


Article Figures & Data
Figures
- FIGURE 1.
PFS according to RANO criteria and 18F-FET PET response assessment. Responders according to RANO or 18F-FET PET showed longer PFS than did nonresponders (RANO: mean PFS, 7.92 mo for responders vs. 2.25 mo for nonresponders, n = 9 vs. n = 2, respectively, P = 0.015; 18F-FET PET: mean PFS, 10.24 mo for responders vs. 4.1 mo for nonresponders, n = 5 vs. n = 6, respectively, P = 0.025; MWU test). Comparison of the 2 groups reveals that 18F-FET PET responders tended to have longer PFS than RANO responders (mean PFS, 10.24 vs. 7.92 mo, P = 0.25; MWU test).
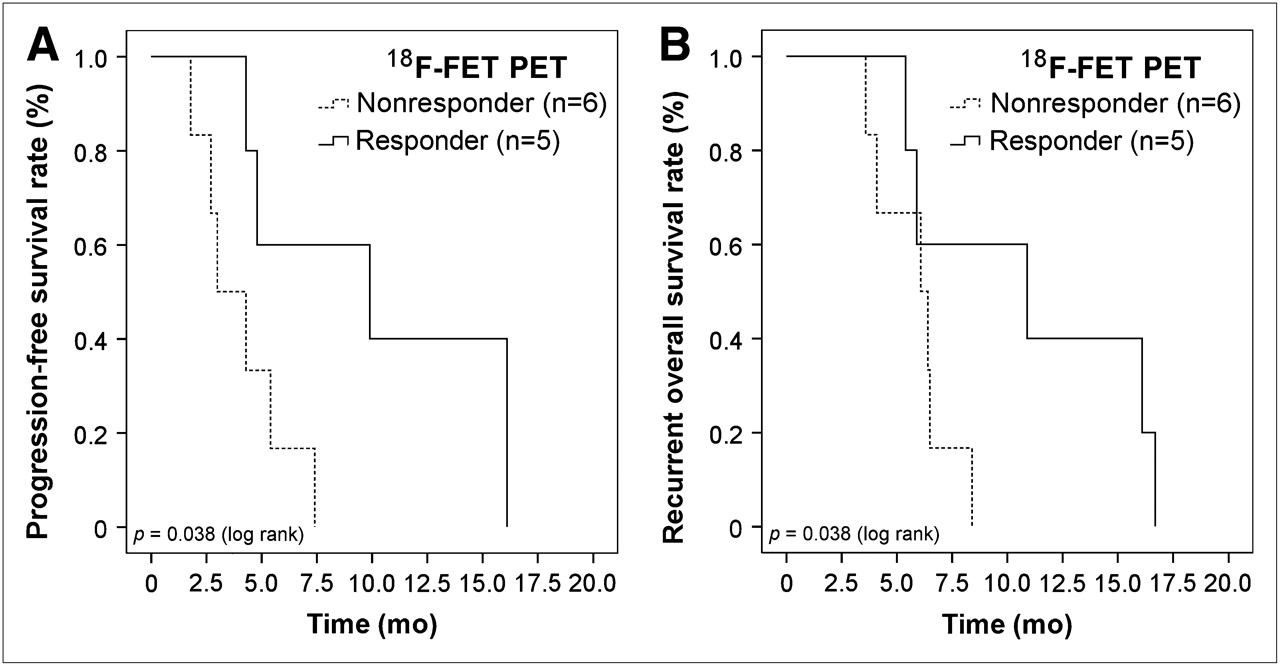
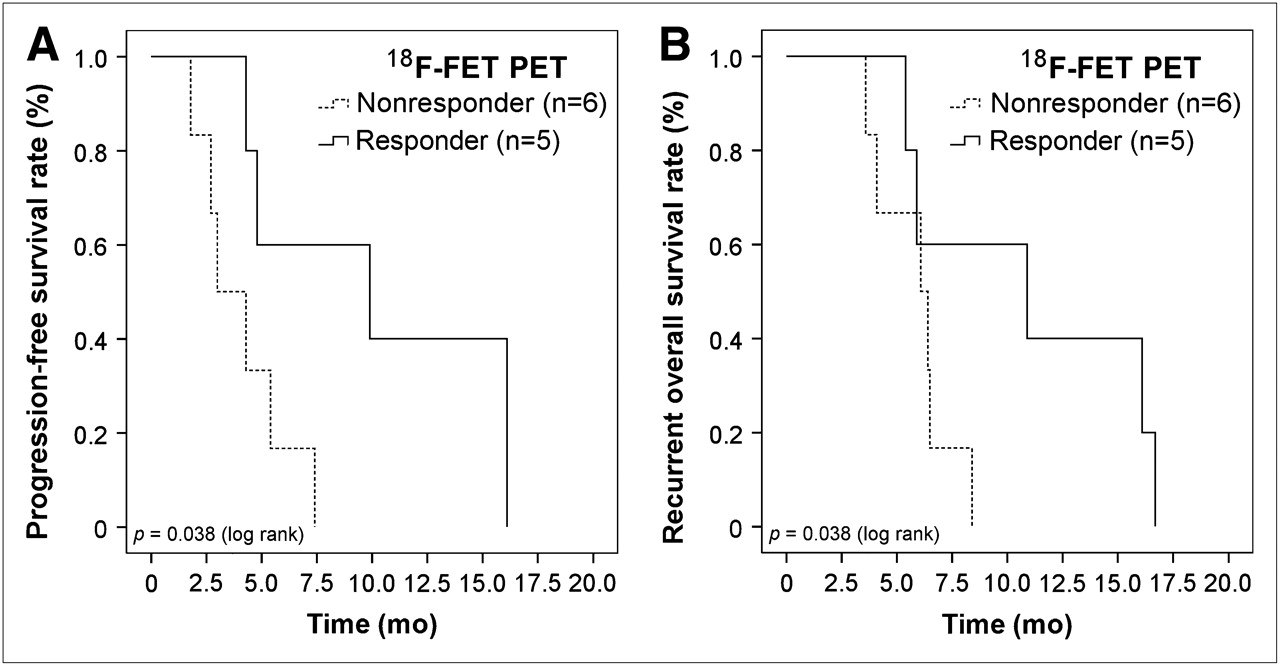
- FIGURE 2.
Univariate survival analysis of 18F-FET PET responders vs. nonresponders during antiangiogenic treatment. (A) 18F-FET PET analysis predicts significantly longer PFS for responders than for nonresponders (P = 0.038, log rank test). (B) 18F-FET PET responders tend to have longer rOS than do nonresponders (P = 0.098, log rank test).
- FIGURE 3.
Changes in MRI and 18F-FET PET tumor volumes during antiangiogenic treatment. Median cT1 tumor volumes decreased in both patient populations—that is, long-term survivors (PFS ≥ 6 mo; n = 3) and short-term survivors (PFS < 6 mo; n = 8)—by 67.2% vs. 33.9% (P = 0.45, MWU test), respectively. Median hT2 volumes also decreased in long-term survivors (n = 3) and short-term survivors (n = 8), by 20.9% vs. 1.6% (P = 0.31, MWU test). In contrast, 18F-FET PET showed tumor to have significantly decreased by 86.3% in long-term survivors, whereas in short-term survivors it had increased by 23.8% (P = 0.042, MWU test).
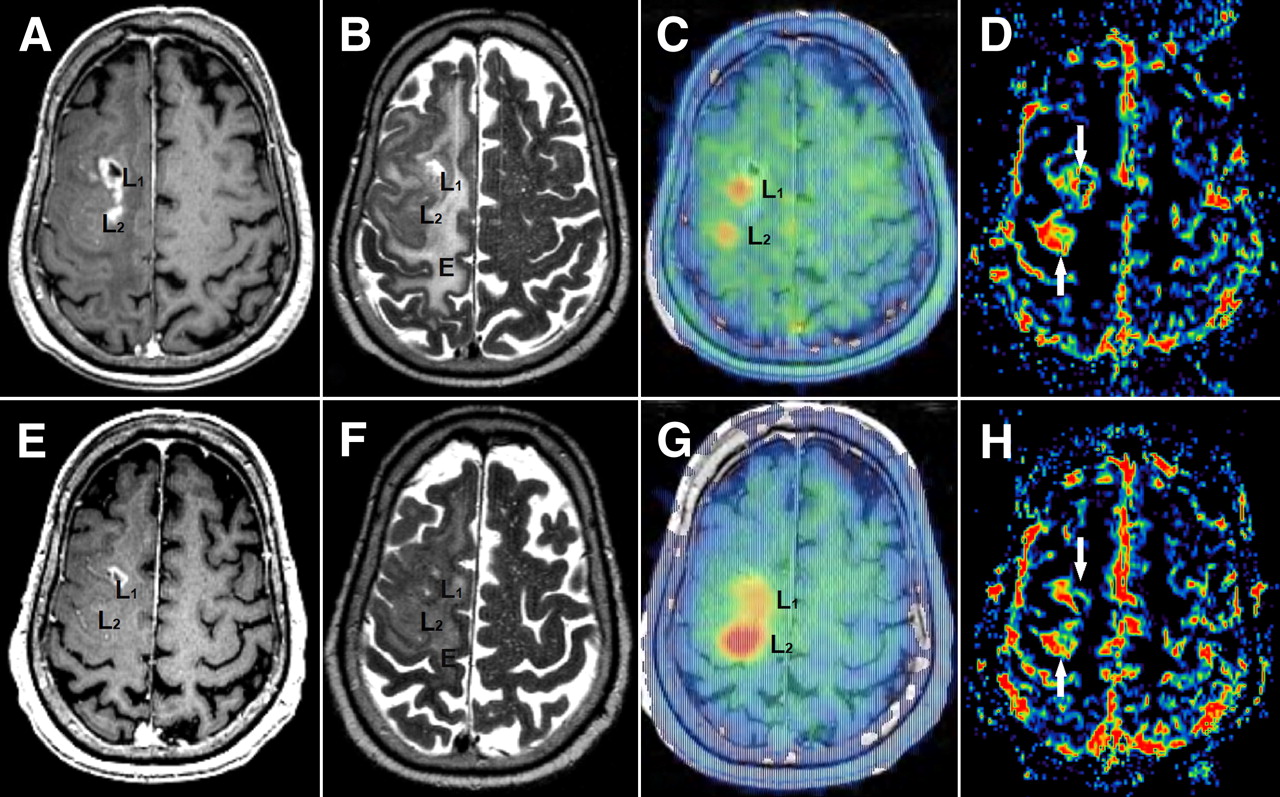
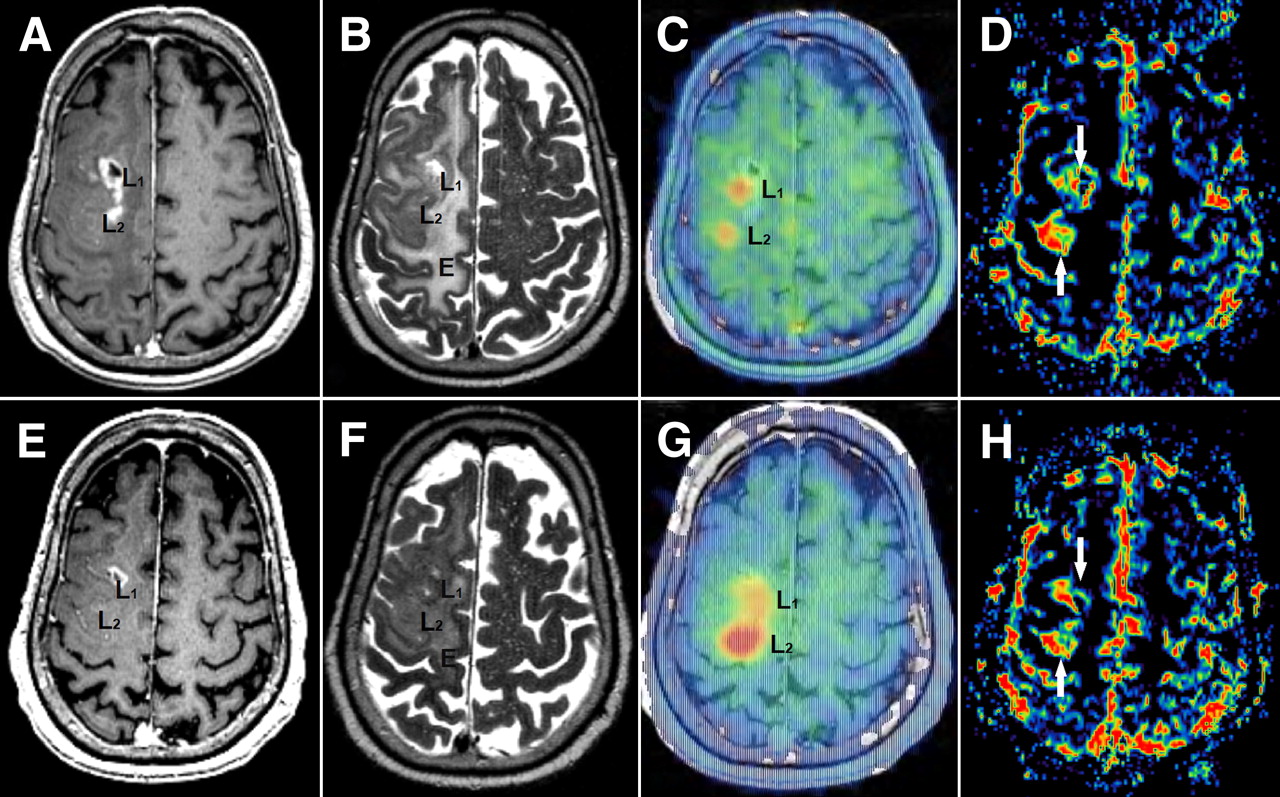
- FIGURE 4.
(A–D) Pretreatment images. (A) Contrast-enhanced T1-weighted MRI shows a small central necrotic contrast-enhancing lesion in ventral part of the tumor (L1, cT1-positive) and nonenhancing tumor lesion in dorsal tumor mass (L2, cT1-negative). (B) MRI shows T2-hyperintense tumor and perifocal edema (E). (C) MRI/FET PET image fusion reveals tracer uptake in both MRI lesions L1 and L2. (E–H) Imaging after 12 wk of treatment. (E and F) MRI shows decrease in T1 contrast enhancement (L1) as well as in T2 signal hyperintensity in peritumoral edema (E). (G) 18F-FET PET/MRI image fusion shows partial response for cT1-positive ventral metabolic lesions (L1) but progression for dorsal tumor part (L2). (D and H) MRI perfusion reveals increased local cerebral blood volume in both tumor fractions (white arrows). This observation suggests differently involved molecular pathways in tumor angiogenesis and gliomagenesis (ventral lesion: VEGF-dependent; dorsal lesion: VEGF-independent). E = peritumoral edema; L1 = ventral, cT1-positive tumor part; L2 = dorsal, cT1 negative tumor part.
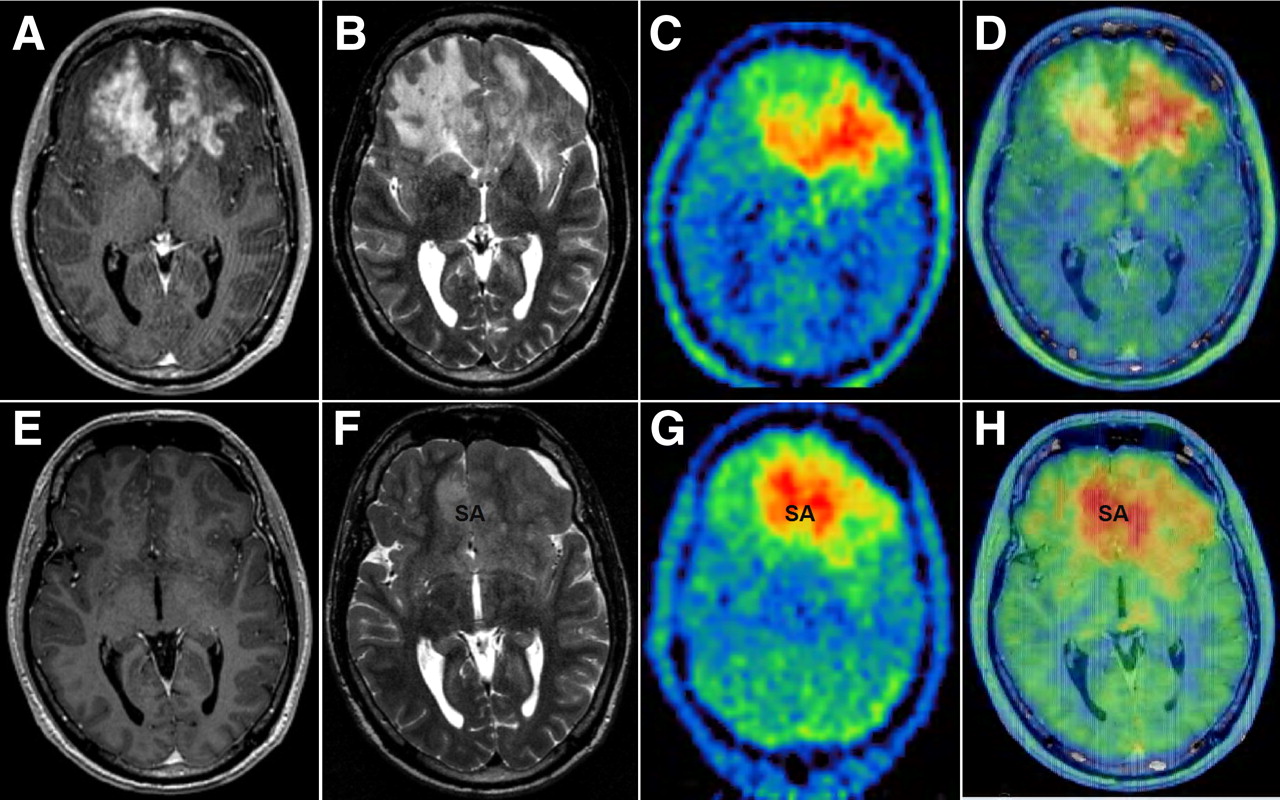
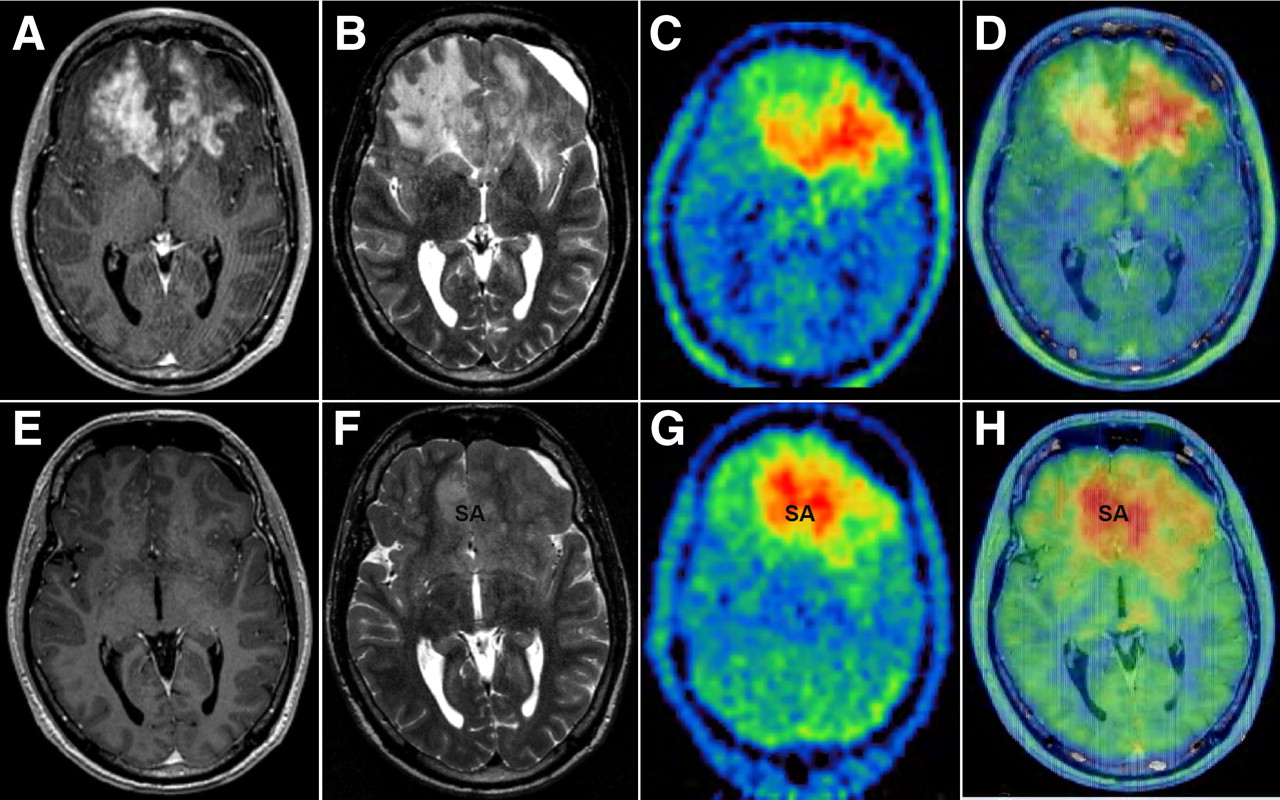
- FIGURE 5.
Comparison of MRI and 18F-FET PET during antiangiogenic therapy for patient (Table 1). (A–D) Pretreatment images. (A and B) Contrast-enhanced T1-weighted MR image shows bifrontal tumor mass with large cT1 (A) and hT2 volume (B). (C) 18F-FET PET reveals large hypermetabolic tumor left frontal lobe, whereas contrast enhancement is more pronounced in right frontal lobe. (D) 18F-FET PET/MRI image fusion shows inconsistent overlap of contrast enhancement in T1 and 18F-FET PET uptake. (E–H) Imaging after 12 wk of treatment, during which patient's neurologic symptoms inexorably progressed. (E and F) MRI shows decrease in T1 contrast-enhancement (E) and T2 signal hyperintensity (F, signal abnormality). (G) 18F-FET PET reveals slight decrease in volume (−13%) but striking change in hypermetabolic distribution pattern (decrease in left frontal lobe but increase in ventral corpus callosum and right frontomesial lobe). (H) PET/MRI image fusion shows increased local cerebral blood flow in both tumor fractions. Tumor extent on MRI did not match 18F-FET PET hypermetabolic tumor areas. This discrepancy may provide important information regarding further planning of, for example, radiotherapy. SA = signal abnormality.


Tables
Initial diagnosis Treatment course before B/I therapy Before B/I therapy PFS/OS analysis Patient no. Sex Age at initial diagnosis (y) Tumor location Tumor type KPS* No. of recurrences during treatment course Surgery Radiation† (Gy) Chemotherapy Tumor type KPS* PFS OS rOS 1 F 53 R/T GBM IV 90 2 (0)MTR (1, 2)MTR (0)60 (0)TMZ (1)TMZ GBM IV 70 4.8 81.9 5.4 2 M 37 R/T GBM IV 90 3 (0)MTR (1, 3)MTR (0)60 (0)TMZ (1)SUT, (2)TMZ GBM IV 60 2.7 45.7 3.6 3 M 60 L/P GBM IV 100 2 (0)MTR (0)60 (0)TMZ (1)TMZ GBM IV 70 5.4 Alive Alive 4 M 63 L/P GBM IV 80 2 (0)PR (0)60 (0)TMZ (1)SUT GBM IV 80 1.8 18.2 6.5 5 F 69 R/T GS IV 90 2 (0)MTR (0)60 (0)TMZ (1)SUT GS IV 50 4.3 23.3 5.9 6 F 46 L/F ODG III–IV 90 3 (0)PR(1, 2)MTR (0)− (1, 2)60 (0)PCV (1)TMZ sGBM IV HISTO 80 9.9 50.4 10.9 7 M 37 R/F-T AA III 100 2 (0)MTR(1)MTR (0)60 − (1)Caelyx sGBM IV HISTO 60 7.4 113.6 8.4 8 M 60 R/F-P AA III 100 1 (0)SB (0)60 (0)TMZ sGBM IV MRI 60 4.3 16.4 6.1 9 F 62 L/P AA III 60 1 (0)PR (0)60 (0)TMZ sGBM IV MRI 50 No progress Alive Alive 10 M 44 R/F AA III 90 3 (0)PR (0)60 (0)PCV (1, 2)TMZ sGBM IV MRI 90 No progress Alive Alive 11 M 33 L-R/F OA II 100 5 (0)PR (1, 4)MTR − (1, 2)60 − (3)PCV, (4)TMZ sGBM IV HISTO 70 3 169.5 4.1 ↵* Karnofsky Performance Status (KPS) at initial diagnosis and before B/I therapy.
↵† Extended field.
R = right hemisphere; T = temporal; (0) = primary tumor; MTR = macroscopic total resection; (1) = first recurrence; (n) n recurrences until death/evaluation; TMZ = temozolomide; SUT = sunitinib; L = left hemisphere; P = parietal; PR = partial resection; GS = gliosarcoma WHO IV; F = frontal; ODG = oligodendroglioma WHO III–IV; Caelyx = anthracycline; SB = stereotactic biopsy; OA = oligoastrocytoma WHO II.
At initial diagnosis, histology was confirmed in all 11 patients. Before B/I treatment, histology of sGBM was confirmed in 3 of 6 cases (HISTO); 3 cases were diagnosed by MRI (MRI).
MRI T1 postcontrast (cm3) MRI T2 (cm3) 18F-FET PET (cm3) Response assessment Patient no. Baseline Follow-up Change (%) Baseline Follow-up Change (%) Baseline Follow-up Change (%) RANO* FET PET† 1 68.1 29.3 −57 148.8 177.4 19.2 91.0 49.9 −45 PR Responder 2 7.1 45.4 >1,000 97.5 110.1 13 57.5 94.3 64 PD NR 3 32.8 12.3 −62 218.2 135.4 −38 46.9 74.6 59 PR‡ NR‡ 4 16 11.5 −28 43.3 62.6 45 22.1 20.1 −9 PD NR 5 12.6 3.5 −72 143.0 82.9 −42 16.2 0.2 −99 PR Responder 6 39.7 2.5 −94 62.6 29.0 −54 67.0 5.8 −91 PR Responder 7 54.1 5.3 −90 180.5 154.3 −15 98.3 153.8 57 PR‡ NR‡ 8 7.3 1.8 −75 151.1 168.2 11 7.0 12.8 82 PR‡ NR‡ 9 4.4 2.9 −34 107.7 133.9 24 94.2 12.9 −86 Stable disease Responder 10 11.1 10.1 −9 67.6 53.4 −21 23.3 12.4 −47 Stable disease Responder 11 105.6 6.8 −94 150.7 85.1 −44 104.6 90.8 −13 PR‡ NR‡ ↵* RANO criteria (8): in addition to standard Macdonald criteria, partial response requires stable or improved nonenhancing (T2/FLAIR) lesions; stable disease requires stable nonenhancing lesions; and progressive disease requires a significant increase in nonenhancing lesions.
↵† 18F-FET PET response assessment: responder = uptake reduction ≥ 45%; nonresponder = includes all other situations.
↵‡ Mismatch between RANO (partial responder) and 18F-FET PET (nonresponder) response assessment.
PR = partial response; PD = progressive disease; NR = nonresponder.
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- MRI and 18FET-PET Predict Survival Benefit from Bevacizumab Plus Radiotherapy in Patients with Isocitrate Dehydrogenase Wild-type Glioblastoma: Results from the Randomized ARTE Trial
- Imaging necrosis during treatment is associated with worse survival in EORTC 26101 study
- Influence of Bevacizumab on Blood-Brain Barrier Permeability and O-(2-18F-Fluoroethyl)-L-Tyrosine Uptake in Rat Gliomas
- Combined PET Imaging of the Inflammatory Tumor Microenvironment Identifies Margins of Unique Radiotracer Uptake
- Lessons From Anti-Vascular Endothelial Growth Factor and Anti-Vascular Endothelial Growth Factor Receptor Trials in Patients With Glioblastoma
- Treatment Response Evaluation Using 18F-FDOPA PET in Patients with Recurrent Malignant Glioma on Bevacizumab Therapy
- Progression types after antiangiogenic therapy are related to outcome in recurrent glioblastoma
- Dynamic 18F-FET PET in Newly Diagnosed Astrocytic Low-Grade Glioma Identifies High-Risk Patients
- Assessment of Treatment Response in Patients with Glioblastoma Using O-(2-18F-Fluoroethyl)-L-Tyrosine PET in Comparison to MRI
- Impact of 3,4-Dihydroxy-6-18F-Fluoro-L-Phenylalanine PET/CT on Managing Patients with Brain Tumors: The Referring Physician's Perspective
- 3'-Deoxy-3'-18F-Fluorothymidine PET and MRI for Early Survival Predictions in Patients with Recurrent Malignant Glioma Treated with Bevacizumab