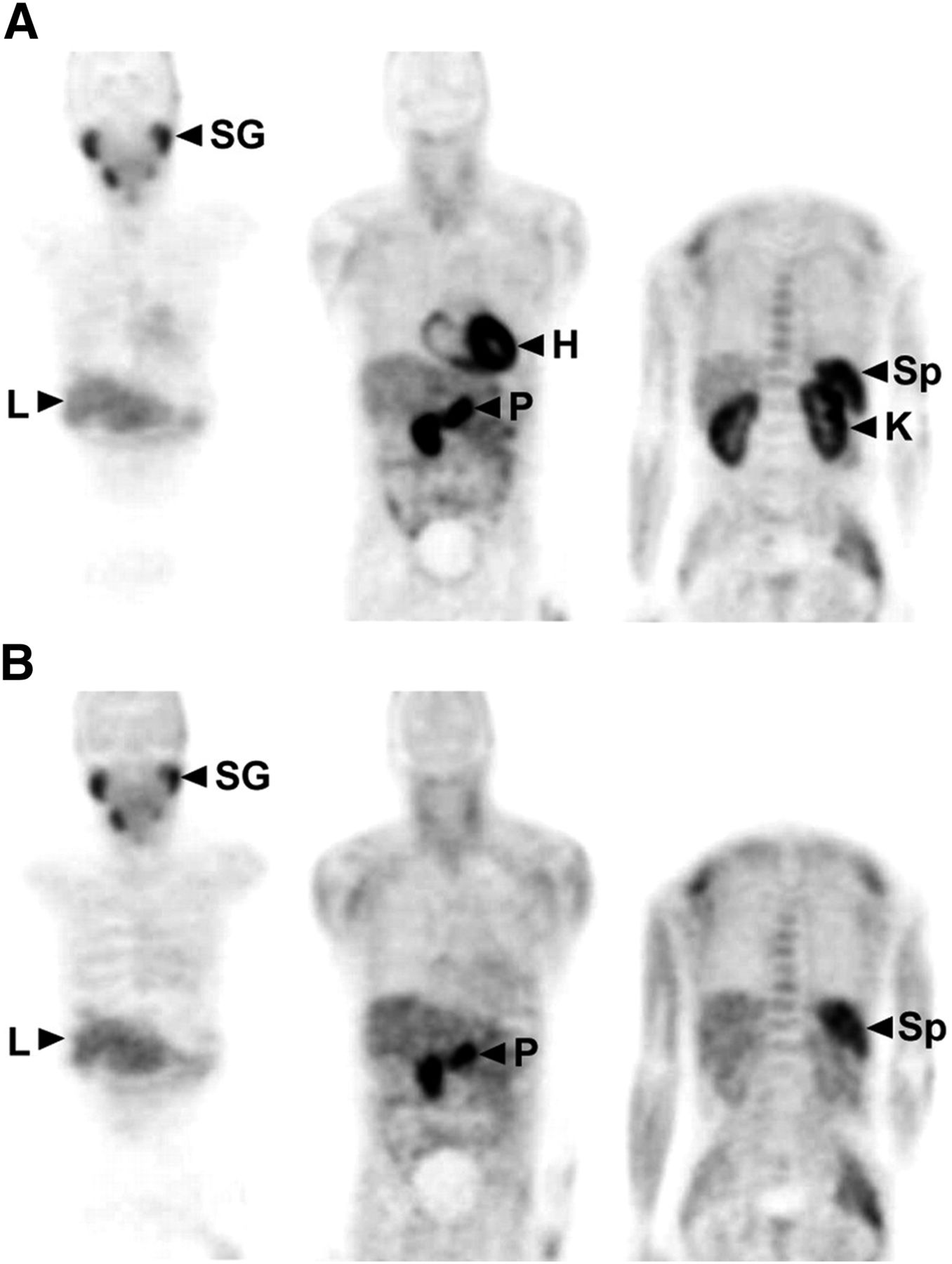
Whole-body 11C-acetate biodistribution images were obtained at 2 min (A) and 28 min (B). Note complete washout of heart activity and significant clearance from kidneys at later time point. Also note absence of bladder activity throughout study. H = heart; K = kidney; L = liver; P = pancreas; SG = salivary glands; Sp = spleen. Reprinted from (24).
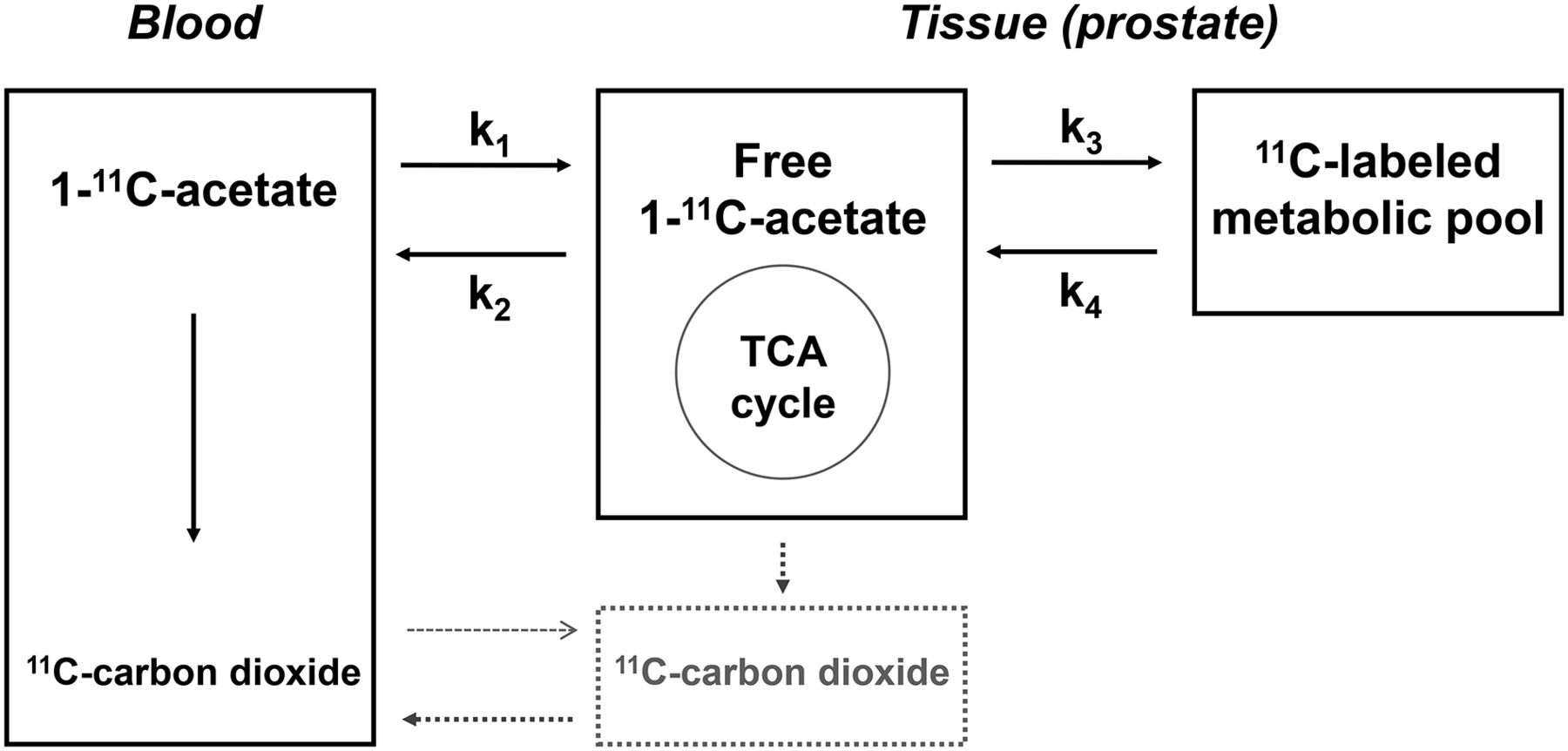
Kinetic model with 3 compartments and 2 tissues for prostate gland. CO2 concentration in tissue is low because of low intracellular pH. Intracellularly labeled CO2 (gray box) is negligible. Blood-to-tissue transport is minimal (gray arrow). Most labeled CO2 is transported rapidly to blood as part of k2. Metabolic pool consists of precursors for lipids, amino acids, fatty acids, and steroids that trap or retain 11C label. Labeled products of cycle also contribute to metabolic pool (as part of k3). Increase in tricarboxylic acid cycle metabolism would lead to increase in both k2 and k3. TCA = tricarboxylic acid. Reprinted from (26).
11C-ACETATE AS A DIAGNOSTIC BIOMARKER IN PROSTATE CANCER
Initially Staging Primary Prostate Cancer
11C-acetate PET cannot reliably distinguish between benign prostatic hyperplasia and prostate cancer. This was systematically demonstrated by Kato et al. (27), who studied 30 research subjects without and 6 patients with prostate cancer. Although the primary prostate cancer was visualized in all patients, differences in the 11C-acetate SUV between the subjects aged 50 years and older with normal prostate or benign prostatic hyperplasia and the patients with prostate cancer were not statistically significant. In fact, the normal prostate showed increasing 11C-acetate uptake with age. Somewhat contradictory findings were provided by Mena et al. (28), who demonstrated that 11C-acetate uptake in tumor was higher than that in normal prostate tissue. However, those authors confirmed that benign prostatic hyperplasia and cancer were indistinguishable. This finding was also previously reported quantitatively using a 3-compartment tracer kinetic model (26).
Despite the comparable tracer uptake in benign prostatic hyperplasia and cancer, the diagnostic accuracy of 11C-acetate PET for detecting primary prostate cancer was evaluated by several groups (Table 1). One of the earliest studies enrolled 22 patients with recently diagnosed prostate cancer (29). 11C-acetate PET detected prostate cancer with a sensitivity of 100%, which was superior to that of 18F-FDG. Mean SUVs ranged from 3.3 to 9.9 and were higher than those of 18F-FDG. The relatively high number of true-positive 18F-FDG studies is likely explained by the fairly advanced disease in 14 of the 22 patients, as evidenced by serum prostate-specific antigen (PSA) levels greater than 20 ng/mL in 15 patients. Because of the study design—only patients with known cancer were included—no data on specificity were provided.
Studies in Patients with Primary Prostate Cancer and Lymph Node Involvement
In the study by Mena et al. (28), 38 patients with presumed localized prostate cancer underwent 11C-acetate PET/CT and multiparametric MRI. All patients underwent prostatectomy after the scans. Serum PSA levels averaged 7.0 ± 8.9 ng/mL and ranged from 1.1 to 54 ng/mL. Fifteen patients had serum PSA levels of less than 4 ng/mL. On histopathology, 167 tumor foci were identified; 80 of those were larger than 5 mm. On a per-patient basis, PET/CT and MRI detected cancer in 34 and 37 of the 38 patients, respectively. On a lesion-based analysis, MRI was more sensitive than PET/CT (88.5% for combined MRI approaches vs. 73.4% for PET/CT; P value was not provided). Detectability with PET depended on lesion size rather than serum PSA levels (28).
Jambor et al. (30) evaluated 36 patients with untreated, nonmetastatic prostate cancer. Histopathology from prostatectomy (n = 10) and biopsy (n = 26) served as the standard of reference. Serum PSA levels averaged 9.8 ± 6.3 ng/mL (range, 2.9–30 ng/mL). A high sensitivity of 88% but a low specificity of 41% were reported at a lobe-based analysis (30). The same authors reported an even lower specificity when data analysis was limited to patients without extraprostatic cancer extension (31). Tumor aggressiveness (Gleason score) and degree of 11C-acetate uptake were unrelated (31). The low specificity may have been accounted for by benign prostatic hyperplasia. However, uptake in inflammatory cells may also have contributed to false-positive findings. Data from Schöder et al. (32) support this notion because a fairly large number of false-positive lymph nodes caused by granulomatous disease (possibly related to prior intravesical bacillus Calmette–Guerin treatment) were observed in their study. Consistently, another group reported increased 11C-choline uptake in a murine model of Chlamydia muridarum genital infection (33). Taken together, these data suggest that activation of lipid synthetic pathways very likely also occurs in rapidly proliferating inflammatory cells, accounting for false-positive findings.
Assessing Regional Lymph Node Involvement
As shown in Table 1, the ability of 11C-acetate PET to evaluate pelvic lymph nodes was determined in 4 studies. The first study included 107 patients with recently diagnosed intermediate- or high-risk prostate cancer who underwent primary surgery (34). All were imaged before surgery and were followed clinically to identify patients whose treatment failed and to determine whether this failure was associated with presurgical 11C-acetate PET findings. Presurgical PET identified abnormal 11C-acetate uptake in the prostate in 103 of the 107 patients. Metastases were seen in 34% of the 107 patients, mostly involving pelvic lymph nodes. The 36 patients with positive lymph nodes on PET had higher Gleason scores and pathology stages than did the patients with negative PET results. Although the sensitivity and specificity of 11C-acetate PET were modest on a per-patient basis, at 68% and 78%, respectively, a multivariate analysis showed that presurgical metastases identified on PET were independently and significantly associated with a 3.26-fold higher risk for treatment failure. This independent predictive power was maintained after surgery when the study was controlled for other postsurgical factors such as pathology stage, surgical Gleason score, and surgical margins.
The second study reported a lower sensitivity in 53 patients with newly diagnosed prostate cancer (35). Histopathology was the gold standard in all patients. The patient-based sensitivity for detecting lymph node involvement was only 38%, with a specificity of 96% and an accuracy of 68%. Positivity by 11C-acetate was associated with a greater number and larger size of involved nodes. Thus, because of the inability of 11C-acetate PET to detect small tumor-involved lymph nodes, the sensitivity of the test for lymph node involvement was not sufficiently high for its routine use to be recommended.
Another study enrolled 50 consecutive patients with high-average serum PSA levels and Gleason scores who were scheduled to undergo primary radiation treatment (36). This group was evaluated for whether the degree and extent of 11C-acetate PET abnormalities were associated with the estimated risk for pelvic lymph node metastases according to the nomogram described by Cagiannos et al. (37). Interestingly, the imaging approach was a better predictor of lymph node involvement than the nomogram. PET findings also affected patient management by changing the radiation approach in more than 40% of the patients.
The final study was performed in 19 patients before initial surgery (38). Pelvic lymph node dissection was the reference standard. Sensitivity and specificity on a patient basis were 90% and 67%, respectively. False-positive nodes were most likely due to inflammation. Importantly, nodal station–based analysis revealed a sensitivity of only 62%.
In summary, the available data on primary prostate cancer detection and lymph node staging with 11C-acetate are sparse. However, because of the modest sensitivity and specificity of 11C-acetate PET, it appears unlikely that this imaging approach will be helpful to diagnose, localize, and stage primary prostate cancers in patients with elevated PSA levels. The study by Haseebuddin et al. (34) suggests that prognostic information can be derived from presurgical 11C-acetate studies. In another report, 11C-acetate studies performed before radiation therapy altered the management in more than 40% of patients (36). These potential applications await further verification in larger prospective studies.
Identifying and Localizing the Source of Biochemical Recurrence
Biochemical evidence of prostate cancer recurrence (Table 2) after radical prostatectomy or radiation treatment, defined as a serum PSA level of 0.2 ng/mL or greater, frequently precedes the clinical manifestations of recurrent disease in the prostate bed, in regional lymph nodes, or at distant sites such as lymph nodes or bones. Local salvage therapy (radiation or surgery) is used in patients with regional pelvic lymph node and prostate bed recurrence, whereas systemic therapy is required to address distant metastases. In patients with locally recurrent disease, salvage radiation therapy can improve survival (39). Once metastatic disease develops, the prognosis is guarded, with a mean patient survival of 5 y (40). Therefore, early and accurate detection of the site of recurrence is critically important for patient management and therapy decisions. Figure 4 shows a representative case.
Studies in Prostate Cancer Patients with Biochemical Recurrence

Images of 59-y-old prostate cancer patient with biochemical recurrence (serum PSA level, 2.2 ng/mL). (A) Coronal whole-body PET image reveals focally increased uptake near pubic symphysis (1) and mild uptake in left internal iliac lymph node (2). (B–D) Axial 11C-acetate PET/CT images depict hypermetabolic left internal iliac lymph node (arrow, B) and pubic symphysis lesion (arrow, C), as well as mild sclerosis that was identified only in retrospect in bone windows (arrow, D).
It is important to understand the sensitivity or diagnostic range of 11C-acetate- and choline-based PET probes in prostate cancer assessments. Although 11C-acetate has the advantage of low or no urinary excretion, 18F-choline is more widely available because of its longer physical half-life. 11C-acetate and 11C-choline identified approximately only 50% of recurrence sites in patients with PSA levels of less than 1 ng/mL (41). Endorectal MRI was superior because it identified recurrence in 15 of 18 patients, suggesting that it was the modality of choice in patients with low serum PSA levels and a low likelihood of distant disease. In another small study in a mixed population of patients with primary or recurrent prostate cancer, 11C-choline and 11C-acetate failed to detect small-volume disease (42). In general, a high concordance between 11C-acetate and 11C- or 18F-choline findings is evident. For instance, 18F-choline and 11C-acetate performed nearly identically in 23 patients with biochemical recurrence after various primary therapeutic approaches. Disease was detected in only 3 of 6 patients having serum PSA levels of less than 1.0 ng/dL. However, detection rates increased with increasing PSA levels (43).
In an early clinical 11C-acetate study using dedicated PET systems in 31 patients, sites of recurrence were identified in 18 patients by biopsy (44). PET correctly identified 15 of these 18 patients. Importantly, disease sites were identified in 5 of 8 patients with serum PSA levels of less than 2.0 ng/mL. No false-positive findings were reported (44).
Oyama et al. (45) reported positive 11C-acetate findings in 59% of 46 patients with biochemical recurrence who were studied using a dedicated PET system. This study group included patients who had undergone prostatectomy (n = 30) and primary radiation treatment (n = 16). Their mean serum PSA levels were 4.9 and 5.8 ng/mL, respectively. Sites of recurrence remained in essence undetected in patients with serum PSA levels of less than 3 ng/mL. It appears quite likely that this comparably low yield is due to the lack of integrated PET/CT technology, which became available only later (46).
Good detection rates of early recurrences were reported by Albrecht et al. (47), who studied 32 patients. One group of patients had been treated with radiation, and another had undergone prostatectomy. Both had evidence of biochemical recurrence. However, median serum PSA levels were lower in the surgical group (mean, 0.4 ng/mL) than in the postradiation group (mean, 6 ng/mL). Identification of recurrence sites was significantly better in the latter group. However, detection of bone involvement was suboptimal.
True-positive findings in 15 of 20 patients but false-positive findings in 3 of 20 were reported by Sandblom et al. (48). This population, which was imaged with PET/CT, included patients with low-average serum PSA levels of 2.0 ng/mL; one site of recurrence was detected in a patient with a serum PSA level of 0.5 ng/mL. All patients with serum PSA levels of 2.0 ng/mL or greater showed abnormal probe uptake. Lung cancer, esophagitis, and nonspecific lymphadenopathy accounted for the 3 false-positive findings. The existence of false-positives is not surprising because of the high proliferation rates of cancer and inflammatory cells, resulting in increased requirements for membrane lipids.
A large retrospective analysis including 120 patients was published recently (49). Sixty-eight percent of the scans had positive findings for disease recurrence. Rates of positivity increased with serum PSA levels and PSA velocity. Using a PSA velocity threshold of 1.32 ng/mL/y resulted in sensitivity and specificity of 74% and 75%, respectively. A serum PSA level of 1.24 ng/mL was associated with a sensitivity and specificity of 87% and 66%, respectively. These data are equivalent to reports on 11C-choline (50,51).
A study that used PET/MRI software fusion may have provided insights into the potential of integrated PET/MRI for prostate cancer imaging (52). A software approach to fuse 11C-acetate PET, CT, and MR images was used in 50 patients who had been treated with radical prostatectomy (mean serum PSA level, 6.3 ng/mL), external beam radiation (mean serum PSA level, 12.4 ng/mL), or seed implantation (mean serum PSA level, 9.9 ng/mL). All had biochemical recurrence. The authors reported that image fusion improved diagnostic information. For instance, fusion with MRI revealed 9 malignant and 5 benign etiologies in 14 patients with equivocal PET findings. Fusion with MR images was more informative than fusion with CT images, suggesting an important potential indication for integrated clinical PET/MRI in patients with recurrent prostate cancer. As a limitation, only a relatively small number of lesions was verified histopathologically. However, clinical management was changed in 28% of the patients.
Assessing Distant Metastatic Disease
A small study of 8 patients demonstrated that distant disease was detected in one more patient with 11C-acetate than with 18F-FDG (53). Whether this difference is clinically meaningful is unknown. In a more recent and much larger study, Spick et al. (54) retrospectively compared conventional bone scans with 11C-acetate PET findings for detecting bone metastases in 90 patients with rising PSA levels after initial definitive therapy. Clinical and imaging follow-up served as the reference standard. Conventional bone scans and 11C-acetate PET were comparable on a patient-based analysis. This observation suggests that 11C-acetate PET imaging can reliably survey the whole body for bone involvement.
11C-ACETATE AS A PREDICTIVE, PROGNOSTIC, AND INTERMEDIATE ENDPOINT BIOMARKER
Well-designed prospective clinical studies to determine whether 11C-acetate can serve as a predictive, prognostic, or intermediate endpoint biomarker are lacking. Predictive biomarkers are designed to determine whether a specific therapeutic target is expressed (Fig. 5) (55). FAS is overexpressed in prostate and other cancers and has been explored as a potential therapeutic target. Orlistat, a selective inhibitor of FAS, was tested for target inhibition in murine prostate cancer models. The degree of target expression as determined with 11C-acetate imaging correlated with response to FAS inhibition (55).

Three different tumor xenografts (arrows) having various expression levels of FASN gene exhibit proportional 11C-acetate uptake. L = liver; S = stomach. Adapted and reprinted from (55).
Limited information on the prognostic value of 11C-acetate PET imaging is available. In one study of 123 patients with biochemical recurrence, 11C-acetate uptake was associated with higher PSA velocity (ng/mL/mo). Further significant correlations with the initial Gleason score also suggest the prognostic value of 11C-acetate imaging in biochemically recurrent prostate cancer (56).
We are unaware of clinical studies that have systematically evaluated 11C-acetate as an intermediate endpoint biomarker. In a preclinical study, mice were imaged with 18F-FDG and 11C-acetate before and after androgen ablation (57). Diethylstilbestrol treatment caused a decrease in 18F-FDG uptake in prostate tumors, whereas a change in acetate tumor uptake in the androgen ablation mice was not significant. Rather than indicating a failure of 11C-acetate to demonstrate treatment-induced changes, these findings point to our need to better understand the interplay among various metabolic pathways and their alterations in response to therapy.
Anecdotal evidence suggests that 11C-acetate may be useful as an intermediate endpoint biomarker in prostate cancer treatment. Changes in 11C-acetate 6–12 wk after the start of systemic therapy correlated with clinical response in 6 patients (53).
VALUE OF 11C-ACETATE IN THE PORTFOLIO OF PET IMAGING PROBES IN PROSTATE CANCER
For 2 decades, PET imaging of prostate cancer was considered frustrating because of the perceived paucity of useful imaging markers. With regard to diagnostic accuracy for initial detection and staging, this negative bias is understandable. However, with regard to disease phenotyping, the imaging community offers a wide spectrum of metabolic, peptide receptor, and antibody PET probes, which are addressed elsewhere in this supplement. Glucose metabolic PET imaging in prostate cancer is underappreciated. For instance, 18F-FDG and 11C-acetate were compared in a mixed population of patients with primary and recurrent prostate cancer. This study provided interesting insights into different metabolic phenotypes. Bone metastases were more glycolytic than primary prostate cancer lesions and pelvic lymph node metastases that showed higher 11C-acetate avidity, suggesting different metabolic needs of primary versus metastatic lesions (58). The phenotypic information derived for primary and metastatic lesions may well provide critically important prognostic and predictive information and may help us arrive at more precise treatment approaches.
CONCLUSION
A wealth of novel imaging probes, together with emerging technologies such as PET/MRI, raises expectations that molecular PET imaging will have a significant role in the management of patients with prostate cancer. How each of the available PET probes will best be deployed remains to be determined.
DISCLOSURE
Johannes Czernin is a founder and shareholder of Sofie Biosciences and Trethera Therapeutics. Ken Herrmann is a consultant of Sofie Biosciences. No other potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 8, 2016.
- Accepted for publication March 10, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- BIOLOGIC CORRELATES OF 11C-ACETATE IN PROSTATE CANCER
- 11C-ACETATE BIODISTRIBUTION AND DOSIMETRY
- 11C-ACETATE AS A DIAGNOSTIC BIOMARKER IN PROSTATE CANCER
- 11C-ACETATE AS A PREDICTIVE, PROGNOSTIC, AND INTERMEDIATE ENDPOINT BIOMARKER
- VALUE OF 11C-ACETATE IN THE PORTFOLIO OF PET IMAGING PROBES IN PROSTATE CANCER
- CONCLUSION
- DISCLOSURE
- REFERENCES
- Figures & Data
- Info & Metrics