


Article Figures & Data
Figures
- FIGURE 1.
Typical factors and corresponding factor images associated with 82Rb (A) and 13N-ammonia (B) dynamic studies in same subject. AU = arbitrary units; MYO = whole myocardium.
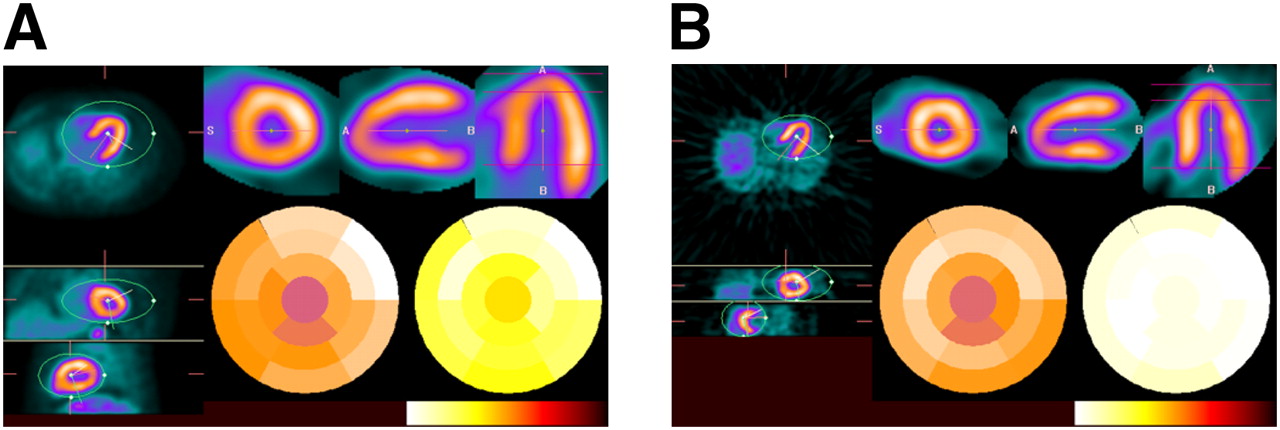
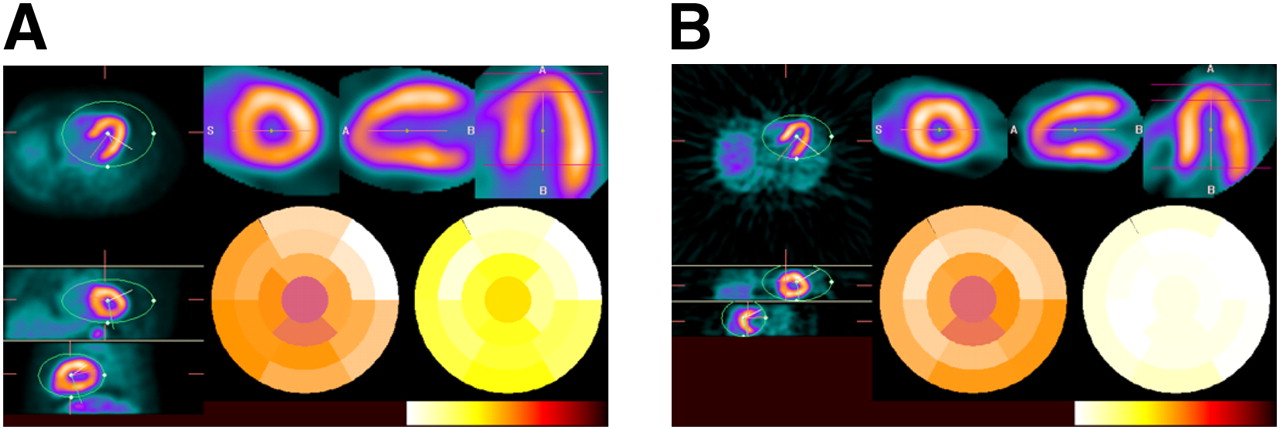
- FIGURE 2.
Transverse, coronal, and sagittal slices (left) as well as short-axis, long-vertical-axis, and horizontal-axis images (top right) of 82Rb (A) and 13N-ammonia (B) stress studies in same subject. Polar maps of relative perfusion (center) and absolute hyperemic MBF (right) are also shown (bottom right); white corresponds to highest values in color scale.
- FIGURE 3.
Intraobserver and GFADS variability of estimation of rest MBF and stress MBF with 82Rb. Mean values for flow from 4 repeated estimates are shown for one observer.
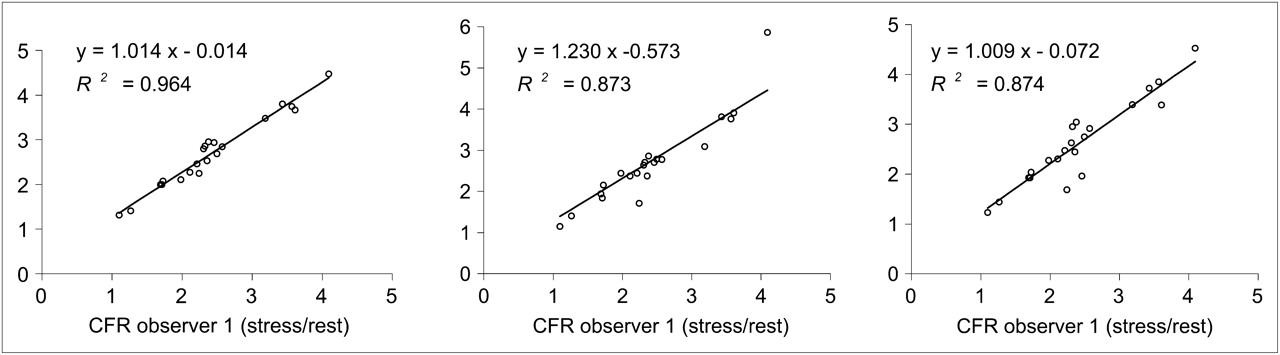
- FIGURE 4.
Interobserver variability of estimation of CFR with 82Rb.
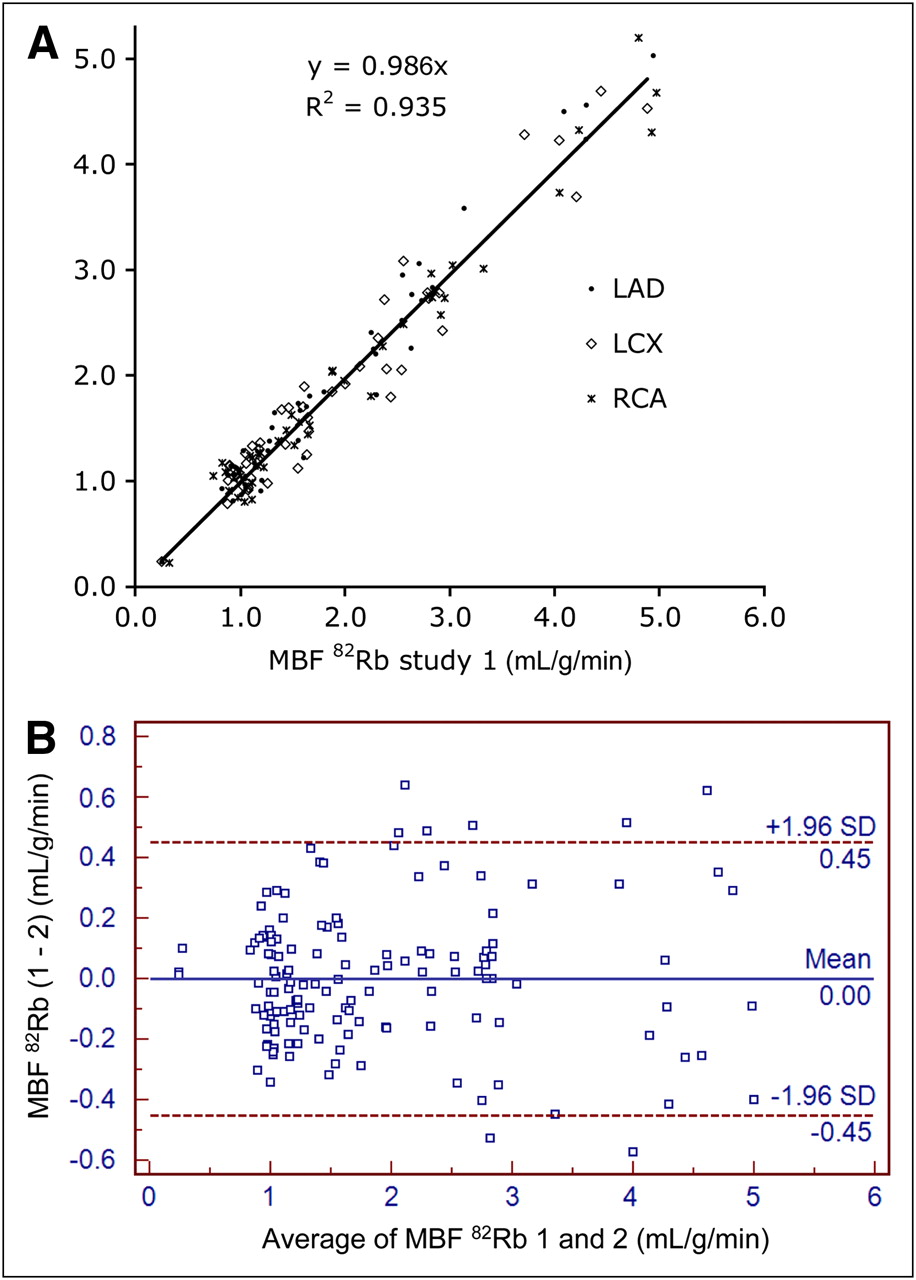
- FIGURE 5.
Reproducibility of rest MBF and stress MBF estimated with 82Rb at 2 visits. (A) Correlation plot of 2 MBF measurements. (B) Bland–Altman plot of 2 MBF measurements.
- FIGURE 6.
Comparison of rest MBF and stress MBF estimated with 82Rb and 13N-ammonia. (A) Correlation plot of 82Rb and 13N-ammonia MBF measurements. (B) Bland–Altman plot of 82Rb and 13N-ammonia MBF measurements. Bland–Altman plot illustrates slight overestimation of MBF at rest and underestimation during peak stress with 82Rb compared with 13N-ammonia.




Tables
Characteristic Reproducibility (n = 22) Accuracy (n = 20) Age (y) 48.0 ± 12.3 34.3 ± 11.6 Female/male ratio 11/11 12/8 Hypertension 4 1 Diabetes 2 0 Smoking 1 3 Dyslipidemia 5 4 Prior CAD 1 0 Prior MI 1 0 Chest pain 1 0 Chronic obstructive pulmonary disease 0 0 Data are reported as number of subjects unless otherwise indicated.
Reproducibility (mean ± SD, n = 22) Accuracy (mean ± SD, n = 20) Parameter 82Rb study 1 82Rb study 2 82Rb 13N ammonia Systemic hemodynamics HR at rest 65 ± 8 65 ± 9 64 ± 11 60 ± 9 Systolic BP at rest 135 ± 17 134 ± 16 126 ± 21 108 ± 8 Mean arterial BP at rest 91 ± 11 92 ± 21 84 ± 14 80 ± 13 RPP at rest 8,682 ± 1,368 8,717 ± 1,575 8,100 ± 2,423 6,588 ± 1,056 Peak HR 80 ± 14 83 ± 11 82 ± 16 87 ± 24 Peak systolic BP 139 ± 23 127 ± 20 124 ± 19 110 ± 16 Peak mean arterial BP 93 ± 15 84 ± 16 81 ± 13 73 ± 31 Peak RPP 11,053 ± 2,657 10,414 ± 2,137 10,165 ± 2,373 9,586 ± 2,976 Coronary hemodynamics MBF at rest 1.13 ± 0.19 1.09 ± 0.18 0.83 ± 0.15 0.61 ± 0.14 MBF at rest, corrected 1.18 ± 0.32 1.15 ± 0.27 0.91 ± 0.23 0.79 ± 0.22 Peak MBF during stress 2.81 ± 1.02 2.71 ± 1.11 1.72 ± 0.41 1.92 ± 0.28 CFR 2.51 ± 0.89 2.40 ± 0.96 2.00 ± 0.67 2.58 ± 0.68 CVR at rest 84.8 ± 23.5 85.1 ± 28.8 103.2 ± 44.7 102.1 ± 34.1 Peak CVR during stress 37.8 ± 16.0 36.9 ± 17.45 51.4 ± 19.6 41.9 ± 4.2 HR = heart rate, in bpm; BP = blood pressure, in mm Hg; CVR = coronary vascular resistance, which is calculated as mean arterial BP/MBF and reported in mm Hg/mL/g/min.
RPP is calculated as heart rate (in bpm) × systolic blood pressure (in mm Hg). MBF is reported in mL/g/min. CFR is calculated as peak MBF during stress/MBF at rest.
- TABLE 3
Per–Vascular Territory Analysis of Reproducibility of MBF, CFR, and Coronary Vascular Resistance (CVR)
82Rb visit 1 82Rb visit 2 Parameter LAD LOX RCA LAD LOX RCA MBF at rest 0.86 ± 0.16 0.89 ± 0.15 0.90 ± 0.18 0.83 ± 0.15 0.85 ± 0.15 0.87 ± 0.14 MBF at rest, corrected 0.91 ± 0.22 0.94 ± 0.20 0.95 ± 0.23 0.90 ± 0.23 0.92 ± 0.22 0.94 ± 0.20 Peak MBF during stress 1.87 ± 0.72 1.86 ± 0.66 1.92 ± 0.77 1.80 ± 0.63 1.84 ± 0.64 1.86 ± 0.64 CFR 2.10 ± 0.76 2.00 ± 0.61 2.09 ± 0.79 2.03 ± 0.65 2.04 ± 0.70 1.99 ± 0.61 CVR at rest 108.36 ± 34.74 103.84 ± 30.10 105.80 ± 38.63 110.04 ± 40.24 107.52 ± 39.99 104.56 ± 40.40 Peak CVR during stress 56.83 ± 23.35 56.17 ± 21.76 55.19 ± 21.38 53.16 ± 26.50 51.48 ± 24.04 50.42 ± 21.35 Data are reported as mean ± SD. MBF is reported in mL/g/min. CFR is calculated as peak MBF during stress/MBF at rest. CVR is calculated as mean arterial blood pressure/MBF and reported in mm Hg/mL/g/min.
- TABLE 4
Per–Vascular Territory Analysis of Accuracy of MBF, CFR, and Coronary Vascular Resistance (CVR)
82Rb 13N-ammonia Parameter LAD LOX RCA LAD LOX RCA MBF at rest 0.80 ± 0.13 0.82 ± 0.18 0.88 ± 0.18 0.61 ± 0.14 0.62 ± 0.18 0.60 ± 0.16 MBF at rest, corrected 0.90 ± 0.24 0.91 ± 0.25 0.98 ± 0.25 0.78 ± 0.22 0.81 ± 0.29 0.77 ± 0.22 Peak MBF during stress 1.70 ± 0.37 1.66 ± 0.36 1.82 ± 0.50 1.97 ± 0.33 1.89 ± 0.29 1.90 ± 0.30 CFR 2.01 ± 0.69 1.93 ± 0.65 1.97 ± 0.76 2.66 ± 0.72 2.55 ± 0.77 2.60 ± 0.64 CVR at rest 105.88 ± 48.38 103.95 ± 45.80 97.22 ± 44.38 102.88 ± 34.05 100.28 ± 36.87 106.92 ± 37.14 Peak CVR during stress 52.29 ± 20.88 52.86 ± 18.61 49.74 ± 19.86 40.48 ± 2.92 43.01 ± 5.17 42.41 ± 5.49 Data are reported as mean ± SD. MBF is reported in mL/g/min. CFR is calculated as peak MBF during stress/MBF at rest. CVR is calculated as mean arterial blood pressure/MBF and reported in mm Hg/mL/g/min.
- TABLE 5
Spearman ρ Nonparametric Correlations Among 82Rb PET Estimates of MBF Obtained by 4 Observers
Spearman ρ Observer 1 Observer 2 Observer 3 Observer 4 Observer 1 1.000 0.935* 0.845* 0.857* Observer 2 0.935* 1.000* 0.891* 0.890* Observer 3 0.845* 0.891* 1.000 0.827* Observer 4 0.857* 0.890* 0.827* 1.000 ↵* Correlation was significant at 0.01 level (2-tailed test).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Coronary Microvascular Function Following Severe Preeclampsia
- Intermuscular Adiposity is Associated with Coronary Microvascular Dysfunction Independently of Body Mass Index and Modifies its Effect on Adverse Cardiovascular Outcomes
- Discovery of cardiac imaging biomarkers by training neural network models across diagnostic modalities
- Cardiovascular Imaging Techniques to Assess Microvascular Dysfunction
- Structural and Practical Identifiability of Dual-input Kinetic Modeling in Dynamic PET of Liver Inflammation
- Myocardial Scar But Not Ischemia Is Associated With Defibrillator Shocks and Sudden Cardiac Death in Stable Patients With Reduced Left Ventricular Ejection Fraction
- Coronary Microvascular Dysfunction and Cardiovascular Risk in Obese Patients
- Reduced Myocardial Flow Reserve by Positron Emission Tomography Predicts Cardiovascular Events After Cardiac Transplantation
- Integrated Noninvasive Physiological Assessment of Coronary Circulatory Function and Impact on Cardiovascular Mortality in Patients With Stable Coronary Artery Disease
- Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging
- Ranolazine in Symptomatic Diabetic Patients Without Obstructive Coronary Artery Disease: Impact on Microvascular and Diastolic Function
- Diagnostic Performance of Resting and Hyperemic Invasive Physiological Indices to Define Myocardial Ischemia: Validation With 13N-Ammonia Positron Emission Tomography
- Excess Cardiovascular Risk in Women Relative to Men Referred for Coronary Angiography Is Associated With Severely Impaired Coronary Flow Reserve, Not Obstructive Disease
- Characterization of 3-Dimensional PET Systems for Accurate Quantification of Myocardial Blood Flow
- Prognostic Value of Coronary Flow Reserve in Patients with Dialysis-Dependent ESRD
- Effect of Outflow Tract Contributions to 82Rb-PET Global Myocardial Blood Flow Computations
- Interaction of Impaired Coronary Flow Reserve and Cardiomyocyte Injury on Adverse Cardiovascular Outcomes in Patients Without Overt Coronary Artery Disease
- Global Coronary Flow Reserve Is Associated With Adverse Cardiovascular Events Independently of Luminal Angiographic Severity and Modifies the Effect of Early Revascularization
- Comparison and Prognostic Validation of Multiple Methods of Quantification of Myocardial Blood Flow with 82Rb PET
- Quantification of Myocardial Blood Flow in Absolute Terms Using 82Rb PET Imaging: The RUBY-10 Study
- Effects of Sex on Coronary Microvascular Dysfunction and Cardiac Outcomes
- Preserved Coronary Flow Reserve Effectively Excludes High-Risk Coronary Artery Disease on Angiography
- Multisoftware Reproducibility Study of Stress and Rest Myocardial Blood Flow Assessed with 3D Dynamic PET/CT and a 1-Tissue-Compartment Model of 82Rb Kinetics
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- Association Between Coronary Vascular Dysfunction and Cardiac Mortality in Patients With and Without Diabetes Mellitus
- Coronary Vascular Dysfunction and Prognosis in Patients With Chronic Kidney Disease
- Comparison of Clinical Tools for Measurements of Regional Stress and Rest Myocardial Blood Flow Assessed with 13N-Ammonia PET/CT
- Stress Myocardial Perfusion Imaging for Assessing Prognosis: An Update
- Improved Cardiac Risk Assessment With Noninvasive Measures of Coronary Flow Reserve
- Clinical Value of Absolute Quantification of Myocardial Perfusion With 15O-Water in Coronary Artery Disease
- Quantitative Relationship Between the Extent and Morphology of Coronary Atherosclerotic Plaque and Downstream Myocardial Perfusion
- Impaired Myocardial Flow Reserve on Rubidium-82 Positron Emission Tomography Imaging Predicts Adverse Outcomes in Patients Assessed for Myocardial Ischemia
- Leaving Relativity Behind: Quantitative Clinical Perfusion Imaging
- Prediction of Short-Term Cardiovascular Events Using Quantification of Global Myocardial Flow Reserve in Patients Referred for Clinical 82Rb PET Perfusion Imaging
- Quantitative PET Measurements of Myocardial Blood Flow in Young, Healthy Volunteers: What Should We Expect?
- Simplified Quantification of Myocardial Flow Reserve with flurpiridaz F 18: Validation with Microspheres in a Pig Model
- Cardiac PET: A Versatile, Quantitative Measurement Tool for Heart Failure Management
- Cardiac Positron Emission Tomography/Computed Tomography Imaging Accurately Detects Anatomically and Functionally Significant Coronary Artery Disease
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- Low-Dose Quantitative Myocardial Blood Flow Imaging Using 15O-Water and PET Without Attenuation Correction