


Abstract
18F-FDG PET has proven invaluable in the staging of patients with metastatic colorectal cancer. The aim of the current study was to determine whether this biologic scan would correlate with other cellular characteristics and the clinical behavior of tumors. Methods: Ninety patients with resectable colorectal cancer metastatic to the liver underwent 18F-FDG PET before hepatectomy. At surgery, tumors were harvested and prepared for assessment by histology and immunohistochemistry. Expression of Ki67 (a marker for cell proliferation), GLUT1 and GLUT3 (markers for glucose transportation), p53 and p27 (markers for cell cycle control), and BCL-2 (a marker for apoptosis) was assessed by a pathologist who was unaware of the PET results and the clinical outcome. Patients were followed to determine outcome. Survival analysis was performed comparing patient outcome in groups segregated according to standardized uptake values (SUVs) greater or less than 5, 7, or 10. Results: Maximum SUV correlated with GLUT1 (P = 0.03), Ki67 (P = 0.026), and p53 (P = 0.024) but did not correlate with p27, BCL-2, or GLUT3. Survival was significantly longer for patients with a low SUV than for patients with a high SUV, with P values of 0.014, 0.025, and 0.0095 for SUV cutoffs of 5, 7, and 10, respectively. Conclusion: 18F-FDG PET is a biologic scan that predicts prognosis in patients with metastatic colorectal cancer. It is uncertain if this ability is due to cellular glucose metabolism or to a correlation with other cellular characteristics of aggressive tumors.
PET using 18F-FDG has become an indispensable staging modality for many types of cancer, including colorectal cancer (1,2), esophageal cancer (3), melanoma (4), sarcoma (5), and lung cancer (6). This imaging technique detects glucose-avid cancer deposits and can enhance the detection of metastatic deposits, resulting in more complete tumor resections and preventing nontherapeutic laparotomies for patients with unresectable disease (7). The result of the application of this technique is more appropriate and more efficient clinical care, resulting in improved long-term outcome (1). This scanning technique is now standard in the preoperative work-up for many types of cancer.
18F-FDG PET is a biologic scanning technique that measures the glucose metabolism in a tumor. Enhanced glucose metabolism has been related to the aggressiveness of cancer cells. Thus, it is not surprising that in some types of cancer, such as esophageal cancer (8), lung cancer (9), and gastrointestinal stromal tumors (10), the quantity of 18F-FDG uptake as assessed by PET correlates with outcome. Whether such a correlation exists for patients with colorectal cancer metastatic to the liver has not been reported and was the subject of the current prospective trial. Because this evaluation was prospective, we were able to secure freshly harvested tumors at resection. Molecular analysis of these tissues allowed an analysis of the correlation between 18F-FDG uptake and those molecular markers thought to be important for prognosis.
MATERIALS AND METHODS
This study was performed under the approval of the Institutional Review Board of the Memorial Sloan-Kettering Cancer Center, and all enrolled patients gave written informed consent. Ninety patients (45 men and 45 women) who were being evaluated for resection of colorectal liver metastases were enrolled. Of these patients, 90 underwent a liver resection. These constituted the patients for this study. All patients were imaged on a high-sensitivity dedicated bismuth germanate PET system (Advance; GE Healthcare) 60–90 min after an injection of 370–555 MBq (10–15 mCi) of 18F-FDG. Iteratively reconstructed images of the 18F-FDG PET scans were read by a nuclear medicine physician who was blinded to the results of other scanning. PET results were quantified by calculating the maximum standardized uptake value (SUV) for lesions detected (11). In brief, the slice with the maximal-intensity voxel was identified and a region of interest was placed around the tumor. Vendor-supplied software corrected the injected dose for decay and patient weight.
Correlation of 18F-FDG PET with Outcome
Follow-up for these 90 patients was conducted through examination of office notes and patient medical records. In patients with multiple tumors, the highest SUV was used for comparison with survival. Survival curves were drawn by the method of Kaplan and Meier, and comparison of survival was performed using log-rank analysis (12). SUVs of 5, 7, and 10 were used as cutoffs for comparisons.
Tissue Preparation and Immunohistochemical Staining
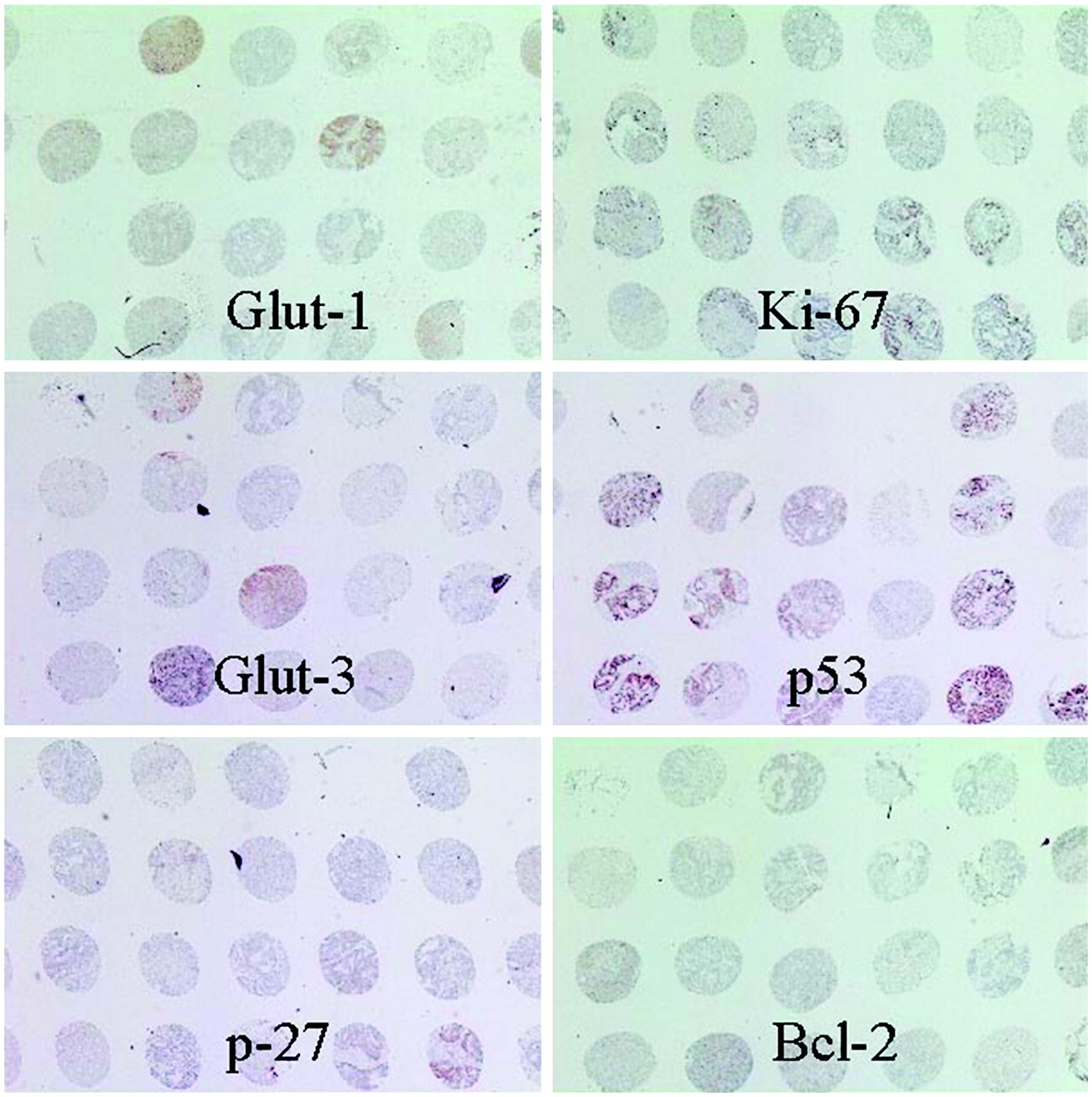
From these 90 patients, the surgical specimen was immediately “bread”-sliced and lesions identified to correlate with the PET findings. The 129 lesions in the specimens were also immediately harvested and placed in paraffin blocks for processing. Nonnecrotic areas on the paraffin blocks were then used to produce tissue arrays (Fig. 1) for further sectioning and analysis. Each specimen was placed in triplicate in the tissue arrays. All immunohistologic analysis was performed with the observers unaware of the PET or clinical results.
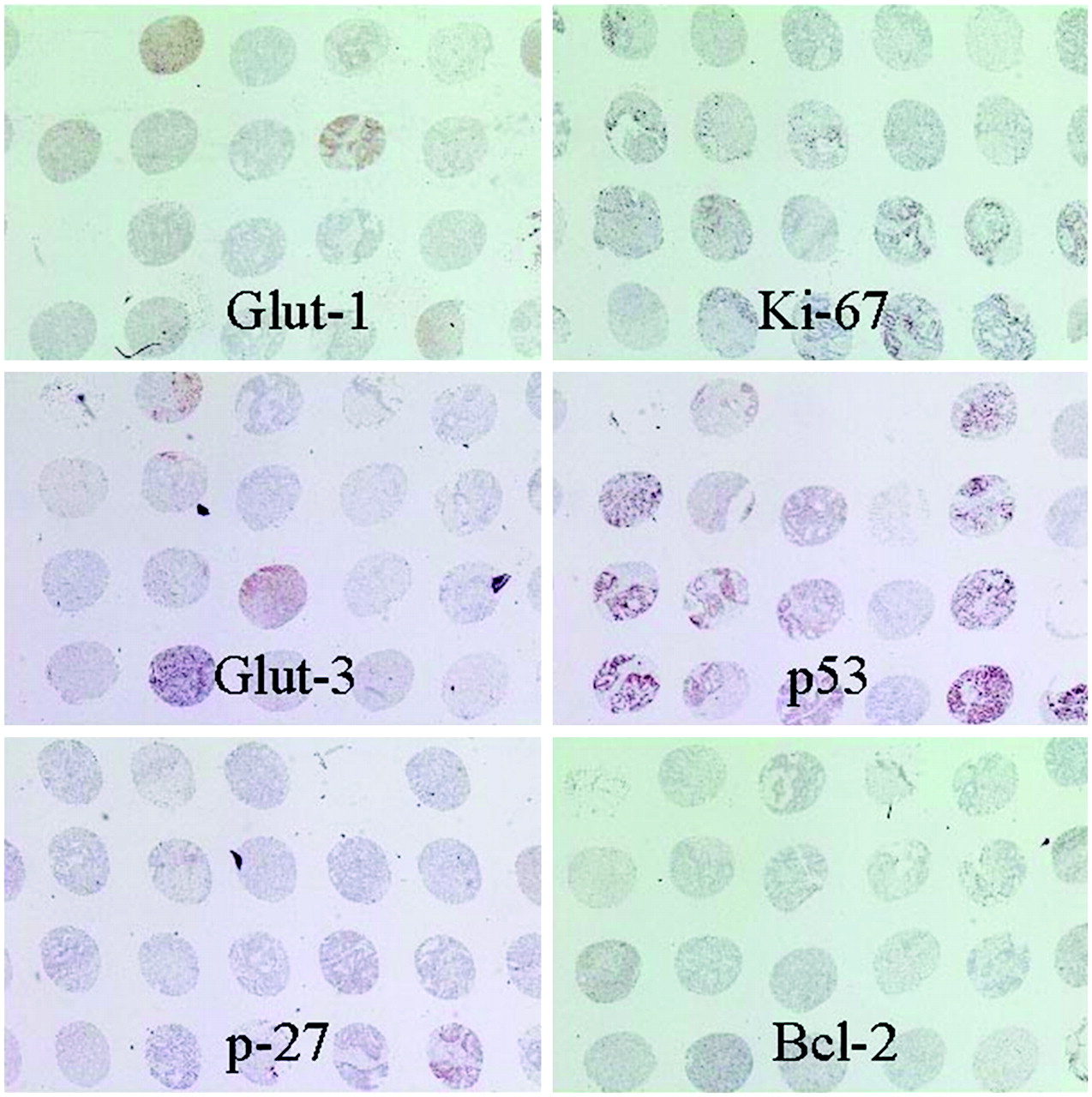
Tissue arrays with immunohistochemistry stains for various biologic markers.
Five-micrometer sections were then cut. The sections were placed on Superfrost Plus microscope slides (Fisher Scientific) and then baked at 60°C for 2 h. Xylene was applied to remove the paraffin, and then the sections were rehydrated through an ethanol gradient to distilled water. Immunohistochemical staining was performed using standard streptavidin-biotin-peroxidase detection techniques, with diaminobenzidine as the chromogen. All sections were pretreated in steam for 30 min at 97°C in a citrate buffer solution (2.1 g/L, pH 6). The sections were allowed to cool in the solution for 20 min at room temperature and were subsequently rinsed with distilled water, followed by phosphate-buffered saline (PBS). Endogenous peroxidase activity was quenched with a 5-min incubation in 3% hydrogen peroxide, and sections were again rinsed in distilled water and then in PBS. The slides were then placed in a bath of 0.05% bovine serum albumin (BSA), diluted in PBS, for 1 min. Normal goat serum was applied at a 1:20 dilution in a 2% BSA/PBS solution on sections to be stained for GLUT1 and GLUT3 (markers for glucose transportation). Normal horse serum was used for p53 and p27 (markers for cell cycle control), BCL-2 (a marker for apoptosis), and Ki67 staining (a marker for cell proliferation). All sections were incubated in a humidity chamber for 10 min. Serum was removed, and the sections were incubated overnight at 4°C with the primary antibody diluted with 2% BSA/PBS.
The primary antibodies used included polyclonal antibodies reactive against GLUT1 and GLUT3 (Chemicon) at a dilution of 1:20,000 monoclonal antibodies recognizing p53, BCL-2, and p27 (Dako Corp.) at dilutions of 1:500, 1:50, and 1:200, respectively, and the Mib-1 monoclonal antibody recognizing Ki67 (Immunotech) at a dilution of 1:50. The next day, the antibody was removed using 3 separate washes of PBS for 10 min each. The secondary antibody, biotinylated antimouse IgG (Vector Laboratories, Inc.), was applied for 60 min at a 1:500 dilution in 1% BSA/PBS, and sections were washed with 3 changes of PBS. The peroxidase-conjugated streptavidin (Dako Corp.) was then applied for 1 h at a dilution of 1:500 in 1% BSA/PBS, and sections were again washed with PBS. Positive staining was visualized using diaminobenzidine as a substrate-chromogen solution. The slides were counterstained with Harris-modified hematoxylin (Fisher Scientific) and dehydrated in graded ethanol, using a mounting medium and cover slip.
For each of the antibodies, negative controls were performed using nonimmune serum instead of the primary antibody. Positive controls consisted of tumor tissues known to positively express GLUT1 and GLUT3 (colonic adenocarcinoma), p53 (bladder tumor), and Ki67 (fibrosarcoma). Positive staining of erythrocytes served as an internal positive control for expression of GLUT1. Protein expression of GLUT1, p53, and Ki67 was scored by a pathologist as either high (≥50%) or low (<50%) on the basis of the percentage of positive viable tumor cells per section. GLUT3 expression was scored as positive or negative. Scoring was done in areas that did not show significant necrosis. Sections with cancer cells that positively demonstrated membranous staining at any frequency and intensity were considered positive for GLUT1 and GLUT3. For p53 and Ki67, microscopic examination for the nuclear reaction product was performed and scored.
For comparisons of SUV and molecular markers, each tumor harvested for histologic analysis was used as an independent data point. Correlation was performed using the Pearson method (13). The statistical software SPSS was used for all analyses (SPSS Systems).
RESULTS
Demographics.
The median age of the patients was 62 y (range, 30–80 y), with the median follow-up being 38 mo. For the 34 patients who died of disease, median follow-up was 32 mo.
Survival.
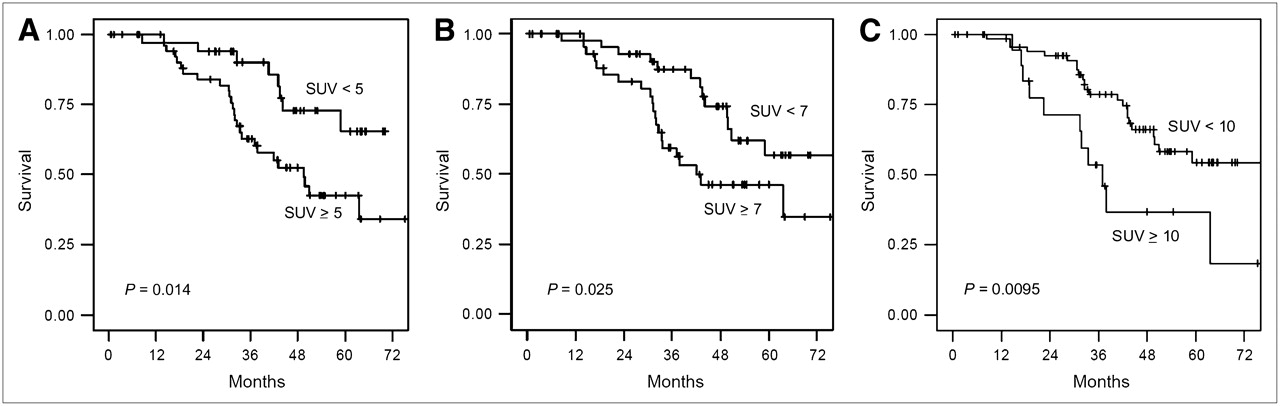
A survival analysis comparing SUV with outcome was performed. The Kaplan–Meier survival curves for patients—with the patients segregated according to whether they had an SUV less than 5, 7, or 10 or an SUV greater than or equal to 5, 7, or 10—are shown in Figure 2. It is clear that higher 18F-FDG uptake correlates with worse long-term outcome after resectioning of metastatic colorectal cancer. Median survival was not reached for patients with an SUV of less than 5 and was 48 mo for patients with an SUV of 5 or more. Two-year survival rates for an SUV of less than 5 and an SUV of 5 or more were 90% and 82%, respectively. Median survival was not reached for an SUV of less than 7 and was 42 mo for an SUV of 7 or more. Two-year survival rates for an SUV of less than 7 and an SUV of 7 or more were 90% and 80%, respectively. Median survival was not reached for an SUV of less than 10 and was 35 mo for an SUV of 10 or more. Two-year survival rates for an SUV of less than 10 and an SUV of 10 or more were 90% and 65%, respectively. Differences in survival between the groups with high SUVs and the groups with low SUVs were significant in all 3 cases, with P values of 0.014, 0.025, and 0.0095 for SUV cutoffs of 5, 7, and 10, respectively.

Survival of 90 patients according to SUV, with cutoff points at 5 (A), 7 (B), and 10 (C). In patients with multiple tumors, highest SUV was used.
Molecular Markers.
Sixty-five percent of cases stained positively for GLUT1, and 16% stained positively for GLUT3. For p53, p27, and BCL-2, the percentages of tumor staining positively were 56%, 38%, and 22%, respectively. Ki67 staining was graded by percentages: When the results were segregated according to whether the Ki67 was higher or lower than 50%, the percentage of tumors with a high Ki67 was 29%. We analyzed the correlation of 18F-FDG PET with these tumor markers. SUV correlated with GLUT1 (P = 0.03), Ki67 (P = 0.026), and p53 (P = 0.024). SUV did not correlate with p27, BCL-2, or GLUT3.
DISCUSSION
Radiologic advances have been invaluable in the development of treatments for malignancies. In the past, imaging has involved mainly tests that assess anatomic detail. However, advancements in imaging have brought about the introduction of biologic scanning modalities that assess cellular behavior or function. The anatomic localization provided by 18F-FDG PET and 18F-FDG PET/CT has successfully been used to more accurately stage patients with common malignancies and to direct therapy (14). In patients with hepatic colorectal metastases, assessment by 18F-FDG PET before liver resectioning has been associated with improved resectability, reduced recurrence, and improved long-term survival (15). This study would suggest that patient outcome could be altered by the extent of preoperative imaging. The importance of this scanning modality for assessing the biologic behavior of tumors has also become apparent. In various types of cancer, such as lung cancer (16) and esophageal cancer (8), ample data show that the intensity of 18F-FDG uptake is an independent predictor of clinical outcome. This finding is not surprising, because many studies had previously shown that high tumor glucose metabolism is a cellular characteristic that correlates with the aggressiveness of tumors (17). The current study adds to the literature by demonstrating that outcome after liver resection is also associated with the intensity of 18F-FDG uptake as documented by maximum SUV on PET. Thus, this biologic scanning modality should be considered not only for accurate staging of patients but also for assessment of prognosis. Future studies should examine the use of quantitative PET in selecting patients for adjuvant therapy, determining the frequency of follow-up studies, and deciding on the length of surveillance.
18F-FDG PET is one of a large number of biologic scanning modalities currently proposed for clinical use in assessing prognosis. Acetate scanning will provide information about tumor lipid metabolism (18), thymidine scanning can provide a way to noninvasively assess tumor DNA synthesis (19), and annexin scanning is showing potential for assessing apoptosis (20). These and other biologic scanning modalities are likely to become important in identifying occult disease but are also useful for determining tumor behavior and the prognosis of these patients. Past and current studies of 18F-FDG PET are important in that they support the concept that biologic scanning modalities can be used for prognostic stratification.
Active investigations are also examining the use of molecular markers as a prognostic variable. The classes of markers being investigated include those related to tumor metabolism, tumor proliferation, and tumor handling of therapeutic agents. We had previously demonstrated that for hepatic colorectal metastases, levels of tumor thymidylate synthase or of the transcription factor E2F-1 would be important in tumor response to chemotherapy and might influence outcome (21). In the current study, we examined several markers related to glucose metabolism and proliferation that had previously been shown to be prognostic factors in cancer (22,23). We confirmed that the expression of GLUT1 (22), p53 (23), and Ki67 (23) correlated with outcome. It is not surprising that GLUT1 expression is related to 18F-FDG uptake, because GLUT1 is the major glucose transporter for colorectal cancer (24). The relationship with indicators of proliferation is also intuitive but had not previously been shown. The importance of the findings is that the correlation of 18F-FDG uptake with outcome may not be due solely to the effects of enhanced glucose metabolism. There may also be effects from interrelated enhanced cellular proliferation or other cellular metabolic pathways.
CONCLUSION
The age of molecular imaging is providing an improved ability to study these complex relationships among various cellular metabolic and proliferative pathways. The various experimental biologic imaging techniques being developed bring the promise of multiple noninvasive imaging tests that may be used on human beings in serial studies. The serial studies will allow examination of tumors before and after multiple treatments to determine the effects on cellular biology. Such imaging studies also allow for colocalization studies to determine the scanning characteristics of various parts of the same tumor. Unlike tissue-sampling studies, which are limited by small samples, imaging studies allow for analysis of the entire tumor. The area of highest glucose metabolism may not be the site with the greatest lipid metabolism. These scanning techniques will allow for comparative metabolic studies. Further, dynamic studies can also be performed to examine the relative kinetic changes in metabolism. We are therefore at the beginning of an era of potentially great progress in the understanding of tumor biology, afforded by the development and refinement of biologic imaging. The current study is a proof of the principle that this imaging can be combined with direct studies of cellular biology.
Acknowledgments
This study was supported in part by grants RO1 CA 75416, RO1 CA/DK80982, and R25-CA096945-3 from the National Institutes of Health and by a grant from the Commonwealth Foundation for Cancer Research (of Mr. and Mrs. William H. Goodwin, Jr.) to the Experimental Therapeutics Center of Memorial Sloan-Kettering Cancer Center.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 16, 2006.
- Accepted for publication January 20, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Oncogene Pathway Activation in Mammary Tumors Dictates FDG-PET Uptake
- Prognostic Value of Metabolic Parameters in Patients with Synchronous Colorectal Cancer Liver Metastasis Following Curative-Intent Colorectal and Hepatic Surgery
- Biological Correlation of 18F-FDG Uptake on PET in Pulmonary Neuroendocrine Tumors
- Heterogeneity in Lung 18FDG Uptake in Pulmonary Arterial Hypertension: Potential of Dynamic 18FDG Positron Emission Tomography With Kinetic Analysis as a Bridging Biomarker for Pulmonary Vascular Remodeling Targeted Treatments
- Cell surface proteomics identifies glucose transporter type 1 and prion protein as candidate biomarkers for colorectal adenoma-to-carcinoma progression
- p53 Negatively Regulates Transcription of the Pyruvate Dehydrogenase Kinase Pdk2
- Biologic Correlation of 2-[18F]-Fluoro-2-Deoxy-D-Glucose Uptake on Positron Emission Tomography in Thymic Epithelial Tumors
- Using Dual-Tracer PET to Predict the Biologic Behavior of Human Colorectal Cancer
- 18F-FDG Uptake in Lung, Breast, and Colon Cancers: Molecular Biology Correlates and Disease Characterization
- Tumor Cell Metabolism Imaging