


Abstract
Some authors have suggested that chronic octreotide use enhances the efficiency of radiolabeled somatostatin receptor (sst) imaging. Conversely, desensitization of sst on tumor tissue (tachyphylaxis) may occur occasionally in patients on chronic octreotide therapy. Assuming that chronic exposure to octreotide induces tachyphylaxis, we hypothesized that chronic exposure of sst subtype 2 (sst2)–expressing cells to octreotide would downregulate binding of 111In-pentetreotide to sst and that this downregulation would be due to a reduction in the gene copy number for sst2. Methods: The clinical scenarios of acute (24 h) and chronic (2 wk) octreotide use, followed by either nuclear imaging exposure (8.6 pmol/L) or therapeutic exposure (510 pmol/L) to 111In-pentetreotide, were modeled in vitro. Receptor binding in IMR-32 human neuroblastoma cells (high sst2 expression) and PANC-1 human pancreatic cancer cells (no detectable sst2 expression) was evaluated. Gene copy numbers for sst subtypes 1−5 in IMR-32 cells were determined by quantitative polymerase chain reaction. Results: Acute or chronic octreotide exposure at low or high doses did not significantly alter sst2 gene copy numbers or binding of either the diagnostic dose or the therapeutic dose of 111In-pentetreotide. Conclusion: In vitro exposure of cells to low or high doses of octreotide for 1–14 d does not result in the development of either tachyphylaxis or upregulation of sst as assessed by changes in gene expression or in high-affinity binding.
Octreotide acetate (OA), an octapeptide somatostatin analog, is a somatostatin receptor (sst) agonist that is used widely in the treatment of sst-expressing neuroendocrine tumors (1–4). A long-acting formulation of this drug, Sandostatin LAR (Novartis Pharmaceutical Co.), administered monthly, is commonly used for the long-term management of the symptoms of diarrhea and flushing associated with the carcinoid syndrome. Alternatively, in some patients, multiple daily subcutaneous injections or continuous subcutaneous infusions (by pump) are used to control the symptoms of these neuroendocrine tumors.
Clinical observations suggest that desensitization of the target tumor tissue (tachyphylaxis) is occasionally a problem in patients using chronic octreotide therapy (5–7). In contrast, some nuclear medicine physicians have noted that chronic octreotide use enhances the efficiency of nuclear imaging with radiolabeled somatostatin analogs (8,9). Finally, some pharmacologists argue that octreotide treatment may have differing effects on sst subtype 2 (sst2) expression or binding depending on the length of treatment and the dose of octreotide (10).
Radiolabeled somatostatin analogs such as 111In-pentetreotide (OctreoScan; Mallinckrodt Medical) are widely used for diagnosis and more recently for targeted radiotherapy. 111In-Pentetreotide is formulated by conjugating 111In to the octreotide–chelator (diethylenetriaminepentaacetic acid) complex. This complex is used in low doses (222 MBq) for imaging and at high doses (6.7–22.2 GBq) for targeted radiotherapy (11).
Receptor-specific cytotoxicity (DNA damage) is produced by Auger electrons emitted from the 111In when it is internalized within the sst2-expressing cells. These Auger electrons have short radii of action; thus, 111In-containing analogs must be internalized to optimize their cytotoxic effects. Higher-energy 90Y- and 177Lu-labeled analogs with greater radii of action are also in therapeutic clinical trials (12,13). These high-energy radiolabeled analogs exert cytotoxic effects not only on the cell to which they bind but also for millimeters to centimeters around the source of radioactive emission, generating an “innocent bystander” effect. The advantage of these targeted radiotherapies is a high degree of specificity due to the high sst expression in neuroendocrine tumors and a relatively lower sst expression in most normal tissues.
If tachyphylaxis occurs in patients receiving long-term octreotide treatment, whether by frequent short-acting subcutaneous injection, by continuous subcutaneous pump delivery, or by monthly subcutaneous long-acting release, the efficacy of this therapy would be expected to decrease over time. Similarly, if receptor downregulation occurs at the gene expression level or inhibition of receptor recycling occurs at the cell membrane level, the efficacy of 111In-pentetreotide, when given at either diagnostic or therapeutic doses, would theoretically decrease in patients using chronic octreotide therapy. Assuming that chronic exposure to octreotide induces tachyphylaxis, we hypothesized that chronic exposure to octreotide would downregulate receptor binding and that this decrease in binding might be the result of sst downregulation at the gene level.
MATERIALS AND METHODS
In Vitro–In Vivo Modeling
In an effort to model the possible clinical scenarios of octreotide use and subsequent diagnostic scanning or therapy with a radiolabeled somatostatin analog, we constructed 3 in vitro scenarios.
Scenario 1 attempted to model an untreated patient. Cells were not pretreated with octreotide and were subsequently exposed to either a low (diagnostic) or a high (therapeutic) dose of 111In-pentetreotide for binding studies. Untreated cells were harvested and frozen at −80°C for subsequent determination of the sst gene expression copy number by quantitative polymerase chain reaction (PCR).
Scenario 2 attempted to model a patient who is using multiple daily doses of subcutaneous octreotide and who stopped therapy for 48 h before exposure to either diagnostic or therapeutic doses of 111In-pentetreotide. The aqueous form of OA has a relatively short (90−120 min) half-life in plasma. Scenario 2 was represented by cells treated with a moderate dose of octreotide (5 × 10−9 mol/L) for 2 wk, washed, allowed to recover in growth medium for 48 h, and then exposed to a low (diagnostic) or high (therapeutic) dose of 111In-pentetreotide. Paired cell cultures were exposed to octreotide at 1 × 10−8 or 1 × 10−12 mol/L for 1 or 14 d and then frozen at −80°C for subsequent determination of the sst gene expression copy number by quantitative PCR.
Scenario 3 attempted to model a patient receiving chronic long-acting-release therapy. A long-acting-release dosage of 30 mg/mo provides an average plasma level of 5 nmol/L (14). Cells were exposed to octreotide at 5 × 10−9mol/L (5 nmol/L) for 2 wk and either were not washed (octreotide present during 111In-pentetreotide scanning or therapy) or were washed immediately before exposure to a low (diagnostic) or high (therapeutic) dose of 111In-pentetreotide for binding analysis (as an assay control). No additional cells were treated for subsequent analysis of sst gene expression copy number by quantitative PCR, because this step was done in scenario 2.
Cell Cultures
To test these hypotheses, we obtained IMR-32 human neuroblastoma cells, which have previously been shown to express sst2 (CCL-127; American Type Culture Collection) (7), and PANC-1 human pancreatic epithelial carcinoma cells, which do not express sst2 (CRL-1469; American Type Culture Collection) (15), and maintained them in culture at 37°C in humidified air with 5% CO2. IMR-32 cells were cultured in Eagle's minimum essential medium with Earle's salts (Gibco) and supplemented with nonessential amino acids, 15% fetal bovine serum (Gibco), and an antibiotic–antimycotic agent (Gibco). PANC-1 cells were cultured in Dulbecco's modified Eagle's medium (Gibco) supplemented with 10% fetal calf serum and antibiotic–antimycotic solution. Both cell lines were passaged once a week; PANC-1 cells were passaged with trypsin (0.25%) and ethylenediaminetetraacetic acid (1 mmol/L), and IMR-32 cells were passaged without enzymatic digestion.
Treatment
For binding experiments, flasks of cells for each cell line were exposed to OA (Sandostatin, 5 nmol/L) for 2 wk or were left untreated as controls. The concentration of OA corresponded to the average plasma level obtained with a 30-mg dose of Sandostatin LAR OA, or a 0.5 mg/d infusion (14). The 3 scenarios required that cell treatment with OA be terminated at cell harvest or plating to set up multiwell plates for the binding experiments (2 d before addition of the radioactive ligand) (scenario 1) or terminated immediately before the addition of radioactive ligand for binding (scenario 2) or not terminated at all (scenario 3). Cells were harvested and counted, and the 3 groups of OA-treated cells were seeded into 6-well culture plates (Costar) at 5 × 104 cells per well. Untreated cells were also harvested and plated for binding experiments. Once the cells had been harvested and plated, cell treatment was terminated at the specified times. The cells in scenario 1 (the first plate) were washed and allowed to recover from the OA treatment for 48 h in growth medium before incubation with 111In-pentetreotide. The cells in scenario 2 (the second plate) were rinsed immediately before incubation with 111In-pentetreotide. For the cells in scenario 3 (the third plate), OA treatment (5 nmol/L) was continued during the incubation with 111In-pentetreotide (i.e., no termination). A fourth plate was seeded with cells that had not been pretreated with OA and served as the control.
Quantitative PCR was used to determine the effect of short- or long-term octreotide exposure on sst copy number. IMR-32 cells were exposed to OA for short (1 d) or long (2 wk) periods. Two concentrations of OA were used for each exposure period: 1 × 10−8 mol/L (high-dose octreotide exposure, equivalent to 60 mg of octreotide per month) and 1 × 10−12 mol/L (low-dose octreotide exposure, equivalent to 100−150 μg 3 times per day). Control cells were maintained in growth medium. Rinsed cells were harvested, frozen, and stored at −80°C before RNA extraction. Cells were maintained at logarithmic growth for the duration of this experiment.
Binding
The radioligand, 111In-pentetreotide, was prepared using a modification of the method used to prepare an 111In-pentetreotide kit (16). Specific activity for 111In-pentetreotide is approximately 1,720,833 GBq/mmol. For each cell line, sst binding (sst2) was estimated using 111In-pentetreotide at 2 concentrations to mimic conditions for either a diagnostic (222 MBq) or therapeutic (13.3 GBq) dose of the radiolabel. To calculate these levels, we estimated the volume of distribution of the radiolabeled drug using 15 L as an average distribution volume (17). The diagnostic dose (222 MBq) provided an 8.6 pmol/L concentration (14.8 kBq/mL; 630,000 cpm per well), whereas the therapeutic dose (equivalent to 13.3 GBq) provided a 510 pmol/L concentration (888 kBq; 3.78 × 107 cpm per well). OA (1 μmol/L) was added to 3 of the 6 wells per plate to assess nonspecific binding.
After 24 h of exposure to 111In-pentetreotide, the cells were washed with ice-cold phosphate-buffered saline (pH 7.5) and harvested, and cell-associated radioactivity was determined using a γ-counter (Gamma 5500; Beckman). This value represents total specific binding. Internalized radioligand was estimated by release of surface-bound peptide with a brief acid wash (10 min with ice-cold phosphate-buffered saline, pH 4.0). Residual radioactivity associated with the cells (internalized) was again determined using a γ-counter. Data were normalized to cellular protein using a Bradford assay (Sigma), and specific binding was expressed as cpm/μg of protein. ANOVA with Bonferroni corrections using combined data (2 experiments; n = 6) was performed for the control and 3 treatment groups for each dose of 111In-pentetreotide.
Gene Expression
The effect of short- and long-term OA treatment on expression of the somatostatin and sst subtypes 1−5 (sst1−sst5) in IMR-32 cells was determined by quantitative PCR as we have previously described (18). Briefly, total RNA was isolated from IMR-32 cells and from the TT thyroid carcinoma cell line, which expresses high levels of both somatostatin and sst2 as well as the SKNSH neuroblastoma cell line transfected with sst1, as shown in Table 1. DNA contamination was removed with the RNeasy MiniKit (Qiagen Inc.). The RNA was then converted to complementary DNA (cDNA) using a reaction mixture of 2 μg of RNA, 200 units of SuperScript II RT (Invitrogen Co.), 500 nmol of dNTPs per liter, 133 ng of random hexamers, 2.5 mmol of MgCl2 per liter, 10 mmol of dithiothreitol per liter, 2 μL of 10× PCR buffer, and H2O to a final volume of 20 μL under the following conditions: 70°C for 10 min, 25°C for 10 min, 42°C for 50 min, and 70°C for 10 min. A reaction without reverse transcriptase was included as a check for genomic DNA contamination. This control is important to ensure that RNA, rather than genomic DNA, is being quantified for intronless genes such as sst1−sst5 (19).
Primer Set and Probes for Quantitative PCR
Oligonucleotide primers and probes for quantitative PCR were designed with Primer Express software (version 1.0; Perkin-Elmer) on the ABI Prism 7700 sequence detector (Perkin-Elmer) and purchased from Applied Biosystems. The primers, probes, and positive control tissue are listed in Table 1. The primers and probe for ribosomal RNA (18S rRNA) were obtained from PE Biosystems and were used as the internal control in each reaction. Quantitative PCR was conducted under the following conditions: 12.5 μL of TaqMan 2× PCR mix (Perkin-Elmer), 1.8 μmol of target primers per liter, 100 nmol of target probe per liter, 2.5 μL of a 1:10 dilution of cDNA synthesis product, 125 nmol of 18S rRNA primers per liter, and 250 nmol of 18S rRNA probe per liter. The quantitative PCR was run for 40 cycles on the ABI Prism 7700. PCR was performed in triplicate for each treatment, with each treatment performed in triplicate. Data were analyzed using the software of the ABI Prism 7700.
RESULTS
Binding
Receptor-specific binding was dependent on the presence of membrane-bound sst2 as demonstrated by the very low specific binding of 111In-pentetreotide in the sst-negative PANC-1 cells under any treatment condition (Fig. 1). In the IMR-32 cells exposed to low-dose 111In-pentetreotide for binding analysis (8.6 pmol/L, 222 MBq; Fig. 1A), a slight increase in binding, compared with control values (14%), was observed in the octreotide-treated cells that had been allowed to rest in drug-free medium for 48 h. A slight decrease in binding, compared with control values, was observed in octreotide-treated cells that were either unwashed (18%) or briefly washed (25%). However, the differences from control values were not statistically significant in any of these treatment groups. When a higher dose of 111In-pentetreotide was used for binding analysis (510 pmol/L, 13.3 GBq; Fig. 1B), an increase in specific binding was observed in all groups. As was seen using a lower concentration of radioligand, all binding levels with 510 pmol of 111In-pentetreotide per liter were statistically similar to control values. Values for internalized radioligand were roughly 60% of total binding in all treatment groups, which is consistent with previously reported data (16). The OA treatments induced no detectable morphologic changes.
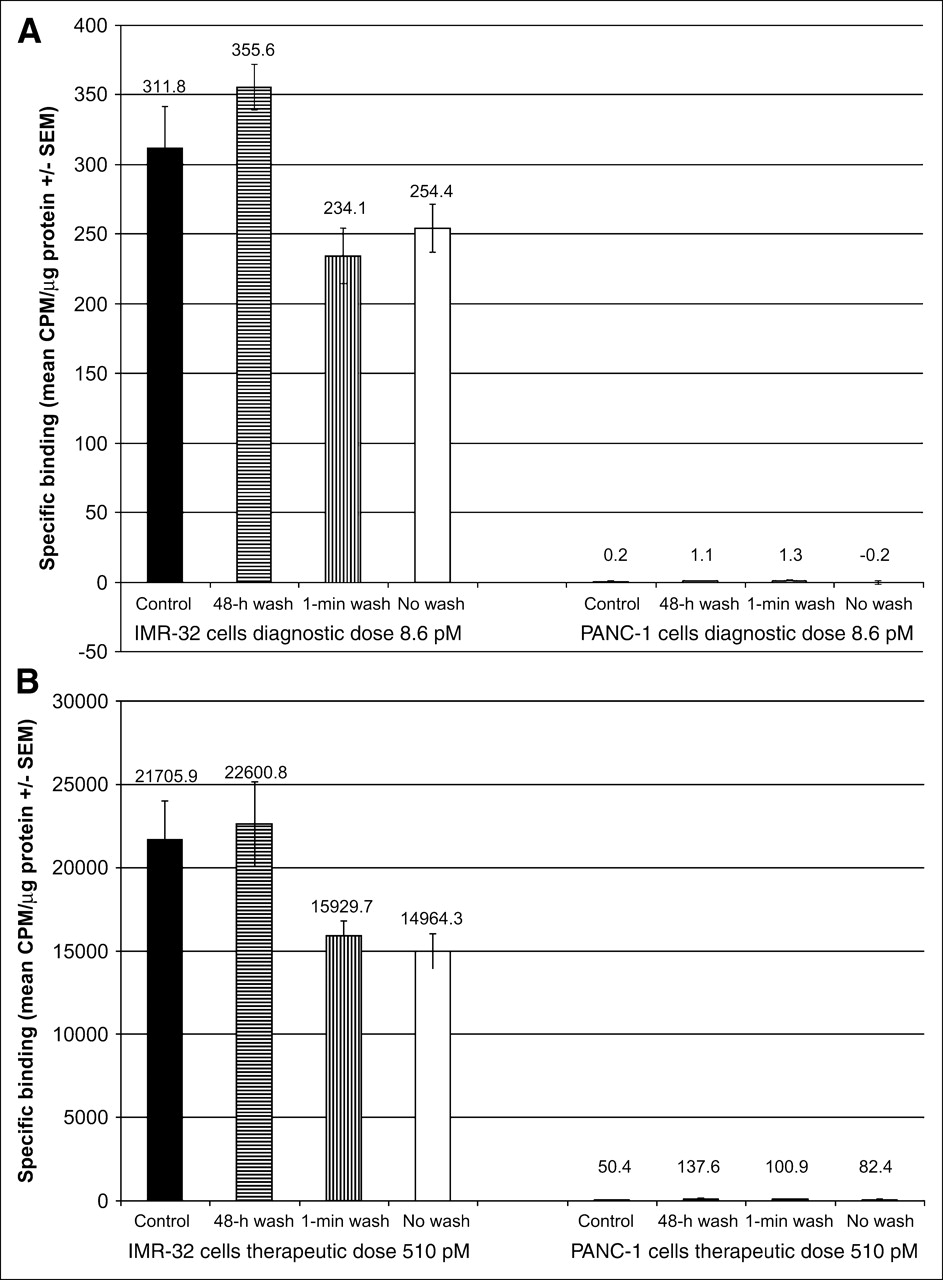
Effect of OA pretreatment on specific binding of 111In-pentetreotide in cells. Binding of sst was assessed in cells pretreated with OA, 5 nmol/L, for 2 wk. Binding conditions included incubation with diagnostic dose (8.6 pmol/L) (A) or with therapeutic dose (510 pmol/L) (B) of 111In-pentetreotide in IMR-32 cells (sst2 positive) or in PANC-1 cells (sst2 negative). Treatments were terminated at 48 h, at 1 min, or not at all (no wash) before incubation with 111In-pentetreotide. Untreated control cells were also assessed for binding. Within each cell type, no statistically significant differences in specific binding of 111In-pentetreotide were found between control group and any pretreated cell group.
Gene Expression
Gene expression of somatostatin and each of the 5 known types of sst was evaluated in IMR-32 cells. As shown in Figure 2A, sst2 expression was 80-fold higher in IMR-32 cells than in TT cells; sst2 expression was neither upregulated nor downregulated by OA treatment under any of the treatment regimens. Somatostatin expression is much lower in IMR-32 cells than in TT thyroid carcinoma cells, but again the relative amount of somatostatin messenger RNA was not significantly changed by OA treatment. Gene expression of sst1, sst3, sst4, and sst5 was not detectable in IMR-32 cells under control conditions or under any OA treatment dose or schedule.
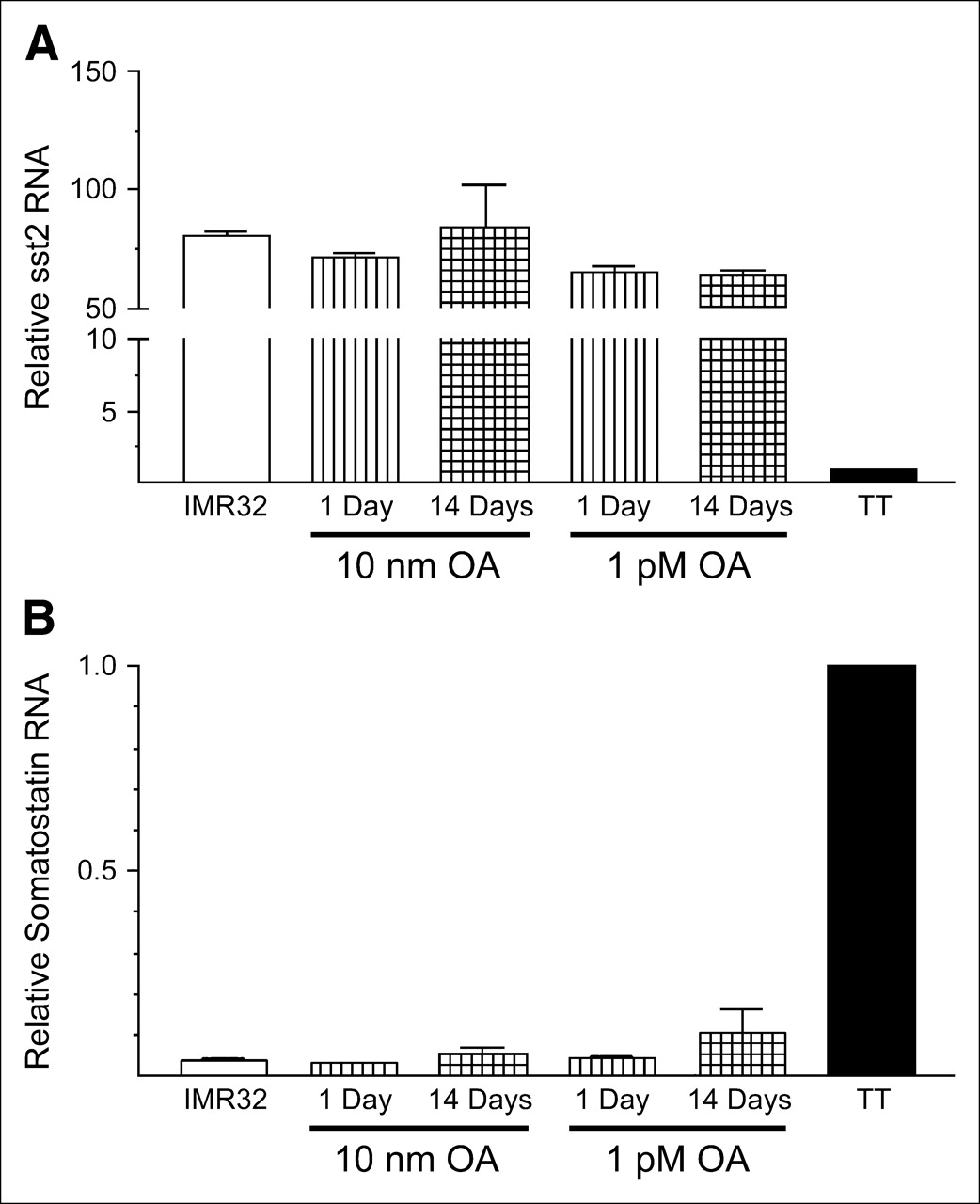
Quantitative PCR analysis of sst2 and somatostatin in IMR-32 cells treated with OA. IMR-32 neuroblastoma cells were cultured in presence of OA, 10 nmol/L or 1 pmol/L, for either 1 d or 2 wk. Untreated IMR-32 cells and TT cells were cultured as controls. Cells were then harvested, and RNA was isolated and converted to cDNA. Quantitative PCR was performed using primers and probes specific for sst2 (A) and somatostatin (B), with 18S rRNA as a control in each well. Results are shown as mean ± SD, relative to sst2 expression in IMR-32 cells and somatostatin expression in TT cells (n = 3).
DISCUSSION
Clinically, the use of somatostatin analogs is the standard of care for the management of peptide or amine-induced symptoms in patients with carcinoid and a variety of other neuroendocrine tumors (1). The use of 111In-pentetreotide for the diagnosis and localization of sst-expressing tumors is widespread. Indeed, for patients with suspected gastrinomas, 111In-pentetreotide has become the first-line diagnostic radiographic study of choice (20). Considering the widespread use of octreotide to control symptoms and the frequent use of 111In-pentetreotide for the diagnosis, localization, and subsequent follow-up of patients with neuroendocrine tumors, a better understanding of the interactions of these 2 compounds is critical. Recently, the use of high-dose (6.7–22.2 GBq) 111In-pentetreotide (11) or other radiolabeled analogs (12,13) as therapy for neuroendocrine tumors has made it critical to determine the effect of acute or chronic octreotide exposure on the receptor content and the binding of radiolabeled analogs to sst2-containing cells.
In this study, we have shown that sst2 gene expression is not upregulated in vitro by exposure of sst2-expressing cells to low- or high-dose octreotide therapy for up to 2 wk. In a similar fashion, chronic exposure of sst2-expressing cells to octreotide does not significantly alter the binding or internalization of the radiolabeled analog under any of the scenarios tested. This result may be tumor specific (IMR/neuroblastoma cell lines), and similar studies on other cell lines and biopsies of fresh human tumors must be evaluated before we can postulate that the lack of effect of octreotide on sst gene expression and binding is universal. However, this may be the first study that considers the effect of clinically relevant scenarios on the binding and gene expression of sst2 in neuroendocrine tumors.
Clinically, we have commonly recommended that patients receiving the long-acting-release form of octreotide be switched to the aqueous form of the drug (continuous infusion or multiple daily injections) for 3 mo before therapy. The data presented here suggest that those precautions may be optimal but may not be required in all patients. Binding in the presence of octreotide at a concentration of 5 nmol/L (no wash) was decreased by only 18% for the diagnostic dose and by 31% for the therapeutic dose. The current study also suggests that cessation of the aqueous octreotide for 48 h before a diagnostic scan or therapy with radiolabeled somatostatin analogs is not required.
Acknowledgments
This study was funded, in part, by grant NCI CA47877 from the National Cancer Institute.
References
- Received for publication March 21, 2005.
- Accepted for publication October 31, 2005.





{kind=link}
{kind=link}