


Abstract
National Comprehensive Cancer Network guidelines consider 18F-FDG PET/CT for only clinical stage III breast cancer patients. However, there is debate whether TNM staging should be the only factor in considering if PET/CT is warranted. Patient age may be an additional consideration, because young breast cancer patients often have more aggressive tumors with potential for earlier metastases. This study assessed PET/CT for staging of asymptomatic breast cancer patients younger than 40 y. Methods: In this Institutional Review Board–approved retrospective study, our hospital information system was screened for breast cancer patients younger than 40 y who underwent staging PET/CT before any treatment. Patients with symptoms or conventional imaging findings suggestive of distant metastases or with prior malignancy were excluded. Initial stage was based on physical examination, mammography, ultrasound, and breast MR imaging. PET/CT was then evaluated to identify unsuspected extraaxillary regional nodal and distant metastases. Results: One hundred thirty-four patients with initial breast cancer stage I to IIIC met inclusion criteria. PET/CT findings led to upstaging to stage III or IV in 28 patients (21%). Unsuspected extraaxillary regional nodes were found in 15 of 134 patients (11%) and distant metastases in 20 of 134 (15%), with 7 of 134 (5%) demonstrating both. PET/CT revealed stage IV disease in 1 of 20 (5%) patients with initial clinical stage I, 2 of 44 (5%) stage IIA, 8 of 47 (17%) stage IIB, 4 of 13 (31%) stage IIIA, 4 of 8 (50%) stage IIIB, and 1 of 2 (50%) stage IIIC. All 20 patients upstaged to stage IV were histologically confirmed. Four synchronous thyroid and 1 rectal malignancies were identified. Conclusion: PET/CT revealed distant metastases in 17% of asymptomatic stage IIB breast cancer patients younger than 40 y. Although guidelines of the National Comprehensive Cancer Network recommend against systemic staging in patients with stage II disease, our data suggest that PET/CT might be valuable in younger patients with stage IIB and III disease. Use of PET/CT in younger patients has the potential to reduce the morbidity and cost of unnecessary therapies in young breast cancer patients.
PET/CT with 18F-FDG is useful in staging selected breast cancer patients. The question of which clinical stages of breast cancer patients benefit from a PET/CT scan remains a matter of debate. The 2013 guidelines of the National Comprehensive Cancer Network consider the use of PET/CT scanning in patients with stage III disease or when standard staging studies are equivocal or suspicious (1). Earlier studies reported a high impact of PET/CT mainly for staging of large or inflammatory primary cancers (2–4). More recent reports have demonstrated that PET/CT may also lead to stage changes in patients with earlier stage disease (5–8). For example, Bernsdorf et al. studied 103 stage I–III patients with primary tumors of 2 cm or more (5), with upstaging of the initial stage in 14 (14%).
There is debate whether initial clinical TNM staging of breast cancer is the only factor that should be considered when deciding if a staging PET/CT scan is warranted. In a letter regarding the Bernsdorf study, Gilardi et al. suggested that biologic differences of breast cancers should also be considered, because certain biologic subtypes of breast cancer have a greater propensity to develop metastases even at an early stage (9,10). One clinical factor that portends biologic aggressiveness is patient age. Breast cancer in women younger than 40 y is associated with a higher incidence of biologically unfavorable factors such as higher grade, larger size, and estrogen receptor (ER)–negative histology (11,12). Furthermore, in a retrospective study of 240,012 breast cancer patients, women with stage I/II breast cancer who were younger than 40 y were more likely to die of breast cancer than older women (11). This may be due to higher frequency of metastatic disease undetected by conventional staging techniques. Consequently, staging with 18F-FDG PET/CT may have greater impact in younger breast cancer patients. In this study, we evaluated the impact of 18F-FDG PET/CT staging in clinical stage I–III breast cancer patients younger than 40 y and compared the rate of upstaging between biologic subgroup categories.
MATERIALS AND METHODS
Study Design
This retrospective single-institution study was performed under Health Insurance Portability Account Act compliance and Institutional Review Board approval, with the requirement to obtain informed consent waived by the board. The Memorial Sloan Kettering Cancer Center (MSKCC) Hospital Information System (HIS) was screened for stage I–IIIC breast cancer patients younger than 40 y who had 18F-FDG PET/CT performed before beginning treatment at our institution between January 2003 and December 2012. This range of dates was selected because PET/CT, rather than PET alone, was initiated at our institution in 2002, and data analysis for this study began in January 2013. Electronic medical records were reviewed and patients with the following characteristics were excluded: known stage IV disease before PET/CT; patients with prior malignancies (except nonmelanoma skin cancer); and patients with any treatment before PET/CT, including systemic cancer therapy, local radiation treatment, or curative surgery. In addition, to minimize the selection bias that is inherent to a specialized cancer referral center, we excluded patients with symptoms or conventional imaging findings equivocal or suspicious for stage IV disease before PET/CT and patients with PET/CT scanning performed before their first presentation at our institution.
Electronic medical records were reviewed in the MSKCC HIS, and the following patient characteristics were recorded for each patient who underwent PET/CT: age at diagnosis, race, clinical stage before PET/CT, histology, tumor grade, and receptor phenotype. To address potential selection bias in our cohort of patients who underwent PET/CT, we compared the patient characteristics of our PET/CT cohort with a cohort of all stage I–IIIC breast cancer patients at our institution in the same time period who did not undergo a staging PET/CT before treatment but met all other inclusion and exclusion criteria.
The 18F-FDG PET/CT scan was reviewed, and the following data were recorded: extraaxillary regional (infraclavicular, supraclavicular, and internal mammary) nodal metastases, distant metastases, synchronous malignancies, and the method of verification of PET/CT findings. Histology was the preferred method to verify malignancy for PET/CT findings. When histology was not available, follow-up imaging was used. Lesions had to show typical features of metastatic disease on initial imaging and show response to treatment. For internal mammary lymph nodes without histopathology or follow-up imaging, maximum standardized uptake values (SUVs) of 2.0 or higher were used to validate malignancy. This validation was based on the well-accepted notion that reactive 18F-FDG avidity is rare in internal mammary nodes, especially in patients without prior surgery, and that reactive internal mammary nodes tend to have maximum SUVs below 2.0 (13).
Determination of Stage and Stage Modification
Cancer stages were determined according to the American Joint Committee on Cancer staging manual (14). Initial clinical stage was determined by reviewing the clinical notes of the physical examination, mammography, breast ultrasound, and, if available, breast MR imaging. PET/CT results were then used to determine the patient’s stage after PET/CT. The initial clinical stage was compared with clinical stage after PET/CT to determine the rate of upstaging.
Imaging and Interpretation
Before 18F-FDG injection for PET/CT, patients fasted for at least 6 h. Each patient was injected intravenously with 444–555 MBq (12–15 mCi) of 18F-FDG when plasma glucose was less than 200 mg/dL. After 18F-FDG injection, patients rested for a 60- to 90-min uptake period, followed by image acquisition. PET/CT scans were acquired with the patient supine from the base of the skull to the mid thigh. In most of the cases, low-dose CT scans with oral contrast were obtained. Rarely, intravenous contrast was administered. In all cases, attenuation-corrected images were reviewed on a PACS workstation (AW suite 2.0; GE Healthcare), displaying a maximum-intensity-projection image and multiplanar PET, CT, and PET/CT fusion images. SUVs, normalized to body weight, were determined on the AW suite. According to standard 18F-FDG PET/CT reporting, uptake was considered abnormal when it was focal, it was not considered physiologic or inflammatory, and it had intensity greater than local background. Suspicion for malignancy was based on the integration of the metabolic information from the PET images, the anatomic information on CT images, and the fused PET/CT images.
One reader with 4 y of PET/CT experience evaluated all PET/CTs masked to the original PET/CT report and final diagnosis. If the assessment of the primary reader differed from the original PET/CT report, a second reader, with 9 y of PET/CT experience and masked to the original PET/CT report and final diagnosis, was consulted to determine a consensus.
Statistics
Medians and ranges were used to summarize continuous variables and frequencies, and percentages were used to summarize categoric variables, including extraaxillary lymph node metastases, distant metastases, and upstaging to stage III or IV. Patient subgroups were defined on the basis race, histology, tumor grade, and receptor phenotype, to see if these characteristics were associated with a higher yield on PET/CT. Race was grouped into African American, Asian, Caucasian, and other. Histology was grouped as ductal, lobular, mixed ductal/lobular, and other. Pathologic grade was dichotomized into grade 1–2 versus grade 3. Receptor profiles were grouped as ER-positive/human epidermal growth factor 2–negative (ER+/HER2−), HER2-positive (HER2+), triple negative, and other. The associations between clinical parameters and upstaging, extraaxillary nodal disease, and distant metastases were evaluated using logistic regression. The odds ratio, along with its 95% confidence interval, was provided for each comparison.
The cohort of patients who received PET/CT was compared with a cohort of patients who met all other inclusion criteria but did not undergo PET/CT using the Fisher exact test for categoric variables and the Wilcoxon rank sum test for continuous variables. All analyses were performed using SAS 9.2 (SAS Institute).
RESULTS
Patient and Tumor Characteristics
An HIS search revealed 345 stage I–IIIC breast cancer patients younger than 40 y who underwent 18F-FDG PET/CT before beginning treatment at our institution between January 2003 and December 2012. Of the 345 patients, 211 were excluded because of the following reasons: prior malignancies (n = 18), symptoms (n = 35) or conventional imaging findings (n = 65) suggesting stage IV disease, PET/CT performed at an outside facility before presentation at our hospital (n = 92), and prior outside treatments (n = 68). Some patients met more than one exclusion criterion. The remaining 134 patients form the PET/CT cohort.
The median age of the PET/CT cohort was 36.2 y and ranged from 22.2 to 39.9 y. The median time between initial diagnosis and PET/CT was 21.5 d (range, 0–112 d). Before PET imaging, 15% of the 134 patients were clinical stage I, 33% stage IIA, 35% stage IIB, and 17% stage III. Most patients had invasive ductal cancers (92%), most of the cancers were grade 3 tumors (82%), and most of the cancers were ER+/HER2− (56%). Details on patient and tumor characteristics are summarized in Table 1.
Characteristics of Patients and Tumors
To address potential selection bias in our cohort of patients who underwent PET/CT, we compared the patient characteristics of our cohort with a cohort of stage I–III breast cancer patients who did not undergo a staging PET/CT but met all other inclusion and exclusion criteria, to see if our PET/CT cohort differed in a systematic way. There was no difference between the 2 groups in terms of age (P = 0.41), race (P = 0.16), histology (P = 0.16), tumor grade (P = 1.00), or receptor phenotype (P = 0.11). However, as expected, the 2 groups differed in terms of clinical stage (P < 0.0001). Patients who received PET/CT were of higher stages than the patients who did not receive PET/CT. Details on how patients in our PET/CT cohort compared with patients who did not receive PET/CT are summarized in Table 1.
Upstaging by PET/CT
PET/CT demonstrated unexpected extraaxillary regional nodal and distant metastases in 28 of 134 patients (21%), including 15 (11%) with extraaxillary regional nodal metastases and 20 (15%) with distant metastases, with 7 cases demonstrating both.
Distant Metastases
All 20 patients upstaged to stage IV were proven by histopathology (Figs. 1–3). Of the 20 patients, 16 had osseous metastases, 6 had distant nodal metastases, 5 had liver metastases, 2 had lung metastases, and 1 had a splenic metastasis, with 7 patients having more than one distant metastatic site. Upstaging to stage IV occurred in 1 of 20 initial clinical stage I patients, 2 of 44 stage IIA, 8 of 47 stage IIB, 4 of 13 stage IIIA, 4 of 8 IIIB, and 1 of 2 stage IIIC (Table 2). None of the lesions suspicious for distant metastasis on 18F-FDG PET/CT was false-positive, as all the lesions were biopsy-proven.
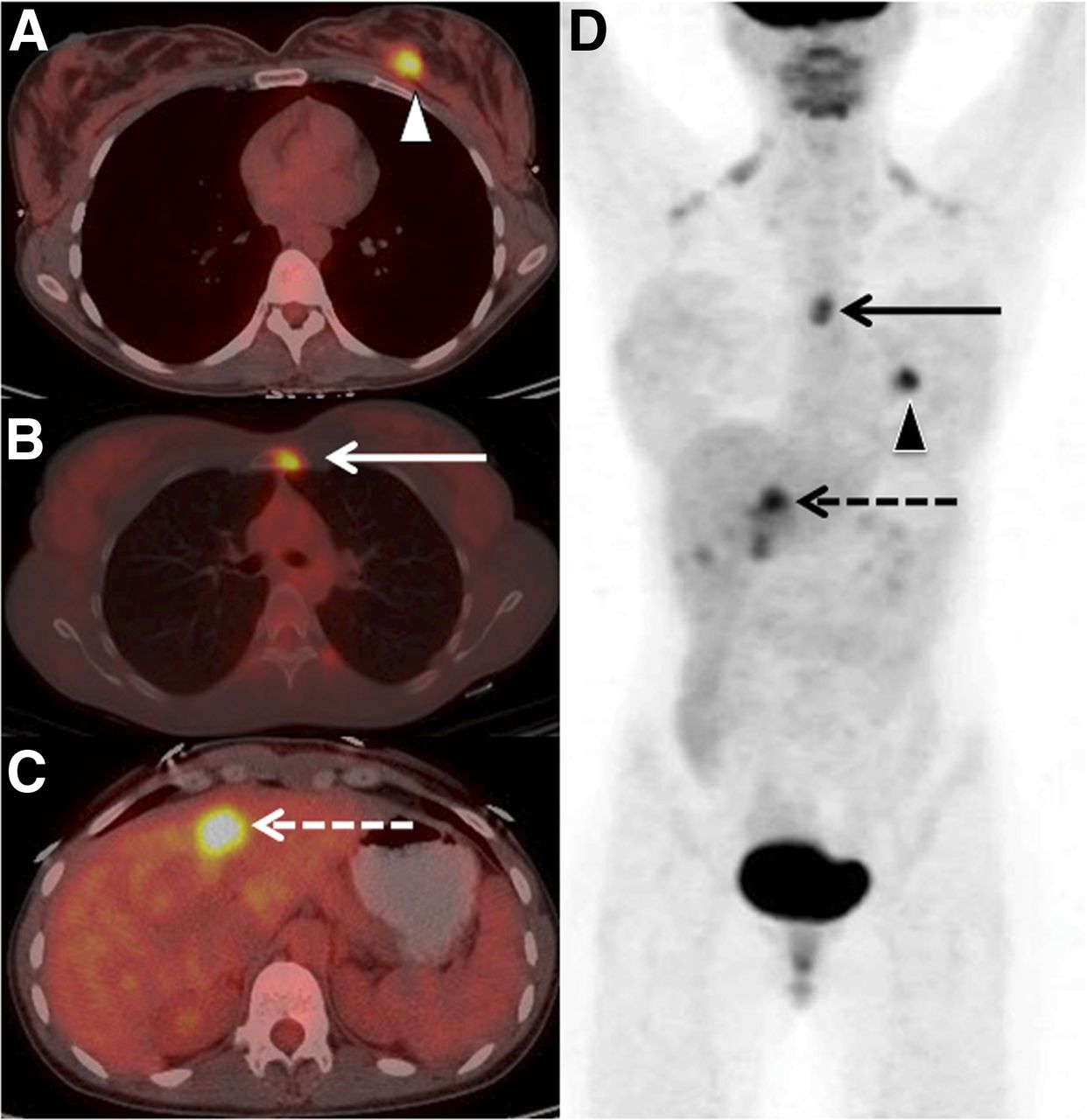
A 29-y-old woman with clinical stage IIA breast cancer upstaged to stage IV by 18F-FDG PET/CT. Axial PET/CT images demonstrated known primary left breast cancer (arrowhead) (A), previously unknown osseous metastasis (solid arrow) (B), and previously unknown liver metastasis (dashed arrow) (C) proven by biopsy. (D) Maximum-intensity-projection PET gives overview of all lesions.

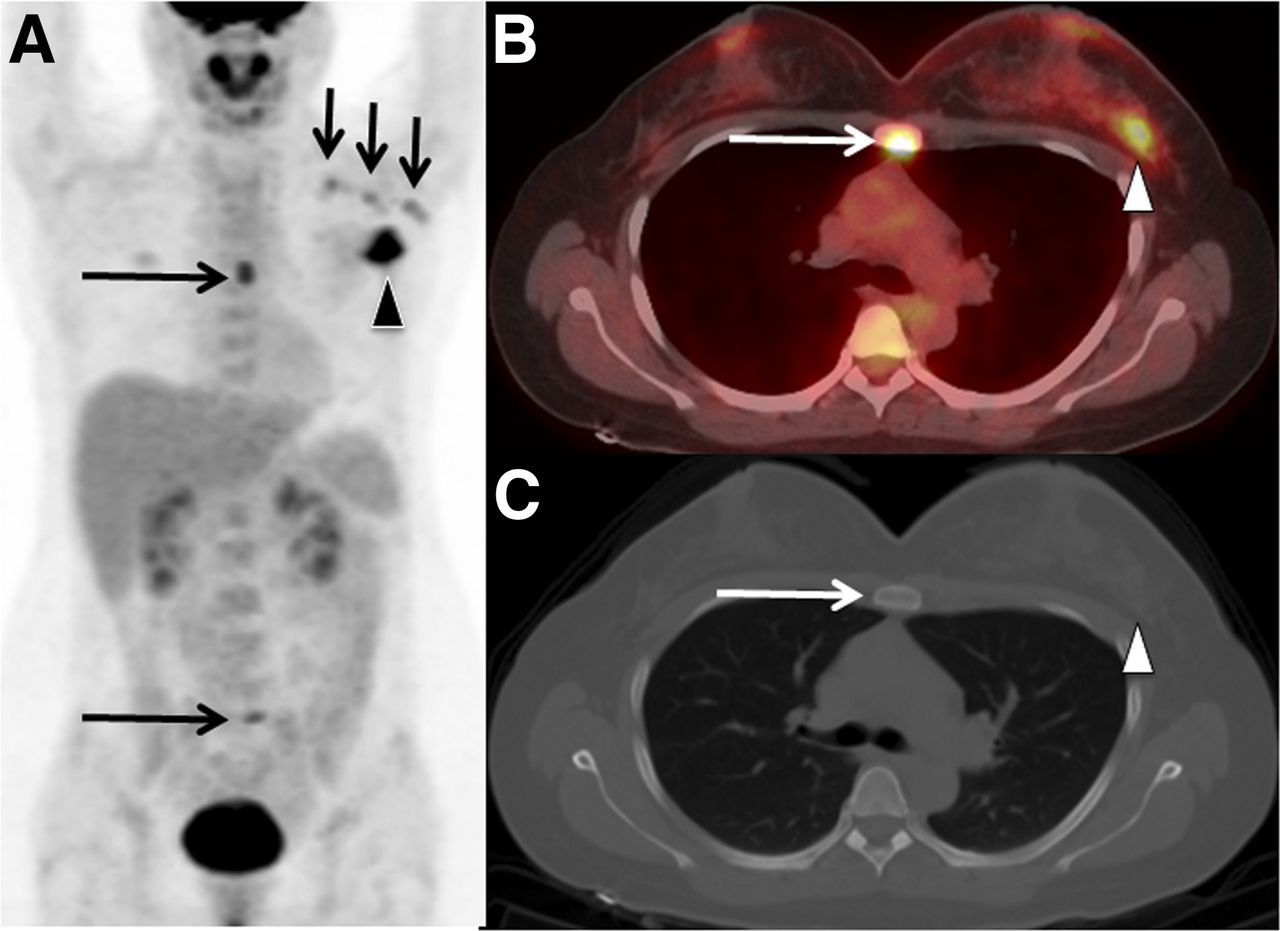
A 32-y-old woman with clinical stage IIB breast cancer upstaged to stage IV by 18F-FDG PET/CT. (A) Maximum-intensity-projection PET demonstrated known primary left breast cancer (arrowhead), known axillary nodal metastases (short arrows), and 2 foci of 18F-FDG uptake in midline of body (long arrows). Axial PET/CT (B) and axial CT (C) through chest demonstrated primary breast cancer (arrowhead) and localized 1 of the midline foci to sternum without osteolytic or osteoslcerotic correlate on CT (long arrows). Biopsy of sternum demonstrated osseous metastasis unknown before PET/CT. Second midline focus was subsequently proven to be sacral metastasis (not shown).

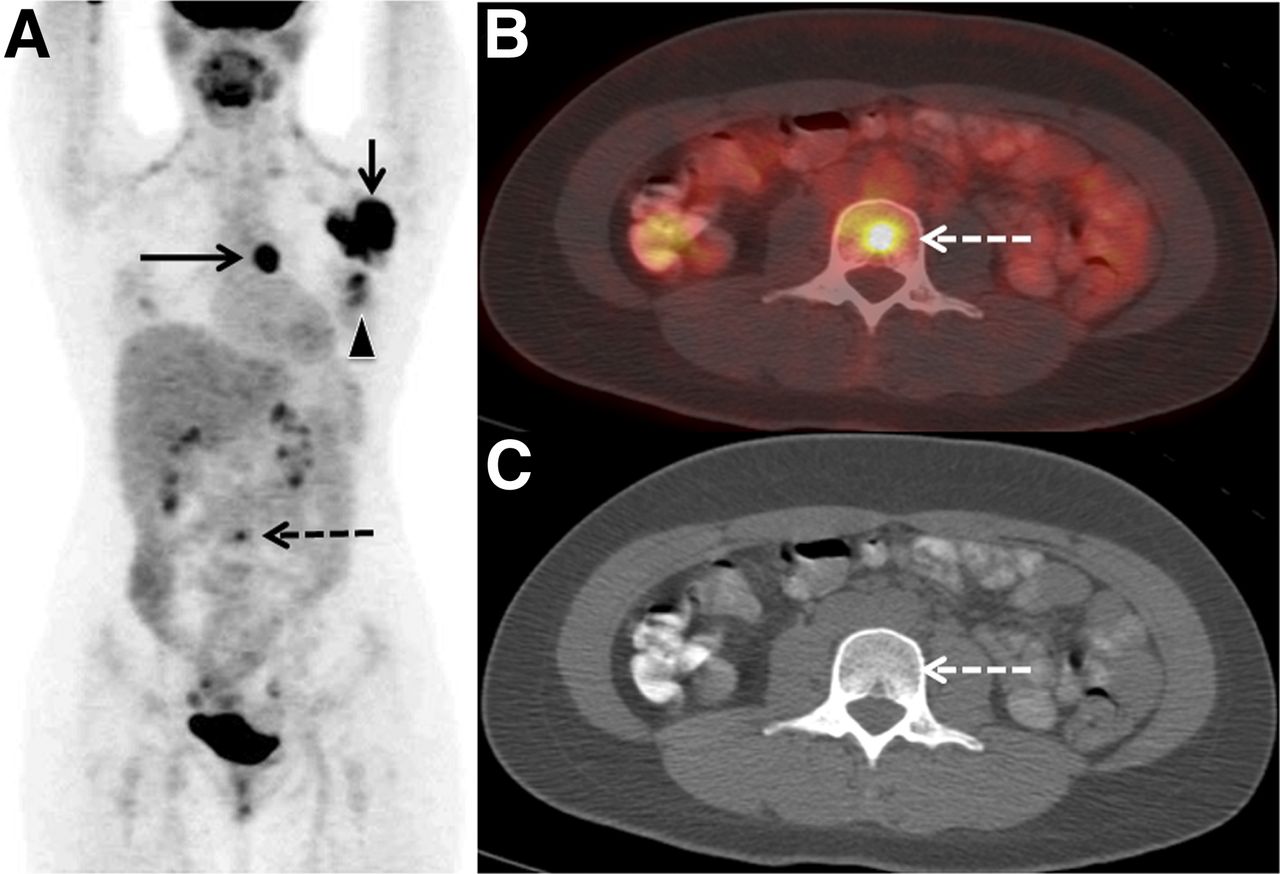
A 35-y-old woman with clinical stage IIIA breast cancer upstaged to stage IV by 18F-FDG PET/CT. (A) Maximum-intensity-projection PET demonstrated known primary left breast cancer (arrowhead), known axillary nodal metastases (short arrow), previously unknown internal mammary node (solid long arrow), and focus of 18F-FDG uptake in region of lumbar spine (dashed long arrow). Axial PET/CT (B) and CT (C) localize latter focus to L3 vertebral body without osteolytic or osteoslcerotic correlate on CT (dashed long arrows). Biopsy of L3 lesion demonstrated osseous metastasis and stage IV disease unknown before PET/CT. Given stage IV disease, biopsy of internal mammary nodal focus was unnecessary.
Summary of Cases Upstaged by PET/CT Based on Initial Clinical American Joint Committee on Cancer Stages (14)
Of the 20 patients with distant metastases detected on PET/CT, 5 (25%) were grade 2 primary malignancies and 15 (75%) were grade 3. In comparison, 17% of the total cohort had grade 2 primary malignancies and 82% were grade 3 (Table 1).
Extraaxillary Regional Nodal Metastases
Fifteen cases of unsuspected extraaxillary regional nodal metastases were included in this analysis. Seven of these also demonstrated distant metastases. In these 7 patients, the extraaxillary nodal metastases were not sampled because biopsy proof of distant metastases confirmed stage IV disease and made regional node biopsy dispensable (Fig. 3). Of the remaining 8 cases, 2 were suspicious infraclavicular nodes that were proven on pathology; 3 were verified by changes on imaging follow-up (Fig. 4); and 3 were suspicious internal mammary nodes with no biopsy or adequate imaging follow-up, which were considered malignant based on their SUV above 2 (3.6, 4.3, and 5.1) (13). One additional internal mammary node called suspicious in the PET/CT report, with an SUV of 1.1 and no means of verification, was not considered positive for the purpose of this analysis. Of the 15 extraaxillary regional nodal metastases, 11 included internal mammary nodes, 4 included supraclavicular nodes, and 2 included infraclavicular nodes.

A 38-y-old breast cancer patient with internal mammary nodal metastasis detected by 18F-FDG PET/CT and verified by imaging follow-up. Axial PET/CT (A) and maximum-intensity-projection PET images (B) demonstrate known primary left breast cancer (arrowheads), known left axillary node (short arrows), and previously unknown left internal mammary node (long arrows). Axial PET/CT (C) and maximum-intensity-projection PET images (D) following 5 mo of neoadjuvant chemotherapy demonstrated complete resolution of all 18F-FDG–avid lesions. Findings on imaging follow-up were considered validation of extraaxillary nodal metastasis.
Subgroup Analysis
We examined the relationship between receptor status and upstaging by PET/CT, metastases, and extraaxillary lymphadenopathy. No statistically significant relationships were found between upstaging and race (P = 0.27), tumor grade (P = 0.99), or receptor phenotype (P = 0.52). Similarly, race, grade, and receptor phenotype were not found to relate to distant metastases (P = 0.33–0.41) or extraaxillary lymphadenopathy (P = 0.63–0.96). Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org) provides more information.
Synchronous Malignancies
Five synchronous malignancies (4%) were found in 134 cases. Four of these cases were papillary thyroid cancers and 1 was a rectal cancer (T3N0M0) that measured 8 × 3 cm in a 35-y-old woman.
DISCUSSION
To maximize yield of 18F-FDG PET/CT, while reducing cost and unnecessary radiation, it is important to determine appropriate criteria for use. Patient age may be 1 criterion that alters the yield of 18F-FDG PET/CT. Several studies suggest that breast cancers arising in young patients may differ from those occurring in older women (11,12). Younger women have tumors that are more likely to be high grade, larger size, ER−/PR−, and lymph node–positive and have a shorter tumor doubling time (11). Indeed, early-stage breast cancer in women younger than 40 y has been reported to have a worse prognosis than in older women (11). One possible explanation for this discrepancy is that younger women more often have unsuspected higher stage disease at the time of diagnosis. Our study investigated the value of PET/CT for detecting unsuspected higher stage disease at the time of diagnosis in women younger than 40 y. PET/CT outperforms conventional imaging modalities in the assessment of distant metastases (2,3,15), which upstage a patient to stage IV. Timely detection of distant metastases spares women futile breast surgeries and changes the intent of systemic therapy from cure to palliation. In addition, early detection of oligometastatic disease may lead to local therapies that are potentially curative (16). In our study, PET/CT revealed unsuspected distant metastases in 5% of stage I, 5% of stage IIA, 17% of stage IIB, 31% of stage IIIA, 50% of IIIB, and 50% of stage IIIC patients. Our data suggest that PET/CT identifies clinically unsuspected stage IV disease in 10% of women younger than 40 y with initial clinical stage I and II breast cancers, a population not currently recommended to undergo 18F-FDG PET/CT. As evident from the figures in this article, many of our patients with stage IV disease could be considered oligometastatic (16).
Other studies have reported false-positive distant metastases on PET/CT in 6% of patients (13/225) (15). There were no known false-positive distant metastases in our PET/CT cohort.
Many studies have pointed to the advantage of PET/CT over conventional imaging modalities in detecting extraaxillary regional lymph nodal involvement, including infraclavicular, supraclavicular, and internal mammary nodes (3,13,17–20). Detection of such disease involvement may upstage patients to stage III, impacts prognosis, and may modify the patient’s initial treatment regimen to include, for example, resection of infraclavicular nodes or radiotherapy to extraaxillary nodes (21). In this study, extraaxillary regional metastases were found in 15 (11%) of 134 patients.
Given the high accuracy of physical examination and conventional regional breast imaging modalities (mammography, ultrasound, and MR imaging) for staging of the primary tumor, as well as the high accuracy of sentinel node biopsy for staging of the clinically negative axilla, PET/CT plays a minor role in the assessment of the primary breast cancer and axillary nodal metastases (17,18,20,22). The impact of PET/CT on the primary breast cancer and axillary nodal staging was therefore not the focus of this study.
Some groups have suggested that young age is only a surrogate for an aggressive tumor subtype (23). In our study, no significant difference could be identified in the rate of upstaging between subgroups based on race, tumor grade, or receptor phenotype, although the statistical power for these comparisons was limited.
18F-FDG PET/CT may detect unsuspected synchronous malignancies, unrelated to the known primary (24,25). The 4% rate of total synchronous malignancies and 1% rate of relevant life-threatening synchronous malignancies in this study are slightly lower than in prior reports, likely because of younger patient population in the current study (24,25).
Because of the retrospective nature of the study, we were not able to evaluate the percentage of cases with modifications in clinical management. In a prospective study, Groheux et al. report detection of additional locoregional involved lymph nodes and distant metastases in 7 (18%) of 39 breast cancer patients and a modification of treatment in 5 (71%) of these cases (6). Another prospective study compared PET/CT and ultrasound for regional staging in 60 patients with invasive breast cancers larger than 3 cm or positive lymph nodes (26). All known extraaxillary lymph node metastases in 17 patients were detected by PET/CT, and 10 (17%) were detected only by PET/CT. Detection of 7 of 10 (70%) led to a modification of treatment.
There are several limitations to our study. Selection bias could affect the rate of upstaging after PET/CT. We attempted to minimize selection bias by excluding all patients with prior equivocal findings on conventional imaging, patients with other suspicion for stage IV disease, and patients who had PET/CT performed at outside facilities before presentation to our hospital. In addition, to evaluate whether patients who underwent PET/CT differed systemically from patients who did not undergo PET/CT, we compared our PET/CT cohort with a cohort of patients who did not undergo a staging PET/CT but met all other inclusion criteria. The only statistically significant difference between these 2 groups was initial clinical stage, with patients undergoing PET/CT having higher clinical stages. This difference was expected, as stage is a dominant factor in determining which breast cancer patients are considered for PET/CT evaluation. Other than stage, there were no significant differences in patient characteristics, including, age, race, histology, tumor grade, and receptor phenotype.
Another limitation involves the histologic subtypes in our cohort: 92% of the patients had ductal malignancies. Thus, the applicability of our results to other histologic subtypes is limited.
Finally, whereas all 20 patients who were upstaged because of distant metastases were proven by histopathology, 6 of 8 patients upstaged because of extraaxillary lymph node metastases were not. Strict imaging criteria were used for extraaxillary nodal metastases without histologic proof; thus, we believe the likelihood for falsely upgraded cases is low.
CONCLUSION
Overall 18F-FDG PET/CT revealed stage IV disease in 10% of breast cancer patients younger than 40 y with clinical stage I and II breast cancers. In particular, 17% of women younger than 40 y with stage IIB disease were found to have distant metastases. Although current National Comprehensive Cancer Network breast cancer guidelines recommend against systemic staging with 18F-FDG PET/CT in women with stage II disease and recommend that use of the modality be considered optional for the work-up of stage III breast cancer, our data suggest that women younger than 40 y might benefit from PET/CT staging even at stage IIB. A prospective study, which minimizes selection bias, should verify these findings.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. We acknowledge the Susan G. Komen for the Cure Research grant KG110441 and the MSKCC Biostatistics Core (P30 CA008748) for financial support of this study. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank both Jane Howard and Jonathan Wills for patient database assistance.
Footnotes
Published online Sep. 11, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 17, 2014.
- Accepted for publication July 30, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of 18F-FDG PET/MRI on Therapeutic Management of Women with Newly Diagnosed Breast Cancer: Results from a Prospective Double-Center Trial
- The Current and Future Roles of Precision Oncology in Advanced Breast Cancer
- Overuse of Chest CT in Patients With Stage I and II Breast Cancer: An Opportunity to Increase Guidelines Compliance at an NCCN Member Institution
- Rate of Distant Metastases on 18F-FDG PET/CT at Initial Staging of Breast Cancer: Comparison of Women Younger and Older Than 40 Years
- Initial Results of a Prospective Clinical Trial of 18F-Fluciclovine PET/CT in Newly Diagnosed Invasive Ductal and Invasive Lobular Breast Cancers
- 18F-FDG PET/CT for Staging and Restaging of Breast Cancer
- Comparison of 18F-FDG PET/CT for Systemic Staging of Newly Diagnosed Invasive Lobular Carcinoma Versus Invasive Ductal Carcinoma
- Breast Cancer Staging: To Which Women Should 18F-FDG PET/CT Be Offered?
- Reply: Breast Cancer Staging: To Which Women Should 18F-FDG PET/CT Be Offered?