


Abstract
This article gives an update on nigrostriatal dopamine terminal imaging, with emphasis on SPECT performed with the presynaptic dopamine transporter (DAT) ligand 123I-FP-CIT. The paper covers the rational use of this technique in the diagnostic work-up of patients with known or suspected parkinsonian syndromes. In detail, it addresses the impact of the method for the proof or exclusion of neurodegenerative parkinsonism, for its early and preclinical diagnosis, and for the evaluation of disease progression. The importance of normal DAT binding for differentiating symptomatic parkinsonism and relevant tremor syndromes from neurodegeneration is highlighted. Particularly emphasized is the role of DAT SPECT for diagnosing Lewy body dementia and its separation from Alzheimer dementia. Finally, some remarks deal with the economic aspects of the use of these imaging techniques in the clinical setting.
- single-photon emission computed tomography
- parkinsonian syndromes
- primary and secondary parkinsonism
- tremor syndromes
- dopamine transporter
- Lewy body dementia
Movement disorders are among the most common neurologic illnesses, with the parkinsonian syndromes (PSs) playing a predominant role. PS is a syndromal umbrella term that comprises 4 etiologically different entities: Parkinson disease (idiopathic parkinsonian syndrome, or PD; Parkinson disease with dementia, or PDD), familial PS, atypical PS (PS caused by other neurodegenerative diseases, or aPS), and symptomatic (secondary) parkinsonism, including common differential diagnoses such as specific tremor syndromes. The group of aPS includes multiple-system atrophy (parkinsonian and cerebellar types), progressive supranuclear palsy, corticobasal degeneration, spinocerebellar atrophy, and Lewy body–type dementia (DLB). Vascular, drug-induced, toxic, and metabolic parkinsonism; parkinsonism associated with inflammation, trauma, and tumor; and normal-pressure hydrocephalus belong to the category of secondary parkinsonism. Essential tremor (ET) and other tremor syndromes are further common differential diagnoses additional to PD and aPS.
The diagnosis of PD is primarily based on the well-defined U.K. Parkinson Disease Society Brain Bank clinical diagnostic criteria (1), which also provide pointers to red flags that may indicate other types of parkinsonism. In early stages of PS, however, if clinical findings are subtle, monosymptomatic (e.g., an isolated tremor), or equivocal, it may be difficult to establish the correct diagnosis. Of note, detection of preclinical disease may be even more challenging. Several publications have addressed the issue of potential clinical misdiagnosis from different points of view, including clinical and postmortem studies (1–5). Nuclear imaging may help to establish a correct diagnosis in many clinically unclear cases, thus informing about the prognosis of the respective disease quite early and guiding toward suitable therapies.
Conventional CT and MR imaging techniques contribute little to the early diagnosis of PS, because in many instances structural abnormalities are present only in more advanced disease or may be difficult to assess in individual subjects. Advanced techniques such as MR volumetry, proton MR spectroscopy, diffusion tensor and diffusion-weighted imaging, relaxometry, neuromelanin imaging, and magnetization transfer may further assist in the differential diagnosis, but they require further validation and are not routine applications yet (6–10).
In contrast, molecular imaging with nuclear medicine techniques addresses key functions of dopaminergic neurotransmission, alterations of which are involved in almost all neurodegenerative PSs, as is well known from experimental, animal, clinical, and postmortem studies.
The basic principles of dopaminergic neurotransmission are well known. Briefly, nigrostriatal and—to a lesser extent—mesostriatal dopaminergic nerve fibers end in the caudate and putamen, where the presynaptic dopaminergic terminals communicate with the postsynaptic dopamine receptors. Nigrostriatal fibers originate in the pars compacta of the substantia nigra. In addition, the ventral tegmental area in the mesencephalon provides not only mesolimbic and mesocortical frontal projections but also mesostriatal dopaminergic projections that include the ventral putamen and the anteroventral striatum. Through the use of specific ligands, SPECT and PET techniques allow evaluation of the integrity, number, and density of presynaptic dopaminergic terminals and postsynaptic dopamine receptors (11,12).
Presynaptic nigrostriatal neuron integrity can be assessed with radioligands suitable for imaging 3 different key functions. First, PET with fluorodopa reflects the aromatic amino acid decarboxylase activity and dopamine storage capacity (11,13). Second, the target region for ligands such as dihydrotetrabenazine is the vesicular monoamine transporter type 2 (14,15). Last, cocaine derivatives and noncocaine derivatives bind with high affinity and sufficient selectivity to the plasma membrane dopamine transporter (DAT), which is located at the presynaptic nerve terminals (11,12). DAT is responsible for reuptake of dopamine from the synaptic cleft; thus, DAT investigations allow in vivo assessment of the integrity of presynaptic nerve terminals. For this purpose, noncocaine derivatives such as methylphenidate and numerous cocaine analogs have been used. Among the latter, in particular use have been the 123I-radiolabeled ligands 2β-carbomethoxy-3β-(4-iodophenyl)tropane (β-CIT), N-(3-iodopropen-2-yl)-2β-carbomethoxy-3β-(4-chlorophenyl)tropane (IPT), N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane (FP-CIT), Altropane, N-(3-iodopro-2E-enyl)-2β-carbomethoxy-3β-(4′-methylphenyl)nortropane (PE2I), and 99mTc-labeled [2-[[2-[[[3-(4-chloropheny)-8-methyl-8-azabicyclo[3.2.1]oct-2-yl]-methyl](2-mercaptoethyl) amino] ethyl] amino]ethane-thiolato(3-)-N2,N2′, S2,S2′]oxo-[1 R-(exo-exo)] (TRODAT-1). Of predominant clinical importance is 123I-FP-CIT (DaTscan), which has been licensed for more than 12 y in Europe and for about 2 y in the United States. At the postsynaptic level, the status of the dopamine D1-like receptors (D1, D5) and the D2-like receptors (D2, D3, and D4) may also be addressed with suitable SPECT and PET ligands (11).
Because of the approval of 123I-FP-CIT by regulatory authorities and thus its widespread availability, this contribution mainly focuses on the use of 123I-FP-CIT and SPECT for the assessment of presynaptic nigrostriatal imaging. The main topic is the clinical application of this technique in the diagnostic work-up of patients with PS. Technical aspects of imaging such as the appropriate use of imaging devices, optimization of acquisition and processing parameters, and suggestions for further data analyses including quantification are not extensively covered in this paper, as they are dealt with in procedural guidelines published by the European Association of Nuclear Medicine (16) and the Society of Nuclear Medicine and Molecular Imaging (17).
PROOF OF NEURODEGENERATIVE PS
Imaging of presynaptic nigrostriatal neuron integrity delivers crucial evidence about whether a patient has neurodegenerative parkinsonism (PD or aPS). The predominant pathology in PD, which accounts for about 70%–80% of PS, is loss of the dopaminergic neurons that project mainly from the substantia nigra pars compacta in the midbrain to the striatum (putamen and caudate nucleus). Typically, the projections to the posterior putamen are earlier and more affected than those to the anterior putamen and caudate. Imaging of presynaptic neuron integrity, therefore, reveals reduced radioligand uptake in the striatum of PD patients, which is often already evident by visual reading. The reduced uptake advances from the posterior to the anterior putamen and finally the caudate. Thus, the posterior putamen is the most- and earliest-affected structure. Frequently, particularly in the early stages of disease, a marked asymmetry of striatal binding is evident, with a more pronounced loss in the striatum contralateral to the clinically more affected limbs (18). This pattern has been reported not only in sporadic PD but also in juvenile, young-onset parkinsonism and patients with parkin gene mutations. Whereas the latter notions were derived mainly from PET investigations, similar observations would have been obtained by the use of DAT SPECT ligands (19–21).
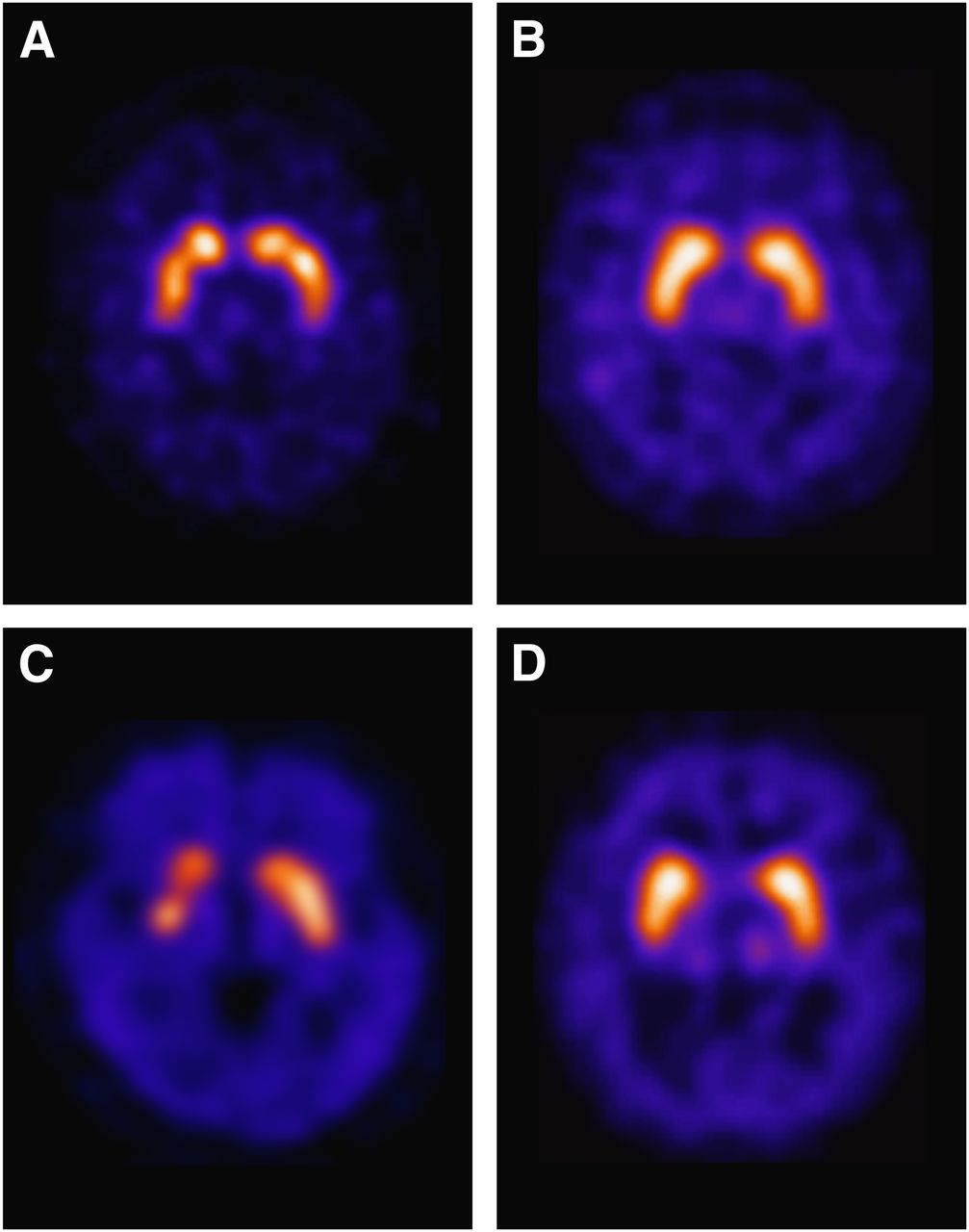
There is histopathologic evidence for a correlation between the extent of compromised DAT binding and the numeric loss of nigrostriatal nerve terminals (12). Similar to the findings observed in PD, in the various forms of aPS marked loss of striatal DAT binding is also present, whereas in aPS asymmetry often may be less exaggerated and the binding gradient from the posterior putamen to the caudate less prominent. Examples of DAT imaging in the various neurodegenerative PSs are shown in Fig. 1. If the presynaptic neuron integrity is compromised in the described pattern, the diagnostic sensitivity for neurodegenerative PS was at least 95% (22).

Representative examples of patients with neurodegenerative parkinsonian syndromes: PD (A), multiple-system atrophy (B), progressive supranuclear palsy (C), and dementia with DLB (D). Each case shows marked pathologic reduction of striatal 123I-FP-CIT binding representing loss of presynaptic neuron integrity in these disorders. In all cases, predominant involvement of putamen is seen, and extent of reduced binding advances from posterior to anterior putamen and finally caudate. Somewhat accentuated striatal asymmetry is evident. Reliable distinction between different entities (PD vs. various shown forms of aPS) based on DAT imaging is not possible (39,40).
Early Diagnosis of Neurodegenerative PS
Imaging studies with DAT ligands of patients with early PD and in particular those with hemi-PD (Hoehn and Yahr stage I) have concordantly reported a bilateral deficit in presynaptic functions. Notably, reduced binding was observed not only in the striatum, and especially the putamen, corresponding to the symptomatic limbs but also already in the contralateral putamen associated with the clinically still yet asymptomatic side of the body (23–25). The reported binding values were significantly lowered compared with those of age-matched healthy controls and showed no or almost no overlap between patients and controls. On the basis of these findings, it was concluded that DAT SPECT examinations are not only a sensitive tool for the early diagnosis of PD but might be sensitive enough to depict even preclinical or premotor disease in neurodegenerative PS.
The capability of imaging presynaptic neuron integrity to depict preclinical and premotor disease is further supported by the notion that clinical (mainly motor) symptoms appear earliest after 50% or more of the nigrostriatal neurons have been lost (26) and by pathologic imaging results for asymptomatic twins and for familial PD, parkin, and other inherited-PD kindreds (19,27–30).
SWEDDS
In the past, a small, specific entity of patients with clinically distinct symptoms of PD revealed completely normal imaging results of presynaptic functions. Today, the pathology of these so-called SWEDD patients (scan without evidence of dopaminergic deficit) is still unclear. SWEDD patients have been identified in several clinical PD trials (Comparison of the Agonist Pramipexole vs. Levodopa on Motor Complications in Parkinson Disease; Earlier versus Later Levodopa Therapy in Parkinson Disease; and Requip as Early Therapy vs L-dopa–PET) and were present in about 11% of the subjects overall (45 of 410 patients included in the mentioned trials). Basically, this rate is consistent with the reported portion of misdiagnosis of early PD by movement disorder specialists. Dystonic tremor has been identified as one possible cause of SWEDD (31). Thus, one conclusion might be that SWEDD subjects are simply incorrectly diagnosed and do not have neurodegenerative PS. Others speculate that SWEDD reflects a different, so far not clearly identified and understood, category of neurodegenerative PS that is not characterized by the typical presynaptic nigrostriatal dopaminergic deficit. To date, there is agreement that SWEDD subjects behave differently from classic-PD subjects in several aspects. They feature no compromised presynaptic function over years, no progressive decline of presynaptic functions, a lack of a clear positive response to dopaminergic medication (an exception may be some patients with dopa-responsive dystonic tremor), and no patterns of glucose metabolism compatible with classic PD. The prognosis of SWEED subjects is considered to be more favorable than that for classic neurodegenerative PS (32–36). To the best of our knowledge, histopathologic proof of SWEDD pathology is still lacking; for further clarification, such studies are clearly needed.
Assessment of Disease Progression
Cross-sectional studies have reported significant correlations between disease severity/disability stage and the extent of reduced presynaptic terminal measures assessed by DAT imaging (12,25,37). Furthermore, longitudinal imaging studies have proven capable of determining intraindividual disease progression (24,38). Concordantly, in those studies the annual rate of decline of DAT binding ranged from 6% to 8%. This range applies primarily to PD patients in the early stages of disease, whereas the annual decline in late stage of disease is markedly lower. For example, in a group of PD patients who were symptomatic for longer than 9 y, an annual decline of DAT binding of only 2.4% was reported. In parallel to the more rapid clinical course of aPS, a significantly faster progression was observed for aPS (mean annual decline of 14.9% at a symptom duration of about 2.1 y) than for PD (mean annual decline of 7.1% at a comparable symptom duration of about 2.4 y) (38).
Differential Diagnosis Between Neurodegenerative Types of PS
Unfortunately, presynaptic imaging plays only a minor role in the differentiation of PD from aPS and in the further discrimination of the different aPS entities (e.g., multiple-system atrophy vs. progressive supranuclear palsy vs. corticobasal degeneration) (18,37,39). Most authors state that, in individual cases, DAT imaging does not allow for reliable discrimination of a PD subject from an aPS subject or for further discrimination of the latter (Fig. 1) (39,40). Favorable nuclear medicine imaging techniques for this purpose would be assessment of either postsynaptic D2-like receptors or assessment of brain glucose metabolism (41–44).
PROOF OF SYMPTOMATIC PARKINSONISM
If presynaptic DAT binding is normal, the presence of neurodegenerative PS is highly unlikely. The main differential diagnoses are then either symptomatic PS or various tremor diseases that might, for example, clinically mimic a monosymptomatic neurodegenerative PS. Thus, the comprehensive appraisal of presynaptic DAT imaging is focused on the question of whether symptoms in a patient might be related to neurodegeneration. This question is frequently the diagnostic challenge for the neurologist in the clinical setting, as studies have indicated that a disease—particular in its early stage—that is not associated with neurodegeneration, such as the various tremor syndromes (including ET); drug-induced, psychogenic, and vascular PS; or even Alzheimer dementia, may be misdiagnosed as a neurodegenerative PS (32,45,46).
Some representative examples of DAT imaging in patients with symptomatic PS and tremor syndromes are shown in Fig. 2. Because of their normal DAT findings in general, all these entities are easily distinguishable from the neurodegenerative types of parkinsonism (PD and aPS). Unfortunately, however, further reliable distinction between the different symptomatic PS or tremor syndromes based on their normal or only minor compromised 123I-FP-CIT findings alone is not possible. For this purpose, further clinical information and in some instances morphologic imaging results (e.g., in normal-pressure hydrocephalus or vascular PS) are needed.
Tremor Syndromes
By now, many studies have addressed the role of presynaptic DAT imaging for the differential diagnosis of tremor syndromes versus neurodegenerative PS.
ET
ET is considered the most frequent form of pathologic tremor. ET may start in adolescence or later in life (also in the elderly), and in more than half the patients a genetic etiology with autosomal-dominant inheritance is discussed. Clinically, the predominant feature of ET is a bilateral, mostly symmetric, kinetic tremor. Other types of tremor such as intentional tremor or—rarer—resting tremor may also be present. Frequently affected are the hands and the arms; however, the ET may also occur in the head and neck, the jaw, the voice, or other body regions such as the legs. Differential diagnosis of ET versus monosymptomatic (tremor-dominant) neurodegenerative PS may be difficult, thus emphasizing the role of DAT SPECT investigations for this purpose. Clinically, these syndromes can sometimes even occur together in the same patient, and this overlap syndrome may require both anti-ET and anti-PD treatment. About a decade ago, the topic of the differential diagnosis between ET and neurodegenerative PS was addressed in a European multicentric clinical trial that finally led to the regulatory approval of 123I-FP-CIT in Europe (22). This study, on a population of 158 clinically diagnosed PS patients, 27 patients with ET, and 35 healthy controls, found a sensitivity and specificity of 97% and 100%, respectively, for discriminating PS from ET. Findings in patients with ET were not different from those in controls and thus were easily distinguishable from those in neurodegenerative PS. These basic observations have been replicated and confirmed by several further studies, including more recent ones. The latter have reported on longer clinical follow-up periods of up to 3 y (47) and have focused on the same basic topic from other perspectives—for example, by including SWEDD and dystonic tremor patients in the population of tremor patients (35) and by assessing DAT binding semiquantitatively in ET versus healthy subjects and patients with hemiparkinsonism (48).
Other Tremor Syndromes
Orthostatic tremor is a rare syndrome that is characterized by unsteadiness in standing caused by a high-frequency tremor of the legs. Even though orthostatic tremor usually manifests during standing, it may more rarely occur during walking. Involvement of other body regions such as the face, hands, and trunk is frequent. Most cases of orthostatic tremor are considered idiopathic, related to orthostatic tremor with PD, or related to degeneration of the dopaminergic system. SPECT studies with 123I-FP-CIT have always reported either normal findings in orthostatic tremor patients (49,50) or only slightly reduced striatal DAT-binding values, which, however, still allowed highly reliable differentiation of orthostatic tremor from PD (51). The isolated action tremor is a characteristic symptom of ET but may also be observed in individuals with PD. Published data on this entity suggest that 123I-FP-CIT SPECT investigations are helpful for correctly assigning patients with isolated action tremor either in the ET category (normal DAT binding) or the PD category (reduced DAT binding) (52). According to reports in the literature, patients with psychogenic tremor also present with normal DAT binding (18).
Vascular PS
In the classic type of vascular parkinsonism, the predominant finding is a gait disorder characterized by shuffling short steps. For this reason, the disease is also referred to as a lower-body parkinsonism. Rigidity may be present, whereas tremor is a less common symptom. Hypomimia, swallowing problems, cognitive deficits, and incontinence of urine and feces are further clinical findings. As compared with PD, symptoms in vascular PS usually show no or only a minor response to antiparkinsonian drugs (53). Reports on DAT binding in vascular PS provide heterogeneous results, which might indicate that vascular PS is a mixed entity that is not yet well characterized (40). Some authors have reported normal or only a slight but insignificant reduction of DAT binding in patients with suspected vascular PS (45,54,55); others have found significantly reduced binding values (56,57). This discrepancy may be attributed to differences in patient populations and the relatively small numbers of subjects investigated. There is consent that DAT binding is reduced in striatal subregions directly affected by infarction, as demonstrated by structural defects in corresponding CT and MR imaging examinations (a “punched-out” striatum, a subgroup of patients with an acute start of symptoms and a close timing between the symptoms and the event). Usually, these findings can be clearly distinguished from those in neurodegenerative PS. Review of anatomic imaging, therefore, is highly recommended to best interpret DAT imaging results in patients with vascular PS. On the other hand, Zijlmans et al. suggested another course of vascular PS—one characterized by a slow, insidious onset of symptoms in known small-vessel disease of the brain and associated with pathologic DAT binding (56). Lorberboym et al. used DAT SPECT to investigate 20 patients with cerebrovascular disease (lacunar infarcts and territorial infarcts) who developed clinical symptoms of vascular PS (57). The investigators observed that the 9 patients with normal DAT binding showed a poor response to dopaminergic medication whereas 5 of 11 subjects with diminished binding showed a good response. Therefore, it was suggested that DAT imaging not only may indicate the presence or absence of nigrostriatal degeneration in vascular PS but also may be helpful to define a subset of patients who might respond to dopaminergic medication. Contrafotto et al. analyzed the striatal asymmetry index of DAT binding in patients with vascular PS, PD, and ET. On observing that the index was significantly lower in vascular PS than in PD subjects, the authors suggested that this parameter may be used for differentiating vascular PS from PD with a good degree of certainty (58).
Drug-Induced PS
During treatment with neuroleptic drugs, parkinsonian symptoms attributable to the blockade of postsynaptic dopamine receptors may develop. The extent of the occupation and blockade of these receptors may largely differ and depends on the respective drug category. Typical neuroleptics such as haloperidol, for example, lead to an extensive receptor blockade even in relatively low-dose treatments; thus, the threshold for causing extrapyramidal side effects and herewith parkinsonian symptoms is rather low. In atypical neuroleptics, this threshold is markedly higher; however, in this class of drugs dopamine receptors are also occupied to some degree and therefore extrapyramidal symptoms may also occur. According to information from the Parkinson Disease Society, in about 7% of patients with parkinsonism the symptoms develop after treatment with drugs. Reports on SPECT investigations with 123I-FP-CIT have confirmed that patients with drug-induced PS present with normal DAT binding and thus can be reliably distinguished from those with neurodegenerative PS. Apart from the main distinction between drug-induced PS and primary neurodegenerative PS, patients may also present with a drug-exacerbated parkinsonism in which parkinsonian symptoms become manifest upon exposure to the offending drugs but do not completely resolve once they are discontinued. Such a drug-exacerbated parkinsonism may represent patients at a prodromal state of PD who do not tolerate the offending medication. Furthermore, it has concordantly been reported that in patients suspected of having drug-induced PS who, however, presented with pathologic DAT binding, either neurodegenerative PS alone or a combination of neurodegenerative and drug-induced PS was finally determined to be present (45,59–61).
Psychogenic PS
As expected, patients with psychogenic PS present with normal striatal DAT binding of 123I-FP-CIT. Booij et al. determined, in a series of 31 patients with inconclusive symptoms of parkinsonism, that psychogenic PS was present in 4 patients, all of whom had normal DAT binding (45). In another series, of 9 patients with suspected psychogenic PS, normal DAT binding was found in 8 (62). Interestingly, in the one patient presenting with reduced DAT binding, a parkin gene mutation was detected, suggesting that the DAT scan did correctly point to the presence of neurodegenerative PS (62).
Normal-Pressure Hydrocephalus
Normal-pressure hydrocephalus is clinically characterized by the classic symptom triad of gait disturbance, urinary incontinence, and dementia or cognitive decline. The gait disturbance, which is most often the first symptom, is typically called gait apraxia and has been described as a “glued” or “magnetic” gait. Persons with this gait disturbance, even though clinically distinct from the typical parkinsonian shuffling gait, may be misdiagnosed as having PD instead of normal-pressure hydrocephalus. CT and MR imaging scans typically show enlarged ventricles and signs of atrophy. Because neurodegeneration of presynaptic nigrostriatal nerves is absent in normal-pressure hydrocephalus, patients with this disease present with normal DAT binding values and thus can be easily differentiated from patients with neurodegenerative PS (63).
Dopa-Responsive Dystonia (DRD)
DRD is, like juvenile parkinsonism, a hereditary disease with onset at younger ages. Clinically, DRD presents with a dystonic gait disorder, with slowness of movements, instability, and occasionally tremor, which in some stages may resemble PD. The disease responds well to dopaminergic medication and, in contrast to juvenile parkinsonism, presents with normal striatal DAT binding (64,65). Therefore, for example, if the patient history is unclear, 123I-FP-CIT SPECT examinations may help to differentiate between DRD and juvenile parkinsonism.

Representative examples of patients with tremor syndromes and symptomatic parkinsonism: ET (A), drug-induced parkinsonism (B), vascular parkinsonism (C), and normal-pressure hydrocephalus (D). Each case shows normal preserved striatal 123I-FP-CIT binding. Vascular PS case reveals small striatal defect in right anterior putamen corresponding to infarction at this location and slightly reduced binding in caudate compared with putamen, but pattern is clearly different from cases with neurodegeneration. Case with normal-pressure hydrocephalus shows, apart from normal DAT binding, marked enlargement of ventricles that increases the distance between striata. All these entities are easily distinguishable from the various forms of neurodegenerative PS shown in Fig. 1.
DIFFERENTIAL DIAGNOSIS OF DLB
Among the neurodegenerative dementias, DLB seems to be much more frequent than supposed in the past and today is thought to account for up to 30% of dementia cases. Differentiation of DLB from other dementias solely on the basis of clinical symptoms is often difficult. However, differentiation is important for therapeutic management because a considerable number of DLB patients respond well to cholinesterase inhibitors and many patients are highly sensitive to neuroleptic drugs and develop severe extrapyramidal side effects (66).
Because of the close pathologic and clinical relationship between PD and DLB, similarities with respect to the effect on the dopaminergic pathway can be expected. In particular, between PDD and DLB some overlap may occur because the clinical distinction between them is somewhat arbitrarily based on the “one-year rule” that in PDD, the onset of dementia is at least 1 y behind the presentation of motor symptoms whereas in DLB, cognitive and motor impairment are concordantly present. Autoradiographic studies on DLB postmortem tissue have indeed demonstrated a remarkable loss of presynaptic dopaminergic ligand binding in the striatum (67). Single-center studies (68,69) and a large-scale multicenter study (4) have shown that this loss of presynaptic binding also excellently separates in vivo DLB subjects from Alzheimer dementia subjects. Similar to PD and aPS, DLB is also characterized by a marked loss of DAT binding, which is often already evident by visual reading of the images (Fig. 1). Therefore, pathologic striatal DAT binding assessed by visual and quantitative analysis allows for a reliable differentiation of DLB from Alzheimer dementia, with the latter being the most important differential diagnosis. Alzheimer dementia patients usually present with mostly preserved, not significantly reduced, DAT binding (with a preserved putamen-to-caudate ratio), compared with healthy controls. Studies concordantly report sensitivities of 80% and specificities of 90%–94% for the differential diagnosis of DLB from Alzheimer dementia (4,68,69). A recent metaanalysis of 4 studies including a total of 419 patients reported a pooled sensitivity of 86.5% and a specificity of 93.6% for the differentiation of DLB from non-DLB using 123I-FP-CIT (70). Interestingly, abnormal scan findings also seem helpful for correctly assigning patients with an unclear diagnosis (“possible DLB”) into the “probable-DLB” group (71). Even more convincing is the high correlation between findings of 123I-FP-CIT examinations in vivo and the corresponding results at autopsy. In such a comparative series of 20 patients, DAT imaging showed a sensitivity of 88% (7/8) and a respective specificity of 100% (12/12), whereas comparing the clinical diagnosis with autopsy results revealed a sensitivity and specificity of only 75% and 45%, respectively (72). The convincing data led to the inclusion of imaging results in the consensus diagnostic criteria for establishing the diagnosis of DLB. A recent review stated that pathologic DAT binding in 123I-FP-CIT SPECT currently appears to be the most reliable and valid biomarker for differential diagnosis of DLB from Alzheimer dementia, even though other imaging modalities such as assessment of cardiac 123I MIBG uptake in SPECT, occipital hypometabolism on 18F-FDG PET, and preservation of medial temporal lobe structures on MR imaging show similar benefits (73). Differentiating DLB from frontotemporal dementia on the basis of DAT imaging may be less distinct. In a recent study, one third of the patients with frontotemporal dementia (4/12) presented with reduced DAT binding (74). Further studies are needed to determine whether nigrostriatal loss in frontotemporal dementia is quantitatively distinct from DLB and PDD.
SELECTED METHODOLOGIC CONSIDERATIONS
As outlined earlier, it was not the aim of this article to provide detailed technical information on performing and processing FP-CIT SPECT investigations. Instructions on preparing patients, handling the radiopharmaceutical, setting up the camera system to obtain sufficient counting rate statistics, obtaining an adequate pixel size, choosing the reconstruction procedure and filter, and so forth may be derived from published procedure guidelines (16,17). Apart from these issues, users frequently ask for more detailed information about the need and role for image quantification and about whether medication may interfere with the imaging results.
In the past, clinical diagnostic judgments were often based on purely visual interpretation of scans and showed high sensitivities and specificities regarding the key question of whether presynaptic neuron integrity was disturbed (mostly a “yes” or “no” answer). In those quite easily interpretable cases, semiquantification often just confirmed the visual impression. A specific added diagnostic value of quantification was attributed to the analyses of borderline and inconclusive cases (e.g., unclear asymmetry, homogeneous reduction of striatal binding, and borderline putamen–caudate gradient) and follow-up studies. In the past, poor standardization and lack of general availability of more specific software tools for semiquantification, in conjunction with lack of an accessible large-scale reference database, undervalued the role of quantification. Even though single centers were highly experienced with their own methodology, such issues as sharing of reference values between centers or data pooling were problematic. With the recent availability of a large-scale reference database allowing age-related reference values to be defined and implemented in commercial software products that follow standardized quantification procedures, the historic drawbacks are expected to be overcome and the appropriate value of semiquantification reassessed (75). Currently, comparative studies are under way to fully define the role of these procedures.
With respect to possible interference of medication with DAT SPECT findings, detailed information is given in a review article by Booij and Kemp (76). They recommend withdrawal of drugs (including drugs of abuse) preferably 5 plasma half-lives (if acceptable on clinical grounds) before FP-CIT scanning to rule out a remarkable influence on visual and quantitative analyses. Such drugs include cocaine, amphetamines, methylphenidate, phentermine and ephedrine, modafinil, some antidepressants (bupropion, radafaxine, mazindol), and anticholinergics (benzatropine). Selective serotonin reuptake inhibitors and selective serotonin–norepinephrine reuptake inhibitors will increase striatal binding ratios, but the authors do not generally recommend their withdrawal because the effect was considered too small to cause misinterpretation of an individual scan (effects only around 10%). Because even small differences may be relevant in scientific studies, in this setting withdrawal of all kind of drugs that may influence DAT binding is preferable.
ECONOMIC CONSIDERATIONS
The diagnostic impact of presynaptic nigrostriatal DA imaging has been extensively highlighted in this article, but the economic role of implementing such modalities in distinct diagnostic pathways also requires attention. Several studies have indicated that diagnoses of PS established on clinical grounds are associated with uncertainties and that the results of DAT imaging can influence therapeutic management. For example, it has been shown that a considerable number of patients have been treated with dopaminergic medication in the absence of a neurodegenerative PS and, vice versa, that some patients have not received adequate medication because their neurodegenerative PS was not recognized (2,77,78). Apart from the consequence for the individual patient, such types of data ask for economic evaluations (79,80). Some studies have already focused on this issue. For example, an Italian study reported an overall decrease of costs for the health care system by implementing 123I-FP-CIT SPECT for differential diagnosis of ET versus IPS, as compared with the conventional diagnostic pathway based on clinical judgment alone (81). Other recent prospective multicentric studies have looked at the impact of 123I-FP-CIT SPECT on clinically uncertain PS and demonstrated that for the subgroup of patients who underwent the scanning procedure, medication was changed at a significantly earlier time point and there was significantly greater confidence in the diagnosis 4 wk, 12 wk, and 1 y after the initial diagnosis. Inclusion of imaging, therefore, has had a significant impact on clinical management, diagnosis, and diagnostic confidence in a patient population with uncertain PS (82).
CONCLUSION
In patients with PS, the establishment of a correct diagnosis has a significant impact on the therapeutic strategy and determines the individual prognosis of the diseased subject. Today, imaging of presynaptic nigrostriatal neuron integrity is a firmly established method of proving or excluding neurodegenerative PS. Preserved presynaptic DAT binding is indicative of symptomatic PS (vascular, drug-induced, or psychogenic), normal-pressure hydrocephalus, or tremor syndromes such as ET. If presynaptic DAT binding is compromised, the presence of a neurodegenerative PS is proven. The differential diagnoses then comprise PD and the various forms of aPS (e.g., multiple-system atrophy, progressive supranuclear palsy, or corticobasal degeneration). Further differentiation between these entities based on presynaptic imaging alone is not reliable. For this purpose, apart from clinical findings, further modalities such as postsynaptic dopamine receptor imaging or assessment of glucose metabolism may be required. Presynaptic nigrostriatal imaging plays an increasing role in the differential diagnosis of neurodegenerative dementias, because with these techniques DLB can be diagnosed with high reliability and distinguished from Alzheimer dementia. Some newer reports also address the economic aspects of the use of these imaging modalities by showing their cost-effective implementation for diagnostic pathways in various clinical settings.
Footnotes
Published online Jul. 17, 2013.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the radiopharmaceuticals used to evaluate nigrostriatal dopamine imaging; (2) the pattern of uptake of these radiopharmaceuticals in parkinsonian syndromes; and (3) the role of these radiopharmaceuticals in the evaluation of parkinsonian syndromes.
Financial Disclosure: Dr. Tatsch is a meeting participant/lecturer for GE Healthcare. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, participants can access this activity through the SNMMI Web site (http://www.snmmi.org/ce_online) through August 2016.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.↵
- 7.
- 8.
- 9.
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.
- 30.↵
- 31.↵
- 32.↵
- 33.
- 34.
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.
- 43.
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- Received for publication May 10, 2013.
- Accepted for publication June 24, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pearls & Oy-sters: Idiopathic Normal Pressure Hydrocephalus With Synucleinopathy: Diagnosis and Treatment
- Determining the Degree of Dopaminergic Denervation Based on the Loss of Nigral Hyperintensity on SMWI in Parkinsonism
- A dominant-negative variant in the dopamine transporter PDZ-binding motif is linked to parkinsonism and neuropsychiatric disease
- Optimization of Parameters for Quantitative Analysis of 123I-Ioflupane SPECT Images for Monitoring Progression of Parkinson Disease
- Impairment of cross-modality of vision and olfaction in Parkinson disease
- Diagnostic Performance of the Visual Reading of 123I-Ioflupane SPECT Images With or Without Quantification in Patients With Movement Disorders or Dementia
- Is ioflupane I123 injection diagnostically effective in patients with movement disorders and dementia? Pooled analysis of four clinical trials