


Abstract
Attenuation correction is recommended to optimize the performance of cardiac SPECT. The 2.5-mA CT commonly used for this purpose in myocardial perfusion SPECT is generally considered “nondiagnostic” in quality. In other areas of cardiac and hybrid imaging, diagnostically relevant abnormal findings on higher-quality CT studies have been described. The purpose of this study was to establish the frequency and significance of abnormal findings on low-amperage-CT cardiac SPECT/CT scans and to assess whether a systematic review of the nondiagnostic CT findings should be recommended. Methods: Two hundred consecutive patients who underwent clinical low-amperage-CT attenuation-corrected myocardial perfusion studies acquired on a SPECT/CT system were included in the study. The cardiac CT images were reviewed in consensus by both an experienced CT reader and a nuclear medicine resident less experienced in CT. Abnormal CT findings of varying significance were recorded. Results: Eighty-one patients had no abnormal CT findings. In the remaining 119 patients, 234 abnormalities were detected. Twenty-five major findings (in 21 patients) were seen, and 16 of these had been previously unrecognized. Sixty-four minor and 131 minimal findings were noted. Fourteen findings were labeled as equivocal (i.e., the CT findings were not definite). Conclusion: Potentially significant abnormal findings on the nondiagnostic-CT portion of the cardiac SPECT/CT examination were detected in 10.5% of our patients. These data suggest that, in addition to the review of the emission image dataset, low-amperage-CT findings should routinely be assessed for major diagnostic abnormalities.
Myocardial perfusion SPECT is a well-established clinical tool that provides diagnostic and prognostic information about coronary artery disease. Attenuation correction is now recommended to improve the diagnostic accuracy of myocardial perfusion SPECT (1). Attenuation maps are usually obtained with a transmission scan from a radioactive line or point source or with CT. The method using CT has the potential advantage of producing a higher-quality attenuation map because it has higher photon-flux, better resolution, and lower noise than do radionuclide transmission sources (2). At present, the low-amperage-CT component of myocardial perfusion SPECT/CT is used almost exclusively for attenuation correction, and only recently have recommendations to review the attenuation maps for quality control purposes been published (1).
Diagnostically relevant abnormal findings on the higher-energy, diagnostic-quality CT portion of the study have been described in other areas of cardiac imaging, especially coronary artery calcium scoring (3–5), and in other areas of fusion imaging such as PET/CT (6). Osman et al. (6) showed important diagnostic findings on the CT portion for 3% of patients referred for oncologic PET/CT examinations using a multislice (80 mA) CT scanner with a 0.8-s rotation. Most cardiac SPECT/CT systems provide only a low-power (2.5 mA) CT scan and have a slow gantry rotation requiring a relatively long time for scan acquisition. The value of independent CT interpretation is not clear, because the diagnostic value of the CT used by the hybrid SPECT/CT systems is obviously limited by the much lower power settings and lower speed than are used with standard CT and by lack of the contrast material used with standard CT. These factors degrade the CT image quality.
We sought to establish the frequency and significance of abnormal anatomic findings on CT attenuation-corrected cardiac SPECT/CT scans to assess whether a systematic routine diagnostic review of the CT portion should be recommended.
MATERIALS AND METHODS
Patients
We retrospectively evaluated the images from 200 patients (103 female and 97 male; mean age, 55 ± 14 y; range; 17–87 y) who consecutively underwent CT-attenuation-corrected myocardial perfusion studies during 2 periods of approximately 1 mo each (6/10/04 to 7/13/04 and 4/1/05 to 4/26/05). The studies were acquired on a Millennium VG Hawkeye SPECT/CT system (GE Healthcare), and all patients had been referred for the clinical evaluation of coronary artery disease. SPECT at rest and stress was performed according to standard clinical protocols for myocardial perfusion imaging. In our practice (based on 112 of the included patients), most patients (87%) have both arms above the head for SPECT/CT, 9% have the right arm at the side and left arm above the head, and 4% have both arms at the side. The retrospective image review was approved by the institutional review committee, and the need for informed consent was waived.
CT Scanning
The single-slice nonspiral CT scanner (x-ray tube current, 2.5 mA; voltage, 140 kVp) has a slice thickness (and axial resolution) of 10 mm with a scan time of more than 5 min for a typical 13-cm field of view. The field of view was chosen to fully include the heart (from the ascending aorta to the apex) based on the CT scout image. CT attenuation correction was performed twice for each patient: once for the resting images and once for the stress images. Both were obtained immediately after the acquisition of the SPECT images. The patients received no special breathing instructions (tidal breathing). Table 1 summarizes the characteristics of the CT scans used for attenuation correction.
Characteristics of CT Used for Attenuation Correction in Our Study and of Typical Diagnostic Thoracic Spiral CT at Our Institution
Analysis
The CT scans were retrospectively and independently reviewed at a workstation (Xeleris; GE Healthcare) by an expert in body CT (R1) and by a nuclear medicine resident who had not yet received formal training in CT (R2). Each scan was reviewed at 3 different window settings, including a lung window, a soft-tissue window, and a bone window. The SPECT/CT system provided preset values for each of these windows, and the reader manually optimized the window in each case.
Abnormal findings on CT were recorded and rated as to their significance. The clinical significance was judged to be major when it was thought to require further testing or follow-up or would be important in a patient with symptoms and signs of cardiovascular disease, especially someone suspected to have coronary artery disease. Other findings were classified as minor (less significant than major findings but deemed of some clinical significance and such as would have been mentioned on standard CT) or minimal (less significant than minor findings; possibly of minimal or no clinical significance or of no added value to a standard clinical history). In addition, some findings could be classified only as equivocal (i.e., the CT findings were not definite). After the review of the CT portion of the SPECT/CT study, the patient's electronic medical record was reviewed to decide whether the minor and major findings had been known or unknown at the time of SPECT/CT.
For a subset of 50 patients, both the rest and stress CT studies were reviewed routinely to establish how many findings were seen during only one of the test conditions. For the remaining 150 patients, only the rest CT study was reviewed routinely; stress CT was reviewed when deemed necessary (to distinguish between findings and possible artifacts, all “equivocal” findings). Of note, all types of findings were recorded as 1 finding: For example, the presence of multiple osteophytes in the spine or of multiple calcified mediastinal lymph nodes was recorded as 1 finding. The 2 reviewers then read the scans together, and in virtually all instances, the less experienced reviewer concurred with the more experienced reviewer. Thus, the following results represent the consensus CT interpretation.
RESULTS
All CT scans had some degree of breathing artifacts, likely because of the relatively long scanning time. These were not noted as abnormalities.
Number of Findings
Eighty-one patients had no abnormal CT findings. In the remaining 119 patients, 234 abnormalities were detected. There was an average of 2 findings per patient. Most patients had only 1 finding (58 patients) or 2 findings (36 patients). Ten patients had 3 findings, 7 had 4 findings, 6 had 5 findings, 1 had 6 findings, and 1 had 10 findings.
Significance of Findings
The potential clinical significance of findings was classified as major, minor, minimal, or equivocal (Tables 2 and 3). There were 25 potentially major findings (e.g., pulmonary mass or infiltrates, dilated aorta, or coronary calcification) (Table 4; Figs. 1–5). In addition, there were 64 minor findings (e.g., vascular calcifications or liver lesions) and 131 minimal findings (e.g., osteophytes, calcified lymph nodes, or a pacemaker). Fourteen findings were classified as equivocal because the CT findings were not definite and no corroborative information could be extracted from the patient's record. Because 3 patients had more than 1 major finding, a total of 21 patients had 25 major findings. Most of the equivocal findings (n = 9) were seen in the first 50 patients.

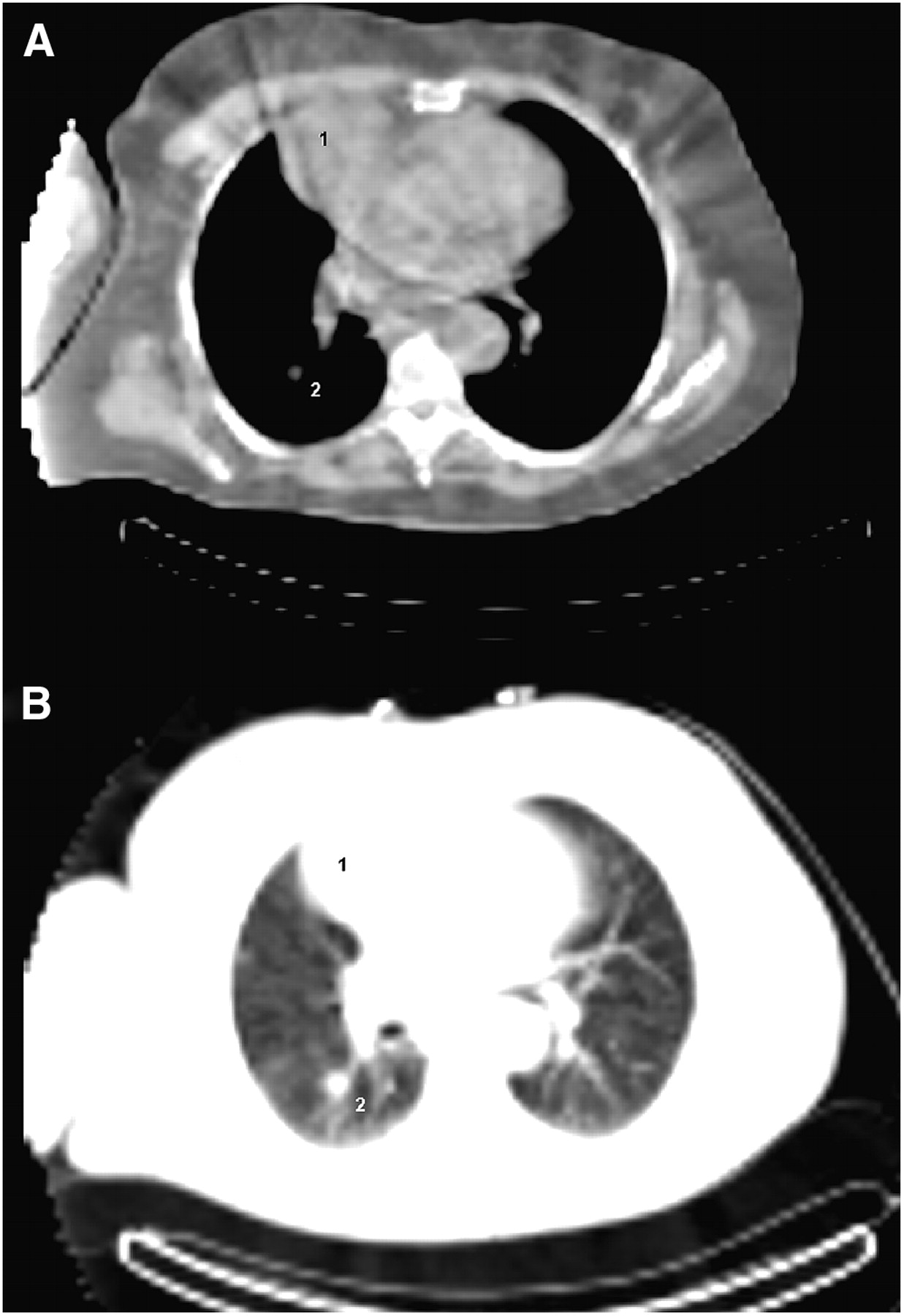
Transaxial CT slice of 73-y-old woman with fatigue and exertional dyspnea. Images were obtained with soft-tissue window (A) and with lung window (B). Myocardial perfusion SPECT findings were normal. Large anterior mediastinal mass (1) and lung nodule (2) are seen on CT portion of images. Mediastinal mass is likely pericardial cyst. Both findings were unknown, and there were no follow-up studies for over 1.5 y. Patient was then diagnosed with adenocarcinoma of right lung and underwent resection. Mediastinal cyst was confirmed at surgery.

Transaxial CT slice of 83-y-old man with coronary artery disease and atypical chest pain. Calcification of left anterior descending artery is seen. In patient with established diagnosis of coronary artery disease, finding is of doubtful clinical significance.

Selected transaxial CT slices of 81-y-old man with dilated ischemic cardiomyopathy and substernal chest pain, fatigue, and anorexia. Images were obtained with soft-tissue window (A) and with lung window craniad to soft-tissue window (B). Chest radiography 4 d before SPECT/CT showed small left-sided pericardial effusion. SPECT/CT shows large pericardial effusion (1), at least moderate-sized left-sided pleural effusion (2), and significant compressive atelectasis and consolidation (3). These findings were later confirmed by chest radiography and transthoracic echocardiography. Metal artifact from automatic implantable cardioverter-defibrillator is noted as well.

Four separate CT slices 1 cm apart of 54-y-old man with dyspnea and exertional substernal chest pain. Chest radiography 9 d before SPECT/CT showed large consolidation in right lower lobe appearing compatible with pneumonia. This finding is also seen on SPECT/CT. Follow-up chest radiography approximately 6 wk later showed resolution after antibiotic treatment.

Transaxial CT slice of 58-y-old woman with atypical chest pain. Images were obtained with soft-tissue window (A) and lung window (B) and demonstrate mass in right lower lobe of lung. Five days before SPECT/CT, patient underwent diagnostic CT with intravenous contrast material to rule out pulmonary embolism. CT showed mass or masslike infiltrate in right lower lung. Follow-up was recommended but was not performed so far.
Summary of Major and Minor Abnormal Findings
Summary of Minimal and Equivocal Abnormal Findings
Characteristics of Patients with Major Findings
One Versus Two CT Studies
A total of 77 findings were seen in the 50 patients for whom both stress and rest CT findings were systematically reviewed. One finding (major: pulmonary nodule) was apparent on stress imaging but was not seen on rest imaging because of the less cranial field of view of the latter.
Known Versus Unknown Findings
Sixty percent (15/25) of the major findings and 48% (30/62) of the minor findings were unknown at the time of SPECT/CT. However, of the 8 patients with coronary calcifications, all had been referred for myocardial perfusion imaging and 6 (75%) were known to have coronary artery disease or calcifications. Incidentally identified coronary calcifications are probably less significant in these patients than in those referred for other reasons (Fig. 2).
DISCUSSION
Myocardial perfusion scintigraphy is a well-established and commonly used technique for the evaluation of coronary artery disease. Its use continues to grow, given the continued increase in cardiovascular disease. In the United States, the current recommendation is to use attenuation correction (1) to process the images. An increasingly popular approach to attenuation correction is a low-amperage (in our case, 2.5 mA) slow-speed CT scan of the heart, or mid to lower thorax. This CT scan, covering about 13 cm in about 5 min, is often blurred by respiratory motion and, given the relatively low photon flux, is generally considered nondiagnostic. To our knowledge, the diagnostic relevance of the findings on this nondiagnostic low-amperage CT scan obtained for attenuation correction has not been systematically studied.
We observed a total of 234 findings in 200 patients, of which 25 findings were classified as having potentially major clinical significance. Significant abnormal findings on the CT portion of the cardiac SPECT/CT study were detected in 10.5% (21/200 patients) of our population. Potentially significant unknown findings (n = 15) were seen in 6% of the patients (n = 12). In general, the stress and rest scans had nearly identical findings. Because we had a subjective impression of slightly less motion degradation on the CT scan obtained at rest, examining the rest study alone should be adequate. The field of view is guided by the scout CT images, which are rich in anatomic information and allow the technologist to choose similar fields of view between the rest and stress images. Because stress images are obtained at 30–60 min after exercise, a similar lung volume was expected for both stress and rest images. In the 50 patients in whom both stress CT and rest CT were systematically reviewed, there was 1 additional finding that was apparent only on the stress study. Therefore, review of both sets of images probably will provide a modest improvement over review of 1 set of images in a few patients if the field of view is consistent between rest and stress imaging.
The higher percentage of significant findings, compared with that found by Osman at al (6), who evaluated 250 patients with PET/CT, could be explained by their exclusion of coronary calcifications and lung nodules smaller than 7 mm. We believe that these findings were significant in our population (especially in the patients without known coronary artery disease) because the population was referred for cardiovascular (and not oncologic) evaluation. Further, the size of a lung nodule imaged at a 1-cm CT slice thickness could easily be underestimated. In 3 other studies evaluating electron-beam CT for noncardiac or noncoronary abnormalities (3–5), the detection rates for abnormalities ranged from 20% to 53% for all findings and were 4.2%, 7.8%, and 9.3% for significant or important findings. This range seems to be due to differences in the way lesions and significant lesions were defined; in the precise methods of CT acquisition, including the use of intravenous contrast material for CT angiography; and, likely, in the patient populations.
The mean age of our patient population (which consisted of patients referred from the emergency room for evaluation of a variety of types of chest pain and outpatients with known or suspected coronary artery disease) might have been less than that of centers having a larger fraction of patients with known coronary artery disease, and the rate and characteristics of incidental findings may vary depending on the practice.
The importance of examining the CT scan used for attenuation correction will certainly increase as higher-quality CT scanners, with attendant improvements in CT image quality, are integrated into SPECT/CT systems.
CONCLUSION
Potentially significant abnormal findings on the nondiagnostic low-amperage-CT portion of the cardiac SPECT/CT study were detected in 10.5% (21/200 patients) of our population. We recommend that the CT used for attenuation correction be assessed for major abnormalities of the lung, vascular structures, and soft tissues. As higher-quality CT components are added to SPECT/CT systems, such a review will likely become even more important.
Acknowledgments
Preliminary results of this study were presented at the 2005 annual meeting of the Society of Nuclear Medicine.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 19, 2006.
- Accepted for publication April 21, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Holistic AI analysis of hybrid cardiac perfusion images for mortality prediction
- Ancillary Finding on Myocardial Perfusion Imaging Due to Urinary Bladder Displacement
- The Clinical Dilemma of Incidental Findings on the Low-Resolution CT Images from SPECT/CT MPI Studies
- Lesion Detection Performance: Comparative Analysis of Low-Dose CT Data of the Chest on Two Hybrid Imaging Systems