


Abstract
High-activity 111In-pentetreotide has been used to treat patients with disseminated neuroendocrine tumors. There is, however, little information related to the efficacy of this agent beyond the normal 6-mo assessment period. Before we can assume that such treatment would be beneficial to patients with neuroendocrine tumors the outcome of the patients over a longer time course should be determined. Methods: The case records of 16 patients who had received high activities of 111In-pentetreotide (with cumulative activities as high as 36.6 GBq) over a 2.5-y period, from January 1, 1997, to June 30, 2000, were reviewed. There were 8 female and 8 male patients (age range, 32–76 y): 10 patients had carcinoid, 2 had medullary cell carcinoma of the thyroid, and 1 each had a gastrinoma, glucagonoma, fibrolamellar cancer, and malignant histiocytoma. The minimum number of treatments received was 1 in 2 patients (with activities of 3.1 and 7 GBq); the maximum was 10 treatments (total, 36.6 GBq). Treatment was given using an infusion pump and was repeated at 4- to 12-wk intervals (mean number of treatments per patient, 6). Response to therapy was determined by changes in the size of the tumor on CT using the response evaluation criteria in solid tumors. Toxicity was measured using blood and urine tests of renal, hepatic, thyroid, and bone marrow function. The mean and median time from the last treatment to progression of disease and death (if applicable) was also calculated. Results: No significant or long-lasting toxicity was encountered. At 6 mo after the patient’s last treatment, 5 patients (30%) had disease progression, 2 had complete responses, and 3 had partial responses. Twelve months after their last treatment, 9 patients (56%) had disease progression, and, at 18 mo, 11 patients (69%) had disease progression. The mean progression-free survival was 12.25 mo (median, 9 mo). For those who survived 6 mo after their last treatment, the mean survival was 15.75 mo (median, 16 mo). At the 6-mo assessment point, there had been 3 deaths (19%): 1 death was not related to cancer. At 12 mo, there was 1 additional cancer death. At 18 mo, there were 3 additional deaths (1 was not related to the patient’s carcinoid tumor but was due to a second coexistent cancer). By the end of the 18-mo assessment period, 7 patients (44%) had died. The mean time interval between disease progression and death was 5 mo. Conclusion: In patients treated with high-activity 111In-pentreotide, 70% had some benefit for at least 6 mo after the end of treatment; however, 31% of patients will have sustained benefit at 18 mo from this treatment. This was obtained without significant toxicity.
Most neuroendocrine tumors (NETs) strongly express somatostatin receptors (SSRs) of subgroups SSR2, SSR3, and SSR5 (1). These can be imaged using 111In-diethylenetriaminepentaacetic acid-D-Phe1-octreotide (pentetreotide) because it binds preferentially to SSR2 and SSR5 receptor subtypes (2,3). 111In-Pentetreotide is considered to be the most sensitive imaging modality for metastatic NETs and is often used as the first-line investigation of these tumors (4).
It has previously been possible to treat disseminated NETs with targeted therapy using 131I-metaiodobenzylguanidine (131I-MIBG), which has been shown to have some clinical activity in those 60% of patients who have expression of the amine uptake gene (5). However, this is not an option if there is no or poor uptake of 131I-MIBG in the tumor.
The therapeutic options for patients with progressive metastatic NETs are often limited (6). Chemotherapy is not only toxic but also has limited efficacy (7). Interferon on its own has no tumorcidal properties although, in combination with Sandostatin (Novartis, Basel, Switzerland), preliminary data suggest some benefit but, again, this maybe associated with significant morbidity (8). Hepatic artery embolization should be reserved for those patients with large liver metastases but will not impact on extrahepatic disease (9). The limitations of all of these therapies, including 131I-MIBG, have led to the development of other tumor-targeting strategies. Because a higher percentage of NETs have uptake of 111In-pentetreotide than have uptake of 131I-MIBG, it would be logical to try to use this agent in the targeted treatment of disseminated NETs. Unlike iodine, an isotope of indium with β-emissions is not readily available. 111In-Pentetreotide is known to be internalized by the NET cell (10); therefore, if given in sufficient activities, 111In-pentetreotide, which produces an Auger electron with a range of about 80–200 nm, could have a therapeutic effect. This would mean that administration of high-activity 111In-pentetreotide could result in significant ionization within the target cell but less damaging γ-irradiation to surrounding cells (11). Because the Auger electrons are less energetic than the β-electrons produced from isotopes such as 131I or 90Y, they may be less toxic to adjacent normal tissue. Recent studies have shown that 111In-pentetreotide can be given in activities of up to 5 GBq with minimal toxicity (12,13). The aim of this study was to perform a retrospective review of the efficacy of high-activity 111In-pentetreotide used as a therapy for metastatic NETs.
MATERIALS AND METHODS
Patient Population
Sixteen patients (8 men, 8 women; age range, 32–76 y), each with an established histologic diagnosis of disseminated NET, were treated. Ten patients had disseminated carcinoid, 2 patients had a medullary carcinoma of the thyroid (MCT), and 1 each had a gastrinoma, glucagonoma, fibrolamellar liver tumor, and malignant histiocytoma (Table 1). Biochemical or imaging evidence of disease progression in the 6 mo leading up to the commencement of the treatment was established in all patients.
Characteristics of Patients Studied and Treatment Given
Patients were selected for treatment with high-activity 111In-pentetreotide only if all other standard treatment options had failed or were deemed inappropriate (e.g., unresectable liver tumor). All patients were reviewed in a multidisciplinary clinic before the decision to treat was approved. To be eligible for treatment, patients had no uptake of 123I-MIBG or had good uptake but failed treatment with 131I-MIBG.
The study had approval of the local ethics committee, and all patients understood the experimental nature of the treatment and gave informed consent. All patients were treated under a research license from the Administration of Radioactive Substances Advisory Committee.
Treatment Schedules
Patients were treated using 2 different regimes. Those with fast-growing tumors and significant symptoms were treated with 3 infusions of 111In-pentetreotide, given at 4- to 6-wk intervals. If there was evidence of response, the patients were then maintained on 3-mo treatments. In those patients with more indolent disease, 3-mo treatments were used from the outset. Injections were stopped for the day of treatment in patients taking octreotide subcutaneously. For those on long-acting somatostatin analogs (Sandostatin long-acting release [Novartis]; or Lanreotide [Ipsen, Paris, France]), the patients were treated without these drugs being stopped. Amino acid coinfusion was not used because no renal toxicity was expected with this agent (13).
Preparation of High-Activity 111In-Pentetreotide
High-activity 111In-pentetreotide was prepared within the radiopharmacy of the Royal Free Hospital using a method we have described (13). Labeling efficiency as measured by thin-layer chromatography, and this had to be >95%. For treatment to be given, each patient was then administered 3–5 GBq 111In-octreotide containing about 30 μg pentetreotide (Mallinckrodt Nuclear Medicine, Petten, The Netherlands). Administration of the labeled product to the patient was performed in a designated room on the oncology ward using an infusion pump positioned behind a lead “castle wall” (13).
The patient was discharged when the retained activity of 111In-octreotide was calculated to have fallen to <400 MBq. A scan was obtained after therapy on the day of discharge.
Assessment of Toxicity
From the results of our previous study (13), which showed no significant toxicity despite repeated administration, patients were monitored before treatment with a complete blood count, plasma creatinine, electrolytes, and liver function tests. These were repeated at 3-mo intervals. In those patients with a rising creatinine level, 3-mo glomerular filtration rate was estimated using blood clearance of 51Cr-ethylenediaminotetraacetate. Toxicity was assessed using World Health Organization criteria.
Assessment of Efficacy
To ensure that it was possible to compare the results of this study with other techniques used in the treatment of patients with disseminated NETs, the number and size of visible lesions were assessed in 15 patients by serial 111In-pentetreotide scanning and anatomic imaging using CT, MRI, or sonography. These scans were determined as showing disease progression, disease stability, and partial or complete response using the response evaluation criteria in solid tumors (14). In the 16th patient, assessment was by reviewing the serial 111In-pentetreotide scans after therapy and by biochemical means because the patient had a radiologically occult tumor. Progression-free and overall survival curves were drawn using SPSS software, version 6.0 (SPSS, New York, NY).
RESULTS
Seventy-six treatments with high-activity 111In-octreotide therapy were given over 3 y (Table 1). In 3 patients (2 with carcinoid tumor, 1 with a malignant histiocytoma), there was a significant reduction in the tumor mass classifiable as a partial response by 6 mo after the last therapy (Table 2). In an additional 2 patients, there was a complete response at 6 mo with no anatomically or scintigraphically visible tumor seen (Fig. 1). Both of these patients had medullary cell carcinoma of the thyroid. In 1 patient, the serum calcitonin fell from 48 mmol/L to an undetectable level and in the other patient it fell from 39 mmol/L to an undetectable level. A further 7 patients attained stability (i.e., no change in the size of a previously growing tumor) at 6 mo after the last treatment. There was further tumor progression in the remaining 4 patients, 3 of whom died within the initial 6-mo assessment period.

Patient with MCT shows disease extent in neck and chest and abdomen (arrows) before treatment (A) and complete response 9 mo later after 3 treatments with high-activity 111In-pentetreotide (B). Note colonic uptake is physiologic.
Results of Treatment
Toxicity
There was no evidence of significant treatment-associated toxicity during this trial or for at least 18 mo after the last treatment. Of the 7 deaths recorded in the initial 18-mo follow-up period, 1 was a cancer death from a second primary (small cell lung cancer) tumor and another was from gastrointestinal bleeding that was not related to the patient’s tumor. Each of these patients had a carcinoid tumor.
Two patients had immediate side effects from the treatment: 1 patient had transient flushing for 15 min after each administration and a second patient had abdominal cramps after administration of the 111In-pentetreotide.
Efficacy
At the initial assessment, 6 mo after the last treatment, 5 patients (30%) had progressive disease (Fig. 2). These patients included 3 with carcinoid tumors and 2 with nonsecreting tumors but with bone metastases: 1 with gastrinoma and 1 with fibrolamellar tumor and cardiac secondary tumors. At 12 mo after the final treatment, 9 patients showed disease progression (56%); the additional 4 patients included 3 with carcinoids (2 of whom had or developed bone metastases) and the 4th patient had a glucagonoma. By 18 mo after the last therapy, 11 patients (69%) had disease progression. The 2 new patients with progressive disease included a patient with a carcinoid and the patient with malignant histiocytoma (who was the only patient with an initial response who had disease progression by 18 mo). The mean progression-free survival was 12 mo, although the median was lower at 9 mo. For those 11 patients who survived 6 mo beyond their last treatment, the mean progression-free survival was 15.75 mo, with a median of 16 mo.
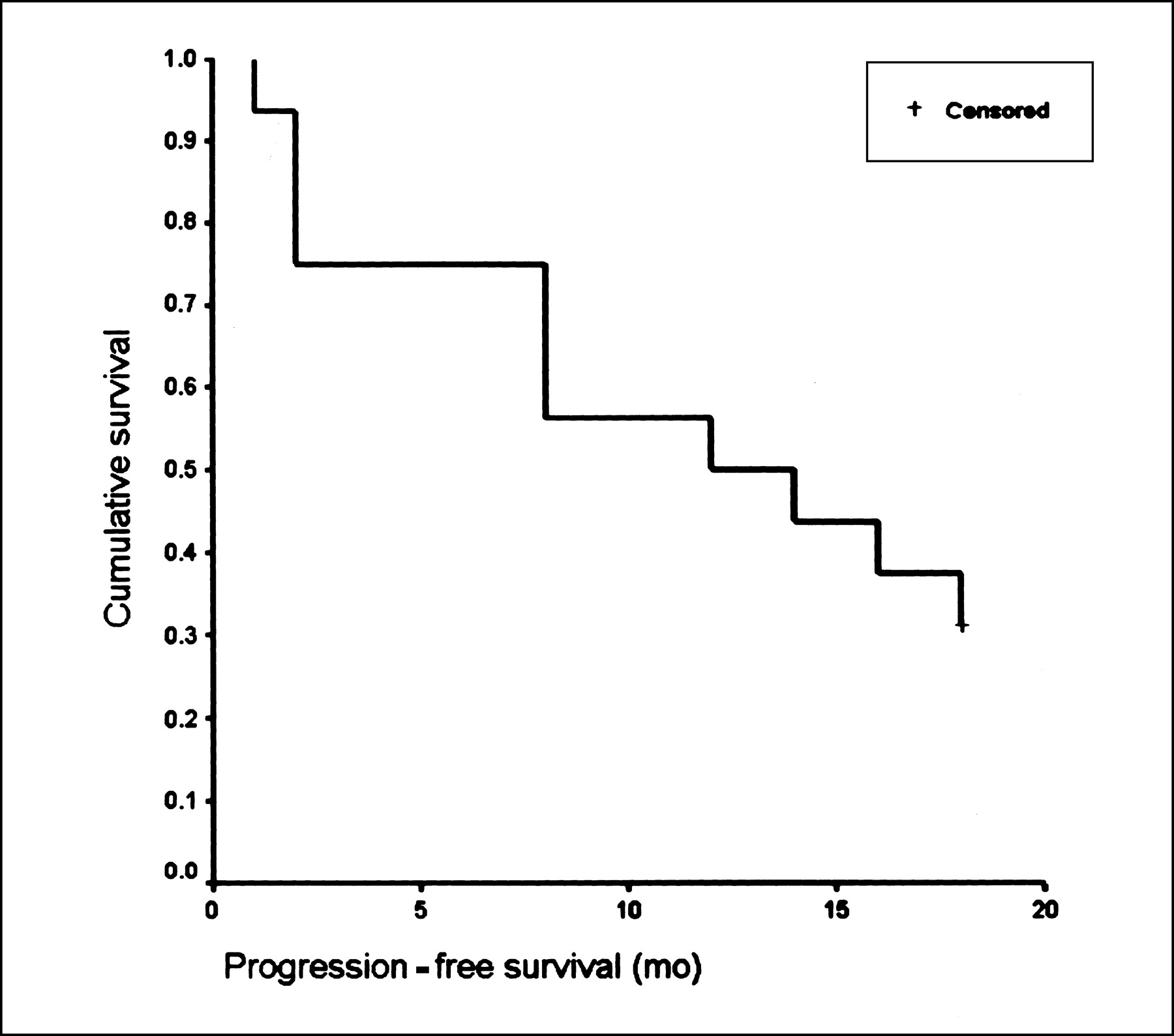
Disease-free survival curves for 18 mo after last treatment with high-activity 111In-pentetreotide. Censored denotes last data point plotted by SPSS.
Of the patients without evidence of disease progression at 18 mo, 2 patients had medullary cell carcinoma of the thyroid and 3 patients had carcinoid tumors, but with disease mainly limited to the liver.
Mortality
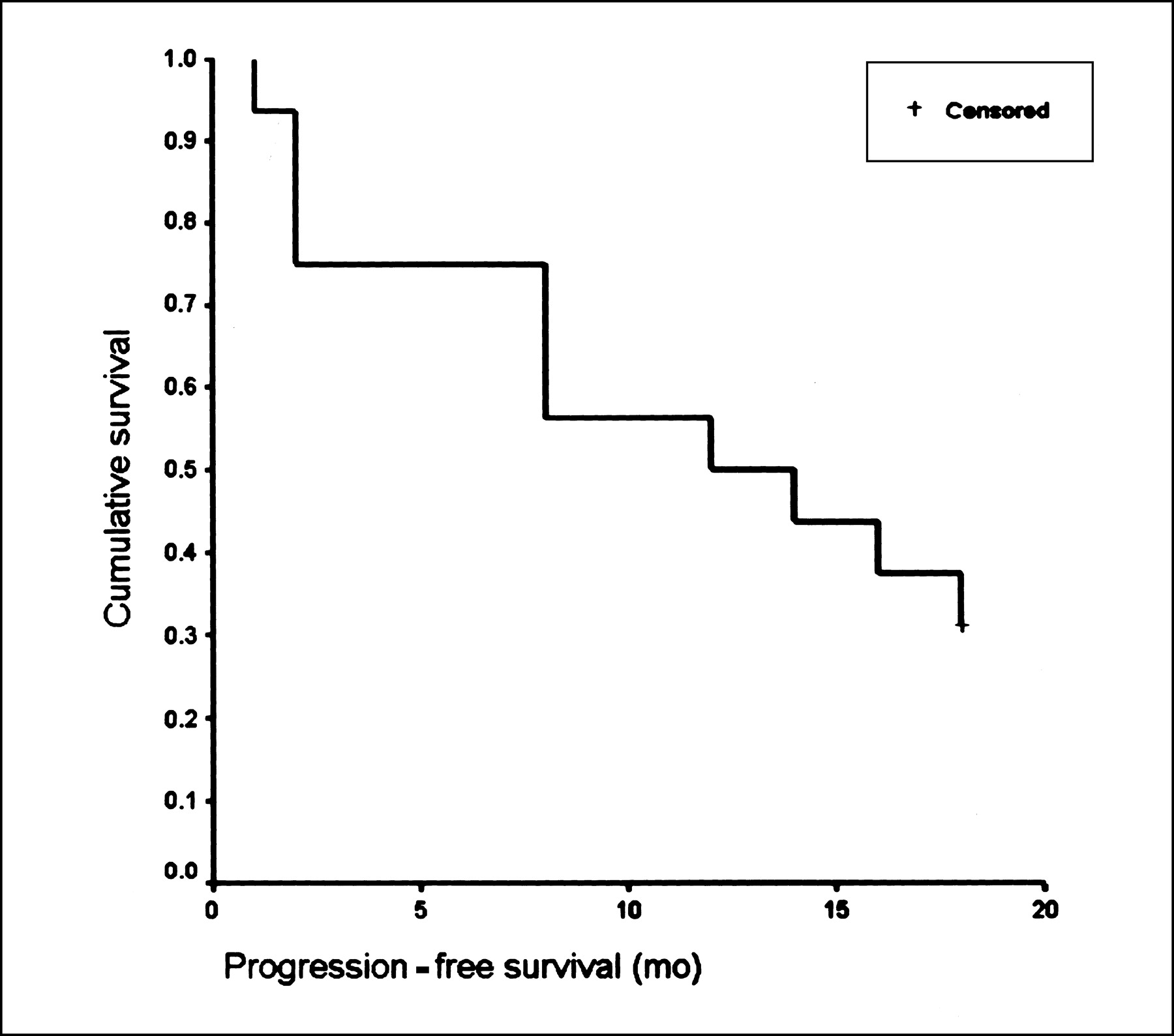
At 6 mo, there were 3 deaths, 1 of which was not related to cancer (Fig. 3). At 12 mo, there was 1 additional cancer death. At 18 mo, there were 3 additional deaths (1 was a cancer death but from small cell lung cancer and not from the patient’s carcinoid). Therefore, there was a total mortality of 7 of 16 patients (44%) at 18 mo after the last treatment. The mean time interval between disease progression and death was 5 mo, with 6 of these patients dying within 6 mo of the disease progression.

Survival curves for 18 mo after last treatment with high-activity 111In-pentetreotide. Censored denotes last data point plotted by SPSS.
DISCUSSION
Previous studies performed by our group and others have shown that high-activity 111In-pentetreotide can show antitumor activity (13,15). In this series of patients, 31% had an objective response from the treatment of their disease with high-activity 111In-pentetreotide. A further 44% had a period of tumor stability, with no growth in tumor size for at least 6 mo after the end of treatment. Therefore, at least 75% of patients showed some benefit from the treatment. This finding compares well with the results of de Jong et al. (16), where 14 of 21 patients (67%) showed either stability or a response. However, a higher proportion of their patients showed partial or complete response (43%). This finding probably reflects that, on average, their patients received twice the activity of 111In-pentetreotide (5–7 GBq for each administration) that our patients received. The number of nonresponders in both groups is almost identical (25% for our group and 33% for the group of de Jong et al.). However, the profile of the patients treated in terms of tumor type and degree of progression may be very different in different studies, making comparison difficult. In addition, one needs to take into account the nonhomogeneous nature of the tumors, so that not all cells have an equal uptake of 111In-pentetreotide.
It is possible that increasing activities of 111In-pentetreotide convert more of the responders from stability to tumor shrinkage. Unfortunately, de Jong et al. (16) do not indicate how long the stability or the tumor regression they reported was maintained.
The response of the tumor may be related to tumor burden so that any given amount of radiation will be spread among more tumor if there is a large tumor bulk, thus reducing the amount of radiation per gram of tumor. This may explain why the 2 patients with MCT had a good tumor response, because they both had a low tumor load compared with some of the carcinoid patients. This may also explain why the patients with MCT did well in our group compared with those treated by de Jong et al. (15,16). In the Dutch group, the patients with MCT all had widespread disease with significant tumor mass. To treat larger tumor masses it may be important to use an isotope that emits a β-particle that can pass through several cells, resulting in a path of ionization across these cells and increasing tumor kill. This could be one of the reasons why good tumor reduction has been reported in some patients with bulky tumors treated with 90Y-labeled somatostatin (17).
The results of our group were achieved with no toxicity, which was not the experience from a similar study performed in the United States. In this American study, 2 treatments of 4–6 GBq were given 4–6 wk apart (12). This resulted in 4 patients having some toxicity; 2 had grade 3 hematologic toxicity needing supportive therapy. Most of our patients received a lower activity (about 3–4 GBq), but had more treatments, which would result in a more fractionated dose of radiation to the marrow and kidneys, a technique often used to reduce morbidity from radiation therapies (18). However, it is also clear that the dosimetric assessment of the agents may not be accurate because it would be expected that, in patients receiving therapeutic activities of 111In-pentetreotide, the radiation dose to the kidneys would be above the level at which toxicity would be expected (19). This does not appear to the case with these patients or those series reported by our group and others (12,13,16).
The treatment was remarkably well tolerated by all of the patients, although 2 had some shaking and abdominal cramps; this was probably related to of the base octreotide given and, despite the low dose (30 μg), there was some pharmacologic action though this was self-limiting. Interestingly, this finding was not related to previous exposure because 1 patient had previous somatostatin analog therapy and 1 had not. This low level of side effects, compared with those expected from radiolabeled antibodies, probably occurs because they are less allergenic, containing no product of animal origin, and the fact that much smaller amounts of product are given—for example, in antibody therapy, anything from a milligram to a gram of antibody may be used. However, the response rate using high-activity 111In-pentetreotide appears to be better than that seen with therapeutic radiolabeled antibodies in solid tumors (20).
There remains the question of whether the natural history of progression of the patient’s disease has been altered. This is difficult to answer from our study, alone, because it is a phase II study without the use of a control, no-treatment arm. It may be possible to look at historical controls but the problem is that the patient mix may be different. Most studies look at all patients with NETs in all stages of the disease or those who are still eligible for surgery where the 5-y survival may be as high as 53% (21). However, the patients treated by 111In-pentetreotide tend to be those who have been refused a surgical option, normally because of more advanced disease. The closest population to that included in our study that can be used for comparison is the group of patients in the above study who did not have surgery and in whom 67% survived 1 y but only 34% survived 3 y. However, until one can identify a good control group, it is difficult to determine that treatment with 111In-pentetreotide changes the natural history of disease.
CONCLUSION
This study has helped to establish the principle that radiotargeted therapy with peptides can be effective in stopping tumor progression in some patients. 111In-Pentetreotide is safe to give and is well tolerated. There can be a sustained response for many months after treatment and this can be achieved with minimal or no toxicity. The best results were seen in those patients with less tumor burden.
Acknowledgments
The authors thank the staff of the nuclear medicine, radiation protection, and pharmaceutical departments who assisted in this project and the staff of Moore Ward at the Royal Free Hospital. This work was supported by the Special Trustees of the Royal Free Hospital and the Research and Development Directorate of the National Health Service Executive.
Footnotes
Received Feb. 11, 2002; revision accepted Jul. 25, 2002.
For correspondence or reprints contact: John R. Buscombe, MD, Department of Nuclear Medicine, Royal Free Hospital, London NW3 2QG, U.K.
E-mail: j.buscombe{at}rfc.ucl.ac.uk
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-Term Hematotoxicity After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Hitting the target: where do molecularly targeted therapies fit in the treatment scheduling of neuroendocrine tumours?
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- Gastrointestinal neuroendocrine tumors: a role for targeted therapies?
- Trifunctional Somatostatin-Based Derivatives Designed for Targeted Radiotherapy Using Auger Electron Emitters
- Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours
- Long-Term Efficacy of Radionuclide Therapy in Patients with Disseminated Neuroendocrine Tumors Uncontrolled by Conventional Therapy