


Abstract
Restoration of the blood–brain barrier (BBB) after antiangiogenic therapy of gliomas with bevacizumab may result in a decrease in contrast enhancement on MRI despite tumor progression. This so-called pseudoresponse is difficult to differentiate from a true tumor response with conventional MRI. Initial patient studies have indicated that PET using O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) may be helpful for solving this diagnostic problem. This study was performed to investigate the effects of bevacizumab on BBB permeability and 18F-FET uptake in a human xenograft model. Methods: Human U87 glioblastoma cells were implanted into the striatum of immunodeficient RNU rats. 18F-FET PET scans and ex vivo autoradiography were performed in animals receiving a single high dose of bevacizumab (45 mg/kg 2 d before PET; n = 9) or in animals receiving 2 lower doses (10 mg/kg 9 and 2 d before PET; n = 10) to evaluate short-term and long-term effects on the BBB, respectively, and in control animals without bevacizumab treatment (n = 8). Time–activity curves, slope, and tumor-to-brain ratios of 18F-FET uptake (18–61 min after injection) were evaluated using a volume-of-interest analysis. After PET scanning, Evans blue dye (EBD) was injected into animals, and cryosections of the brains were evaluated by autoradiography, by histology, and for EBD fluorescence to assess BBB permeability. Results: Compared with the control, short-term bevacizumab therapy resulted in a trend toward BBB restoration (P = 0.055) and long-term therapy resulted in a significant decrease (P = 0.004) in BBB permeability, as assessed by EBD fluorescence. In contrast, no significant differences in tumor-to-brain ratios or slope of 18F-FET uptake were observed in PET and autoradiography (P > 0.05). Conclusion: 8F-FET uptake in glioblastomas seems to be largely independent of BBB permeability and reflects the viability of tumor tissue during antiangiogenic therapy more reliably than contrast-enhanced MRI.
Brain tumor diagnostics using PET with radiolabeled amino acids, such as l-[methyl-11C]methionine (11C-MET), O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET), or 3,4-dihydroxy-6-18F-fluoro-l-phenylalanine (18F-FDOPA), are gaining interest and were recently recommended by the Response Assessment in Neuro-Oncology Working Group for every stage of management of patients with brain tumors (1,2). Amino acid PET provides important information beyond that provided by standard MRI with respect to delineation of the extent of tumor for biopsy guidance or resection planning, estimation of prognosis, grading, differentiation of treatment-related effects from tumor progression, and treatment monitoring (3–13). Compared with 11C-MET, 18F-FET and 18F-FDOPA have logistic advantages because of the longer half-life of 18F (110 vs. 20 min) (14–18).
The humanized monoclonal antibody bevacizumab (Avastin; Genentech/Roche) inhibits the biologic activity of vascular endothelial growth factor. From 2007 to 2014, bevacizumab was intensively evaluated in phase 2 and 3 trials, particularly in the early phase of the course of malignant gliomas—that is, in newly diagnosed glioblastomas or at first recurrence or progression (19). However, at this stage of disease, the use of bevacizumab has not improved overall survival (20). Currently, bevacizumab is frequently used in many neurooncologic centers at a late stage of disease, particularly when standard treatment options—such as surgery, radiation, and alkylating chemotherapy—are no longer helpful or possible or when a reduction in the corticosteroid dosage for symptomatic therapy is considered. Bevacizumab is usually administered intravenously (10 mg/kg every 2 wk) as a single agent or as a combined therapy. Treatment influences brain tumor vasculature and leads to restoration of the blood–brain barrier (BBB), resulting in decreased contrast enhancement on MRI and reduced peritumoral edema. An important problem in the follow-up of malignant glioma, however, is a decrease in contrast enhancement on MRI after antiangiogenic therapy with bevacizumab; this feature does not reflect a true antitumoral effect and is called a pseudoresponse (21). This decrease in contrast enhancement caused by restoration of the BBB can be mistaken for a treatment response, as MRI contrast enhancement primarily reflects impairment of the BBB (22).
The Response Assessment in Neuro-Oncology Working Group suggested new recommendations for evaluating the response to antiangiogenic drugs, including fluid-attenuated inversion recovery or T2 signal alterations, as criteria for determining tumor response or progression (23). However, these new criteria do not provide quantitative values, and various pathologies can result in hyperintense fluid-attenuated inversion recovery or T2 signal alterations, which are difficult to distinguish from a nonenhancing tumor (21). Consequently, alternative diagnostic methods are needed to assess the effects of bevacizumab treatment (24).
Dynamic 18F-FET PET has been shown to be superior to other imaging methods for differentiating progression from nonneoplastic changes (7,10,25). Initial pilot studies with this technique for bevacizumab treatment monitoring in patients with malignant gliomas demonstrated that PET using 18F-FET detected treatment failure earlier than MRI—on the basis of the criteria of the Response Assessment in Neuro-Oncology Working Group—and predicted favorable outcomes of responders (26–28). However, data on the influence of bevacizumab-related alterations of the BBB on 18F-FET uptake are limited, and further evaluation is needed.
In this preclinical study, the influence of antiangiogenic treatment with bevacizumab on BBB integrity, 18F-FET uptake, and the slope of the late phase of the time–activity curve was tested in a U87 human glioblastoma xenograft model. This tumor model was chosen because it is largely resistant to bevacizumab on the one hand but shows a significant decrease in contrast enhancement on MRI after bevacizumab treatment on the other hand (29,30). Therefore, it appears to be well suited for simulating the phenomenon of the pseudoresponse and for testing the role of 18F-FET PET in this setting.
MATERIALS AND METHODS
Animals
Twenty-seven male immunodeficient RNU rats (Charles River Laboratories) were included in this study. All animals were handled in accordance with the Animal Research Committee of the Research Center Jülich GmbH, the German Animal Welfare Act, and the European Community Council directives regarding the protection of animals used for experimental and scientific purposes (2010/63/EU). All rats weighed 250–310 g and were kept under standard housing conditions with free access to food and water. Human U87 glioma cells were implanted into the striatum of the animals, and the presence of a brain tumor was verified by histologic staining with 4′,6-diamidino-2-phenylindole (DAPI) after completion of the studies.
Animals were divided into a control group (n = 8), a group receiving short-term bevacizumab treatment (n = 9), and a group receiving long-term bevacizumab treatment (n = 10). All animals were sacrificed after 18F-FET PET, and cryosections of the brains were analyzed by autoradiography (AR), by histology, and for Evans blue dye (EBD) fluorescence to assess BBB permeability.
Tumor Inoculation and Bevacizumab Treatment
U87 cells (HTB-14; American Type Culture Collection) were cultured in Eagle minimum essential medium supplemented with 10% fetal calf serum, penicillin/streptomycin, glutamate, and 1% nonessential amino acids. At a confluence of approximately 95%, cells were prepared for inoculation. Cells were washed twice with phosphate-buffered saline and detached by incubation with trypsin/ethylenediaminetetraacetic acid for approximately 5 min. Cells were resolved in growth medium to a concentration of 500,000 per 5-μL implantation volume. Cells were stereotactically implanted into the right basal ganglia under anesthesia as described previously (31). PET scans, EBD staining (2% EBD [500 μL/kg] in NaCl, administered intravenously 30 min before sacrifice), and histologic evaluations were performed on day 13 or 14 after tumor implantation.
Rats receiving long-term bevacizumab treatment (n = 10) received 2 injections of bevacizumab (10 mg/kg intravenously) 9 and 2 d before 18F-FET PET. Rats receiving short-term bevacizumab treatment (n = 9) received 1 injection (45 mg/kg intravenously) 2 d before 18F-FET PET. The control group (n = 8) received no treatment. For technical reasons, only 6 rats from the control group were evaluated for EBD extravasation and by AR.
Imaging Methods
After isoflurane anesthetization, a venous catheter was inserted into 1 tail vein. The rats were positioned in the field of view of a small-animal scanner (INVEON; Siemens-CTI) (32). Body temperature was maintained at 37.8°C ± 0.3°C (mean ± SD) with an infrared lamp. Breathing rate was regulated at 48–55 breaths/min with a pressure-sensitive pad positioned under the rats. 18F-FET with a specific radioactivity of greater than 200 GBq/μmol was synthesized in-house as described elsewhere (33). After a transmission scan (10–20 min), dynamic data acquisition was performed in the 3-dimensional list mode for 61 min starting with an injection of 40 ± 3 MBq of 18F-FET in saline into the tail vein (bolus injection of 0.5 mL in 1 min). Emission data were framed into a dynamic sequence of 6 × 10 s, 5 × 60 s, 5 × 3 min, and 10 × 4 min frames. Filtered backprojection (ramp filter; cutoff, 0.5) was applied to reconstruct 159 slices with an image voxel size of 0.7764 × 0.7764 × 0.796 mm (matrix size, 128 × 128 × 159). Images were corrected for random coincidences, scatter radiation, and attenuation. Because an INVEON software update during the course of the experiments affected data reconstruction, a calibration factor of 1.20 was applied to a portion of the data to guarantee comparability. After the PET scan and EBD injection, rats were sacrificed.
Brains were removed, quickly frozen in liquid isopentane (−50°C), and cut into 20-μm-thick slices with a cryostat. The presence of a brain tumor was verified by fluorescence staining with DAPI. EBD extravasation was evaluated quantitatively on the basis of fluorescence intensity per animal by defining regions of interest in a single brain slice in the area of the tumor with an Aida Image Analyzer (AIDA version 4.50; Raytest). Regions of interest were placed in healthy contralateral tissue and in the tumor after consideration of histologic staining. EBD extravasation in the tumor area is reported as tumor-to-brain ratios (TBRs).
For AR, an imaging plate (Fuji Imaging Plate; Raytest) was exposed overnight to every tenth slice and freshly prepared 20-μm 18F standards for a calibration curve; samples were scanned (Fuji BAS Reader 5000; Raytest) and evaluated for 18F-FET uptake in a pixel size of 200 μm (AIDA version 4.50).
Anti–von Willebrand factor antibody (ab6994; Abcam) staining was performed using a standard protocol for diaminobenzidine staining to visualize blood vessels. Cell nuclei were counterstained with hematoxylin.
Data Analysis
Analysis of PET data was performed with Pmod version 3.4 (PMOD Technologies Ltd.). 18F-FET uptake in the tissue was expressed as the SUV by dividing the radioactivity (kBq/mL) in the tissue by the radioactivity injected per gram of body weight. Summed PET images (18–61 min after injection) were used for volume-of-interest (VOI) analysis as described previously (34). The tumor VOI on 18F-FET PET scans was determined by a 3-dimensional autocontouring process with a cutoff of greater than or equal to 1.7 for the TBR of 18F-FET uptake; this cutoff proved to be reliable for indicating the actual tumor size (34). 18F-FET uptake in the unaffected brain tissue was determined from a larger VOI placed in an area of normal brain tissue including white and gray matter (250 voxels; 120 mm3) in the contralateral hemisphere. The mean TBR (TBRmean) was calculated by dividing the mean VOI (Bq/mL) of the tumor by the mean VOI of normal brain tissue; the maximum TBR (TBRmax) was calculated by dividing the maximum VOI (5 hottest voxels) of the tumor by the mean VOI of normal brain tissue. A linear regression line was fitted to the late phase of time–activity curves (18–61 min after injection) to determine the slope.
Statistics
Descriptive statistics are provided as mean and SD. One-way ANOVAs with all pairwise multiple-comparison procedures (Holm–Sidak method) were performed for PET data, EBD evaluations, and AR to detect differences among the treatments without correction for multiple testing. P values of less than or equal to 0.05 were considered significant. Statistical analysis was performed using SigmaPlot for Windows version 12.5 (Systat Software, Inc.).
RESULTS
Consecutive representative overviews of histologic DAPI staining, EBD fluorescence, AR, and corresponding 18F-FET uptake from PET scans of a control brain, a brain receiving short-term treatment with bevacizumab, and a brain receiving long-term treatment with bevacizumab are shown in Figure 1. In the control group, intense EBD fluorescence indicated BBB impairment in the area of the tumor, whereas fluorescence was less intense in the group receiving short-term treatment and no longer visible in the group receiving long-term treatment. 18F-FET uptake in AR was restricted to the tumor areas, and summed images (18–61 min after injection) seemed to be unaffected by bevacizumab treatment (Figs. 1C and 1D) despite a reduction in BBB permeability (Fig. 1B).
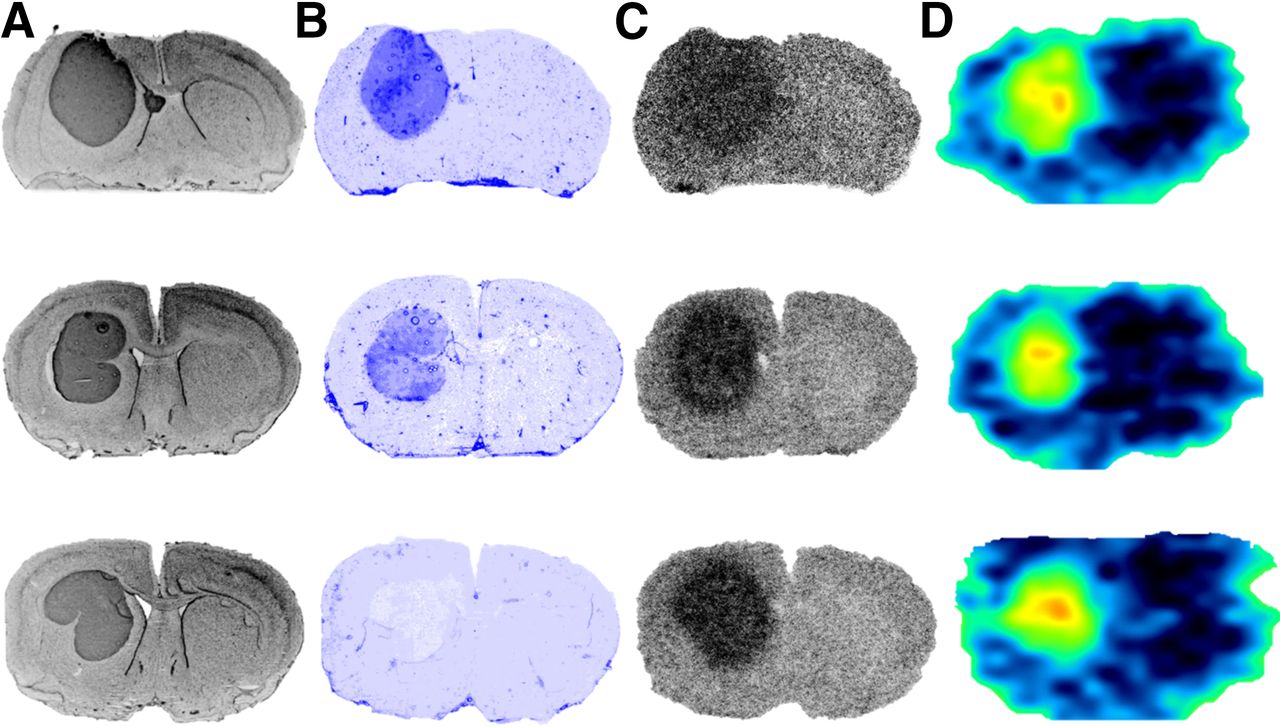
Overviews of different imaging methods. (A) DAPI nuclear stains show tumor dimensions. (B) EBD fluorescence images show BBB impairment. (C) Ex vivo autoradiographs show 18F-FET uptake 65 min after injection. (D) Summed PET images (18–61 min after injection) show 18F-FET accumulation. (Top) Representative brain from baseline group. (Middle) Representative brain from group receiving short-term bevacizumab treatment. (Bottom) Representative brain from group receiving long-term bevacizumab treatment.
Vascular staining revealed normal blood vessels in contralateral tissue in all 3 groups, whereas vessels in untreated tumors and tumors receiving short-term treatment were dense and larger than those in normal tissue. In tumors receiving long-term treatment, the number of vessels was considerably diminished, and the vessels were smaller (Fig. 2).
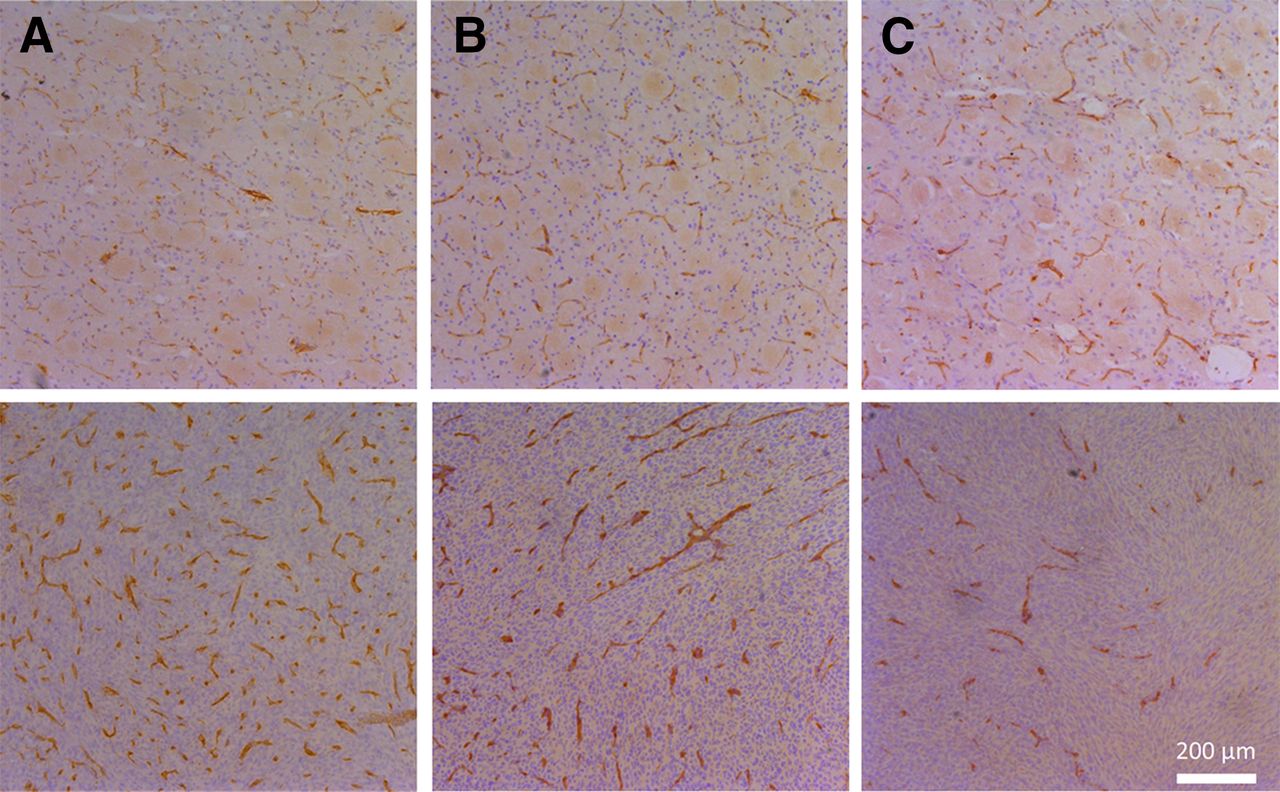
Blood vessel staining. (Top) Results of staining of blood vessel endothelia (brown) in contralateral tissue were similar for control group (A), group receiving short-term bevacizumab treatment (B), and group receiving long-term bevacizumab treatment (C). (Bottom) Tumor vessels in control group (A) and group receiving short-term bevacizumab treatment (B) were large and dense, whereas fewer and smaller vessels were detected in group receiving long-term bevacizumab treatment (C).
Using ANOVAs, we confirmed the stability of 18F-FET uptake shown by the TBRmean from AR (control, 2.04 ± 0.30; short-term treatment, 1.89 ± 0.08; long-term treatment, 1.89 ± 0.24; P = 0.419) and PET, as bevacizumab treatment did not significantly influence the factors TBRmean, TBRmax, and slope. The area under the curve for the group receiving long-term treatment was significantly smaller than that for the control group (P = 0.002) (Table 1). The tumor volume, as defined by the VOI, was smallest in the group receiving long-term treatment but, because of the great variance in tumor sizes, the difference was not significant.
PET-Derived Values
These results are underlined by the similarity of time–activity curves from 20 min after injection in all 3 groups, as shown in Figure 3. Bevacizumab treatment also did not influence 18F-FET uptake in normal brain tissue (Fig. 3).

Time–activity curves. Graph shows averaged time–activity curves and SDs for 18F-FET uptake (SUV) in all 3 treatment groups. Highest SDs for brain curves were superposed on lower SDs for every time point. Bevacizumab (BEV) treatment reduced tracer uptake in early uptake phase (up to 20 min after injection), but there were no significant differences among treatment groups in later phase.
Although the 18F-FET TBRmean and TBRmax remained unchanged with bevacizumab treatment, BBB permeability—as measured by EBD extravasation—decreased, depending on the duration of the treatment rather than the dose. A high dose (45 mg/kg) 48 h before the final scan (short-term treatment) resulted in a trend toward BBB restoration (control, 4.00 ± 2.01; short-term treatment, 2.43 ± 1.04), but only long-term treatment with 2 doses of bevacizumab (10 mg/kg) 2 and 9 d before the final scan had a significant impact on BBB permeability (control, 4.00 ± 2.01; long-term treatment, 1.73 ± 0.45; P = 0.014) (Fig. 4).

Influence of BBB restoration by bevacizumab (BEV) on 18F-FET TBR. Bars show trend toward decrease (P = 0.055) in EBD TBR after short-term treatment (st) with BEV and significant decrease (P = 0.004) after long-term treatment (lt), whereas 18F-FET TBR in PET and AR were constant. **P = 0.004.
DISCUSSION
PET using 18F-FET is increasingly being accepted as a complementary tool for brain tumor diagnostics and therapy monitoring. The influence of BBB disruption on 18F-FET uptake, however, is a matter of continued discussion because there is a significant correlation between contrast enhancement on MRI and 18F-FET or 11C-MET accumulation in brain tumors with different grades of malignancy (35,36). This correlation, however, is probably attributable to the fact that the degree of contrast enhancement on MRI on the one hand and 18F-FET or 11C-MET uptake on the other hand is more pronounced in malignant tumors than in low-grade tumors and leads to the assumption of a causal relationship between the parameters (37). Experimental studies have demonstrated that the uptake of 18F-FET by brain tumors is dominated by increased transport via transport system L for large neutral amino acids—namely, the subtypes LAT1 and LAT2—which are expressed at the intact BBB (38).
Therefore, a disruption of the BBB is not a prerequisite for intratumoral accumulation, and increased 18F-FET uptake has been reported in many low-grade gliomas without BBB leakage (8,9,39,40). As opposed to these observations, we hypothesized that if 18F-FET uptake were influenced to a major extent by passive tracer influx across the disrupted BBB, then a restoration of the BBB after bevacizumab treatment should lead to a reduction in tracer uptake similar to the reduction in EBD extravasation.
The results of the present study clearly refute this hypothesis. Although the BBB permeability of U87 tumors—as demonstrated by EBD extravasation—was clearly reduced after long-term bevacizumab therapy, there was no significant effect on the TBRmean and TBRmax of 18F-FET uptake in the U87 tumor model. Tumor size seemed to be smaller in the group receiving long-term treatment than in the control group or the group receiving short-term treatment, but the differences were not significant, consistent with the observation of limited reduction in tumor progression in other studies (29,30).
The results of the present study are in line with those of a previous study using the amino acid tracer 3H-MET and the artificial amino acid trans-1-amino-3-fluoro-1-14C-cyclobutanecarboxylic acid in the U87 tumor model (30). Therefore, the present study confirms the previous experimental and clinical finding that PET using 18F-FET and other amino acid tracers is able to disclose the phenomenon of pseudoprogression, which is a frequent diagnostic problem in conventional MRI during antiangiogenic therapy. This method may allow the earlier detection of treatment failure so that unnecessary adverse effects can be avoided.
Another important aspect of the present study was the influence of bevacizumab treatment on the time–activity curve of 18F-FET uptake. Several studies have demonstrated that evaluation of the time–activity curve of 18F-FET uptake in tumors may be helpful for estimating tumor aggressiveness (9–13). High-grade gliomas are characterized by an early peak in the time–activity curve, at about 10–15 min after tracer injection, followed by a decrease in 18F-FET uptake; the time–activity curve of low-grade gliomas (World Health Organization grade II) slightly and steadily increases (10,12). It has been suggested that the decrease in 18F-FET uptake in high-grade gliomas is influenced by facilitated backdiffusion of unbound tracer due to BBB leakage (12). The results of the present study indicated that restoration of the BBB by bevacizumab treatment did not influence the slope of the time–activity curve of 18F-FET uptake in the late phase of tracer uptake. However, bevacizumab treatment did have an influence on the early accumulation phase, which was delayed—especially in animals receiving long-term treatment—and which had a significant impact on the area under the curve (Table 1). This observation may reflect reduced vascularization (Fig. 2), as the signal from 18F-FET radioactivity in the blood pool was high during the first 15 min after injection (16). However, this possibility can be analyzed only by pharmacokinetic modeling, which was not available in our experimental setup.
Several experimental studies have already examined the usefulness of different PET tracers for monitoring antiangiogenic therapy (30). Beyond radiolabeled amino acids, the proliferation tracer 3′-deoxy-3′-18F-fluorothymidine (18F-FLT) has been investigated in 2 clinical trials (41,42). A reduction in 18F-FLT uptake after bevacizumab treatment had a high predictive value for the survival time of patients, but a limitation of this tracer is that BBB breakdown is a prerequisite for 18F-FLT uptake—and even high-grade gliomas with a high proliferation index may be 18F-FLT–negative if they lack contrast enhancement on MRI (24).
Finally, animal models may not correctly reflect the human situation. Although the human xenograft model may be more appropriate than rat glioma models, the biologic properties and growth patterns of implanted tumors differ from those of human tumors. For example, the time–activity curve of 18F-FET uptake in the U87 tumor model exhibited a plateau phase beyond 20 min after injection, whereas human glioblastomas usually show a decreasing time–activity curve in the late phase. Furthermore, for the specific issue in the present study, a cell line that was largely resistant to bevacizumab was selected. Therefore, the data should be considered with caution. Nevertheless, the experiments provide convincing evidence for the relationship of 18F-FET uptake and BBB permeability and confirm the observations in humans in previous studies (26,27).
CONCLUSION
The results of this experimental study suggested that monitoring of antiangiogenic therapy in glioblastomas with 18F-FET PET seems to be largely independent of BBB permeability and could solve the problem of the pseudoresponse in contrast-enhanced MRI. This method may allow the earlier detection of treatment failure so that overtreatment and unnecessary adverse effects can be avoided.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Michaela Bohlen, Melanie Heymann, and Larissa Grochowski for animal husbandry and Erika Wabbals, Silke Grafmüller, and Sascha Rehbein for technical assistance in the radiosynthesis of 18F-FET.
Footnotes
Published online Feb. 2, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 11, 2016.
- Accepted for publication December 26, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}