


Visual Abstract

Abstract
We hypothesized that 18F-FDG PET/MRI would reveal thymus activation in children after coronavirus disease 2019 (COVID-19) vaccination. Methods: We retrospectively analyzed the 18F-FDG PET/MRI scans of 6 children with extrathoracic cancer before and after COVID-19 vaccination. We compared pre- and postvaccination SUVmax, mean apparent diffusion coefficient, and size of the thymus and axillary lymph nodes using a paired t test. Results: All 6 patients showed increased 18F-FDG uptake in the axillary lymph nodes after vaccination (P = 0.03). In addition, these patients demonstrated increased 18F-FDG uptake in the thymus. When compared with baseline, the postvaccination scans of these patients demonstrated an increased mean thymic SUV (P = 0.02), increased thymic size (P = 0.13), and decreased thymic mean apparent diffusion coefficient (P = 0.08). Conclusion: 18F-FDG PET/MRI can reveal thymus activation in addition to local lymph node reactions in children after COVID-19 vaccination.
The coronavirus disease 2019 (COVID-19) pandemic sparked the rapid development and deployment of messenger RNA (mRNA) vaccines to millions of people, including children (1). Recent efforts to understand the immune response to mRNA vaccines revealed germinal center responses in axillary lymph nodes (2). In adults, an increased size and metabolic activity of axillary lymph nodes have been described after COVID-19 vaccination (3). A retrospective study showed that 54% (75/140) of adult patients had 18F-FDG–avid lymph nodes ipsilateral to the mRNA vaccine injection site on 18F-FDG PET/CT scans (4). Similarly, a large nationwide cohort study reported that 46% of vaccinated patients (332/728) had 18F-FDG–avid axillary lymph nodes (5).
In patients with cancer, an increase in the size and metabolic activity of lymph nodes can indicate tumor recurrence or progression and play an important role in guiding treatment decisions. Several case reports have demonstrated that vaccine-related lymphadenopathy may confound disease assessment in oncology patients such as those with breast cancer (6), metastatic melanoma (7,8), or Hodgkin lymphoma (9). Therefore, it is important to understand typical imaging findings that allow differentiation of vaccination from cancer-related lymphadenopathy.
COVID-19 vaccinations were initially Food and Drug Administration–approved for adults only and then were extended to children and teenagers. Unfortunately, our knowledge of postvaccination 18F-FDG PET imaging findings in children and young adults remains limited. Experimental studies have demonstrated strong T-cell activation in response to mRNA vaccines (10). Since children have T-cell–rich thymus tissue (11), we hypothesized that 18F-FDG PET/MRI would reveal an increased metabolic activity in the thymus in addition to that in the local lymph nodes after COVID-19 vaccination.
MATERIALS AND METHODS
Study Design
This was a secondary analysis of medical imaging data obtained as part of a retrospective study on pediatric cancer staging with whole-body 18F-FDG PET/MRI, which was approved by our institutional review board (approval 48854). The inclusion criteria included children or young adults diagnosed with cancer, receipt of at least 1 dose of the COVID-19 vaccine, and completion of at least 2 18F-FDG PET/MRI examinations, one before and one after vaccination. The exclusion criteria involved any instances of nonsimultaneous 18F-FDG PET/MRI. We included 6 children and young adults: 5 female and 1 male, with a mean age (±SD) of 13.67 ± 3.67 y (range, 10–19 y). All 6 patients had an extrathoracic malignancy.
18F-FDG PET/MRI Protocol
All patients underwent clinical standard 18F-FDG PET/MRI studies before and after COVID-19 vaccination. The scans were obtained on average 49.83 ± 45.67 d after the most recent vaccination dose (range, 6–121 d). All patients received the Pfizer-BioNTech vaccine. Of the 6 patients, 2 received a total of 3 intramuscular vaccination doses at separate intervals, 2 were administered 2 doses of vaccine, and 2 received a single vaccination dose. All vaccinations were completed before the postvaccination 18F-FDG PET/MRI scan. Before each PET imaging study, the patients fasted for at least 6 h. The serum glucose level at the time of 18F-FDG injection was less than 120 mg/dL. 18F-FDG PET/MR images were acquired 60–70 min after intravenous administration of 18F-FDG (3–5 MBq/kg of body weight), using a 3-T PET/MRI scanner (Signa; GE Healthcare). The PET data acquisition time was 3 min 30 s per bed position (89 slices per bed position) for 5–9 bed positions.
18F-FDG PET images were reconstructed using ordered-subset expectation maximization with 2 iterations and 28 subsets. A 2-point Dixon sequence was used for attenuation correction of the PET/MR images. The obtained 18F-FDG PET images were then color-encoded and fused with MRI scans using MIM software (version 7.0.5; MIM Software Inc.).
MRI included an axial contrast-enhanced T1-weighted liver acquisition with volume acquisition (repetition time, 4.2 ms; echo time, 1.7 ms; fractional anisotropy, 15; slice thickness, 3.4 mm) for coregistration with 18F-FDG PET data, as well as axial diffusion-weighted images (repetition time, 7,824 ms; echo time, 56 ms; b values, 50 and 800 s/mm2; slice thickness, 6 mm). The apparent diffusion coefficient (ADC) maps were automatically generated by the software.
Image Analysis
One board-certified radiologist and 1 board-certified nuclear medicine physician jointly evaluated the original and fused whole-body 18F-FDG PET/MRI and diffusion-weighted MRI scans and determined the size, metabolic activity, and restricted diffusion of the axillary lymph nodes and thymus in each patient. The readers were not aware of the clinical data or vaccination status of the patient while analyzing images. On 18F-FDG PET images, a fixed SUV scale (threshold, 42%) and color table were used. An increased 18F-FDG uptake was defined as focal tracer uptake higher than that of the mediastinal blood pool. The SUVmax was measured by placing a 3-dimensional volume of interest in the thymus and lymph nodes. The longest and shortest transverse diameters of the thymus were calculated as well.
For analysis of diffusion-weighted MRI, mean ADC values were measured through operator-defined regions of interests. All measurements were obtained using MIM software (version 7.0.5) and OsiriX software (version 10.0, 64 bits; Pixmeo).
Statistical Analysis
Statistical analysis was performed with Microsoft Excel. Continuous data are presented as mean ± SD. The 2-tailed paired t test was used to compare differences in the SUVmax and mean ADC of the axillary lymph nodes and thymus before and after vaccination, as well as changes in thymic size. A P value of less than 0.05 was considered significant.
RESULTS
Evaluation of 6 patients revealed uniformly normal axillary lymph nodes and thymus at baseline, with a metabolic activity below that of the mediastinal blood pool. After COVID-19 vaccination, there was a marked increase in the metabolic activity in the ipsilateral axillary lymph nodes across all patients (Fig. 1). The mean SUVmax of the axillary lymph nodes increased by a factor of 3.0, from 0.87 ± 0.44 before vaccination to 2.61 ± 1.21 after vaccination (P = 0.03).

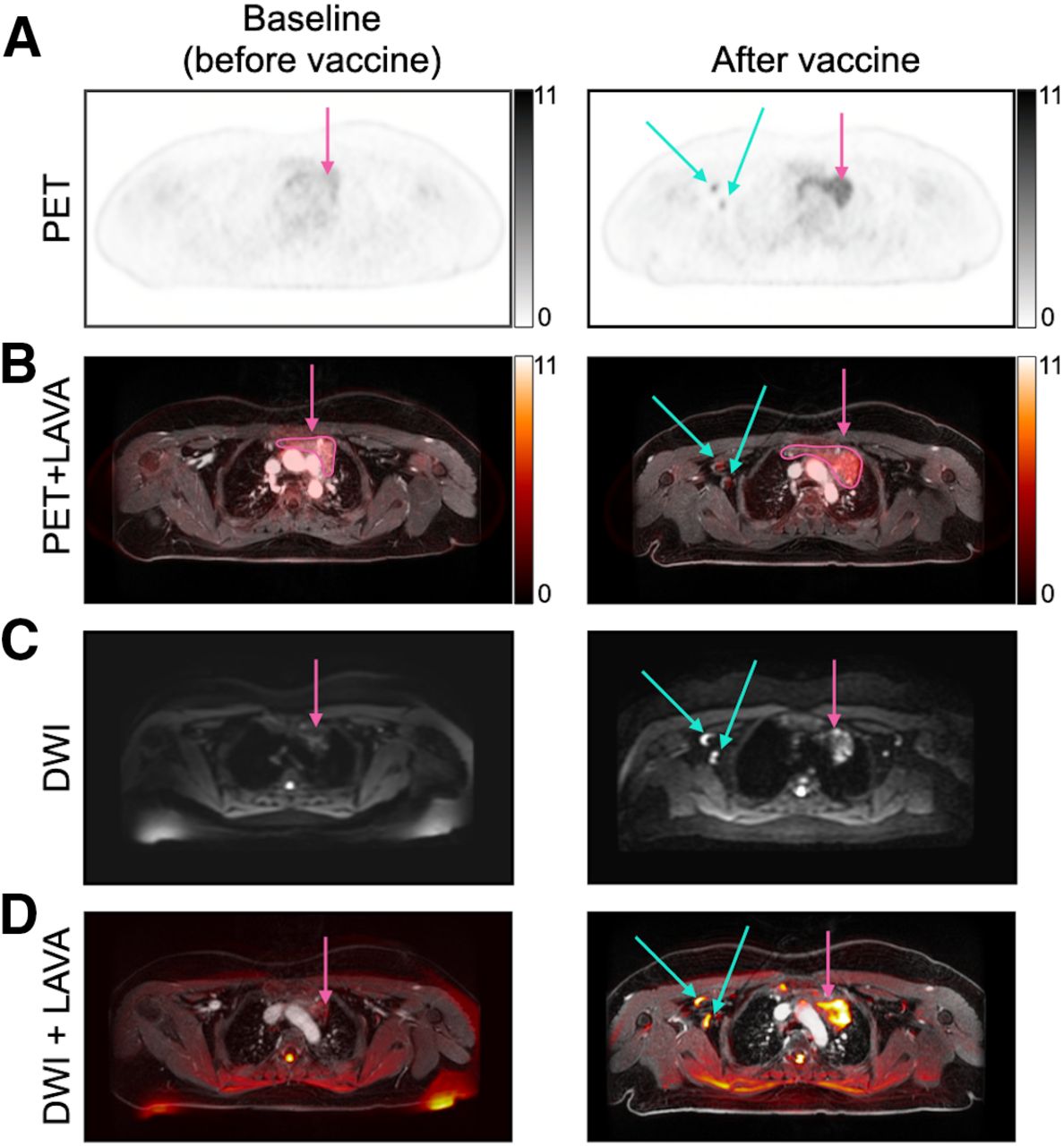
Axial 18F-FDG PET (A), 18F-FDG PET/T1-weighted gradient echo (LAVA) MRI (B), axial DW MRI (C), and DW MRI/LAVA MRI (D) in 14-y-old girl with bilateral ovarian Sertoli-Leydig tumors. Scans were obtained 3 mo before first COVID-19 vaccination dose (first column) and 2 mo after third vaccination dose (6 mo after first vaccination; second column). After vaccination, 18F-FDG PET and 18F-FDG PET/LAVA MRI showed increased uptake in thymus (pink arrows in A and B) and axillary lymph nodes (blue arrow in A and B); similarly, DW MRI and DW MRI/LAVA MRI showed restricted diffusion in thymus (pink arrows in C and D) and axillary lymph nodes (blue arrows in C and D). DWI = diffusion-weighted imaging; LAVA = liver acquisition with volume acquisition.
In addition, all 6 patients who were previously diagnosed with extrathoracic cancers also demonstrated an increased size, increased metabolic activity, and restricted diffusion of the lymph nodes and thymus after COVID-19 vaccination (Fig. 1). The mean SUVmax of the thymus increased 2-fold, from 1.77 ± 0.97 before vaccination to 3.46 ± 1.35 after vaccination (P = 0.017). The size of the thymus, approximated as the product of the shortest and longest transverse diameters, increased 1.7-fold, from 7.02 ± 5.41 to 11.91 ± 11.85 cm (P = 0.13). The mean ADC of the lymph nodes decreased from 1.11 to 0.92 (P = 0.26), and the mean ADC of the thymus decreased from 1.53 to 1.09 (P = 0.08). Data are shown in Figure 2.

18F-FDG PET/MRI parameters before and after COVID-19 vaccination: SUVmax of thymus and axillary lymph nodes (A and B), LDi × SDi of thymus (C), mean ADC of thymus (D), and mean ADC of lymph nodes (E). Follow-up 18F-FDG PET/MRI scans for patients 1, 2, 3, 4, 5, and 6 were obtained 76, 21, 66, 9, 121, and 6 d after their last vaccination, respectively. SUVmax of thymus (P = 0.02) and axillary lymph nodes (P = 0.03) significantly increased after vaccination, thymic size approximated by LDi × SDi increased (P = 0.13), and mean ADC of thymus (P = 0.08) and axillary lymph nodes (P = 0.07) decreased. Significance was computed using 2-tailed paired t test. LDi = longest transverse diameter; SDi = shortest transverse diameter.
DISCUSSION
Here we show for the first time, to our knowledge, that 18F-FDG PET/MRI can reveal thymus activation in addition to local lymph node reactions in children after COVID-19 vaccination. Six patients demonstrated increased 18F-FDG uptake and restricted diffusion of the locoregional lymph nodes and thymus after receiving the COVID-19 vaccination. The observed decrease in the mean ADC values of the thymus after vaccination indicates increased cellularity of the thymus tissue, which could be related to immune cell infiltration or proliferation in response to the vaccination. The observed increase in the SUVmax of the thymus after vaccination indicates increased metabolic activity of the thymus tissue, which could be related to immune cell activation.
Our results are consistent with a recent case study reporting increased 18F-FDG uptake in the thymus and left axillary lymph nodes in a 35-y-old woman after vaccination (12). The history of recent vaccination, the combination of metabolically active axillary lymph nodes and thymus, and the absence of bone marrow activation can all help with the correct diagnosis.
Differential diagnoses include recurrent or metastatic cancer and thymic rebound after chemotherapy (13). In survivors of leukemia and lymphoma, thymic hyperplasia after completion of chemotherapy is typically characterized by thymic enlargement and hypermetabolism, without changes in local lymph nodes (14). Thymic rebound after chemotherapy is often accompanied by an increased metabolic activity of the bone marrow. By contrast, our patients demonstrated activated lymph nodes and normal bone marrow. Radiologic evaluation of the morphologic and metabolic appearance of the thymus allowed us to exclude tumor lesions. Thymic tumors cause mass effects (i.e., compression of the veins, deviation of the trachea), which were not observed. 18F-FDG uptake of the thymus was homogeneous and bilateral, and no focal 18F-FDG uptake was observed, suggesting that the increased metabolic activity was of an inflammatory nature.
It is important to note limitations in our current analysis. Further studies with larger sample sizes are needed to confirm our findings. The interval between vaccination and imaging, combined with the fact that immunologic responses can vary significantly among individuals (15), may contribute to a wide range of immune responses to vaccination. Expanding our analysis to include patients who have autoimmune diseases or are heavily immunosuppressed, as well as conducting a time-series analysis to examine changes in the metabolic activity of the thymus and lymph nodes after vaccination, could provide a more nuanced understanding of how vaccination is represented on 18F-FDG PET/MRI. However, our current study’s retrospective nature makes this kind of time-series analysis challenging. Understanding the duration of thymic activity after vaccination and modulatory factors affecting thymic activity can assist in optimizing vaccine administration and imaging schedules to avoid confounding results.
CONCLUSION
The detection of increased 18F-FDG activity in the local lymph nodes and thymus after COVID-19 vaccination on 18F-FDG PET/MRI scans could be helpful to confirm a vaccine-induced immune response in cancer patients. 18F-FDG PET/MRI can reveal thymus activation in addition to local lymph node reactions in children after COVID-19 vaccination. These findings underscore the importance of verifying a patient’s vaccination status before an imaging examination, as vaccination-associated changes can lead to false-positive diagnoses.
DISCLOSURE
This work was supported by a grant from the National Cancer Institute (Grant No. R01CA269231). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 18F-FDG PET/MRI reveal thymus and lymph node activity after COVID-19 vaccine administration?
PERTINENT FINDINGS: We evaluated 18F-FDG PET/MRI scans for 6 children and young adults before and after COVID-19 vaccine administration. The scans demonstrated thymus activation in addition to local lymph node reactions in children after COVID-19 vaccination.
IMPLICATIONS FOR PATIENT CARE: Understanding postvaccination imaging findings in patients with cancer is important because these results may be confounded with tumor relapse or metastasis.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 26, 2023.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 3, 2023.
- Revision received September 17, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.