


Abstract
Predicting outcome after aggressive therapy for advanced rectal cancer remains difficult. 18F-FDG PET has emerged as a valid method for predicting patient outcomes after therapy in an increasing number of cancers. We evaluated the prognostic information obtained from the degree of change in tumor 18F-FDG PET uptake induced by chemoradiation before radical curative surgery in patients with T3/T4 rectal cancer. Methods: The study included 34 consecutive patients with T3/T4 Nx M0 rectal cancer on structural imaging, who underwent staging and postchemoradiation 18F-FDG PET before planned curative surgery. Change in 18F-FDG uptake was graded visually as complete (CMR), partial (PMR), or no (NoMR) metabolic response. Pre- and postchemoradiation 18F-FDG PET–derived standardized uptake values (SUVs) were then obtained for PMR patients to determine whether SUV further stratified this subgroup. Operative findings were available in 30 patients (3 excluded because of 18F-FDG PET–defined M1 disease, 1 refused surgery). Clinical status at study closeout (alive free from disease, FFD; alive with disease, AWD; or died of disease, DOD) was available for all patients. Results: A pathologic complete response was found in only 6 of 30 patients (5 CMR, 1 false-positive PMR). However, after an estimated median 3.1 y of follow-up, all 17 CMR patients were FFD, 6 of 10 PMR patients were FFD, 2 of 10 had DOD, and 2 of 10 were AWD. All 3 NoMR patients DOD. PET response was highly significantly associated with overall survival duration (P < 0.0001) and time to progression (P < 0.0001). Pathologic complete response was the only other statistically significant prognostic factor (P < 0.03). The percentage of maximum SUV change after chemoradiation was not predictive of survival in PMR patients. Conclusion: Using a simple qualitative assessment, postchemoradiation 18F-FDG PET scintigraphy provides good medium-term prognostic information in patients with advanced rectal cancer undergoing radical surgery with curative intent.
Multimodality treatment of locoregionally advanced rectal cancer appears to improve local control and overall survival (1–4). Further, improved long-term outcomes have been found only where pathologic assessment showed complete or nearly complete response to this therapy (5,6). Therefore, accurate, noninvasive assessment of tumor response after chemoradiation would be extremely useful. However, limitations inherent in structural imaging have reduced their effectiveness in this clinical situation (7). Studies examining the use of 18F-FDG PET for therapy monitoring have consistently shown good prognostic stratification potential in an increasing series of cancers treated with preoperative chemoradiation, including squamous cell tumors of the neck (8) and esophagus (9). Furthermore, an increasing series of small 18F-FDG PET studies (10–16) have all shown that 18F-FDG PET may also stratify patients with locally advanced rectal cancer into good or poor outcomes, according to various quantitative 18F-FDG-based criteria. This is despite showing a variable degree of accuracy in determining the degree of tumor cell reduction after chemoradiation (12–16).
However, quantitative 18F-FDG PET approaches using a reduction in the standardized uptake value (SUV) as the criterion for therapeutic response require a baseline study and are significantly impacted by the initial 18F-FDG uptake intensity. Specifically, tumors with very high SUVs have a greater potential for a large percentage reduction in SUV compared with less-avid tumors for which a return to background levels of activity may represent a relatively small percentage reduction in the SUV. Evaluation of the percentage reduction in SUV is also complicated by issues related to changes in tumor volume and changes in regional radiotracer distribution within the radiation treatment volume, rendering assignment of regions of interest for semiquantitative analysis difficult and, therefore, prone to interobserver variability. Several groups have previously demonstrated that simple qualitative interpretation of 18F-FDG PET after radical chemoradiation for non–small cell lung cancer (17) or treatment of non-Hodgkin's lymphoma (18) provides powerful prognostic stratification and, by application of pattern recognition, may be less affected by chemoradiation (19). The current study was therefore performed to assess whether application of a similar simple, visual assessment scale of changes in 18F-FDG uptake induced by chemoradiation is able to also stratify outcome in a consecutive group of patients with advanced rectal carcinoma who underwent surgery with curative intent.
MATERIALS AND METHODS
Patients undergoing a PET scan at this center are routinely asked to participate in an ethics-approved prospective study aimed at assessing the clinical impact of PET in predefined malignancies from long-term clinical follow-up, including access to ancillary test results. All patients in this series agreed to inclusion in this protocol and signed written, informed consent.
Patients
The study population was selected from a consecutive series of patients with biopsy-proven rectal cancer who were prospectively considered suitable for aggressive neoadjuvant chemoradiation with a potential view to radical surgery after presenting with locally advanced rectal carcinoma. Each patient had to have undergone a staging 18F-FDG PET scan and a second 18F-FDG scan after completion of their chemoradiation, usually just before surgery in those patients who underwent this procedure. Patients with known metastatic disease (M1 disease) on conventional imaging (10 patients) were excluded, leaving 34 patients eligible for this study. Conventional TNM staging using current AJCCS (American Joint Committee on Cancer Staging) criteria was obtained from each remaining patient's CT scans and also, in 32 of 34 patients, by findings on pelvic MRI (23 patients) and transrectal ultrasound (31 patients). Only 2 patients had neither ultrasound nor MRI scan assessment of T stage 1 with involved paraaortic nodes at initial PET, which changed the stage from T3 N0 M0 to T3 N2 M0 and, therefore, the T stage was deemed to be of limited importance. The other progressed to M1 on postchemoradiation PET and was excluded from the surgical series.
Treatment Protocols
All 34 patients had intermittent megavoltage radiotherapy, over 5–6 wk to a total dose of 50.4 Gy to the pelvis given in at least 10 fractions. The target volume included the primary tumor and regional pelvic nodal regions. Treatment planning and dosimetric evaluation with CT was used in all cases. This included conventional simulation with endoluminal contrast material. PET-defined nodal disease was incorporated into the treatment volume even if not involved by CT criteria. Chemotherapy was given for the duration of radiotherapy to all but 2 patients in whom side effects caused early cessation (at 4 wk and after 3 d). In all 34 patients, this consisted of intermittent high-dose 5-fluorouracil infusions with leukovorin rescue or continuous oral medication of capecitabine, a fluoropyrimidine prodrug of 5-fluorouracil. Two other patients received additional oxaliplatin and 1 patient received additional carboplatin. Biopsy confirmation of nodal involvement was not routinely performed.
The decision to proceed to radical surgery was made by the surgeons in consultation with the patients' specialist oncologists and review of PET and CT results in a multidisciplinary clinical review meeting. Of the 34 patients, 30 patients underwent total mesorectal excision by a specialist colorectal surgeon. The surgery was anterior resection in 20, abdominoperineal resection in 9, and pelvic exenteration in 1. The surgical specimens were examined in detail in a university hospital pathology department setting and reports were obtained to determine the presence or absence of residual tumor cells within the primary tumor. All of the excised lymph nodes were examined for the presence or absence of residual tumor, as were any accompanying organ biopsies.
PET Scan Procedure and Interpretation
From 2000 to 2002, PET scans were performed on a GE Healthcare Quest 300-H scanner (UGM Medical Systems Inc.). Emission data were processed using iterative reconstruction both with and without attenuation correction. Transmission data used for attenuation correction were acquired using a 137Cs (single photon) collimated point source. The performance characteristics of this scanner and processing methods have been described previously (20,21). From January 2002, patients were studied on a dedicated PET/CT scanner (Discovery; GE Healthcare) 1 h after injection of 300–400 MBq of 18F-FDG unless the baseline scan had been performed on the older scanner. Bladders were routinely catheterized for studies performed on the 3-dimensional (3D) Quest system and on most studies performed on the 2-dimensional (2D) Discovery system. Images were acquired from the neck to upper thigh. The first scan was performed just before the commencement of treatment. The posttherapy 18F-FDG PET scan was to be performed 3–4 wk after completion of chemoradiation but was dependent on the timing of surgery and booking constraints of a busy clinical PET Center. Posttherapy scanning occurred in all but 1 patient who had a midtherapy PET study (which showed no response) but he refused to undergo a posttherapy scan before surgery.
All baseline PET studies were reported at the time of the scan, in conjunction with the structural imaging data (which was available in all cases), by physicians experienced in PET and CT interpretation. Qualitative analysis of PET metabolic response was determined from side-by-side visual inspection of PET images from the baseline and follow-up PET study and did not rely on the posttreatment CT except for purposes of anatomic localization in the case of PET/CT images. Both PET studies were displayed on a liquid crystal diode screen in a standardized format (22) normalized to background soft tissues outside the radiation treatment volume.
The changes in a tumor's 18F-FDG pattern were scored as follows:
Complete metabolic response (CMR): no identifiable activity in all previously defined sites of 18F-FDG activity or where 18F-FDG uptake was indistinguishable from or less than any diffuse bowel activity immediately adjacent to the original site of uptake and within the radiation treatment volume (Fig. 1).
Partial metabolic response (PMR): incomplete improvement—that is, residual uptake of higher intensity than adjacent bowel and at a site of previous abnormality.
Stable metabolic disease (SMD): where intensity of 18F-FDG uptake was unchanged by treatment.
Progressive metabolic disease (PMD): where new sites of disease or increasing intensity of initially seen sites of abnormal 18F-FDG uptake is evident. For the purposes of this study, SMD and PMD were combined as no metabolic response (NoMR).
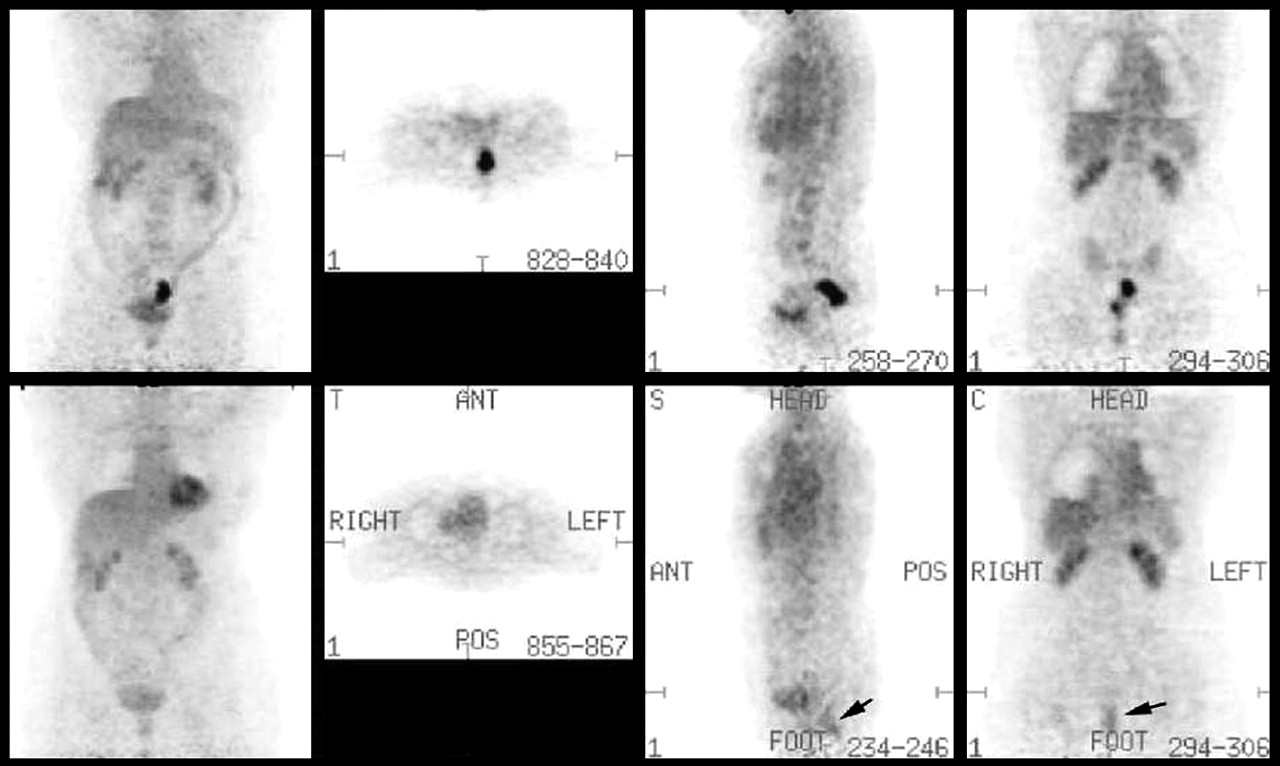
Coregistered and normalized pre- (top) and post- (bottom) chemoradiation 18F-FDG PET scans show complete resolution of metabolic activity at site of this T3 N0 M0 tumor. Reference maximum-intensity-projection images demonstrate normalization of scan appearances. Corresponding transaxial (middle left), sagittal (middle right), and coronal (right) planes through the level of the tumor demonstrate no residual metabolic abnormality and were graded as CMR. Note appearance of mildly increased uptake distal to initial tumor site but within the radiation volume. This was reported as probable radiation proctitis and was consistent with sigmoidoscopy findings. This patient is FFD at 4 y. ANT = anterior; POS = posterior.
On the posttherapy scans, increased uptake proximal and distal to the primary tumoral site and within the radiation treatment volume were interpreted as representing postradiation inflammatory change rather than progressive disease irrespective of the SUV recorded for these sites.
This grading system is potentially limited by using PMR for any degree of incomplete improvement. To determine whether PMR patients could be further stratified by the quantitative degree of their response to chemoradiotherapy, a ratio of the initial SUVmax/posttherapy SUVmax (SUVmax is maximum SUV) was obtained for this subgroup. The absolute SUVmax was not considered suitable for analysis because the study used PET scanners of different generations and crystal type, particularly because one system used a 3D acquisition protocol and the other studies were acquired in 2D mode.
The initial imaging TNM status was determined as follows. The T stage was always obtained from structural imaging (generally either MRI or endorectal ultrasound). A separate N stage was determined independently from pretherapy PET and structural imaging findings. No method of determining the outcomes in discordant results was available because biopsy of suggestive or discordant lesions was not routinely performed before chemoradiation. However, the predictive power of each of the 2 staging methods was compared. The M stage was obtained from structural imaging and PET. Patients with systemic metastasis were defined as having M1 disease with any discordance being resolved by confirmation at surgery or biopsy or on subsequent follow-up imaging.
Clinical Follow-up
Patient follow-up was performed at 3- to 6-mo intervals, in conjunction with medical review and follow-up scans, to establish the presence or absence of ongoing disease. Each patient received further therapy if necessary, as determined by the treating oncologist. Progressive disease was defined as new or expanding lesions on structural imaging; new areas of 18F-FDG uptake, which were subsequently followed by corresponding structural imaging abnormalities; histologic examination of subsequent biopsy specimens from needle biopsies or colonoscopy examinations; or progressive increases in biochemical parameters such as carcinoembryonic antigen (CEA) measurements. Surviving patients were classified as either free from disease (FFD) or alive with disease (AWD) at their dates of last contact. For all patients who died, a cause of death was established from their hospital records or contact with the treating doctor.
Statistical Analysis
Survival was measured from the date of radical surgery to the date of death from any cause. Time to progression was measured from the date of radical surgery to the date of progression. The data were analyzed with a closeout (study censor) date of January 17, 2005. The only patient whose status was unknown at the closeout date was known to be alive and free from progression in November 2004. His survival time and time to progression were censored at this date. Patients who died without progression on, or before, the closeout date had their times to progression censored at the date of death. Survival estimates were obtained using the Kaplan–Meier method. Because of the small number of deaths in the 30 patients undergoing radical surgery, survival comparisons were made using the exact value of the log-rank test for comparing 2 groups. The Cox proportional hazards regression model was used to obtain a test for trend where appropriate. The Fisher exact test was used to compare binomial proportions. All statistical analyses were performed using S-PLUS 2000 (MathSoft, Inc.), SPSS for Windows (10.0.7; SPSS Inc.), and StatXact statistical software (StatXact 6.0; CYTEL Software Corp.). Ninety-five percent confidence intervals (95% CIs) have been given for the main results. One-sided P values have been reported for testing trends with increasing extent of disease, anticipating that the greater the extent of disease, the worse the prognosis. No adjustment has been made for multiple comparisons. Comparisons within the PMR subgroup were performed using a 2-sided Mann–Whitney U test.
RESULTS
The 34 patients who were included in this study had their initial PET study between February 2000 and February 2003. There were 12 females and 22 males, with a mean age ± SD of 62 ± 12 y (range, 33–81 y). Four of these patients did not undergo surgery with curative intent. This included 2 patients initially thought to have only local disease on conventional staging who had M1 disease on PET (subsequently confirmed on structural imaging) and 1 patient who developed distant metastases in the period between the 2 PET studies. All 3 of these patients had their management intent changed by PET from curative to palliative, although 1 patient did undergo local surgery. The fourth patient refused surgery after chemoradiation. In the remaining 30 patients who underwent surgery with curative intent, the time between the completion of chemoradiation and the second follow-up 18F-FDG PET scan occurred at a mean of 26 ± 9 d (range, 7–43 d), with 8 being within 3 wk of ending treatment. These patients were analyzed for survival. The potential follow-up duration from the date of surgery to the closeout date ranged from 1.6 to 4.7 y, with an estimated median duration of 3.1 y.
The pathologic findings from the surgical specimens and the effect of therapy on the 18F-FDG PET scans are found in Table 1. Note that only 6 of 30 M0 patients who had potentially curative surgery had a complete pathologic response. These included 5 of 17 (29%) apparently CMR patients and 1 false-positive PMR patient, where the only abnormality was a site of abscess formation around the rectum at the prior tumor site. This patient remains FFD at 3.6 y. Examination of the surgical specimens also demonstrated clear surgical margins in 28 patients. One T3 patient (PET CMR) had tumor cells at >2 mm from the radial margin of the tumor and just beyond l0 mm from the distal longitudinal margin, and a T4 patient (PET PMR) had tumor at the margin of the operative specimen. Both remain FFD.
PET Response, Prechemoradiation TNM Stage, and Surgical Pathology
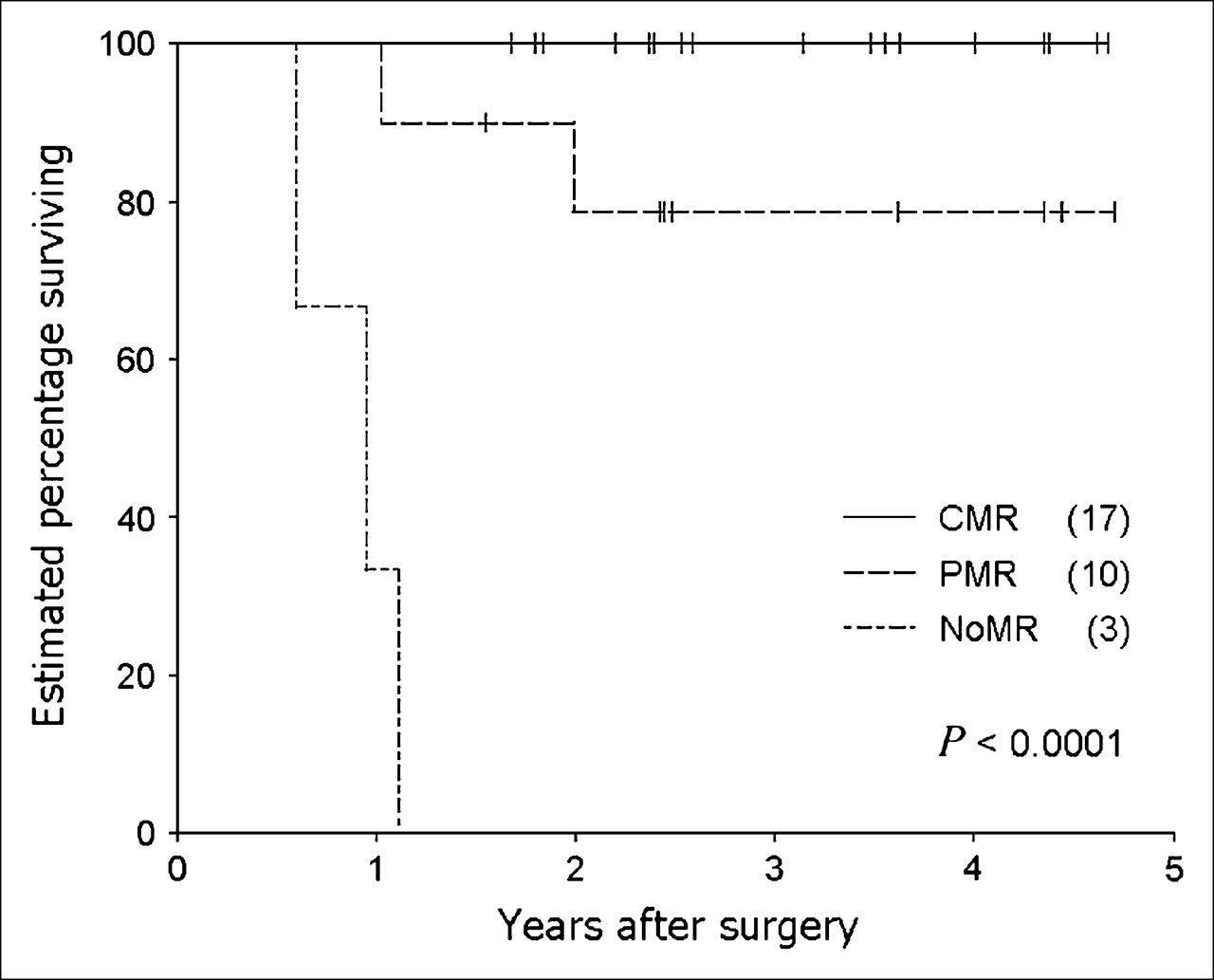
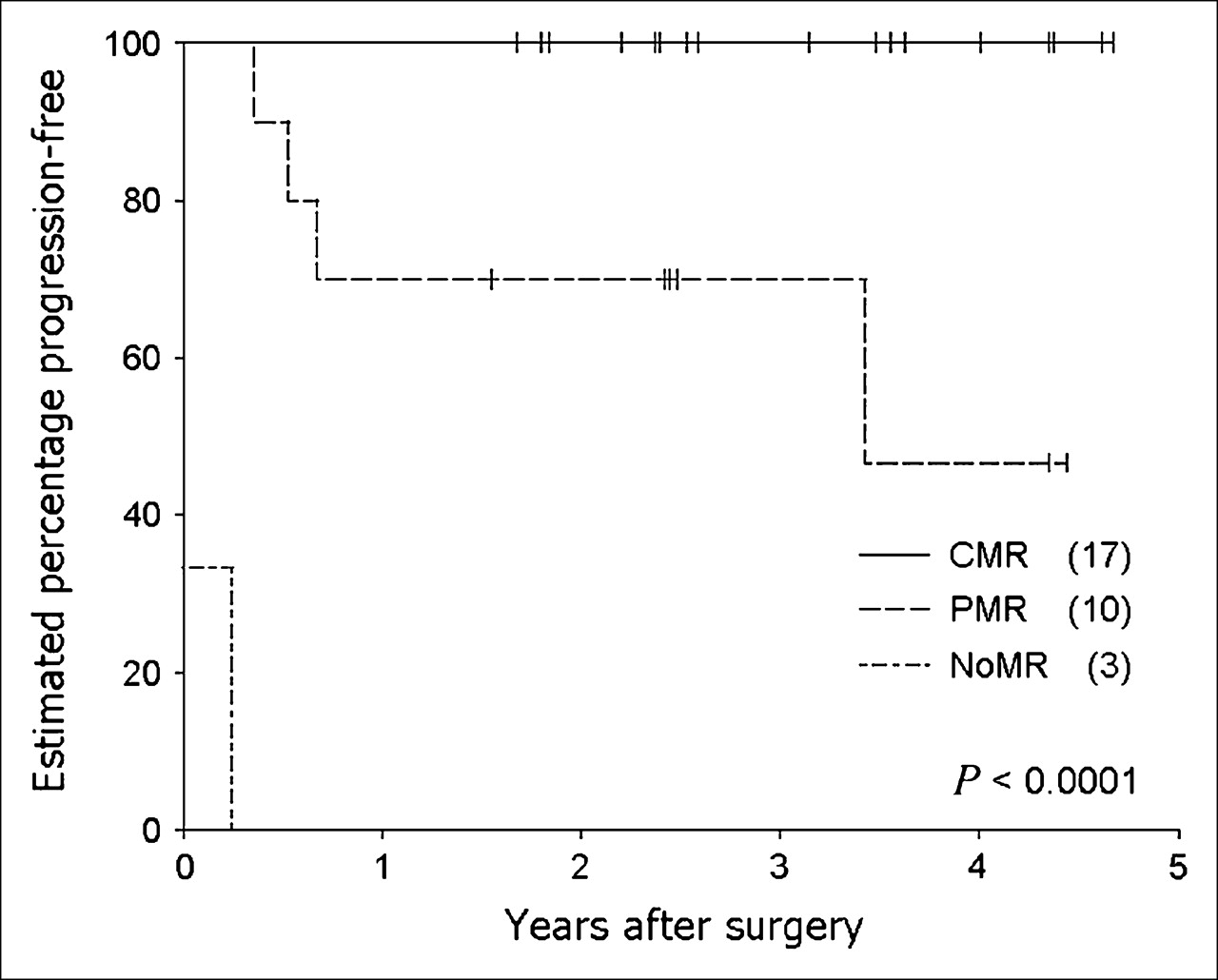
Table 2 shows the influence of PET metabolic response, CT/MRI response, absence of residual tumor on histology and prechemoradiation T stage on survival, and time to progression after radical surgery. PET response was highly significantly associated with overall survival duration (P < 0.0001; Figure 2) and time to progression (P < 0.0001; Figure 3). PET response was also a highly significant prognostic factor when data were analyzed for presence or absence of CMR (P = 0.0095 and P = 0.0008, respectively) Note that at closeout, all 17 patients with PET CMR were FFD. However, all 3 NoMR patients have died of their disease. In the remaining 10 PMR patients, 6 remain free of disease at study closeout (although 1 had a mildly raised CEA: 5.5), 1 is alive with distant metastases, 1 has very extensive local recurrence, and 2 have died of widespread metastatic disease. In the PMR subgroup, there was no significant difference (P = 0.35:) between the percentage of SUVmax reduction of those who relapsed (50% ± 16%) versus those whose who remain FFD (40% ± 18%).

Kaplan–Meier survival curves illustrate highly significant effect of PET-determined metabolic response to chemoradiation on overall survival in the 30 T3/4 Nx M0 patients who underwent radical surgery. (X) = number of patients in each group.
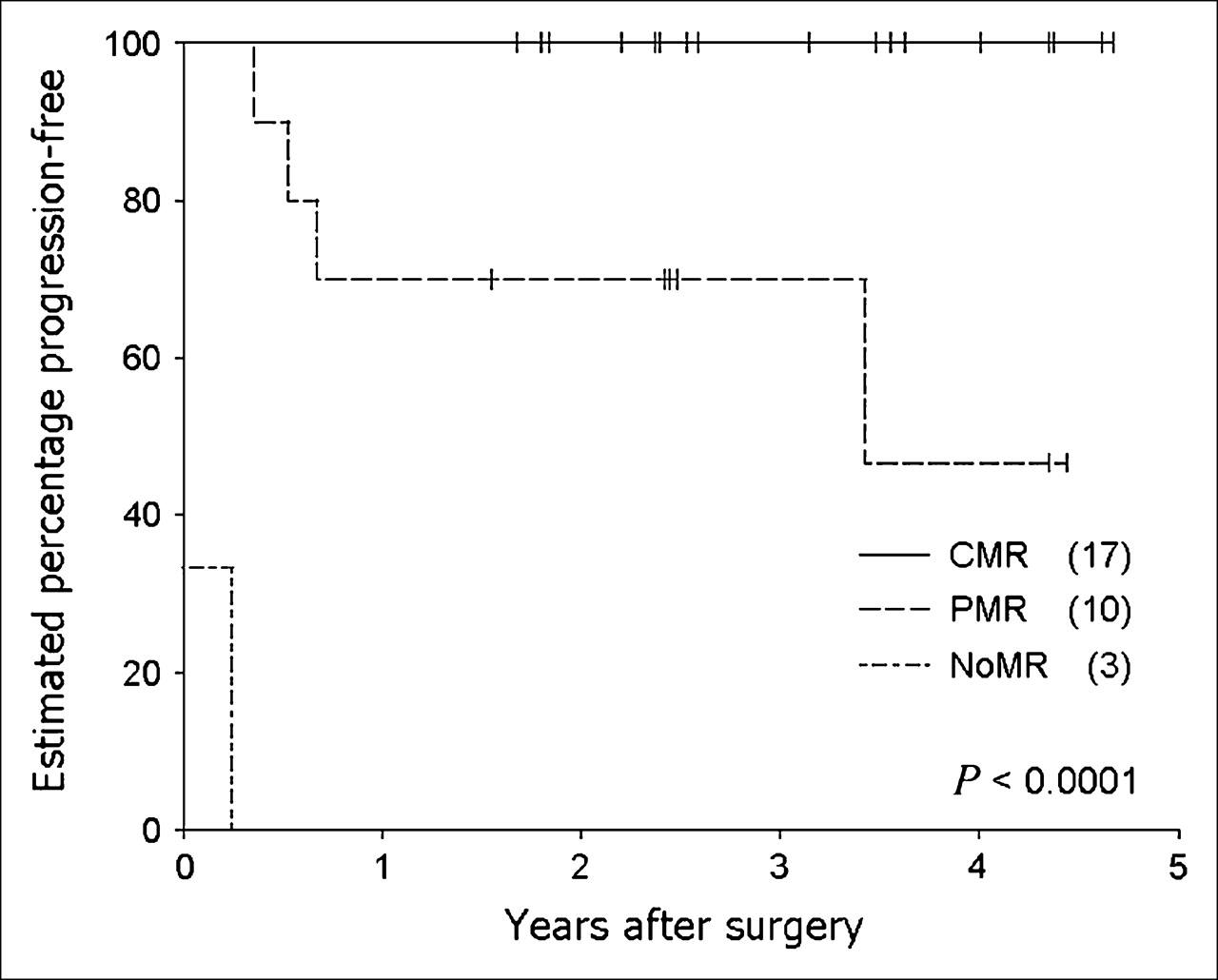
Very significant effect of PET metabolic response to chemoradiation on time-to-disease progression is demonstrated in Kaplan–Meier plot. (X) = number of patients in each group.
Estimated Survival and Time to Progression After Radical Surgery
There was a statistically significant trend for an increasing degree of spread of tumor at surgery (none vs. primary site only vs. primary and nodes) to be associated with decreasing overall survival duration (P = 0.027; Figure 4), but there was no similar association with the time to progression.
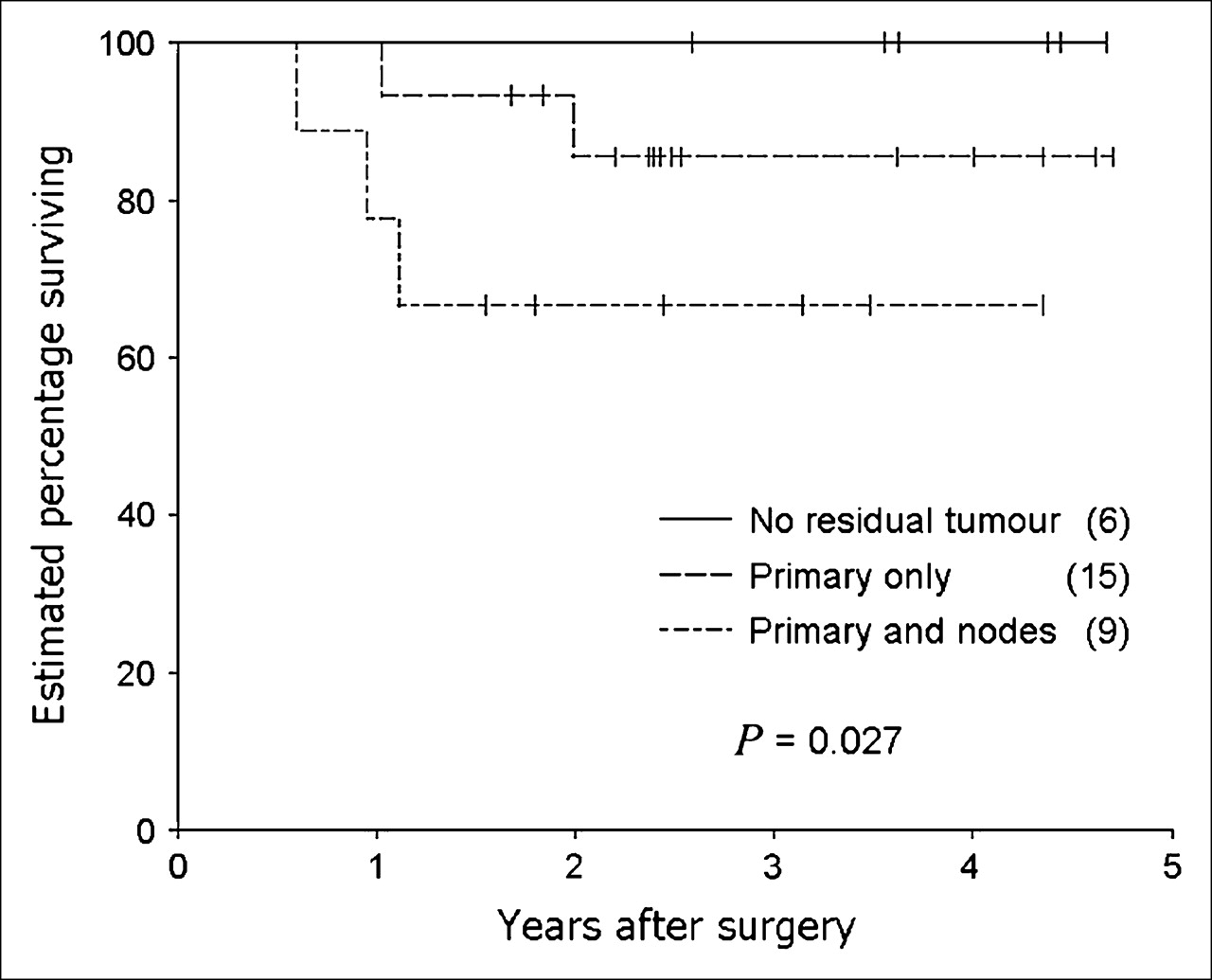
Kaplan–Meier survival curves show significant effect of degree of residual tumor at laparotomy on overall survival in the 30 Tx Nx M0 patients who underwent radical surgery. Note small number of patients with no evidence of residual tumor in this patient population. (X) = number of patients in each group.
Although clinically important survival differences were associated with histologic evidence of residual tumor in regional lymph nodes and T stage on prechemoradiation structural imaging (Fig. 5), these differences were not statistically significant, possibly because of the small number of patients studied. Of interest, but not shown in Table 2, is the observation that the prechemoradiation N stage—whether defined by PET or structural imaging—was not predictive of outcome.
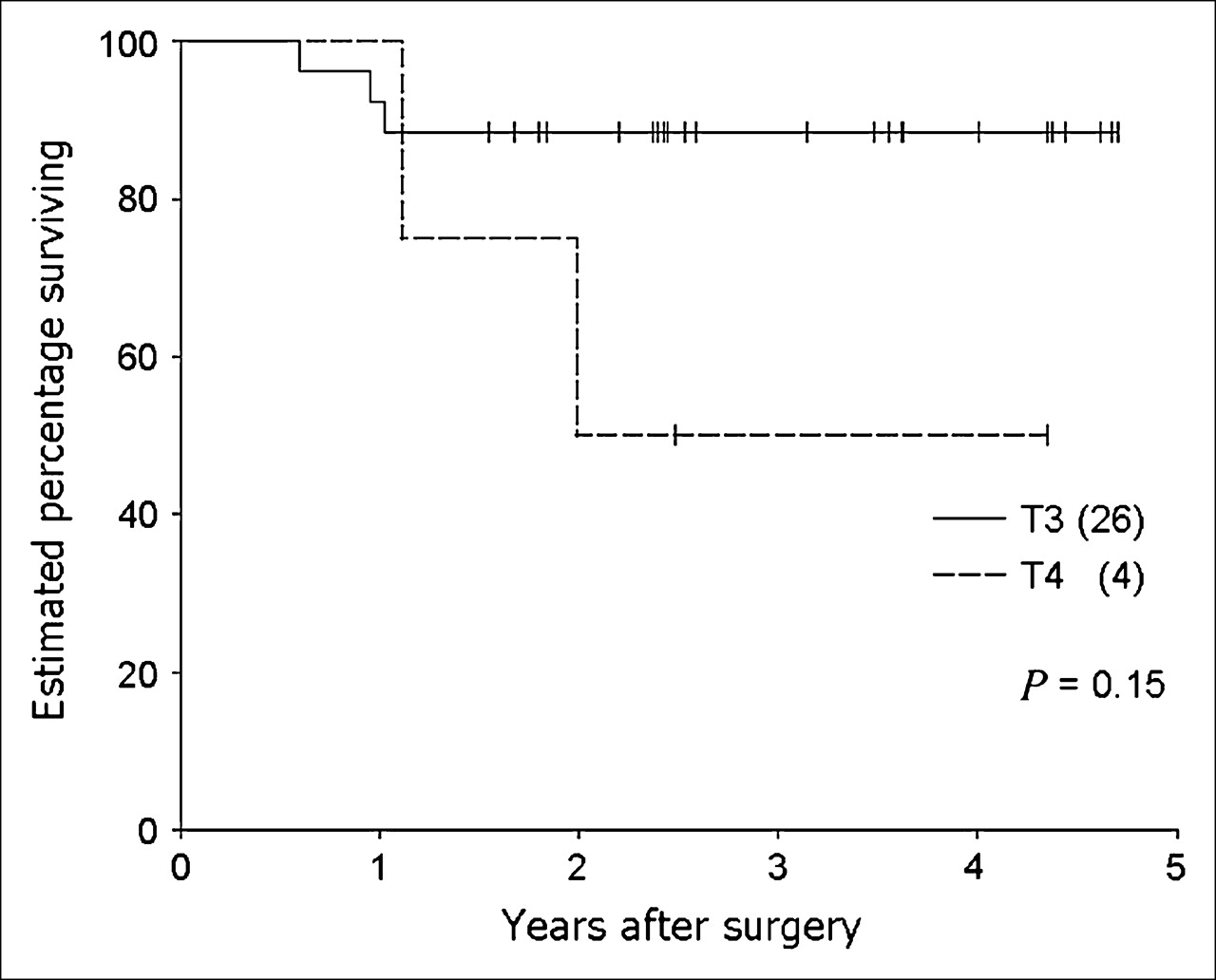
Kaplan–Meier survival curves show effect of initial tumor T stage on overall survival in the 30 Tx Nx M0 patients who underwent radical surgery. Small number of patients with T4 limits evaluation of the prognostic power of this parameter. (X) = number of patients in each group.
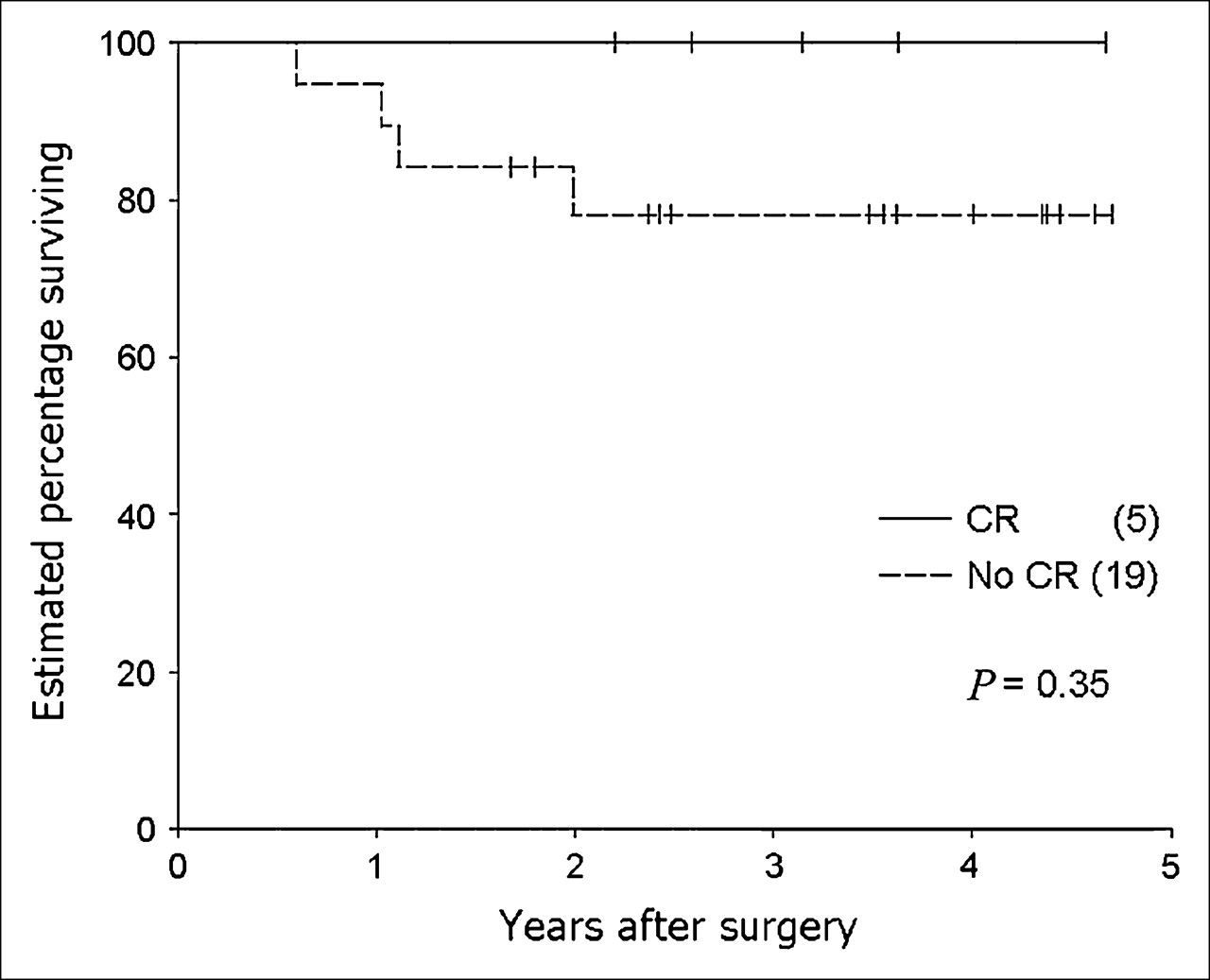
In the 24 of 30 patients who had both pre- and postchemoradiation CT or MRI scans, the CT/MRI response was not a statistically significant prognostic factor (Fig. 6). Although a complete response was associated with a good outcome, there were only 5 such patients. All 5 patients also achieved a PET CMR, as did 9 of the remaining 19 patients.

Kaplan–Meier curves illustrate effect of CT/MRI response to chemoradiation on overall survival. There were no deaths before the closeout date in the complete response (CR) subgroup, but there were only 5 patients in this category. (X) = number of patients in each group.
Radiation proctitis, as defined in this study, did not pose a significant problem for scan interpretation, occurring in only 2 patients (imaged 29 and 35 d after chemoradiation). However, the possibility that imaging performed earlier after chemoradiation may have underestimated the therapeutic response (particularly in PMR patients) is more difficult to exclude. Based on the shortest interval—between treatment and imaging in patients with PMR who relapsed—being 22 d, we defined PET scans <3 wk after chemoradiation as being “early.” There were 8 patients in this subgroup: 5 CMR and 2 PMR, all FFD, and 1 NoMR patient: DOD. Although FFD was achieved in both PMR patients in this early subgroup compared with 4 of 8 remaining PMR patients, both still had residual viable disease on surgical pathology. Furthermore, the mean interval—from the end of treatment to imaging of the PMR patients who relapsed—was not significantly different in the PMR patients who remained FFD, 26 + 3 d (range, 22–28 d), compared with 25 + 9 d (range, 10–44 d) for PMR patients who remained FFD (P = 0.60). Therefore, it appears unlikely that early imaging contributed to a substantially lower positive predictive value for treatment failure.
Follow-up of the 4 patients who completed chemoradiation but were excluded from survival analysis because surgery with curative intent was not performed found that 3 died of distant disease at 11, 12, and 20 mo. One PET-defined M1 patient had palliative surgery (abdominoperineal resection) and remains alive with extensive distant disease at 32 mo, having responded well to initial chemoradiation and subsequent chemotherapy.
DISCUSSION
This study has shown that using simple qualitative assessment of posttreatment 18F-FDG PET uptake after aggressive chemoradiation but before surgery is able to prognostically stratify patients with locally advanced M0 rectal cancer even in patients who undergo what is hoped to be curative surgery. A CMR on 18F-FDG PET appears to offer a very good medium-term prognosis despite more than two thirds of these patients still showing evidence of tumor cells in their postoperative specimens. Conversely, patients who show NoMR do badly despite apparently complete resection. Patients who show a partial reduction in 18F-FDG–avid disease have an intermediate prognosis, which in this series did not appear to be further refined by the use of currently accepted (23) semiquantitative techniques. Finally, this study again demonstrates that a small but significant number of patients (3/34) with apparently localized extensive rectal cancer on structural imaging alone have distant metastases found on 18F-FDG PET that change their planned management from curative to palliative intent (15,21,24).
Local tumor recurrence after resection of rectal cancer is a challenging problem for both surgeons and oncologists. High surgical patient numbers (25), subspecialty colorectal training (26), resection with total mesorectal excision (27), and adequate longitudinal (28) and circumferential margin (29) have all correlated with improved outcome. Patients with T4 rectal cancers can achieve survival rates similar to those with less advanced tumors if en bloc resection of involved structures is performed with clear margins (30). All patients in this study had optimal definitive tumor resection performed by colorectal surgeons in tertiary hospitals. Within a predefined group of patients with locally advanced rectal cancer, this study has found that metabolic response after completion of chemoradiation may provide the most useful information regarding medium-term prognosis. The good prognosis of M0 patients achieving a CMR compared with those with a PMR or NoMR, even when all patients underwent surgery with curative intent, suggests that PET can accurately evaluate biologic response to chemoradiation. Presumably this may be because responsiveness of cells at sites of macroscopic disease, able to be visualized by PET, and included within radiation and surgical resection volumes, reflects the responsiveness of microscopic foci of disease beyond the treatment margins and undetected by current imaging techniques.
The presence of at least microscopic disease in the surgical specimens of most of the M0 patients with apparently complete remission on 18F-FDG PET is in keeping with the known spatial limitations of 18F-FDG PET. Other 18F-FDG PET rectal cancer studies with more comprehensive pathologic examination of the operative specimens after adjuvant chemoradiation (12,13,16) have found that, although the degree of 18F-FDG uptake was proportional to the percentage of malignant cells present in the operative specimen, very few were completely clear of histologically evident disease. Thus, until it can be proven that the apparently viable tumor cells have lost their ability to proliferate, surgery in CMR patients is still required. This conclusion is further supported by an early study (31) which found that an apparently complete 18F-FDG response to adjuvant radiotherapy alone without surgery was still associated with early local recurrences in one third of cases.
Our findings are consistent with other studies of neoadjuvant chemoradiation in that the majority of patients responded favorably to the initial chemoradiation (12,13,16) and that prognosis was related to the presence of residual disease in the primary or resected nodes, as has been generally found in larger surgical series (6,7,32,33). The poor stratification of patient outcome by CT or MRI response is in keeping with the known limitations of structural imaging in this situation. The low frequency (22%) of complete resolution of structural abnormalities with chemoradiation seen in this study and the inability of these imaging modalities to determine the presence or absence of residual disease in these structures appear to account for these difficulties.
Quantitation of 18F-FDG uptake (34) is appealing because the degree of 18F-FDG uptake appears to reflect tumor aggressiveness and, therefore, potentially an independent predictor of patient outcome (35). However, the optimum methodology for quantitative analysis and the accuracy of retrospectively determined threshold values for such approaches have not been prospectively validated in rectal cancer (13–16). Whatever the technique, considerable variability still remains in the outcome of those patients with values close to the cutoff values of the derived thresholds. Our PMR subgroup likely corresponds to the group with intermediate reduction in quantitative parameters of 18F-FDG uptake; thus, it is not surprising that the percentage of SUV change did not further stratify this subgroup.
The potential reasons for the limitations of quantitative approaches (22,36) include variability in tumor size, true disease burden, tumor aggressiveness, responsiveness to therapy, degree of inflammatory response generated by therapy, size of radiation field, degree of tumor hypoxia, and adequacy of surgical resection. However, our study suggests that these complex interactions are less predictive of outcome than the simple qualitative assessment of whether 18F-FDG PET abnormalities have responded to therapy. In particular, resolution of 18F-FDG–defined disease after chemoradiation appears to be the best predictor of survival in patients undergoing surgery with curative intent. These findings are consistent with the prognostic utility of standardized qualitative scoring of metabolic response in lymphoma (18) and lung cancer (17). Thus, given the lack of consensus regarding the optimum methodology for semiquantitative or quantitative analysis and classification of therapeutic response, qualitative reporting represents a reasonable approach for clinical implementation and should be further tested in other oncologic therapeutic intervention studies.
There are several limitations in this study. The initial part of the study used a sodium iodide PET camera, which has a lower sensitivity for small-volume intraabdominal disease than contemporary PET scanners (37). Nevertheless, we have demonstrated that this older system has good diagnostic accuracy and is clinically useful in colorectal malignancy (21,38). Further, the good prognosis of patients with a CMR in this series suggests that false-negative results did not significantly impact outcome in those undergoing curative resection. The longer follow-up of patients imaged on this system warrants their inclusion in a series evaluating the prognostic ability of metabolic response in rectal cancer. PET/CT significantly improves certainty of separation of disease from normal physiologic uptake (12) but it remains to be established to what degree it will improve stratification beyond having the ability to perform contemporaneous correlation of structural and functional imaging. The change to a dedicated PET/CT camera precluded the use of the initial or posttherapy SUVmax measurement as a potential prognostic indicator. Because follow-up studies were performed on the same scanner as the baseline scans, it was possible to determine the percentage change in SUVmax in PMR patients. This parameter did not appear to further stratify this patient subgroup, but larger patient numbers may enable further prognostic stratification within partial metabolic responders.
Another potential limitation was the necessity to image some patients <3 wk after chemoradiation, thereby possibly reducing the likelihood of PMR patients becoming complete responders. However, both PMR patients who were imaged early after treatment still had residual viable tumor, suggesting that this was not a major confounder in this study. The incidence of radiation proctitis was also quite low and did not limit image analysis, although some contribution to activity seen in the PMR patients cannot be excluded and remains a potential problem for all PET studies.
The relatively small number of patients also prevented us from examining the interrelationships between several of the variables analyzed and was possibly responsible for some of them not reaching statistical significance. However, the observed trends were generally in the directions to be expected and were consistent with clinically important differences in outcome. The fact that the 18F-FDG PET response remained a powerful prognostic factor suggests that the signal measured by 18F-FDG PET is robust.
Finally, although the prognostic ability of this technique appears quite useful for a medium-term outlook, the time of follow-up in our surviving subjects precludes us from offering valid comment on the long-term survival benefit of 18F-FDG findings. This may require up to 6 y as radiotherapy alone for advanced rectal cancer has a median time to relapse of 34 mo for local and 24 mo for distant metastases (39).
CONCLUSION
The current study found that visual analysis of posttreatment 18F-FDG PET scans can provide information regarding the prognosis of patients undergoing curative resection of rectal cancer after neoadjuvant chemoradiation. Although a CMR with 18F-FDG PET does not indicate a complete pathologic response in most cases, it confers a good medium-term prognosis. An incomplete metabolic response—and, in particular, lack of metabolic response—carries a poor prognosis even after surgery. The relevance of this study's findings includes the need for trials of further adjuvant therapy to be initially focused on this latter patient subgroup.
Acknowledgments
We acknowledge the radiochemists and nuclear medicine technologists of The Peter MacCallum PET Center for their role in imaging these patients; and the colorectal surgeons, oncologists, and general practitioners who provided the clinical follow-up information that is so necessary for this type of study.
References
- Received for publication July 21, 2005.
- Accepted for publication October 18, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 15-Year Experience of 18F-FDG PET Imaging in Response Assessment and Restaging After Definitive Treatment of Merkel Cell Carcinoma
- The Role of Interim 18F-FDG PET/CT in Predicting Early Response to Neoadjuvant Chemotherapy in Breast Cancer
- [18F]FDG PET/CT imaging of colorectal cancer: a pictorial review
- Monitoring and Predicting Response to Therapy with 18F-FDG PET in Colorectal Cancer: A Systematic Review
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors
- Time Course of Early Response to Chemotherapy in Non-Small Cell Lung Cancer Patients with 18F-FDG PET/CT