


Abstract
PET/CT technology is in rapid evolution. It remains unclear if the unenhanced CT portion, performed for attenuation correction and lesion localization, provides additional independent diagnostic information not apparent on PET alone. The objective of the current study was to evaluate the incremental added value and frequency of potentially clinically significant incidental findings from the independent reading of the unenhanced CT portion of PET/CT studies by an expert CT radiologist. Methods: PET/CT was performed on 250 patients (123 men and 127 women; mean age, 56.5 y) referred for clinical evaluation of known or suspected cancer. Unenhanced CT studies were read without knowledge of findings from PET and PET/CT fused images. Findings from unenhanced CT were considered clinically significant if they were not detected or explained by PET findings and were considered, after examination of all available clinical data, to clearly require additional work-up. Small pulmonary nodules < 7 mm were not considered to require immediate work-up. Results: Unenhanced CT revealed potentially clinically significant incidental findings in 7 patients. Three patients had indeterminate renal lesions, 1 patient had a solid renal mass, 1 patient had sclerotic bone metastases (albeit inactive on PET), 1 patient had liver cirrhosis with portal hypertension, and 1 patient had a 5 cm abdominal aortic aneurysm. These findings were generally not detected on PET. Conclusion: Clinically significant findings from the unenhanced CT portion of PET/CT are relatively infrequent (3%) but could be serious enough to warrant major alterations in clinical management. Thus, we believe it is most appropriate for the CT portion to be interpreted by a physician skilled in CT interpretation with special attention to the lesions that PET alone can fail to detect.
Diagnosis and staging of cancer are commonly performed using anatomic imaging modalities, such as CT or MRI. PET using 18F-FDG provides information on the metabolic and functional status of cancers, thus complementing morphologic modalities. 18F-FDG PET enables diagnosis, staging, and restaging of many cancers with accuracies ranging from 80% to 90% and is often more accurate than anatomic imaging (1). However, the lack of anatomic landmarks and limited spatial resolution of PET can make precise anatomic localization challenging, thus limiting accurate evaluation of cancer patients.
In PET/CT, the use of CT for attenuation correction and image fusion offers several advantages, including shorter image acquisition (and the consequent improvement in patient comfort and scanner throughput), better lesion localization and identification, and more accurate tumor staging (2). However, although rapid attenuation correction and precise anatomic localization are clearly useful, the value of the independent CT interpretation is not clear, especially because many CT scans obtained as part of PET/CT are obtained at somewhat lower power settings than are standard CT scans and with no or limited use of contrast material. The objective of the current study was to evaluate the incremental added value and frequency of clinically significant incidental findings from the unenhanced, high-quality CT portion of PET/CT studies through independent interpretation by an expert CT radiologist.
MATERIALS AND METHODS
The study included 250 sequential patients (123 men and 127 women; mean age, 56.5 y) referred for clinical evaluation of known or suspected cancer from June 2001 to December 2001. The PET/CT scanner was a Discovery LS PET/CT system (GE Healthcare).
CT Protocol
The Discovery LS includes a multidetector helical CT scanner. Parameters were as follows for acquisitions at 5–7 bed positions: 140 kV, 80 mA, 0.8 s per CT rotation, a pitch of 6, a table speed of 22.5 mm/s, coverage of 722.5–1,011.5 mm, and an acquisition time of 31.9–37 s. The CT acquisition was performed before the emission acquisition. CT data were resized from a 512 × 512 matrix to a 128 × 128 matrix to match the PET data, fuse the images, and generate CT transmission maps. All patients placed their arms at their sides during the CT acquisition. No oral or intravenous contrast material was used.
PET Protocol
The patients fasted at least 4 h before the PET acquisition and received an intravenous injection of approximately 555 MBq (15 mCi) of 18F-FDG. The blood glucose level was measured immediately before 18F-FDG injection and was <200 mg/dL in all patients. They were instructed to sit in a quiet injection room without talking during the subsequent 45–60 min of the 18F-FDG uptake phase and were allowed to breathe normally during image acquisition, without specific instructions. Emission data were acquired at 5–7 bed positions, typically from the base of the skull through the mid-thigh (722.5- to 1,011.5-mm coverage, identical to the CT protocol). The acquisition time was 5 min at each bed position (35 scanning planes, 14.6-cm longitudinal field of view, and 1-slice overlap). Images were reconstructed with an 8 mm gaussian filter using a 128 × 128 matrix. PET images were reconstructed using CT for attenuation correction with the ordered-subset expectation maximization iterative reconstruction algorithm (2 iterations and 28 subsets). Images without attenuation correction were obtained as well.
CT Analysis
The unenhanced CT scans were read on a MagicView 1000 CT workstation (Siemens Medical Solutions) by an experienced, board-certified CT radiologist who did not know the PET or PET/CT findings. Findings from unenhanced CT were considered clinically significant by consensus if they were not detected or explained by the PET findings and were considered, after all available clinical data had been examined, to clearly require immediate additional work-up. Small pulmonary nodules < 7 mm and coronary artery calcifications were not considered to require immediate work-up.
RESULTS
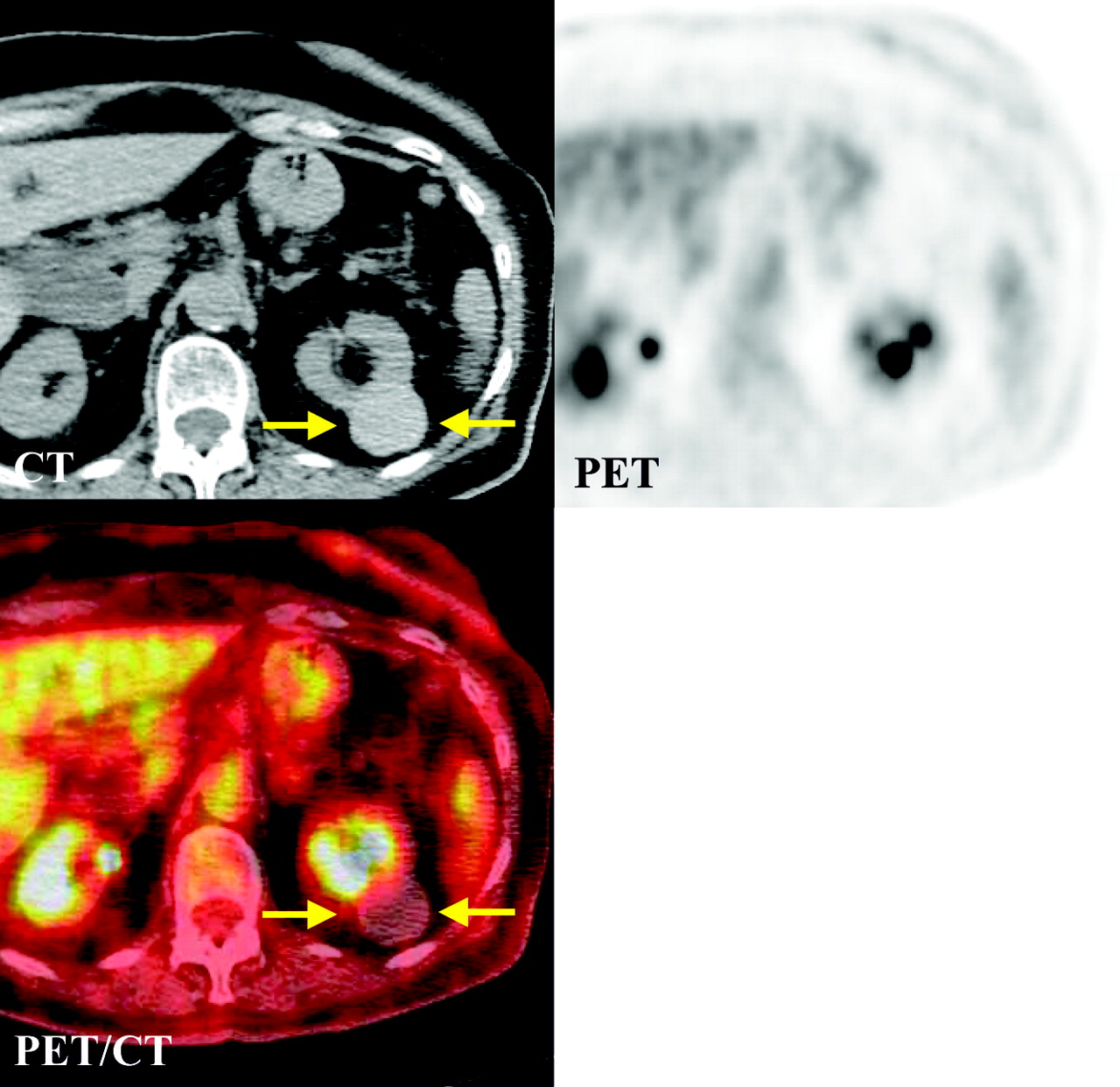
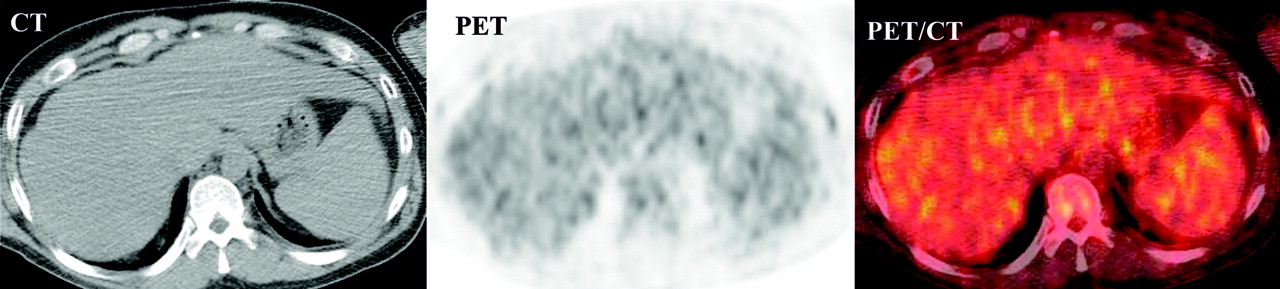
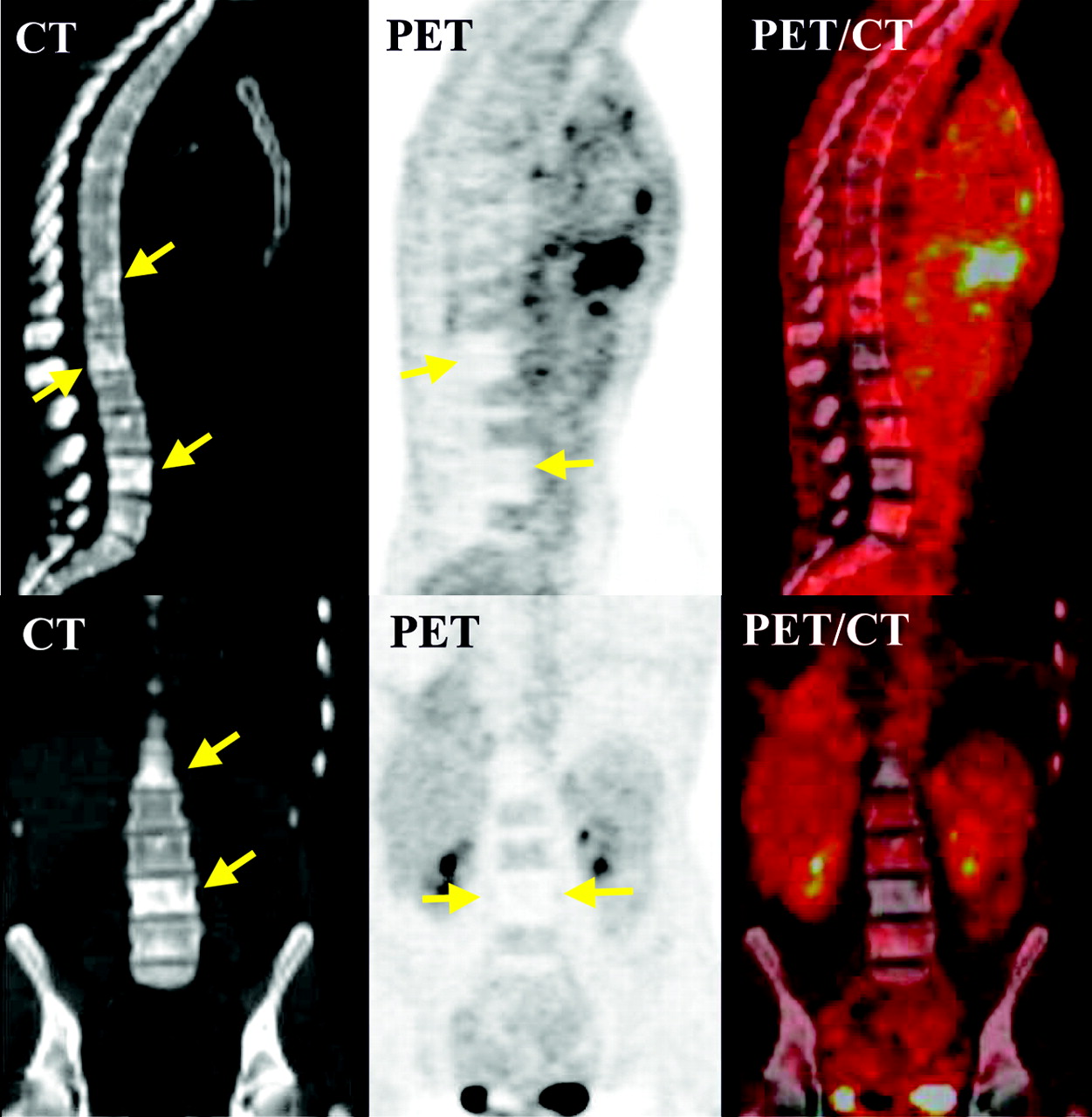
Unenhanced CT revealed potentially clinically significant incidental findings in 7 of 250 patients (3%). Table 1 summarizes the patients’ characteristics. Three patients had indeterminate renal lesions; no follow up was available for 2 of them and the third underwent contrast-enhanced CT, which revealed multiple renal cysts. Figure 1 shows an indeterminate lesion in the left kidney of a 50-y-old man with a history of testicular cancer. Figure 2 shows a solid renal mass in an 85-y-old woman with a history of cancer in the right breast. This patient underwent PET/CT because of the recent finding of bilateral pulmonary nodules. The findings of unenhanced CT raised the possibility of primary renal cell cancer with lung metastases; however, the patient died 4 wks after the PET/CT scan and no autopsy was performed. Figure 3 shows liver cirrhosis with portal hypertension in a 40-y-old man with a history of lung cancer. The diagnosis of liver cirrhosis and portal hypertension was confirmed by subsequent contrast-enhanced CT scans. The sixth patient was a 74-y-old man with lung cancer, in whom a 5 cm diameter abdominal aortic aneurysm was found (Fig. 4). The aneurysm was confirmed by a subsequent contrast-enhanced CT study, which showed the diameter to have grown to 7 cm, and was then resected. Furthermore, sclerotic bone metastases involving the lumbar spine were detected in a 32-y-old patient with lymphoma (Fig. 5). MRI confirmed the diagnosis of bone metastases. Because 18F-FDG PET indicated that this disease was likely of low activity at the time of the study, CT may have had less additional value in this patient. Nonetheless, the CT study clearly showed the reason for the markedly abnormal PET study by detecting non–18F-FDG-avid sclerotic bone lesions.

Indeterminate lesion (arrows) in left kidney of 50-y-old man with history of testicular cancer.

Solid renal mass (arrows) in left kidney of 85-y-old woman with history of cancer in right breast.

Liver cirrhosis in 41-y-old man with history of lung cancer.

Large abdominal aortic aneurysm (arrows) in 74-y-old man with lung cancer.

Sclerotic bone metastases (arrows) in 32-y-old woman with treated Hodgkin’s disease.
Patients with Clinically Significant Incidental Findings Detected by Unenhanced CT Only
DISCUSSION
PET/CT now accounts for more than 80% of current PET sales, and its market share is anticipated to grow. PET/CT fusion of anatomic and functional imaging modalities is in rapid evolution and rapid clinical dissemination. A recent prospective study assessed the clinical performance of a combined PET/CT system in 204 patients with various types of cancer (3). PET/CT provided information in addition to that from the separate interpretation of PET and CT for 99 patients (49%). Furthermore, the use of PET/CT has been advocated as a first-line imaging modality for whole-body tumor staging and restaging and for assessing response to therapy in different types of cancer (4). Currently, the CT portion of PET/CT in many centers is a lowered-dose, unenhanced study and used only for image fusion and attenuation correction. However, useful information potentially can be added through independent readings of the unenhanced-CT portion of PET/CT by a radiologist skilled in CT. This is particularly true not only for patients with cancer types known to have the potential to produce false-negative PET results but also for patients with non–18F-FDG-avid, noncancerous abnormalities. In our study, 250 PET/CT scans were reviewed, and unenhanced CT revealed clinically significant incidental findings in 7 patients (3%). Renal cysts are typically photopenic by 18F-FDG PET. However, visualization of renal cancer appears to depend on tumor grade and size because 18F-FDG PET may fail to detect smaller, lower-grade tumors (5). In our study, 3 patients had indeterminate kidney lesions and 1 patient had a large, solid left renal mass. Although, because of that patient’s death, no pathologic confirmation was done, it is possible that the patient (Fig. 2) had pulmonary metastases from renal cancer rather than from breast cancer. Liver cirrhosis detected by unenhanced CT in patient 3 of Table 1 (Fig. 3) was confirmed by subsequent contrast-enhanced CT scans and required further work-up. To the best of our knowledge, 18F-FDG PET patterns in liver cirrhosis have not previously been evaluated; hence, evaluation of liver cirrhosis by PET alone is difficult and not reliable. Figure 4 shows a relatively important abnormality that can be missed by PET. This patient had a large abdominal aortic aneurysm and initially refused surgery; however, he presented 2 mo later to the emergency department with severe back pain and underwent surgical repair for what was then a 7-cm aortic aneurysm. Also, sclerotic bone lesions seen in patient 7 of Table 1 are potentially valuable CT findings that can easily be missed on PET. This finding has previously been reported for different kinds of cancer and was attributed to relative acellularity and a lower glycolytic rate in sclerotic metastases (6). Special attention to the lung and bone windows of the unenhanced CT may enable the detection of non–18F-FDG-avid lung nodules and of sclerotic bone lesions.
Our study may underestimate the true value of the CT portion of PET/CT because we specifically did not include the study of small pulmonary nodules in our “significant” list. It is clear that some nodules smaller than 7 mm may be malignant and difficult to detect on PET alone because of the resolution limitations of current systems. Nonetheless, a substantial number of small pulmonary nodules are present in many patients because of prior granulomatous disease, and we chose not to include such lesions in this analysis because many may not be of clinical significance. We also likely underestimated the incremental value of the CT portion by virtue of its having been performed without intravenous or oral contrast material, during tidal breathing, and at a relatively low amperage. Nonetheless, the unenhanced CT scans in our studies produced infrequent but important findings.
CONCLUSION
Clinically significant findings from the unenhanced CT portion of PET/CT are relatively infrequent (3%) but could be serious enough to warrant major alterations in clinical management. Thus, we believe it is most appropriate for the CT portion to be interpreted in its own right, by a physician skilled in CT interpretation, with special attention to lesions that PET alone may fail to detect.
Footnotes
Received Jan. 3, 2005; revision accepted Apr. 8, 2005.
For correspondence or reprints contact: Richard L. Wahl, MD, Johns Hopkins Medical Institutions, 601 N. Caroline St., Room 3223A, Baltimore, MD 21287-0817.
E-mail: rwahl{at}jhmi.edu
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Incidental Diagnosis of Thrombus Within an Aneurysm on 18F-FDG PET/CT: Frequency in 926 Patients
- Agreement of Visual Estimation of Coronary Artery Calcium From Low-Dose CT Attenuation Correction Scans in Hybrid PET/CT and SPECT/CT With Standard Agatston Score
- Business Aspects of Cardiovascular Computed Tomography: Tackling the Challenges
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- Improvements in Cancer Staging with PET/CT: Literature-Based Evidence as of September 2006
- Clinical Significance of Small Pulmonary Nodules with Little or No 18F-FDG Uptake on PET/CT Images of Patients with Nonthoracic Malignancies
- Clinically Significant Abnormal Findings on the "Nondiagnostic" CT Portion of Low-Amperage-CT Attenuation-Corrected Myocardial Perfusion SPECT/CT Studies
- CT in PET/CT: Essential Features of Interpretation