


Abstract
The preoperative staging of colorectal cancer (CRC) with 18F-FDG PET is not as yet generally considered to be evidence based. We have found only 1 study that evaluated 18F-FDG PET in a nonselected population with proven CRC. Several other studies have concentrated on more advanced disease. The aim of this study was to assess the potential clinical benefit of 18F-FDG PET in the routine staging of CRC. Methods: Thirty-eight consecutive patients who had had CRC histologically proven by colonoscopy underwent prospective preoperative staging by plain chest radiography, sonography, CT, and 18F-FDG PET. Sensitivity, specificity, and accuracy were retrospectively assessed by comparison with the histologic results after surgery (36 patients) or clinical follow-up (2 inoperable cases—both patients died within 1 y of the PET examination). The impact of 18F-FDG PET on therapeutic decision making was evaluated by comparing medical records before and after 18F-FDG PET. Results: 18F-FDG PET correctly detected 95% of primary tumors, whereas CT and sonography correctly detected only 49% and 14%, respectively. Lymph nodes were involved in 7 patients. The sensitivity, specificity, and accuracy of 18F-FDG PET were 29%, 88%, and 75%, respectively. CT and sonography did not reveal any lymph node involvement. Liver metastases were present in 9 patients. 18F-FDG PET, CT, and sonography had a sensitivity of 78%, 67%, and 25%, respectively; a specificity of 96%, 100%, and 100%, respectively; and an accuracy of 91%, 91%, and 81%, respectively. 18F-FDG PET revealed further lesions in 11 patients. Levels of carcinoembryonic antigen and carbohydrate antigen 19-9 tumor markers were elevated in, respectively, only 33% and 8% of cases of proven CRC. 18F-FDG PET changed the treatment modality for 8% and the range of surgery for 13% of patients. In total, 18F-FDG PET changed the method of treatment for 16% of patients. Conclusion: Plain chest radiography and sonography did not bring any clinical benefits. No correlation was found between the level of tumor markers and the stage of disease. CT is necessary for confirmation of PET findings at extraabdominal sites (PET-guided CT) and for their morphologic specification at abdominal and pelvic sites before an operation. 18F-FDG PET is the best method for the staging of CRC in all localities, despite the high rate of false-negative PET findings in patients with lymph node involvement. PET should be performed as a first examination after verification of CRC. We propose a PET/CT hybrid system as optimal in the staging of CRC.
Colorectal cancer (CRC) is one of the most common malignancies, representing 13%–14% of all oncologic diseases in the Czech Republic. The incidence of this type of tumor has increased by 190% within the past 20 y. The highest number of patients with CRC lies in the 65- to 75-y age group (1). If diagnosed in its early stages, CRC is highly curable by surgical treatment, with minimal morbidity and mortality. This fact demonstrates the need for improved earlier diagnosis (2). It is beneficial for the surgeon to be able to identify patients who have more lesions than previously supposed, enabling these patients to be ruled out from undergoing an initially planned operation, especially an extensive one. On the other hand, the range of surgery can be modified for patients with unsuspected liver metastasis. Sonography and CT cannot evaluate normal-sized lymph nodes, nor can they reliably differentiate malignant lesions from benign ones in the liver. PET with 18F-FDG has the potential to detect malignant cells by their increased glucose metabolism.
In conclusions reached during the 3rd German Interdisciplinary Consensus Conference (3), therapy control and restaging of CRC in cases of suspected relapse were considered to be evidence based, but preoperative staging of CRC was not.
Eleven studies dealing with the preoperative staging of CRC were found in MEDLINE (U.S. National Library of Medicine). Seven studies (4–10) chose, for 18F-FDG PET examination, patients with known or suspected metastasis of the liver or high-risk patients who showed elevated levels of carcinoembryonic antigen or were at an advanced stage of disease. Only Abdel-Nabi et al. (11) and Mukai et al. (12) used consecutive patients with biopsy-proven or highly clinically suggestive CRC preoperatively, although the latter study focused on the diagnosis of primary CRC and the detection of metastases in regional lymph nodes only. Therefore, little is known about the clinical benefits of 18F-FDG PET in consecutive patients.
The introduction of 18F-FDG PET into the routine staging of CRC, which has been put into practice at 1 referring surgical department, has raised the question of whether a clear clinical benefit results. Our study addresses this question.
MATERIALS AND METHODS
Patients
We examined 38 consecutive patients (11 female, 27 male) with an average age of 66 y (range, 38–83 y). They all had CRC histologically proven by colonoscopy and underwent prospective preoperative staging by plain chest radiography, sonography, CT, and 18F-FDG PET. A radical lymphadenectomy and a detailed histologic examination of a large number of nodes were performed for all operated patients.
18F-FDG PET
Patients fasted for at least 6 h before the examination. 18F-FDG was administered into a peripheral vein in amounts representing 525 MBq per 70 kg of body weight. Data were acquired using the ECAT EXACT dedicated PET scanner (CTI/Siemens). Sixty to 70 min after 18F-FDG administration, 2-dimensional emission scanning from the groin to the base of the skull (5–6 bed positions) was performed, lasting 5.6 min per bed position, in combination with a “hot” transmission scan lasting 2.4–4.4 min per bed position (transmission scanning time was corrected to allow for decay of the transmission sources). The data acquired were reconstructed by iterative ordered-subsets expectation maximization (8 subsets, 2 iterations, 6- to 8-mm gaussian filter) implemented using ECAT 7.2 software.
Sonography and CT
We examined patients from 1 surgical clinic, but sonography, for the most part, as well as some CT examinations had been performed on many of these patients at other hospitals throughout the Czech Republic. For this reason, we have not specified the sonographic technical data. The CT scanner used on most patients was the Somatom Plus 3 (Siemens).
Statistical Analysis
Routinely visually assessed 18F-FDG PET findings were retrospectively categorized by 1 nuclear physician. Clear PET findings indicating high consumption of glucose in lesions were classified as positive, whereas equivocal and clearly negative findings were classified as negative. Sensitivity, specificity, and accuracy were retrospectively assessed by comparison with the histologic results from surgery (36 patients) or clinical follow-up (2 inoperable cases). The impact of 18F-FDG PET on therapeutic decision making was assessed by comparing the medical records before and after 18F-FDG PET. The final postoperative TNM stage was assessed for each patient. Five patients were included at clinical stage I, 14 patients at stage II, 5 patients at stage III, 11 patients at stage IV, and 2 patients at stage X.
RESULTS
18F-FDG PET correctly detected 95% (35/37) of primary tumors, whereas CT and sonography correctly detected only 49% (17/35) and 14% (5/36), respectively. PET provided false-negative findings in 2 patients. The primary tumor of 1 patient could not be assessed because a preexisting vesicorectal fistula led to the presence of “hot” urine in the colon, preventing appropriate evaluation.
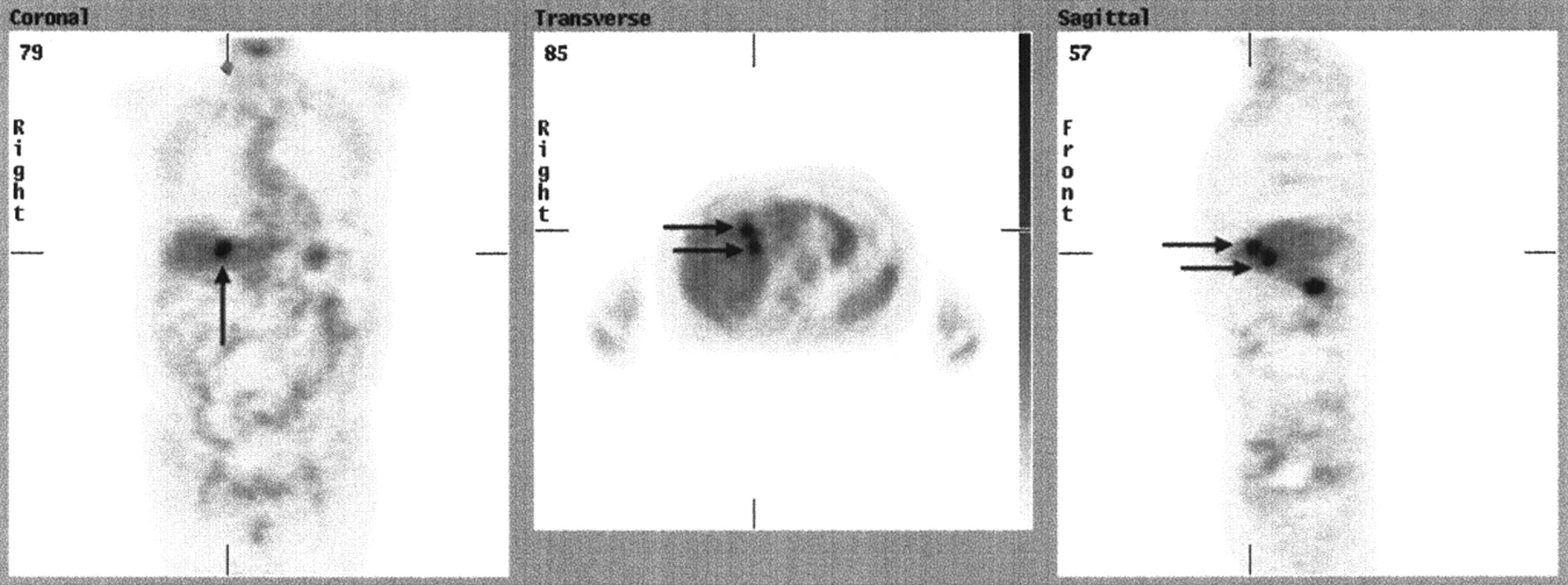
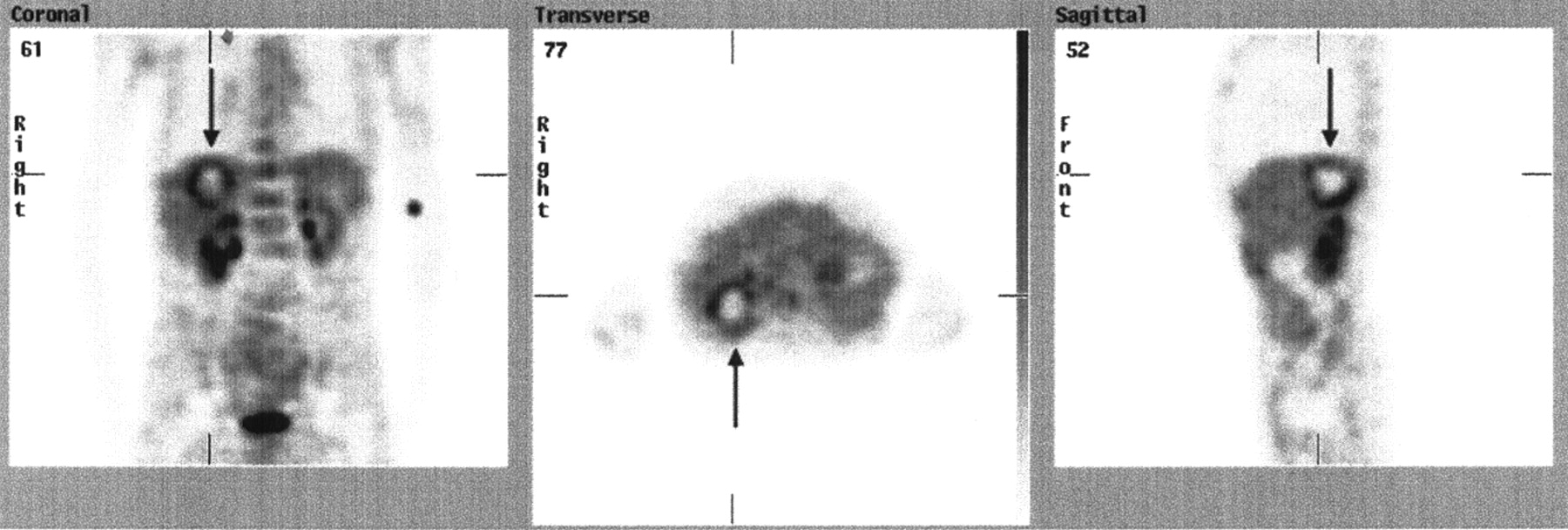
Lymph nodes were involved in 7 patients. The sensitivity, specificity, and accuracy of 18F-FDG PET were 29% (2/7), 88% (22/25), and 75% (24/32), respectively. CT and sonography did not reveal any lymph node involvement. PET findings were false-negative in 5 of 7 patients with lymph node involvement and false-positive in 3 of 25 patients without lymph node involvement. Figure 1 is an example of true-positive PET findings.

18F-FDG PET scan of 78-y-old woman with primary rectal carcinoma (solid arrows) and histologically proven metastasis in lymph nodes (dashed arrows). PET findings were true-positive, and CT findings were false-negative. Shortly before PET examination, hypermetabolic focus on surface of right hypogastrium showed inflammatory reactive changes after previous appendectomy.
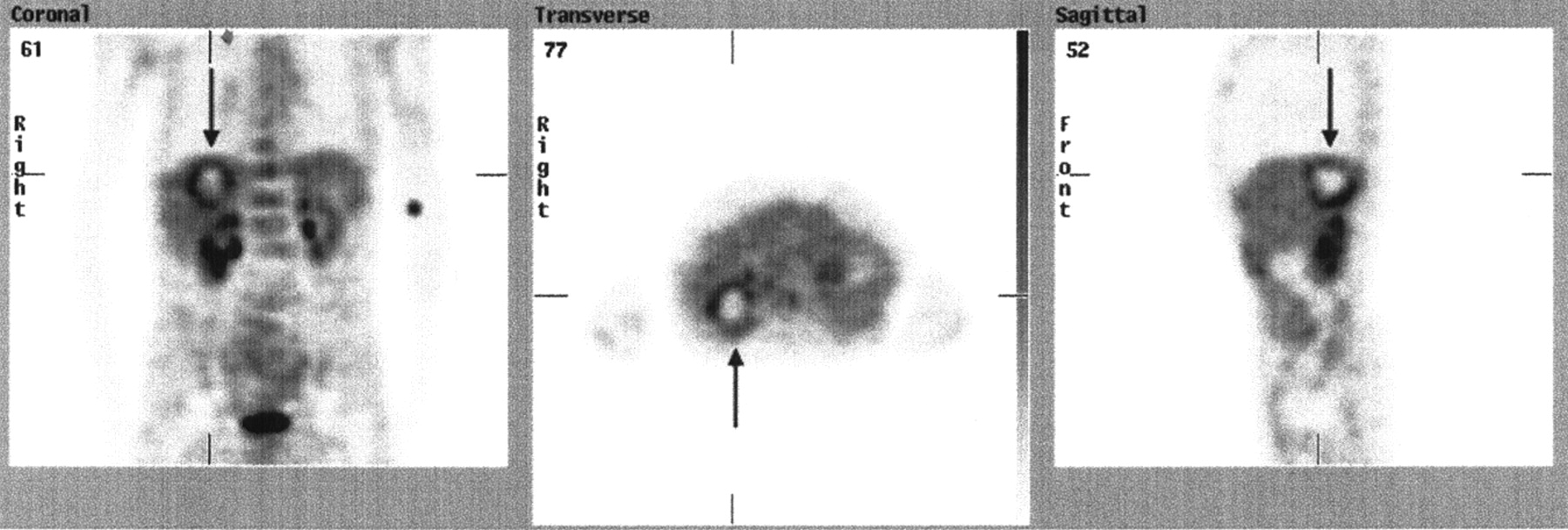
Liver metastases were present in 9 patients. 18F-FDG PET, CT, and sonography had a sensitivity of 78% (7/9), 67% (6/9), and 25% (2/8), respectively; a specificity of 96% (24/25), 100% (23/23), and 100% (24/24), respectively; and an accuracy of 91% (31/34), 91% (29/32), and 81% (26/32), respectively. The PET findings were true-positive in 7 of 9 patients with liver metastases (Fig. 2), and in 2 patients the PET findings were false-negative (sonographic and CT findings were also false-negative; they did not provide any additional information). The PET findings were true-negative in 24 of 25 patients without liver metastases.
18F-FDG PET scan of 69-y-old man with liver metastases of CRC revealed by PET (arrows). CT performed before PET had false-negative findings.
In 11 patients, 18F-FDG PET revealed further lesions missed by conventional staging: 4 of 7 highly suggestive neoplasms were confirmed as being malignant, and all but one of these were found by CT follow-up. The neoplasm not found by CT follow-up was a small focus of high glucose consumption in the thoracic vertebra (a follow-up examination had not been performed because the neoplasm was generalized). One lesion was confirmed as benign, and 2 are still unresolved. Four other lesions were characterized by 18F-FDG PET as low-probability neoplasms, 2 were verified as benign disease, and 2 others are still unresolved. Most lesions revealed by PET were outside the field of view on CT scans performed before the PET examination.
The carcinoembryonic antigen and carbohydrate antigen 19-9 tumor marker levels were elevated in, respectively, only 33% (9/36) and 8% (3/36) of patients with proven CRC.
18F-FDG PET changed the treatment modality for 8% of patients (3/38) and the range of surgery for 13% (5/38). In total, 18F-FDG PET changed the treatment methods for 16% of patients (6/38).
DISCUSSION
For imaging of a primary tumor, 18F-FDG PET had the highest sensitivity (95%, or 35/37) of all the modalities used in our series. This finding confirms the results of the cited studies. Abdel-Nabi et al. (11) found a PET sensitivity of 100%, or 37 of 37, but the sensitivity was slightly lower—95%, or 37 of 39 lesions—when the 2 small foci of carcinoma arising in tubulovillous polyps, found incidentally with negative 18F-FDG PET scans, were included. Mukai et al. (12) detected a primary tumor in 23 of 24 patients (sensitivity, 96%). Whiteford et al. (9) found PET sensitivity to be dependent on histologic type: In detecting mucinous cancer, PET had a sensitivity of 58%, and in detecting nonmucinous cancer, the sensitivity was 92%. Gupta et al. (13) found the overall 18F-FDG PET sensitivity in the detection of tumor sites (including primary tumors, lymph node involvement, and liver) to be 90% (18/20). We had 2 false-negative PET findings: In the first patient, a primary tumor 1.5 × 1.5 cm in size was histologically shown to be an invasive villous adenoma with foci of incipient malignancy (Abdel-Nabi et al. had the same result in 2 cases); in the second patient, glucose consumption was slightly higher in the rectum, so we considered it a physiologic variant.
For detection of lymph node involvement, 18F-FDG PET had low sensitivity (29%, or 2/7) but high specificity (88%, or 22/25) and accuracy (75%, or 24/32). Neither CT nor sonography provided any additional information. The results of sensitivity and specificity in the study of Abdel-Nabi et al. (11) were the same as ours (29%, or 4/14, and 96%, or 26/27, respectively). Mukai et al. (12) found a similar sensitivity (22.2%, or 2/9). Our specificity and accuracy were high enough because we considered equivocal findings to be negative. The reasons for our low sensitivity might be the radical lymphadenectomy that had been performed and the detailed histology that found the microscopic lesions. These cannot be seen with PET, which is a macroscopic examination. The localization of regional lymph nodes in the abdomen and pelvis, where physiologic uptake in the gut can be seen, also presents a problem. Therefore, if the lesions are small, they are difficult to distinguish and, in certain cases, difficult to differentiate from such a large range of primary tumor. We had 5 false-negative PET findings: In 2 cases, lymph nodes surrounded a large primary tumor, that is, stage N1 or N2 (in 1 case they were 1 cm in size). In another 2 cases, the lymph nodes were 4 mm in size (this is less than the spatial resolution of the device) at stage N1 and 1 cm in size at stages N1–N3. One patient had a generalized neoplasm in the abdomen, and he received only palliative treatment (which explains why the size of the lymph nodes is not known).
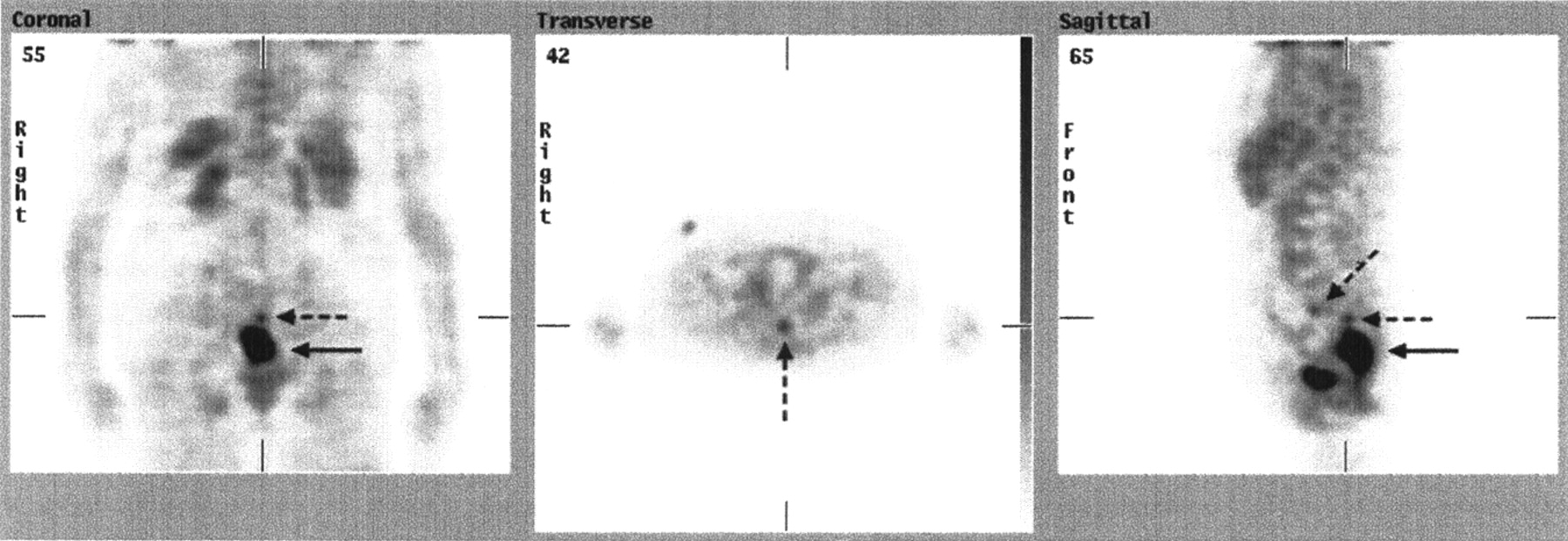
Concerning the detection of liver metastases, 18F-FDG PET and CT showed a similar sensitivity, specificity, and accuracy, and both were better than sonography. Our sensitivity was 78% (7/9). The cited study of Boykin et al. (4) found a PET sensitivity of 100% (6/6 patients). They used patients who had undergone resection of a primary tumor and were already known or suspected to have liver metastases, and the patients appeared to be in an advanced stage of disease. PET sensitivity in the study of Zhuang et al. (14) was also 100% (28/28), but the selection of patients is not known. In the study of Topal et al. (5), sensitivity was 99% (90/91). They chose patients with known metastases revealed by conventional diagnostic methods. The studies of Rohren et al. (6) and Ogunbiyi et al. (10) estimated the sensitivity at 95%. PET sensitivity in the study of Abdel-Nabi et al. (11) was 88% (7/8). In the study of Fong et al. (8), 85% of hepatic lesions larger than 1 cm but only 25% of those smaller than 1 cm were detected. Ruers et al. (7) found that PET had an even lower sensitivity on a lesion basis (65%) than did CT (80%) and that the sensitivity was related to tumor size. We had 2 false-negative PET findings: The first patient had 1 metastasis of differentiated tubular cancer in the liver, sized 0.8 cm (Abdel-Nabi et al. had the same result in 1 patient). The second patient had 2 metastases of mucinous cancer in the liver, each 2 cm in size. The reason behind the false-negative findings may be the small size of the lesions (7,8) or the histologic type (9). In 1 patient (Fig. 3), PET was false-positive, sonography was equivocal, CT was not performed, the macroscopic findings were equivocal, and histologic examination revealed a chronic abscess. Regarding specificity, the studies of Abdel-Nabi et al., Rohren et al., and Ogunbiyi et al. found it to be 100%. Our result (96%, or 24/25) confirmed this finding.
18F-FDG PET scan of 63-y-old man with suspected liver metastases found during explorative laparotomy. PET findings were evaluated as positive (arrows), sonographic findings were equivocal, CT was not performed, and histologic examination revealed chronic abscess.
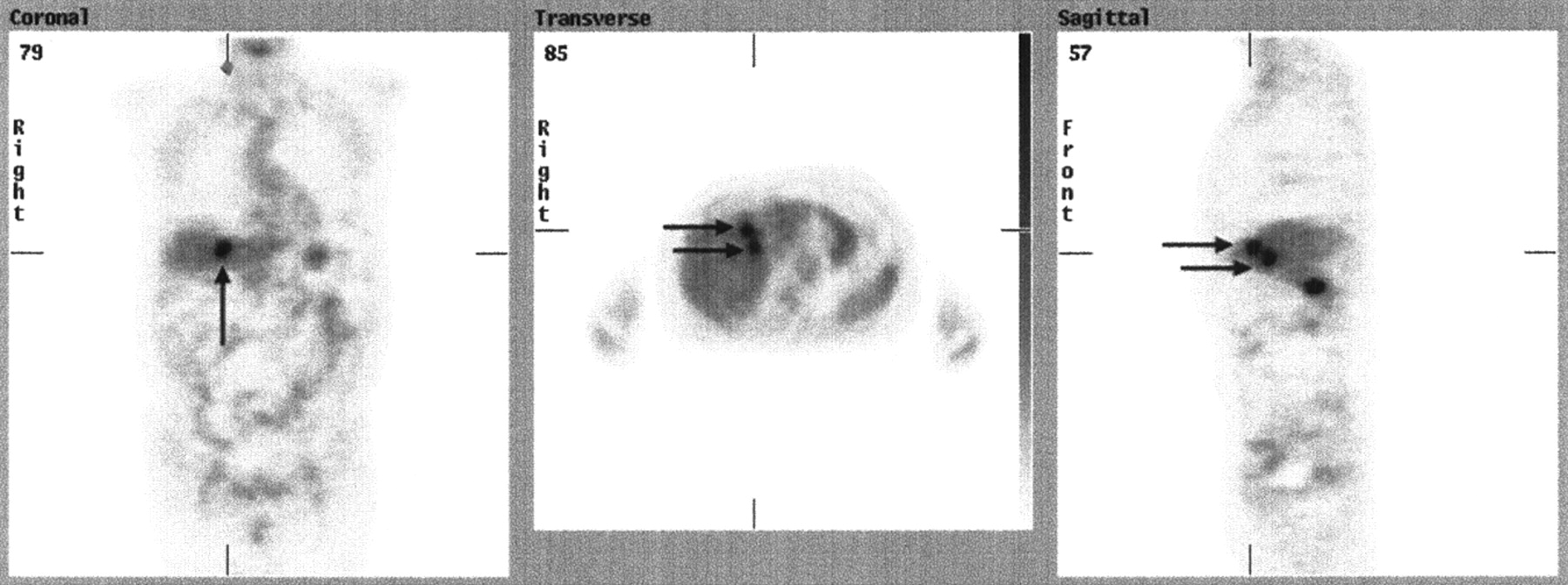
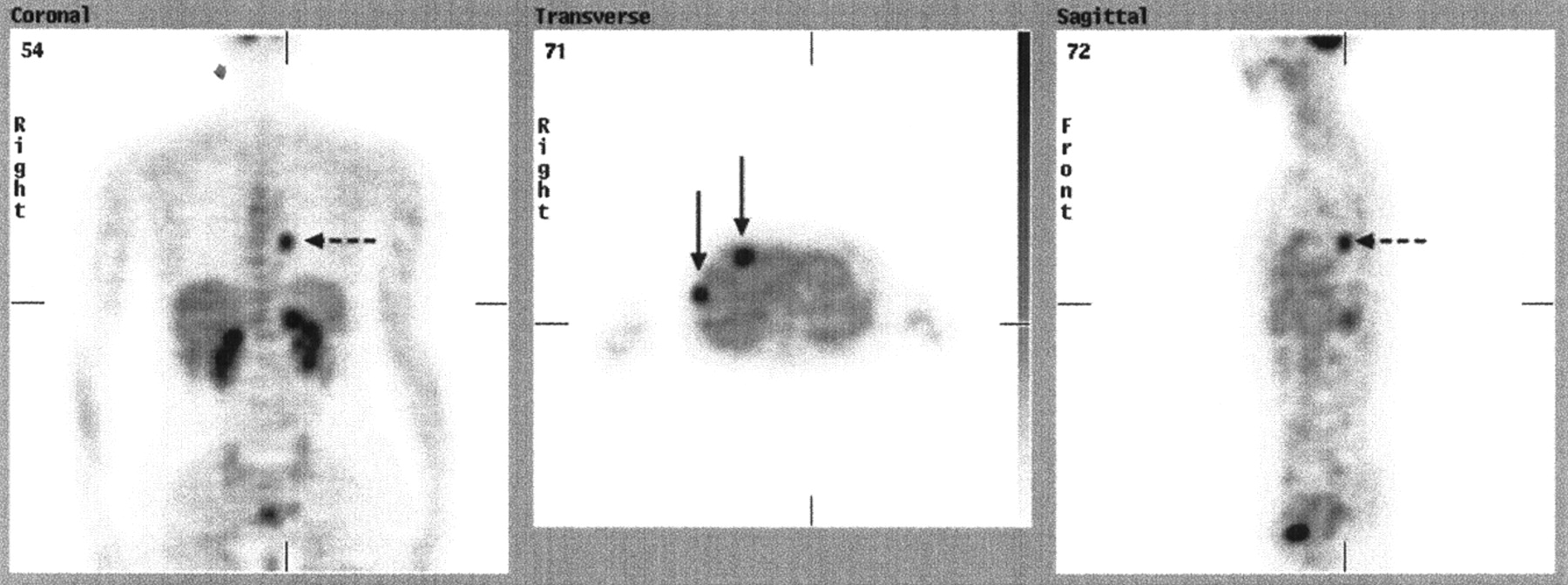
18F-FDG PET revealed 4 further cases of extrahepatic lesions (4/38, or 11%) that were verified as malignant; another 2 lesions highly suspected of being malignant are presently unresolved, which means the number of revealed lesions could be higher. Ruers et al. (7) mentioned 5 unresectable pulmonary metastases in 51 patients (10%) that were detected by 18F-FDG PET. Whiteford et al. (9) mentioned 18 proven extrahepatic metastases in 101 patients (18%). Fong et al. (8) detected extrahepatic disease, including disease in lymph nodes, in 13 of 17 patients by 18F-FDG PET (76%). These studies worked with patients who were already suspected of having metastases—that is, were in an advanced stage of the disease. Topal et al. (5), also working with patients who had suspected or known metastasis in the liver, detected 3 extrahepatic metastases in 91 patients (3%). In the patient with pulmonary metastasis in their study, plain chest radiography performed before 18F-FDG PET was also negative, just as we found in 1 patient in our study (Fig. 4).

18F-FDG PET scan of 38-y-old woman with known liver metastases (solid arrows) and with pulmonary metastasis (dashed arrows) revealed by PET and subsequently confirmed by CT. Plain chest radiography performed before PET had false-negative findings, which may have been due to retrocardiac localization of lesion.
In assessing the influence of PET findings on clinical management, we found fewer changes in therapeutic decision making than did other investigators. In our study, therapy was changed for 16% of patients (6/38); in other studies, therapy was changed for 20% (10/51) (7); was influenced for 40% (16/40) (8) or 43% (10/23) (10); or was directly altered for 23% (9/40) (8) or even 50% (7/14) (4). The reason might be the selection of patients in the other cited studies, because many of those patients had already been known to have advanced disease (in the study of Fong et al. (8), 17/40 patients had extrahepatic disease). Therefore, 18F-FDG PET could easily influence therapy for 40%–50% of patients. We used consecutive patients, and many were in an initial stage of disease. Only 1 study was designed similarly to ours—that of Abdel-Nabi et al. (11). But they did not mention any influence on clinical management. In our series, PET influenced the clinical management of 6 patients. In the first of these patients, CT findings for the abdomen and pelvis were positive only at the site of the primary tumor, and no metastases were found in these localities. Radiotherapy was initiated, PET was performed, and 2 foci of high glucose consumption were found in the liver, indicating suspected metastases. The radiotherapy was therefore suspended and the patient underwent an operation, which confirmed metastases in the liver. The patient subsequently received chemotherapy. In the second patient, PET revealed generalized malignancy; therefore, the patient did not undergo surgery and was treated only palliatively. In the third patient, an exenteration of pelvis was planned, but because of a chest metastasis revealed by PET, only palliative sigmoidostomy and radiotherapy were performed. The fourth patient, a young woman with known liver metastases, underwent PET before surgery. Plain chest radiography had negative findings, but the PET examination found in the left lung a focus of high glucose consumption highly suggestive of metastasis, which was confirmed by subsequent CT. Therefore, the patient did not undergo surgery and instead started on a course of chemotherapy and radiotherapy. In the fifth patient, a concurrent operation of the primary tumor and the liver was planned because of CT findings highly suggestive of liver metastasis. When the PET scan did not confirm this suspicion, the surgical staging was modified. A cyst was found during the operation. For the sixth patient, with a primary tumor and known metastasis in the left lung, 2 operations were planned. PET revealed generalization of the neoplasm, and therefore only palliative radiotherapy and chemotherapy were started.
CONCLUSION
18F-FDG PET had a major impact on treatment decision making in 16% of patients. Despite the high rate of false-negative findings in patients with lymph node involvement, 18F-FDG PET is more reliable than CT or sonography for preoperative staging of CRC in all localities and should be performed as a first examination after CRC has been confirmed. The obvious advantage of using PET is the metabolic information that is provided for a large field of view. Sonography and plain chest radiography have not brought any clinical benefits. There is no place for these types of examinations in the staging of CRC. No correlation has been found between tumor marker levels and the stage of disease, but they can be used for the next follow-up and for diagnosing CRC recurrence. The use of CT cannot be ruled out, as it is necessary to confirm PET findings at extraabdominal sites (PET-guided CT), to specify them morphologically at abdominal and pelvic sites, and to precisely locate them in the liver before an operation. For this reason, a PET/CT hybrid system would be of benefit. The results of this study confirm those of previously cited studies. Only 1 study (11) was designed similarly to our own—that is, used 18F-FDG PET routinely for preoperative staging of CRC. The conclusions of this study show that the use of 18F-FDG PET in the regular preoperative work-up of CRC is worth considering.
Footnotes
Received Mar. 4, 2003; revision accepted Jul. 22, 2003.
For correspondence or reprints contact: Iva Kantorová, MD, PET Centre, Department of Nuclear Medicine, Na Homolce Hospital, Roentgenova 2, 150 30 Prague 5, Czech Republic.
E-mail: iva.kantorova{at}homolka.cz
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Usefulness of Diffusion MRI in Detection of Lymph Node Metastases of Colorectal Cancer
- Clinical and research applications of simultaneous positron emission tomography and MRI
- The Flow-Metabolic Phenotype of Primary Colorectal Cancer: Assessment by Integrated 18F-FDG PET/Perfusion CT with Histopathologic Correlation
- Desmoid tumour (aggressive fibromatosis) of the colon mimics malignancy on dual time-point 18F-FDG PET/CT imaging
- [18F]FDG PET/CT imaging of colorectal cancer: a pictorial review
- Prognostic Implications of the Distribution of Lymph Node Metastases in Rectal Cancer After Neoadjuvant Chemoradiotherapy
- 18F-FDG PET Scanning Correlates with Tissue Markers of Poor Prognosis and Predicts Mortality for Patients After Liver Resection for Colorectal Metastases
- PET-Based Treatment Planning in Radiotherapy: A New Standard?
- Positron emission tomography scanning is not superior to whole body multidetector helical computed tomography in the preoperative staging of colorectal cancer
- "Flying Through" and "Flying Around" a PET/CT Scan: Pilot Study and Development of 3D Integrated 18F-FDG PET/CT for Virtual Bronchoscopy and Colonoscopy
- Findings on 18F-FDG PET Scans After Neoadjuvant Chemoradiation Provides Prognostic Stratification in Patients with Locally Advanced Rectal Carcinoma Subsequently Treated by Radical Surgery
- Whole body positron emission tomography/computed tomography (PET/CT) tumour staging with integrated PET/CT colonography: technical feasibility and first experiences in patients with colorectal cancer
- 18F-FDG PET in Evaluating Patients Treated for Metastatic Colorectal Cancer: Can We Predict Prognosis?