


Abstract
18F-FDG uptake in the thymus, mainly related to hyperplasia after chemotherapy, has been described. Thymic uptake can challenge the accurate assessment of cancer patients by 18F-FDG imaging. The present study defines the incidence, patterns, and intensity of thymic 18F-FDG uptake in relationship to age and time after treatment in a large cohort of patients. Methods: A total of 559 consecutive 18F-FDG PET/CT studies in 160 patients (86 men, 74 women; age, 3–40 y) performed at baseline, during treatment, at the end of treatment, and during follow-up were retrospectively reviewed. PET/CT studies were assessed for the presence or absence (T+ or T−, respectively), pattern, and intensity (SUVmax) of increased 18F-FDG uptake in the anterior mediastinum, localized by the CT component to the thymus. The overall incidence of 18F-FDG avidity in the thymus in relationship to the patient's age and time after treatment administration were statistically evaluated. Results: There were 137 of 559 T+ studies (25%), with equal sex distribution. T+ studies were found in significantly younger patients (20.6 ± 9.3 y vs. 27.4 ± 8.4 y, P < 0.001). Most T+ patients (60%) showed an inverted V pattern of thymic uptake, with additional unilateral mediastinal extension in 24% and focal midline uptake in 16% of studies. T+ studies were encountered in 80% of patients younger than 10 y, compared with 8% of patients in the 31- to 40-y age group. There were 17% T+ studies at baseline, 6% during treatment, 8% at the end of treatment, and 27%–40% during follow-up. The average SUVmax of thymic 18F-FDG uptake was 3.73 ± 1.22. Conclusion: Thymic 18F-FDG uptake was found in 28% of the present study population, more frequently after treatment. T+ patients were significantly younger. Thymic uptake was found in 73% of untreated patients up to the age of 13 y and in 8% of patients in the fourth decade of life. Knowledge of this age- and treatment-related incidence of physiologic thymic 18F-FDG avidity can reduce the number of potential pitfalls in reporting PET/CT studies in cancer patients.
Mediastinal enlargement detected on CT in cancer patients after chemotherapy can represent benign thymic hyperplasia or malignancy, including treatment failure, disease recurrence, metastatic disease, or a second primary neoplasm (1). Thymic hyperplasia may also occur in several additional clinical settings unrelated to cancer and previous treatment, such as after discontinuation of corticosteroid therapy, in patients with hyperthyroidism, during recovery from burn injuries, in patients with infections, and after cardiovascular surgery (1). Physiologic 18F-FDG uptake in the thymus has been reported in children and in sporadic cases in adults after chemotherapy (2). Thymic 18F-FDG uptake in cancer patients is most probably related to hyperplasia, which occurs as a rebound phenomenon during the recovery phase after chemotherapy.
The present study was prompted by the visualization of increased mediastinal 18F-FDG activity, suggesting thymic uptake by its pattern and location, both in children and in adults with cancer. The study was designed to define the incidence, patterns, and intensity of thymic 18F-FDG activity in relationship to patient age and treatment status in a large study cohort of patients.
MATERIALS AND METHODS
Patient Population
This study is a retrospective analysis of 160 consecutive patients, aged 40 y and younger (mean age, 26.2 y). The study population included 86 male and 74 female patients who underwent 559 18F-FDG PET/CT studies between 2001 and 2002. The patients were evaluated for Hodgkin (n = 59) and non-Hodgkin lymphoma (n = 44), sarcoma (n = 13), melanoma (n = 6), carcinoma of the cervix and colon (n = 5 each), other malignancies (n = 19), and benign processes (n = 9). A total of 101 patients (63%) underwent multiple PET/CT evaluations (range, 2–11), and 59 patients (37%) underwent a single study.
Of the 559 studies, 66 were performed at presentation, 78 during treatment, 63 at the end of treatment, and 352 during follow-up after the completion of therapy. Follow-up studies were classified into 4 categories: less than 6 mo, 6–11 mo, 12–24 mo, and more than 24 mo after the completion of treatment. None of the patients had diabetes mellitus. For pediatric patients younger than 18 y, parental informed consent was obtained for the PET/CT study and clinical follow-up.
Imaging Technique
Patients were instructed to fast, except for noncaloric fluid intake, for at least 5 h before the injection of 18F-FDG (370–555 MBq [10–15 mCi]). Children were administered a weight-adjusted dose of 18F-FDG (5.328 MBq/kg [0.144 mCi/kg]). Whole-body PET and non–contrast-enhanced CT were acquired consecutively 60–90 min after the injection of 18F-FDG, using a PET/CT system (Discovery LS; GE Healthcare) combining a third-generation multislice spiral CT with a dedicated full-ring PET scanner with bismuth germinate crystals. Non–breath-hold CT was performed at 80 mAs and 140 kV using a 4-slice device (LS-Light Speed; GE Healthcare). The CT protocol included a beam collimation of 20 mm (4 rows × 5 mm), with a helical pitch of 0.75:1 and a speed of 15.00 mm/rotation. 18F-FDG PET images with a 4-mm slice thickness were acquired and reconstructed iteratively using ordered-subset expectation maximization software. CT data were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images.
Image Interpretation
All PET/CT studies were retrospectively reviewed for the presence of increased 18F-FDG activity in the upper anterior mediastinum, localized on the CT component of the study to the thymus (identified by its shape, regular contours, and separation from other mediastinal structures or masses) (Fig. 1). Patients and studies were classified according to the presence (T+) or absence (T−) of increased 18F-FDG thymic uptake. Patterns of the 18F-FDG–avid thymus were recorded. The intensity of thymic 18F-FDG uptake was measured in 133 of the 137 T+ studies as standardized uptake value (SUVmax) using the commercially available software provided by the manufacturer. A circular region of interest was drawn on the transaxial slice showing the best definition of thymic uptake. In 4 studies, SUV could not be measured because of faulty archiving of the studies.
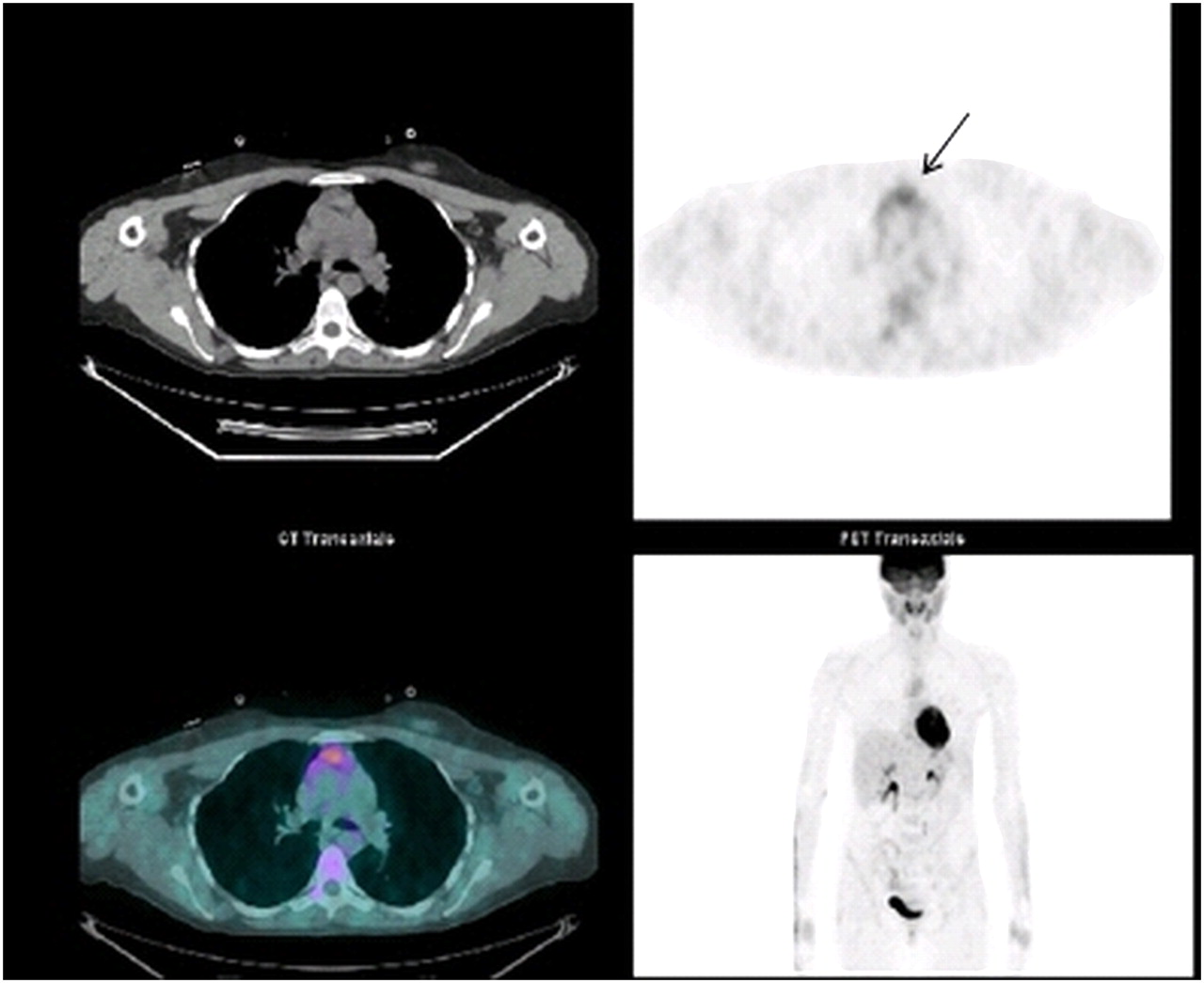
Physiologic 18F-FDG uptake in thymus in 34-y-old female patient with Hodgkin disease assessed during routine follow-up 13 mo after completion of chemotherapy. Note focal midline pattern of uptake with extension to right (arrow), with SUVmax of 3.8.
Data Analysis
T+ or T− thymic 18F-FDG uptake was analyzed in relationship to patients' age and classified into 4 groups by decades (0–10, 11–20, 21–30, and 31–40 y). The incidence and intensity (SUVmax) of thymic 18F-FDG uptake in relationship to treatment (before, during, and after) was recorded. The physiologic nature of 18F-FDG uptake in the thymus was confirmed by the absence of malignancy in this same location for a long-term clinical and imaging follow-up (33.3 ± 21 mo). The times of first visualization and of disappearance of thymic 18F-FDG uptake in patients who had multiple studies were recorded.
Statistical Analysis
The mean age of patients with T+ and T− studies was compared using the nonparametric Mann–Whitney U test. Differences in SUVmax of 18F-FDG uptake in the thymus during treatment, at the end of treatment, and at follow-up were compared using the independent t test method.
RESULTS
18F-FDG uptake in the thymus was identified in 44 of 160 patients (28%) and in 137 of the 559 studies (25%).
The mean age of the 44 patients with T+ studies was significantly lower than that of the 116 patients with T− studies (20.6 ± 9.3 y vs. 27.4 ± 8.4 y, P < 0.001). Thymic 18F-FDG uptake was found in 28 of the 35 studies (80%) in patients younger than 10 y, in 58 of the 114 studies (51%) in patients aged 11–20 y, and in 51 of the 410 studies (12%) in young adults aged 20–40 y, including 34 of 193 studies (18%) in patients younger than 30 y and 17 of 217 studies (8%) in patients aged 30–40 y (Table 1).
Incidence and Age-Related Distribution of 18F-FDG Uptake in Thymus in 559 PET/CT Studies
Before the start of therapy, there were 11 of 66 T+ studies (17%), including 3 patients younger than and 8 patients older than (73%) 13 y (range, 3–35 y). Of the studies performed on treated patients, 132 of 519 studies (25%) were T+. Thymic uptake occurred in 6% of studies performed during treatment, in 8% of studies performed at the completion of treatment, and in 33% of studies performed during follow-up. The first appearance of a T+ study was seen in 11 of 44 patients (25%) at the time of diagnosis and in 26 of 44 patients (59%) during follow-up after the completion of treatment. The distribution of thymic uptake in relationship to treatment is shown in Table 2, and thymic uptake in relationship to both age and treatment is shown in Table 3.
Physiologic 18F-FDG Uptake in Thymus in Relationship to Treatment Administration
Frequency of T+ Studies According to Patient Age and Treatment Status
Sequential PET/CT studies were performed on 30 of the 44 T+ patients (68%) and showed disappearance of the thymic uptake in 9 of 30 patients (30%) in follow-up studies performed at 10–24 mo after completion of treatment. In 21 patients (70%), follow-up studies remained T+ for a period of 12–36 mo.
During a follow-up period of up to 85 mo, none of the patients had evidence of malignancy in the anterior mediastinum, excluding one 16-y-old patient with soft-tissue sarcoma of the diaphragm. This patient showed uptake in a mediastinal mass in a different location from the previously detected hyperplasic 18F-FDG–avid thymus, diagnosed as recurrent disease.
Thymic uptake showed an inverted V or triangular pattern in 60% of T+ studies. Uptake was unilateral, extending mainly into the right mediastinum in 24% of the studies, and was a focal, midline 18F-FDG–avid area in 16% of the studies (Fig. 2).

Patterns of physiologic 18F-FDG uptake in thymus: classic inverted V triangular (A), unilateral right extension (B), and focal midline (C).
Overall intensity of thymic 18F-FDG uptake had a measured SUVmax of 3.73 ± 1.22. SUVmax measurements were statistically significantly lower in studies performed during treatment and at the end of the treatment, compared with SUVmax measurements in studies performed before treatment and during follow-up (P < 0.05 or lower) (Table 4).
Intensity of Physiologic 18F-FDG Uptake in Thymus Measured by SUVmax in Relationship to Treatment Administration
DISCUSSION
Thymic 18F-FDG uptake in the anterior mediastinum may represent a potential pitfall in the assessment of PET/CT studies in patients with malignancy, mimicking or masking 18F-FDG–avid tumor sites (3,4). Cancer-related conditions such as a failure of treatment with viable residual tumor, recurrence in the mediastinum, and second primary malignancy can result in 18F-FDG–avid mediastinal enlargement and need to be considered in the differential diagnosis of increased tracer activity associated with benign thymic hyperplasia. 18F-FDG uptake in the normal or hyperplasic thymus after chemotherapy is a relatively common finding in the pediatric population with cancer (5).
Embryologically, the thymus originates from the third branchial pouch on both sides; it fuses in the midline and migrates from the pharynx to the anterior mediastinum (6). Thymic tissue can persist anywhere along its path of migration (7). Although unusual locations in the neck and in the superior and posterior mediastinum between the great thoracic vessels have been previously reported (8), in the current series the thymus in all patients was identified in its characteristic anterior superior mediastinal location.
From birth, the thymus grows slowly, reaching its peak weight at puberty, followed by a decrease in size and gradual replacement of its glandular tissue by fatty infiltration (9). Total fatty involution of the thymus occurs around the age of 40 y, when only about 5% of residual thymic tissue is retained (9,10). Thus, we set the upper age limit of the patient population evaluated in the current series at 40 y.
In children, the thymus has a quadrilateral shape, which then changes to a triangular or arrowhead appearance (11). Although this classic triangular or inverted V shape of thymic 18F-FDG uptake was observed in 60% of patients in the present series, unilateral (mainly right mediastinal extension) and focal midline uptake representing additional patterns of tracer activity was found in 40% of patients.
Change in size of the thymus in response to stress has been previously described and is related to, among other causes, the presence of sepsis, congenital heart diseases, administration of steroids, radiotherapy, or cytotoxic effects of chemotherapy (12). Regrowth of the thymus occurs after recovery or after completion of steroid therapy or chemotherapy (13). An increase in thymic volume of more than 50%, compared with at baseline, is defined as rebound caused by overgrowth of normal thymic elements and tissue hyperplasia (14).
18F-FDG uptake in thymic hyperplasia has been previously described mainly in children and after treatment (2,15). Knowledge of the variable 18F-FDG PET/CT patterns and the overall incidence of 18F-FDG–avid thymic hyperplasia and its relationship to specific patient groups is clinically significant. False-positive 18F-FDG PET/CT results leading to further invasive diagnostic procedures and, at times, unnecessary therapy can be avoided. The present study addresses the issue of potential false-positive findings in a large patient population.
Physiologic thymic 18F-FDG uptake was found in 28% of cancer patients younger than 40 y, with no sex prevalence. This percentage was slightly higher than the previously reported range of 11%–25% thymic enlargement demonstrated on CT (14,16) and similar to the 11%–36% reported for 67Ga uptake (17–19). This incidence is, however, lower than the previously reported 31%–50% for 18F-FDG PET, most probably because previous studies included mainly children and adolescents, with none or few young adult patients (2,10,15,20). 18F-FDG uptake in the thymus has been previously associated mainly with treatment-related hyperplasia in children with cancer and has been only sporadically described in adult patients after chemotherapy (2,21). Brink et al. (2) reported thymic hyperplasia in 5% of adults after chemotherapy using 18F-FDG PET; in the present study, however, the incidence of 18F-FDG avidity of the thymus in young adults was higher. Although as a group the T+ population was significantly younger, the incidence reached 12% in patients in the 20- to 40-y age group; furthermore, 18F-FDG uptake in the thymus was found in a previously unknown 8% of patients in the fourth decade of life. A slow process of fatty infiltration of the thymus can be a possible explanation for the presence of 18F-FDG uptake in older patients (10). An additional reason for the higher incidence of T+ studies in adult patients may be related to the use of PET/CT, compared with PET only, in previously published studies. In the present study, a site of low-level tracer activity that localized to the thymus on CT was defined as T+. Similar findings may have been ignored on PET stand-alone images.
Although 18F-FDG uptake by the thymus has been reported mainly after chemotherapy, in the present study it was also found in 17% of studies performed at presentation, before any treatment. Furthermore, in the group of untreated T+ patients, 73% were older than 13 y, which was previously suggested as the upper age limit of physiologic thymic uptake because the metabolic activity of the thymus ceases at puberty (15).
Thymic activity is suppressed early during chemotherapy (14,16). Current results show a lower incidence of 6% of thymic uptake and a lower SUVmax in studies performed during treatment, compared with baseline studies and mainly with findings after the completion of chemotherapy. A total of 40% of the T+ studies were seen early during follow-up (Table 2), whereas in previous reports the higher incidence of 18F-FDG–avid thymus was found as a rule later during follow-up (12,22,23). There were no significant changes in either incidence or intensity of uptake when comparing serial studies performed on the same patient.
Because of bolstered cell-mediated immunity, thymic hyperplasia has been associated with good prognosis (6,12). Up to 93% of patients with thymic hyperplasia were free of disease, compared with 78% of patients without thymic hyperplasia (16). In the present study, 43 of 44 T+ patients had no further evidence of malignancy in the mediastinum for a long-term follow-up period.
The intensity of thymic 18F-FDG uptake had a mean SUVmax of 3.73 ± 1.22 and was higher than 4 in 44% of patients, all evaluated during follow-up. Previous studies performed on stand-alone PET devices have reported thymic SUV measurements in the range of 1.8–2.7 and have defined values lower than 4 as being most consistent with benign thymic processes (1,5,24,25).
CONCLUSION
The results of the present study indicate that physiologic 18F-FDG uptake in the thymus is not limited or specific to the pediatric patient population; it can be also seen in a relatively large number of adult patients and before any treatment. Knowledge of the incidence and patterns of 18F-FDG thymic uptake and awareness of the subsets of patients and timing when physiologic tracer activity may be encountered can be of clinical consequence, improving the diagnostic accuracy when interpreting mediastinal 18F-FDG–avid foci in patients with cancer.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 28, 2008.
- Accepted for publication February 23, 2009.





{kind=link}
{kind=link}