


Abstract
Myelosuppression may be the dose-limiting toxicity in peptide receptor radionuclide therapy (PRRT). The aim of this study was to investigate the incidence, severity, and reversibility of long-term hematotoxicity in a large cohort of patient undergoing PRRT with 177Lu-octreotate for metastatic neuroendocrine tumors. The impact of potential risk factors, including initial cytopenia, advanced bone metastatic disease, previous chemotherapy, and cumulative administered activity, and the protective effects of splenectomy were of particular interest. Methods: A total of 632 PRRT courses were performed in 203 patients with metastatic neuroendocrine tumors. A mean activity of 7.9 GBq of 177Lu-octreotate was administered per treatment cycle, with a goal of 4 courses at standard intervals of 3 mo. Hematologic parameters were determined before each treatment course, at 2- to 4-wk intervals between the courses, 8–12 wk after the last course of PRRT, and at 3-month intervals for further follow-up. Toxicity was recorded with Common Terminology Criteria for Adverse Events (version 3.0). Results: Myelodysplastic syndrome as a delayed adverse event was documented in 3 patients (1.4%). Relevant but reversible hematotoxicity (grade 3 or 4) occurred in 23 patients (11.3%) and 29 administrations (4.6%), with leukopenia in 2.7% and thrombocytopenia in 1.7%. The mean time to blood count recovery was 12 mo after the termination of PRRT (range, 3–22 mo). The only preexisting factor that contributed to hematotoxicity was initial cytopenia (P < 0.001). A high level of cumulative administered activity (>29.6 GBq) was associated with relevant leukopenia (P < 0.001). None of the patients with a history of splenectomy developed grade 3 or 4 hematotoxicity, and splenectomy was inversely associated with the incidence and degree of leukopenia (P = 0.02) and thrombocytopenia (P = 0.03) Conclusion: PRRT-induced myelosuppression is almost invariably reversible and rarely requires clinical measures. Administered activity and initial cytopenia are the only factors contributing to myelosuppression, whereas splenectomy may exert a protective effect.
Peptide receptor radionuclide therapy (PRRT) with radiolabeled somatostatin analogs is a highly effective systemic treatment in patients with metastatic gastroenteropancreatic neuroendocrine tumors (NETs) (1–9). Bone marrow suppression is regarded as one of the most serious side effects after PRRT (10–13). Because of the lower energy and the shorter tissue penetration of the emitted β particles, treatment with 177Lu-labeled peptides may result in a lower level of overall toxicity than PRRT with 90Y-labeled peptides (14). However, there are only limited data regarding hematotoxicity after PRRT with 177Lu-octreotate and contributing risk factors (2,15,16).
The aim of this retrospective study was to investigate the incidence, severity, and reversibility of myelosuppression in a large cohort of patients with metastatic gastroenteropancreatic NETs treated with 177Lu-octreotate. The impact of potential risk factors, including the presence of advanced bone metastatic disease, previous chemotherapy, and cumulative administered activity, was of particular interest. The protective impact of splenectomy on the development of hematotoxicity was also explored.
MATERIALS AND METHODS
A total of 203 consecutive patients treated with 177Lu-octreotate at the Department of Nuclear Medicine in Bonn (93 men and 110 women; age range, 34–89 y; mean age, 63 y) were included in the retrospective analysis. PRRT has been part of standard care in Germany for several years (17). Inclusion criteria for treatment with PRRT were histologically confirmed, unresectable, metastatic NET; sufficient tumor uptake, that is, uptake greater than or equal to that of the liver on baseline receptor imaging; a glomerular filtration rate of greater than 30 mL/min/1.73 m2; a white blood cell count of greater than or equal to 2,000/mm3; a hemoglobin level of greater than or equal to 8 g/dL; and a platelet level of greater than or equal to 75,000/mm3. A mild reduction in blood counts at baseline was not an exclusion criterion. Seventy-two patients had pancreatic NETs, and 131 patients had nonpancreatic gastroenteropancreatic NETs. All patients showed tumor progression before treatment with 177Lu-octreotate. The study was performed in accordance with the Declaration of Helsinki and with national regulations. The local committee on ethics approved this retrospective study, and all patients signed written informed consent.
PRRT
PRRT was performed with a mean of 7.9 GBq (216 mCi) of 177Lu-octreotate per treatment cycle, with the goal of 4 courses at standard intervals of 3 mo (10–14 wk). 177Lu (IDB Holland) had a specific activity in the approximate range of 100–160 GBq/μmol at the time of administration. Peptide labeling (18,19) was performed such that an apparent specific activity of about 54 GBq/μmol (ratio of activity to the total amount of peptide) was obtained. Nephroprotection was implemented with standard amino acid coinfusion according to the Rotterdam protocol (15,20) (2.5% lysine and 2.5% arginine in 1 L of 0.9% NaCl; rate of infusion, 250 mL/h). Hematologic parameters were determined before each treatment course, at 2- to 4-wk intervals between the courses, 8–12 wk after the last course of PRRT, and at 3-month intervals for further follow-up. Toxicity was recorded with the Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
Statistical Analysis
The association of treatment-induced myelosuppression (grades 1–4) with the baseline characteristics of the study population and the cumulative administered activity was examined by applying nonparametric tests for independent samples as well as multiple regression analysis. The potential protective effect of splenectomy on the development and degree of hematotoxicity was investigated both in the whole patient cohort and in the subgroup of patients with pancreatic NETs. The statistical software package SPSS (version 18.0; SPSS Inc.) was used to analyze the data.
RESULTS
A total of 632 PRRT courses were performed in 203 patients (median, 3 treatment courses per patient; cumulative administered activity, 4.9–37.8 GBq). In 47 patients, treatment was stopped after 1 (n = 18) or 2 (n = 29) cycles because of documented disease progression. The median follow-up period was 31 mo (95% confidence interval, 20–71) from the start of PRRT. At the start of treatment, 14 patients had leukopenia (11 grade 1 and 3 grade 2), 37 patients had thrombocytopenia (36 grade 1 and 1 grade 2), and 69 patients had anemia (60 grade 1, 8 grade 2, and 1 grade 3), according to the CTCAE criteria. One patient received PRRT despite having grade 3 anemia at baseline because of the lack of treatment alternatives and progressing tumor disease.
Relevant hematotoxicity (grade 3 or 4) occurred 2–8 wk after 29 administrations (4.6%) or, expressed per patient, after at least 1 of the administrations in 23 patients (11.3%). Seventeen patients showed a disturbance of only 1 hematologic cell line (leukopenia, 9; thrombocytopenia, 5; anemia, 3), whereas 6 patients showed a significant reduction in 2 or all 3 investigated parameters. The most frequently observed adverse event was leukopenia, occurring after 17 administrations (2.7%); thrombocytopenia occurred after 11 administrations (1.7%), and anemia occurred after 7 administrations (1.1%) (Table 1).
Prevalence of Examined Factors and Percentage of Patients Developing Significant Toxicity
In 8 patients and after 13 administrations, significant bone marrow impairment spontaneously resolved before the next scheduled treatment course. Two patients required blood transfusion during 1 of their hospital stays, and 2 treatment cycles for 1 patient were postponed for 3–4 wk to allow bone marrow recovery. PRRT was discontinued in only 1 patient because of aggravated preexisting anemia after the first cycle. This patient had a history of 6 cycles of cisplatin–etoposide until 5 mo before treatment. However, subsequent chemotherapy with 5-fluorouracil–streptozocin was applied 2 mo later and was well tolerated, with no dose-limiting myelosuppression. In 10 patients, relevant myelosuppression was first observed after the completion of the last intended therapy cycle.
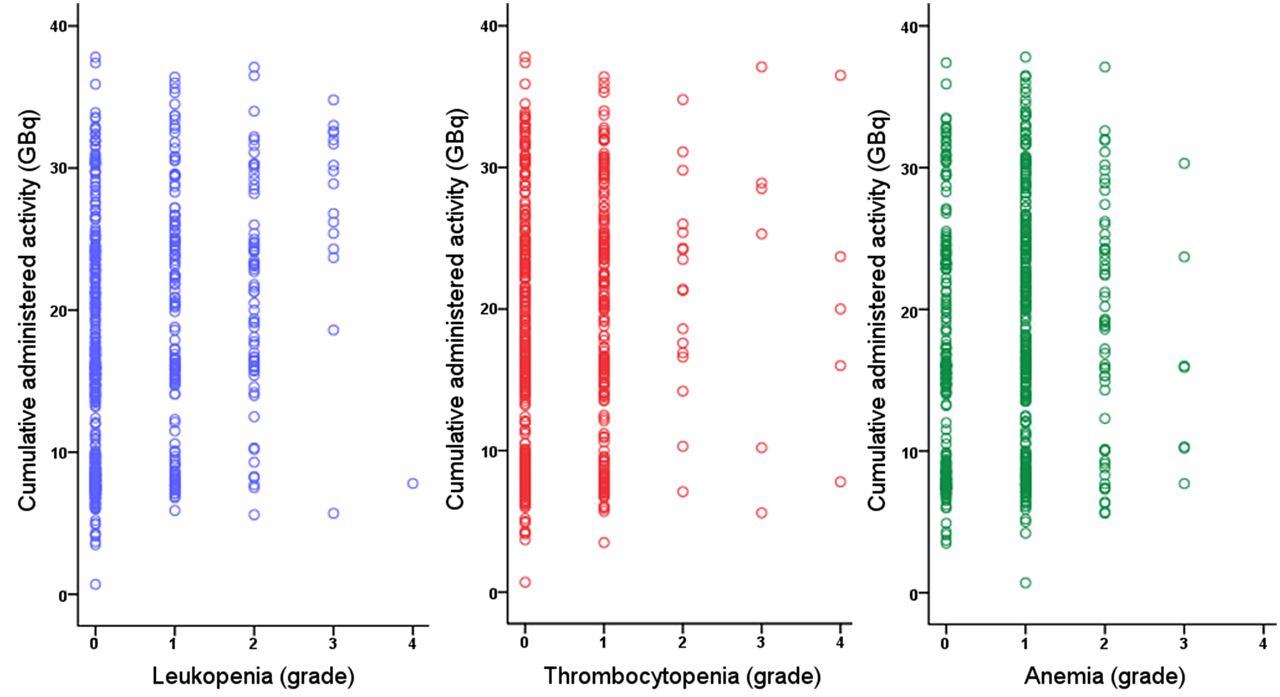
Blood values returned to the reference ranges in all but 1 patient, who died 2 mo after the first therapy cycle because of disease progression. The mean time to complete blood count recovery after the termination of PRRT was 12 mo (range, 3–22 mo). Among the baseline characteristics, a pretreatment reduction of hematologic parameters was the only factor associated with an increased rate of hematotoxicity; this observation remained significant after multiple regression analysis (Table 2). A higher level of cumulative activity was a contributing factor for leukopenia, as shown in Figure 1, and patients who received cumulative doses of less than or equal to 29.6 GBq (800 mCi) developed leukopenia less frequently than patients who received doses of greater than 29.6 GBq (800 mCi) (P < 001) (Fig. 2). None of the other examined variables, including previous chemotherapy (6–18 mo before PRRT), was associated with the incidence or degree of myelosuppression in our cohort (Table 2).
Univariate and Multivariate Analyses for Potential Risk Factors Associated with Hematotoxicity
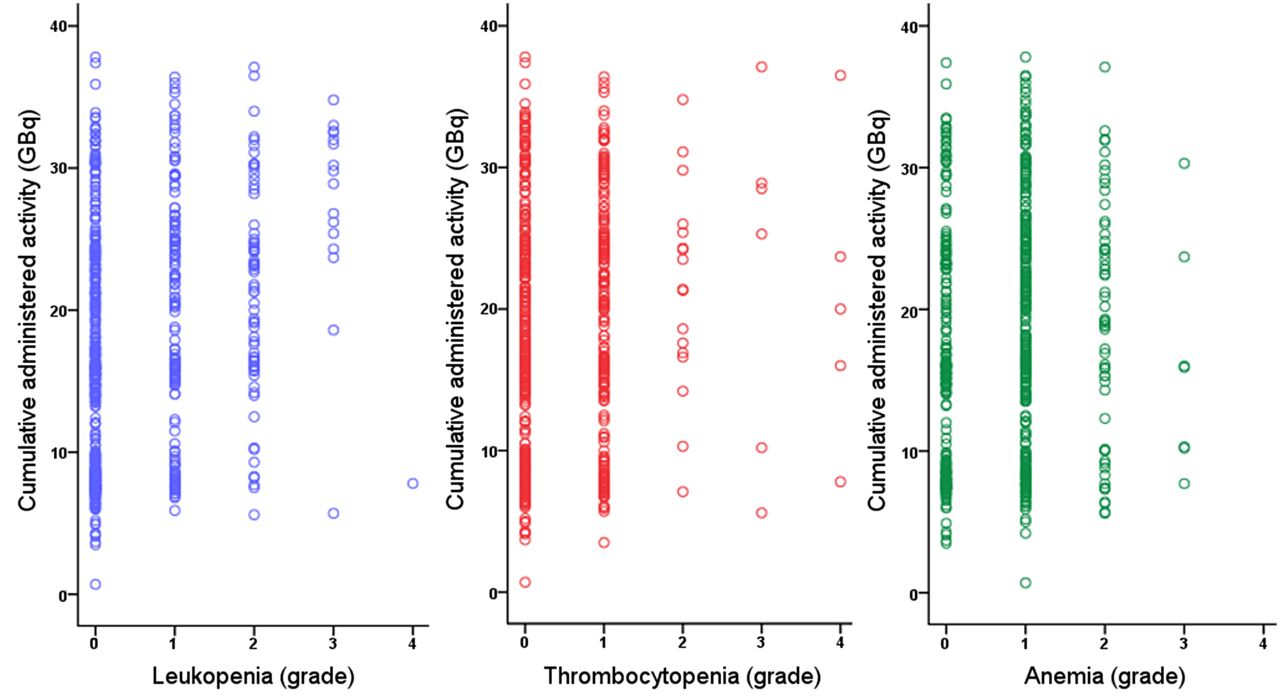
Association of cumulative administered activity and incidence of hematotoxicity after each treatment cycle (n = 632). Higher cumulative administered activity was a contributing factor for leukopenia.

Incidence of significant hematotoxicity in patients receiving cumulative administered activities of less than or equal to 29.6 GBq (≤800 mCi) and greater than 29.6 GBq (>800 mCi). HB = hemoglobin; PLT = platelets; WBC = white blood cells.
None of the 16 patients with a history of splenectomy developed hematotoxicity of grade 3 or 4 (Table 3). Statistical analysis showed that splenectomy was inversely associated with the incidence and degree of leukopenia and thrombocytopenia (Fig. 3). Also, in the subgroup of patients with pancreatic NETs (n = 72), a history of splenectomy was associated with less frequent hematotoxicity.
PRRT-Induced Toxicities
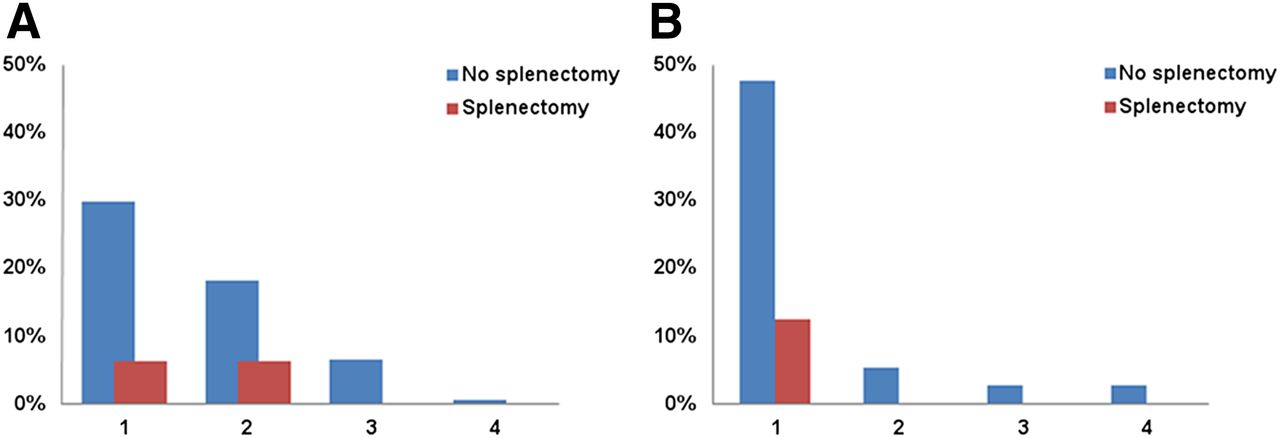
Incidence of hematotoxicity in patients with and without history of splenectomy. (A) Grade of leukopenia. (B) Grade of thrombocytopenia. Grades are shown on x-axes.
Myelodysplastic syndrome as a delayed adverse event, occurring 14, 29, and 34 mo after the termination of PRRT, was documented in 3 patients (1.4%). None of the patients had any of the examined risk factors or received a cumulative activity of greater than 29.6 GBq. The patients were treated with supportive therapy or chemotherapy, such as lenalidomide. One patient with myelodysplastic syndrome developed acute myeloid leukemia 36 mo after the last treatment cycle; this patient received induction chemotherapy with idarubicin and cytosine arabinoside. None of the patients had died from myelodysplastic syndrome by the time this article was being prepared.
DISCUSSION
To avoid PRRT-induced bone marrow hypoplasia, a maximum absorbed dose to the bone marrow of 2 Gy has been suggested (20–22). Several models have been applied for bone marrow dosimetry; these include bone marrow aspiration, calculating the dose to the red marrow from the accumulated activity concentration in the blood, and the MIRD scheme. However, all of these methods are associated with specific difficulties and have limited precision. Furthermore, the high interindividual variability in hematologic alterations after the same absorbed dose to the red marrow makes bone marrow dosimetry in clinical practice less valuable (23,24). In the present study, relevant hematotoxicity (CTCAE grade 3 or 4) occurred after 4.6% of administrations and in 11.3% of patients. These results are in agreement with previously published data reporting significant hematotoxicity in 3.6% of administrations and 9.5% of 504 patients with metastatic gastroenteropancreatic NETs (2).
The results of this large retrospective analysis indicate the acceptable toxicity profile of PRRT (25–29), which compares favorably with the reported toxicities of common chemotherapy regimens, including 5-fluorouracil–streptozocin (20%–30% grade 3 or 4) and sunitinib (>30% grade 3 or 4) for pancreatic NETs (30–33). Our observations provide the first evidence for the minor clinical relevance of hematotoxicity after high cumulative administered activities of more than 29.6 GBq (800 mCi) of 177Lu-octreotate (15,16). First, myelosuppression was almost invariably reversible (202/203 patients), and although 5% of patients completed the treatment with significant impairment in at least 1 of the hematologic parameters, complete bone marrow recovery eventually occurred during follow-up. Second, in only 1 individual in the entire cohort did hematotoxicity (in this case, aggravation of preexisting anemia in a patient previously treated with cisplatin–etoposide) lead to discontinuation of treatment.
The only baseline predictor of significant hematotoxicity in the present study was initial cytopenia. In contrast to other studies (15,34), we observed no correlation between a history of previous chemotherapy and the incidence of hematotoxicity (Table 2); this finding may encourage the use of PRRT with 177Lu-octreotate in groups of patients with generally fewer therapeutic options. Even advanced bone metastases did not promote the risk of hematotoxicity in our cohort (P > 0.2). This finding argues against the suggested relative contraindication of advanced bone metastases for PRRT in terms of toxicity and fits well with the excellent response outcome reported earlier for this condition (35).
A high level of cumulative administered activity was associated with increases in the incidence and severity of leukopenia (Fig. 1). This correlation was also observed with lower levels of activity (cumulative doses of ≤29.6 GBq [≤800 mCi]), in which most treatments will range with currently used protocols (2,15,16). We found no other report in the literature linking the cumulative administered activity of 177Lu-octreotate to hematotoxicity. However, as stated before, hematotoxicity was rarely of clinical relevance, even when high administered activities were used.
The spleen is a major reservoir of blood cells and receives the highest absorbed dose of all organs during PRRT, partly because of the presence of somatostatin receptors on lymphocytes (36,37). This intensive radiation may damage blood cells accumulating in the spleen and consequently reduce peripheral blood cell counts. In the present study, splenectomy indeed was shown to have a protective effect against hematotoxicity (Fig. 3). To the best of our knowledge, this is the first study to show the potentially beneficial effect of this condition in patients undergoing PRRT.
In accordance with other studies (2,20,38), myelodysplastic syndrome was observed as a rare delayed side effect in 3 patients (1.4%) and at least 14 mo after the termination of PRRT. Two of the 3 patients were still alive at the end of the study (follow-up: 32–56 mo). Considering the limited prognosis of patients with advanced metastatic NETs, the low risk of this late side effect should not represent a major argument against performing PRRT.
Selective targeting of B cells has been proposed to be the main cause of lymphopenia after PRRT (39). Unfortunately, differential blood counts were not available for our patients; therefore, alterations in this subset of leukocytes could not be analyzed. However, the main limitation of the present study was the retrospective setting. Nevertheless, because of the general lack of prospective studies in the field of PRRT, retrospective analyses of large cohorts of patients may be regarded as the best available alternative.
CONCLUSION
The overall incidence of PRRT-induced myelosuppression was acceptable, and this condition had a transient nature, even after the use of high levels of cumulative administered activities (>29.6 GBq). Besides administered activity, initial cytopenia was the only factor contributing to myelosuppression, whereas splenectomy may exert a protective effect. Contrary to the findings of previous studies, we found that advanced osseous metastatic disease and previous chemotherapy did not increase the rate of hematotoxicity and should not preclude patients from receiving PRRT with 177Lu-octreotate.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to Professor Eric Krenning, Professor Dik Kwekkeboom, and Professor Wouter A.P. Breeman (Erasmus Medical Center, Rotterdam, The Netherlands) for sharing their experience in the receptor targeting field and making somatostatin receptor–mediated treatment at our institution possible. We also thank Professor Richard P. Baum (Department of Nuclear Medicine and PET Center, Zentralklinik, Bad Berka, Germany) for his critical and constructive input in this field. We also are grateful to the personnel of the Department of Nuclear Medicine in Bonn and especially to the nursing staff of the therapy ward.
Footnotes
Published online Sep. 5, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 28, 2012.
- Accepted for publication May 9, 2013.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Limitations of the radiotheranostic concept in neuroendocrine tumors due to lineage-dependent somatostatin receptor expression on hematopoietic stem and progenitor cells
- Elevated Baseline Mean Corpuscular Volume Predicts the Development of Severe Hematologic Toxicity After 177Lu-DOTATATE Therapy
- Spleen Volume Reduction Is a Reliable and Independent Biomarker for Long-Term Risk of Leukopenia Development in Peptide Receptor Radionuclide Therapy
- Safety and Efficacy of Para-Aminohippurate Coinfusion for Renal Protection During Peptide Receptor Radiotherapy in Patients with Neuroendocrine Tumors
- SPECT/CT Image-Derived Absorbed Dose to Red Marrow Correlates with Hematologic Toxicity in Patients Treated with [177Lu]Lu-DOTATATE
- Specific Uptake in the Bone Marrow Causes High Absorbed Red Marrow Doses During [177Lu]Lu-DOTATATE Treatment
- Specific Uptake in the Bone Marrow Causes High Absorbed Red Marrow Doses During [177Lu]Lu-DOTATATE Treatment
- Evaluation of Hepatotoxicity from Peptide Receptor Radionuclide Therapy in Patients with Gastroenteropancreatic Neuroendocrine Tumors and a Very High Liver Tumor Burden
- Long-Term Outcomes of Submaximal Activities of Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE in Neuroendocrine Tumor Patients
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Somatostatin Receptor-Targeted Radiopeptide Therapy in Treatment-Refractory Meningioma: Individual Patient Data Meta-analysis
- Peptide Receptor Radionuclide Therapy of Late-Stage Neuroendocrine Tumor Patients with Multiple Cycles of 177Lu-DOTA-EB-TATE
- Phase I study of the 177Lu-DOTA0-Tyr3-Octreotate (lutathera) in combination with nivolumab in patients with neuroendocrine tumors of the lung
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Phase I Trial of Well-Differentiated Neuroendocrine Tumors (NETs) with Radiolabeled Somatostatin Antagonist 177Lu-Satoreotide Tetraxetan
- Bone Marrow Absorbed Doses and Correlations with Hematologic Response During 177Lu-DOTATATE Treatments Are Influenced by Image-Based Dosimetry Method and Presence of Skeletal Metastases
- Efficacy and Safety of High-Specific-Activity 131I-MIBG Therapy in Patients with Advanced Pheochromocytoma or Paraganglioma
- Dose Mapping After Endoradiotherapy with 177Lu-DOTATATE/DOTATOC by a Single Measurement After 4 Days
- Pitfalls in the response evaluation after peptide receptor radionuclide therapy with [177Lu-DOTA0,Tyr3]octreotate
- Myeloid neoplasms after chemotherapy and PRRT: myth and reality
- High risk of myelodysplastic syndrome and acute myeloid leukemia after 177Lu-octreotate PRRT in NET patients heavily pretreated with alkylating chemotherapy
- PRRT: Defining the Paradigm Shift to Achieve Standardization and Individualization