


Abstract
PET/CT with 18F-FDG is increasingly being used for staging, restaging, and treatment monitoring for cancer patients. CT is still frequently used only for attenuation correction and lesion localization. However, increasing sales of high-end scanners that combine PET with 64-detector CT strongly suggest that the field is moving toward a comprehensive concept, whereby diagnostic CT studies during intravenous contrast material application are combined with the highest-quality PET studies. At many institutions, in-line PET/CT has replaced separately acquired PET and CT examinations for many oncologic indications. This replacement has occurred despite the fact that only a relatively small number of well-designed prospective studies have verified imaging findings against the gold standard of histopathologic tissue evaluation. However, a large number of studies have used acceptable reference standards, such as pathology, imaging, and other clinical follow-up findings, for validating PET/CT findings. From these data, we believe, has emerged reliable evidence in support of the notion that PET/CT offers diagnostic advantages over its individual components for the major cancers.
Early clinical studies reported dramatic improvements in the diagnostic accuracy of in-line PET/CT over PET alone, as demonstrated for lung cancer patients (1). This finding was surprising because PET alone had been reported to stage and restage cancer with accuracies in excess of 90% (2). Recent reports of more modest gains in the diagnostic accuracy of PET/CT for lung cancer, colorectal cancer, breast cancer, lymphoma, and others were therefore not unexpected (Table 1).
Clinical Performance of PET/CT: Direct Comparison with PET or CT
We conducted extensive searches of medical databases using various combinations of key words to identify relevant contributions to the literature on the clinical value of PET/CT for head and neck cancers, thyroid cancer, lung nodules and lung cancer, breast cancer, cancers of the gastrointestinal tract and urogenital system, lymphoma, melanoma, and unknown primary cancers. A selection of these publications is listed in Table 1. Because most of the reviewed studies are discussed in more detail in the individual contributions to this supplement, we limited this review to reporting comparative PET/CT and PET or CT accuracy data. We recognize that the inclusion of publications in this review remains somewhat arbitrary and possibly incomplete because relevant publications may have escaped our search.
HEAD AND NECK AND THYROID CANCERS
Head and Neck Cancers
The diagnosis of recurrent or residual head and neck cancers after surgical resection, chemotherapy, or radiation treatment by conventional anatomic imaging remains challenging, even with 18F-FDG PET. False-positive 18F-FDG PET findings can arise from brown fat tissue (3) as well as from asymmetric skeletal muscle or mucosal or glandular activity. In addition, regions with normal or physiologically increased 18F-FDG uptake may mask pathologic 18F-FDG uptake and cause false-negative results. Differentiation of posttherapeutic alterations attributable to scarring, inflammation, and necrosis from residual or recurrent tumors also poses significant problems for CT and MRI.
It is therefore not surprising that head and neck cancers were among the first oncologic entities to be studied with PET/CT. Rather than studying the diagnostic accuracy of PET/CT for staging of head and neck cancers, Syed et al. (4) confirmed, in a prospective study of 24 patients, a significant improvement in lesion localization, together with greater interobserver agreement for PET/CT than for PET alone (κ-coefficient, 0.45 vs. 0.90).
A retrospective study of 47 patients by a group at the University of Pittsburgh suggested an excellent sensitivity of PET/CT of 95% but a limited specificity of only 60% for detecting head and neck cancers (5). Imaging findings were verified by biopsy or surgery in 25 of 33 patients for whom PET/CT findings suggested tumor recurrence. The reasons for the low specificity of 60% included physiologic laryngeal and tongue 18F-FDG uptake. One false-negative PET/CT finding was attributable to a missed laryngeal lesion.
In another retrospective study (6), the majority of the 65 consecutive patients underwent restaging for suspected recurrent disease. Lesions were scored visually by PET, CT, and PET/CT on a 5-point scale. Tumor biopsy, performed for all patients, correlative imaging findings, and clinical follow-up at 6 mo served as reference standards. As determined by lesion-based receiver operating characteristic analysis, the accuracy of PET/CT was 92%; PET/CT was significantly more accurate than PET or CT alone. Several regions of physiologically increased uptake were correctly identified as such only with the help of CT. On the other hand, PET correctly identified malignant lesions that were not seen on CT images in 12 patients. In 8 of these patients, the lesions were not evident even in retrospect on CT images.
Schoeder et al. (7) studied 68 patients, 52 of whom had squamous cell carcinoma. About 50% of the patients were evaluated for recurrent disease. Lesions were graded visually as benign, equivocal, or malignant. Biopsy findings as well as endoscopic and other imaging findings served as reference standards. However, only about 30% of the lesions were verified by biopsy. A lesion-based analysis revealed that the accuracy of PET/CT was significantly higher than that of PET alone (96% vs. 90%; P = 0.03). False-positive findings included cases of tonsillitis, chronic and ulcerative inflammatory changes after radiation therapy, and resolving increased 18F-FDG uptake in a lymph node that was likely associated with inflammation. PET/CT proved to be especially helpful in the reevaluation of patients after surgery. In the majority of patients, PET/CT was found to be critical for exact lesion localization and reduced the number of equivocal findings by 50%.
Gordin et al. (8) conducted a prospective, nonmasked image analysis of 51 PET/CT studies acquired in 42 retrospectively enrolled patients with laryngeal cancer. Imaging findings were visually graded as benign, equivocal, or malignant and were verified by biopsy in 26 of 42 patients. In a patient-based analysis, PET/CT was superior to CT and PET with regard to specificity (96%, 8%, and 73%, respectively) but superior only to CT with regard to accuracy (59% for CT, 86% for PET, and 94% for PET/CT). Sensitivity did not differ among the 3 modalities (89% for PET/CT, 92% for CT, and 92% for PET; P = not significant [NS]). In a lesion-based analysis, PET/CT was significantly more accurate than CT or PET alone. Finally, PET/CT altered treatment management in more than 50% of the study population.
The ability of PET/CT to detect nodal metastases was examined in 31 patients with oral cancer staged as N0 by CT or MRI (9). In this setting, the prevalence of nodal metastases is about 20%. Thus, as expected, only a few metastatic nodes were found in this study. PET/CT would be helpful in this situation if it could reliably identify those 80% of patients without lymph node involvement and in whom elective neck dissection could be avoided. The main limitation of PET/CT in this setting was the relatively large number of false-positive findings, largely attributable to benign lymphadenitis. As another problem, micrometastases were missed in 3 patients. However, there is currently no imaging modality that can identify such small metastatic deposits.
Chen et al. compared the TNM staging accuracy of PET/CT with that of PET and CT in 70 patients with nasopharyngeal cancer (10). PET/CT, CT, and PET had comparable accuracies for T and M staging in 20 patients with newly diagnosed cancer. However, the accuracy of PET/CT (95%) for restaging in 50 patients was significantly higher than that of PET (83%) or CT (73%) alone.
Thyroid Cancer
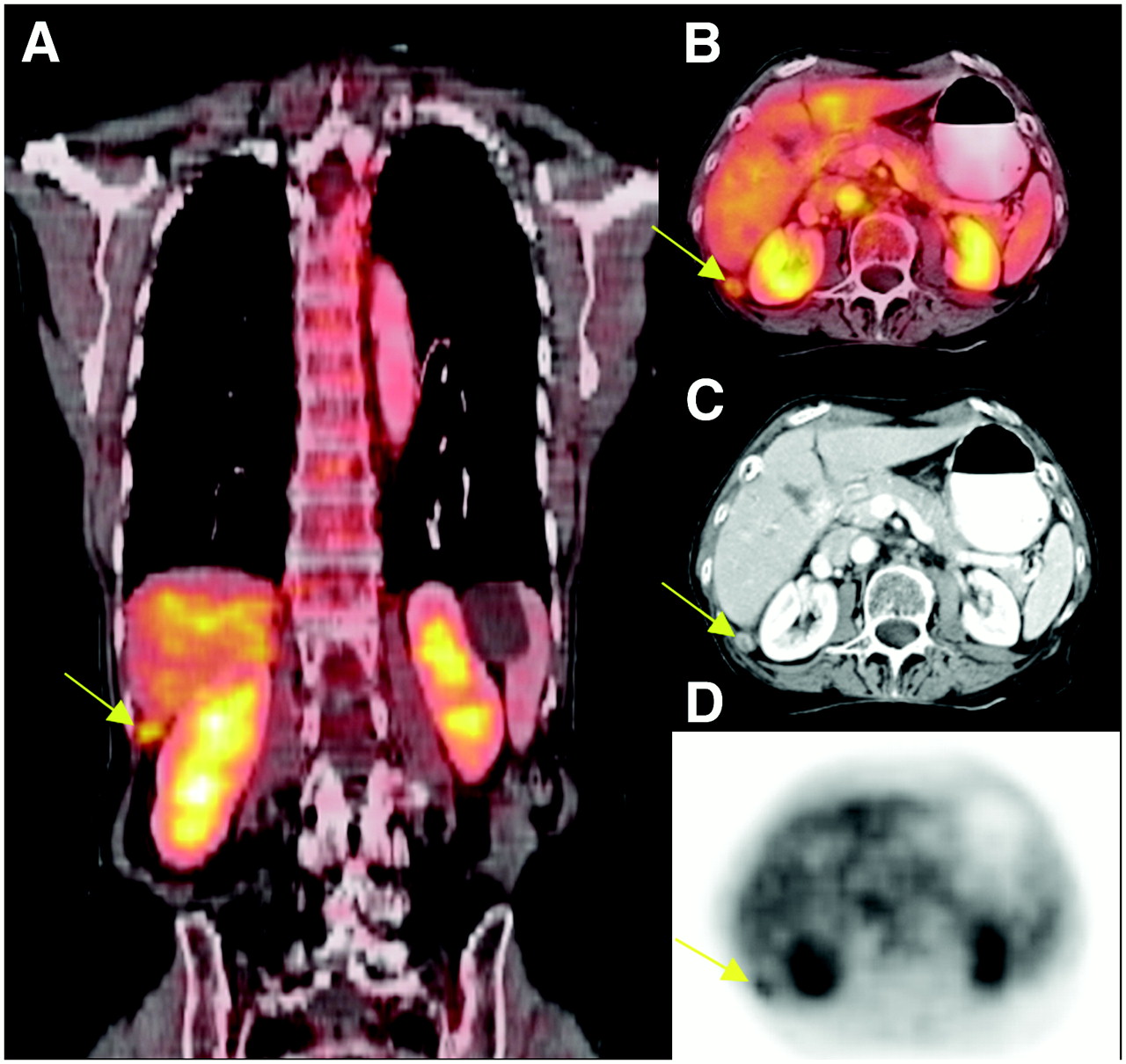
The role of PET/CT in detecting recurrent papillary thyroid cancer was investigated retrospectively in 33 patients by a group at Johns Hopkins University (11). PET/CT findings were categorized as altering the treatment plan, supporting the treatment plan, or having no impact on the treatment plan. The treatment plan was altered or supported in 67% of the patients by PET/CT. Most of these patients had markedly elevated serum thyroglobulin levels and negative 123I scan results. Compared with histopathology as the gold standard, PET had an accuracy of 70%. For 10 pathology-proven lesions, the PET/CT results were false-negative, a finding that was likely explained by their small size. However, the reasons for false-negative scans were not listed. No false-positive results occurred. However, the negative predictive value for malignancy was only 27%, clearly too low to obviate biopsy. An example of a PET/CT study and a 123I whole-body scan in a patient with thyroid cancer is shown in Figure 1.
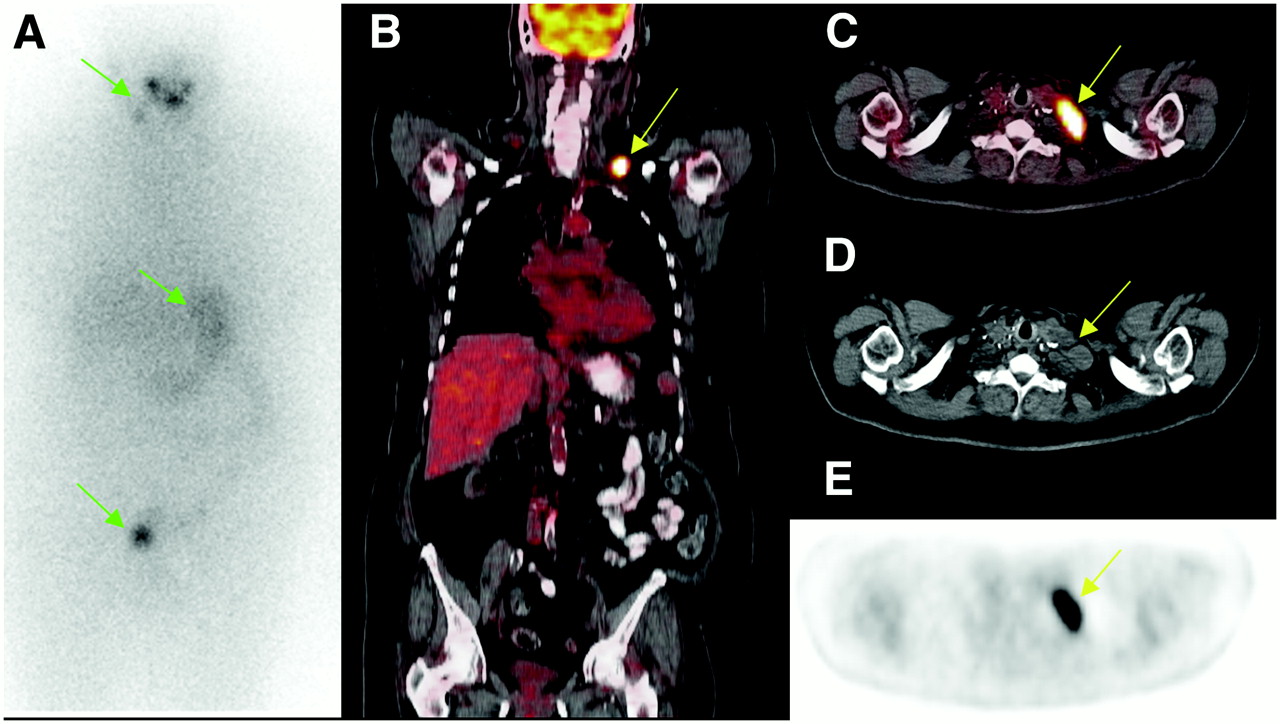
Whole-body 123I (A) and PET/CT (B–E) images obtained in patient who had history of papillary thyroid cancer and who had been treated with surgery and radioiodine therapy. Patient presented with markedly elevated serum thyroglobulin levels. (A) Normal 123I whole-body scan. Green arrows denote physiologic activity in right submandibular region, stomach, and bladder. (B–E) Coronal whole-body PET/CT, axial PET/CT, axial CT, and axial PET images, respectively. PET/CT revealed intensely increased 18F-FDG uptake in left supraclavicular region, corresponding to lymphadenopathy on CT (yellow arrows). Subsequent surgical resection revealed metastasis from papillary carcinoma.
The diagnostic performances of PET/CT and PET were compared directly by Palmedo et al. (12) in a study of 40 patients with suspected differentiated but iodine-negative thyroid cancer. PET/CT was more accurate for the detection of disease than CT alone (93% vs. 78%; P < 0.05). In addition, PET/CT changed the management in 48% of the patients with cancer.
In summary, PET/CT is emerging as an important imaging modality for staging of head and neck and thyroid cancers. Its advantages for head and neck cancers appear to be derived from improved specificity and better lesion localization. It is important to note that no studies comparing the accuracy of PET/CT with that of MRI for head and neck cancers have been published. For thyroid cancer, the improved localization of iodine-negative, 18F-FDG–positive lesions is clinically relevant because it can result in curative removal of metastases.
SOLITARY LUNG NODULES AND LUNG CANCER
Diagnosis and Staging
18F-FDG PET of solitary lung nodules and masses accurately discriminates between malignant and benign lesions (13). A more recent investigation sought to further characterize lung nodules with CT by measuring the degree of contrast enhancement (14). Initial findings suggested that different degrees of contrast enhancement may aid in discriminating between malignant and benign lung lesions, so that the combination of measurements of 18F-FDG uptake and the degree of contrast enhancement may improve lesion characterization.
The diagnostic accuracy of PET/CT for characterizing lung nodules was compared with that of contrast-enhanced CT in 119 patients (15). The study population was enrolled retrospectively. Histologic verification was available for all patients. For contrast-enhanced CT, peak enhancement, net enhancement, and washout were determined. Malignant nodules ranged in size from 9 to 30 mm. As a limitation of the study, only 8 nodules were smaller than 10 mm. Ninety-three of 119 nodules were concordantly characterized by contrast enhancement and washout during CT and by PET/CT. However, in this study population with 40 benign and 79 malignant lesions, PET/CT was significantly more sensitive (96% vs. 81%; P < 0.05) and accurate (93% vs. 85%; P = 0.011) than CT alone. The authors concluded from their findings that PET/CT should be the test of choice for characterizing lung nodules.
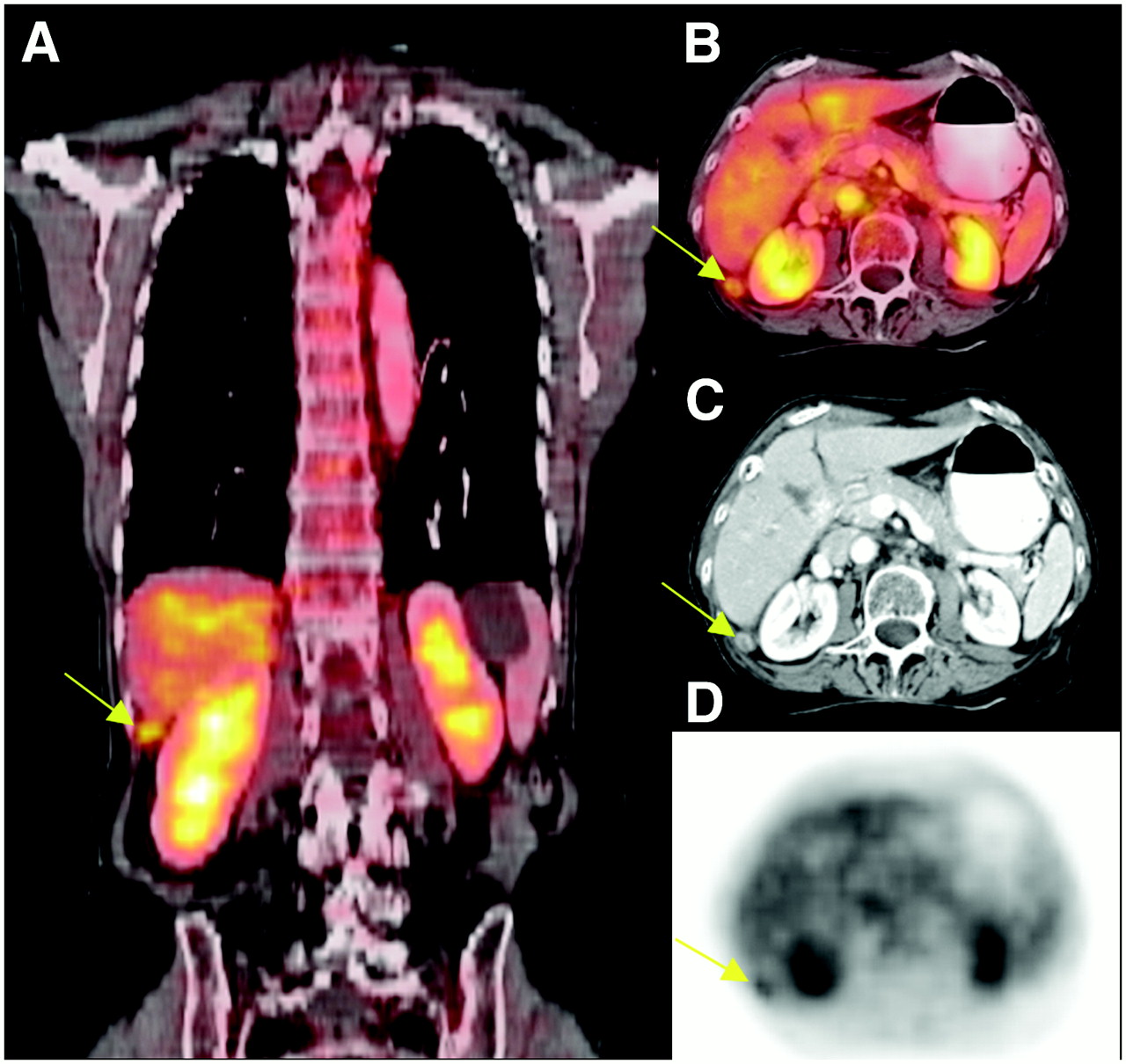
Radiologists interpreting PET/CT studies are faced with the conceptual problem that traditional size criteria for classifying “lesions” as malignant or benign are notoriously unreliable (16). In addition, the accuracy of PET is lower than 100%, and its specificity can be as low as 75% (17). A meta-analysis published in 1999 revealed that imaging of 18F-FDG accumulation with 18F-FDG PET stages the mediastinum with an accuracy that is 15 percentage points higher than that of CT (Fig. 2) (17).

Images obtained in patient with lung cancer after left upper lobectomy and chemotherapy. Study was performed for restaging. (A–D) Coronal whole-body PET/CT, axial PET/CT, axial CT, and axial PET images, respectively. Local recurrence in region of previous resection was evident. Unexpected metastases to left lobe of liver (yellow arrows) and to right iliac bone (red arrow) were identified, underscoring importance of whole-body staging of patients with lung cancer.
An early study (1) compared the diagnostic performance of in-line PET/CT with that of PET, CT, and the side-by-side visual interpretation of PET and CT in 50 patients with proven or suspected non–small cell lung cancer. PET/CT revealed important additional findings in 41% of the patients, was superior to PET with regard to T and N staging, and tended to be more accurate for M staging. The diagnostic advantage of PET/CT over PET alone for T staging was expected, because tumor size is measured accurately by CT. However, PET/CT was also superior to CT alone for T staging, a finding that awaits further confirmation and explanation. It is important to note that the accuracy of PET alone for N staging was only 49%, a value markedly lower than the 92% previously reported in a meta-analysis (17). The accuracy of PET for N staging increased to 85% when equivocal findings were considered positive for disease involvement. However, it is unclear from the presented data how lymph nodes were classified by PET. Surprisingly, PET/CT was not significantly more accurate than CT alone for N staging (P = 0.12). This finding contradicts the findings of numerous previous studies that showed PET to be more accurate than CT for N staging.
Subsequent studies confirmed that the T stage (i.e., tumor size and invasion) is assessed more accurately with PET/CT than with PET (18,19), supporting the notion that lesion size cannot be measured accurately with PET alone. No advantage of PET/CT over PET alone was found for N staging in studies by Antoch et al. (18) and Halpern et al. (19). Shim et al. (20) reported no significant advantage for T staging but reported a significantly higher accuracy for N staging of PET/CT than of CT alone (84% vs. 69%; P < 0.001) in 106 patients who underwent curative surgical resection.
Another retrospective study was conducted in 50 patients with suspected lung lesions (21). The diagnostic performance of integrated PET/CT was compared with that of side-by-side analysis with PET and CT as well as PET or CT alone. Surgical staging was used as the reference standard. As expected, PET/CT was superior to PET and CT for T staging. However, there was only a tendency toward more accurate mediastinal N staging with PET/CT. The TNM stage was most accurately determined with integrated PET/CT (70%); CT and PET staged only 46% and 30%, respectively, of the patients accurately. The reasons for the uniquely low accuracy of CT and PET for TNM staging were not discussed further in this article.
Discrepancies between studies, with some showing improved N staging but others not doing so, might be explained by differences in interpretation criteria and study protocols. Some protocols included intravenous contrast material administration, whereas others used a low-dose, non–contrast-enhanced CT approach. Taken together, however, the reports suggest a marginal diagnostic benefit of PET/CT for N staging and a significant benefit for T staging.
The ability of 18F-FDG PET/CT to detect recurrent lung cancer was investigated by Keidar et al. (22) in a study of 42 patients who were enrolled retrospectively but whose images were interpreted prospectively. In this study, the addition of CT significantly improved the specificity (82% vs. 53%) for cancer detection, but sensitivities did not differ. Unfortunately, the reasons for the very low PET specificity were not explained. For example, in 1 patient, PET/CT excluded the presence of mediastinal lymph node metastases that were suspected by PET alone. It is unclear which CT finding prompted a revision of the PET interpretation. Were these lymph nodes classified as normal by CT size criteria? If so, why were normal-size lymph nodes with increased 18F-FDG uptake classified as benign by PET/CT? In this report, PET/CT affected clinical management in 29% of the patients.
The incidence and nature of solitary extrapulmonary lesions in 350 patients with known non–small cell lung cancer were determined by Lardinois et al. (23). Such lesions were identified in 72 patients (21%) and were, for the most part, found to be malignant on biopsy. Importantly, about 50% of these lesions did not arise from the known primary lung cancer. The findings implied that solitary extrapulmonary lesions in lung cancer patients need to be evaluated carefully.
Restaging and Treatment Monitoring
Patients with stage IIIA lung cancer and in whom neoadjuvant treatment results in “down-staging” may be candidates for potentially curative surgery. PET alone has limited accuracy for restaging disease in the mediastinum after chemotherapy (24). Furthermore, mediastinoscopy may be more accurate than PET/CT for detecting or ruling our residual tumor viability in lymph nodes. De Leyn et al. investigated this issue prospectively in 30 patients with stage IIIA N2 lung cancer (25). They used surgical findings as the gold standard for comparing the accuracy of 18F-FDG PET/CT for N staging with that of mediastinoscopy after neoadjuvant therapy. In this setting, PET/CT was more accurate than mediastinoscopy (83% vs. 60%; P < 0.05) and significantly more accurate than PET or CT alone. The authors suggested that the low sensitivity of mediastinoscopy resulted from posttreatment alterations, such as adhesions and fibrosis, that rendered especially the subcarina space inaccessible.
Pottgen et al. (26) retrospectively studied in 50 patients with potentially operable, locally advanced non–small cell lung cancer the ability of 18F-FDG PET/CT to assess responses to chemoradiation therapy. Follow-up PET/CT scans were obtained after a minimum of 3 chemotherapy cycles. Patients with standardized uptake value (SUV) reductions of greater than 50% had significantly longer progression-free survival than patients with SUV reductions of less than 50%. However, it is not clear from this study how and whether CT information could also be used to improve outcome predictions.
In a prospective trial, Cerfolio et al. compared the accuracies of PET/CT and CT alone for restaging of stage IIIA lung cancer in 93 patients after neoadjuvant chemotherapy (27). The authors reported a significantly higher restaging accuracy of PET/CT than of CT alone for restaging of disease in lymph nodes. However, a considerable number of false-positive and false-negative results strongly suggested that node biopsies were required to avoid the consequences of false-positive PET/CT findings. Figure 2 depicts the findings obtained in a lung cancer patient who underwent restaging after surgery and chemotherapy.
In summary, currently available data for lung cancer confirm that PET/CT is superior to PET alone for T staging. This advantage is largely attributable to the ability of CT to determine tumor extension into adjacent tissue and to measure tumor size accurately. The advantage of PET/CT for N staging appears to be marginal. Given these results, how should readers interpret mediastinal PET/CT findings? Because of the overwhelming evidence that PET stages disease in the mediastinum with a higher accuracy than CT, we suggest using metabolic information as the primary guidance for mediastinal staging. For example, we consider enlargement of lymph nodes without increased 18F-FDG uptake unlikely to represent metastatic disease.
Finally, preliminary data suggest that PET/CT can play an important role in evaluating patients after neoadjuvant chemotherapy and in monitoring treatment effects in lung cancer patients. However, multicenter trials are needed to define treatment response criteria for PET/CT.
BREAST CANCER
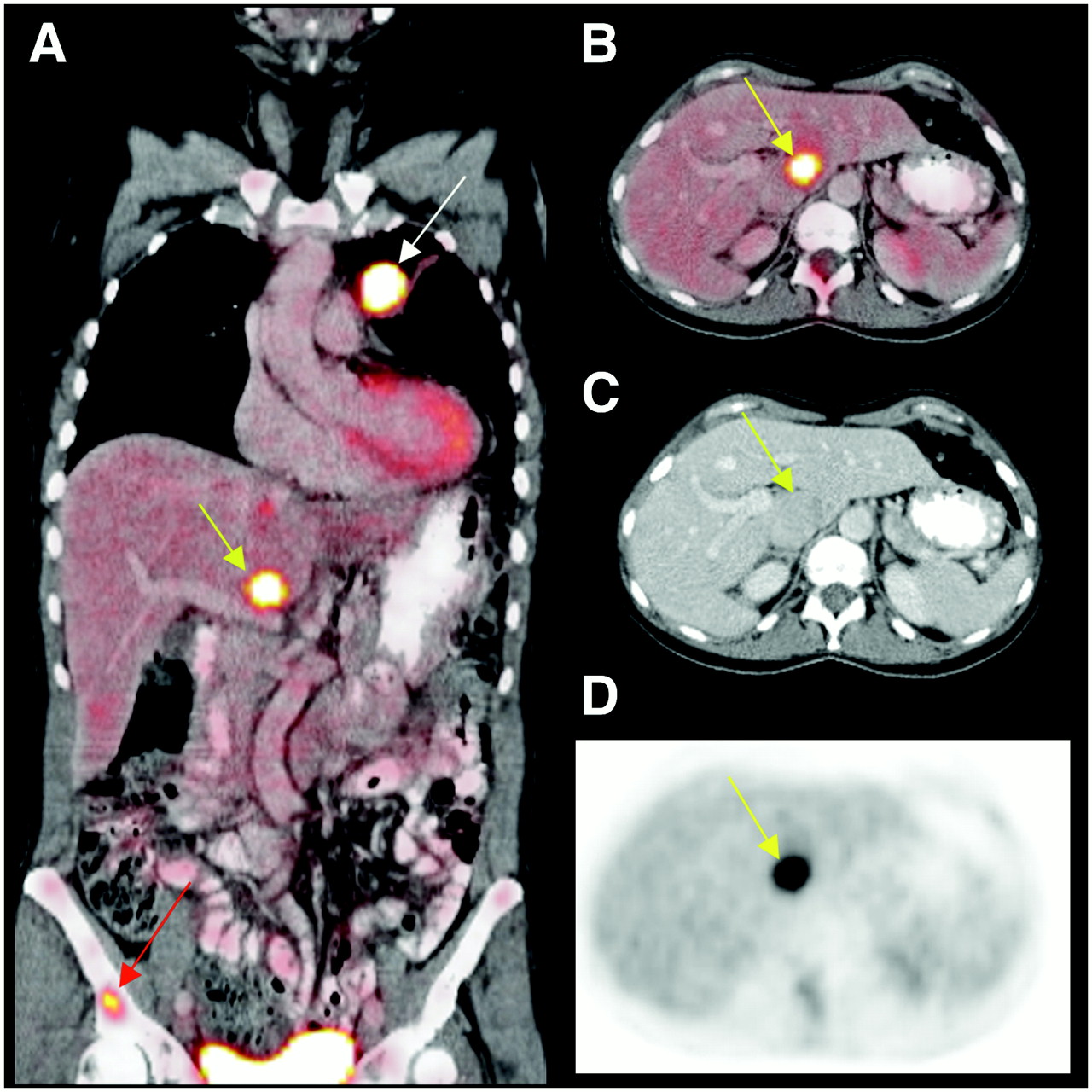
Two studies evaluated the ability of in-line PET/CT to stage or restage breast cancer and reached similar conclusions. Fueger et al. (28) demonstrated that PET/CT tended to be more accurate for restaging in 58 patients than PET alone (90% vs. 79%; P = 0.06), although this improvement was not statistically significant. The majority of patients had infiltrating ductal carcinoma. PET-positive lesions were scored visually. Lesions with mildly hypermetabolic activity, benign inflammatory lesions, physiologic variants, and PET-negative sclerotic bone lesions accounted for false-positive and false-negative PET findings. In the second qualitative PET/CT investigation, Tatsumi et al. (29) reported an improvement with PET/CT over CT alone for 75 breast cancer patients. Further, the staging accuracy was higher with PET/CT than with CT alone (86% vs. 77%; P < 0.05). PET/CT improved reader confidence with regard to both the nature and the location of lesions (Fig. 3).

Coronal PET/CT (A) and axial PET/CT (B), CT (C), and PET (D) images acquired in patient with breast cancer. White arrow on coronal image depicts primary tumor, which was infiltrating ductal carcinoma. Yellow arrows denote metastatic lesion in sternum.
To date, no large prospective studies of PET/CT for detecting breast cancer have been published. However, on the basis of preliminary data, PET/CT appears to add an approximate 10% improvement in diagnostic accuracy to that achieved with PET alone in patients who undergo restaging of breast cancer. Specific issues, such as the diagnostic and prognostic significance of 18F-FDG–negative sclerotic bone lesions, remain unresolved at present and need further investigation. It also remains undetermined at present whether, when, and which patients with breast cancer should be monitored by PET/CT and how this modality could be used best for treatment monitoring.
CANCERS OF GASTROINTESTINAL TRACT
18F-FDG PET stages and restages cancers of the gastrointestinal tract with a high diagnostic accuracy. However, limitations remain. These include the low glycolytic activity of mucin-producing and hepatocellular cancers and the highly variable and sometimes focal physiologic 18F-FDG activity in the bowel. On the other hand, CT images of the abdomen after surgery are difficult to interpret.
Esophageal Cancer
One study of 32 patients with esophageal cancer (30) reported that staging with PET/CT was significantly more specific (81% vs. 59%; P < 0.01) and accurate (90% vs. 83%; P < 0.01) than staging with PET alone. Significant improvements in N staging with PET/CT were reported by Yuan et al. (31) in a study of 45 patients. The imaging findings were corroborated by pathologic assessment. The accuracy of PET/CT was 92%, and that of PET alone was 86% (P < 0.05).
Jadvar et al. (32) studied 60 patients who had esophageal cancer and who underwent initial staging or restaging of the disease. Rather than addressing the diagnostic accuracy of PET/CT, the authors evaluated the studies for concordant and discordant abnormalities revealed by individual imaging modalities. Discordant findings occurred in about 25% of the patients. Such findings included, among others, hypermetabolic but normal-size lymph nodes in 3 patients, hypermetabolic liver lesions without a clear CT correlate, and hypermetabolic foci in the distal esophagus without significant wall thickening. Although a firm gold standard was not available for many patients in this retrospective study, PET/CT provided useful information that resulted in biopsy and subsequent management changes in some patients.
Colorectal Cancer
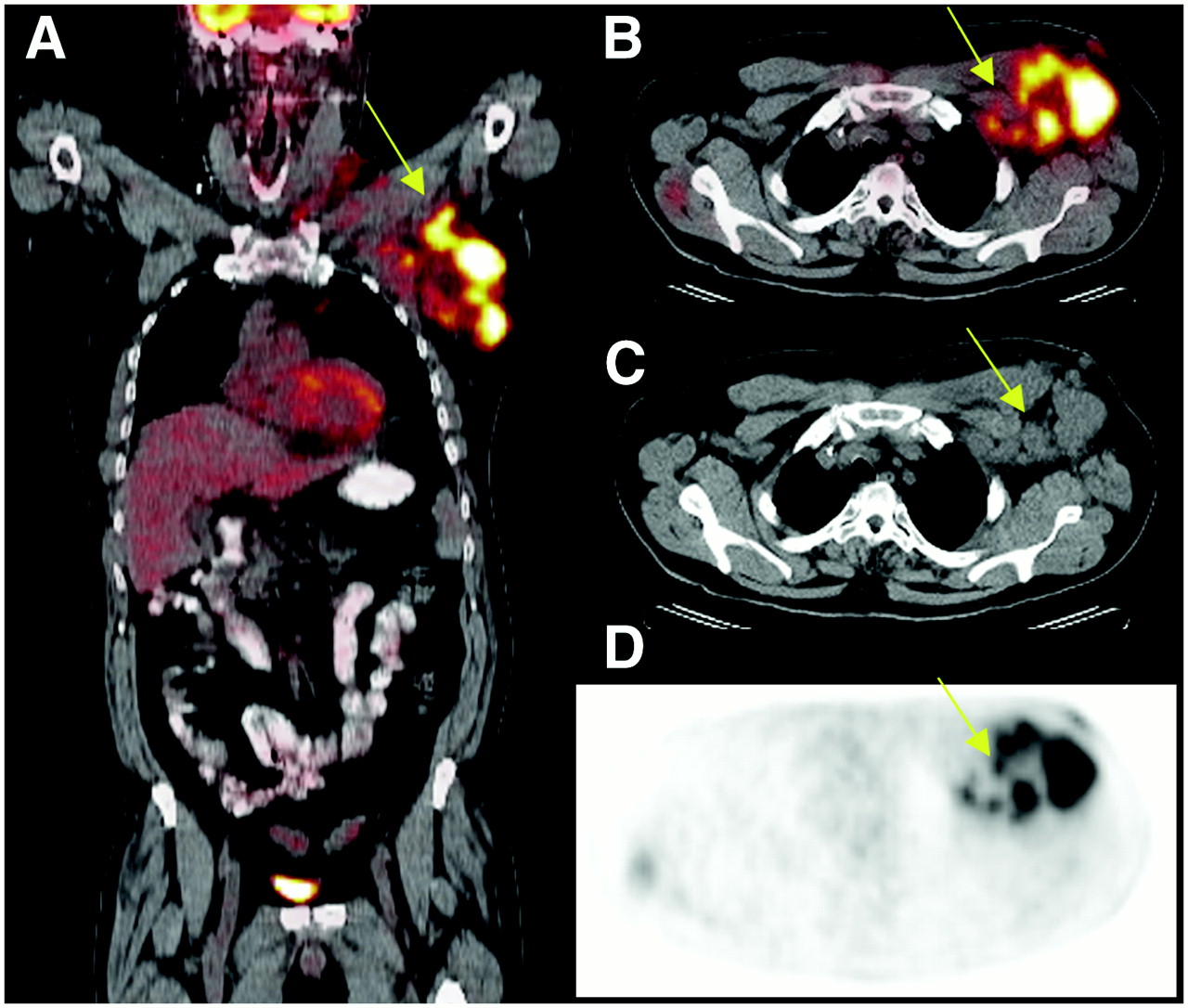
Several investigators studied the performance of PET/CT in patients with colorectal cancer (a case example is shown in Fig. 4) (33–36). All found PET/CT to be superior to PET or CT alone for staging or restaging of cancer. Cohade et al. (33) studied 45 patients and reported a significant gain in accuracy of 11%, from 78% to 89%. The same group of investigators determined the incremental contribution of CT to PET/CT (34) by adding a “dedicated” CT interpretation (by a radiologist) to the PET/CT interpretation. That addition resulted in a significant increase in accuracy that was attributable mainly to improved specificity. This study underscored the importance of careful evaluation of the diagnostic CT portion of a PET/CT study.

Coronal PET/CT (A) and axial PET/CT (B), CT (C), and PET (D) images acquired in patient with colorectal cancer. Increased 18F-FDG uptake in left axilla (yellow arrows), corresponding to lymphadenopathy on CT, was subsequently proven to represent metastatic disease.
Similarly, PET/CT detected recurrent colorectal cancer with a higher accuracy than PET alone in 62 patients who underwent restaging after surgery (37). The most common cause of false-positive PET/CT findings was physiologic uptake in displaced pelvic organs.
Kim et al. (35) addressed several issues in a retrospective analysis of 51 patients with colorectal cancer. They confirmed a higher restaging accuracy of PET/CT than of PET alone (88% vs. 71%; P < 0.01). They also evaluated the performance of software-based fusion of independently acquired PET and CT studies in the same patients. Software fusion failed in 24% of the patients. We have observed a similar rate of failure of software fusion in patients with lymphoma, lung cancer, and breast cancer. Further, in patients for whom fusion was “successful,” the degree of misregistration was significantly greater than that obtained with in-line PET/CT.
Votrubova et al. demonstrated that PET/CT was superior to PET alone for the detection of both intra- and extra-abdominal lesions (36). The impact of PET/CT on treatment was also studied in 76 patients with liver metastases (38). Contrast-enhanced CT and PET/CT detected liver metastases with similar sensitivities, 95% and 91%, respectively (P = NS). However, PET/CT was significantly more specific (P = 0.04) for detecting recurrent liver metastases after partial hepatectomy. PET/CT was also superior for detecting extrahepatic disease that was missed by contrast-enhanced CT in more than 30% of the patients; in comparison, PET/CT missed such disease in only 11% of the patients (P = 0.02). PET/CT altered clinical management in 21% of the patients.
Despite early promising reports (39), 18F-FDG PET has been used infrequently for differentiating benign and malignant pancreatic masses because both frequently exhibit increased 18F-FDG uptake. A study by Heinrich et al. suggested that PET/CT will also not resolve this clinically important issue (40). They attempted to characterize pancreatic lesions that were detected in most patients by contrast-enhanced CT. Pathology served as the gold standard in most patients. In their study, the negative predictive value of PET for cancer was only 64%. False-negative PET studies were explained by small lesion size in 2 patients and elevated serum glucose levels in the remaining 3 patients. Four false-positive PET findings were attributable to inflammatory pseudotumor, tuberculosis-associated pancreatitis, chronic pancreatitis, and high-grade dysplasia. CT performance was not evaluated because PET/CT was performed without intravenous contrast material application. However, even the addition of intravenous contrast material would not have converted false-positive to true-negative PET/CT findings. Separately acquired contrast-enhanced CT scans had a low specificity, only 27%. A different but equally important clinical problem was also addressed in this study (40); PET/CT helped to more appropriately manage treatment by, for instance, excluding 5 patients with metastatic disease from surgery.
Gallbladder Cancer and Cholangiocarcinoma
PET/CT was compared with contrast-enhanced CT for its ability to detect biliary tract tumors (41). Although CT and PET/CT had comparable detection rates for primary tumors, in-line PET/CT was significantly more accurate for detecting distant metastases.
Gastrointestinal stromal tumors (GIST) serve as a model for the paradigm shift in assessing tumor responses to treatment. Oral treatment with imatinib, a kinase inhibitor with predominantly cytostatic effects, results in lasting tumor remissions that can be documented and predicted with 18F-FDG PET as early as 24 h after the start of treatment. In contrast, CT responses were noted only several weeks later (42).
Because of the high predictive accuracy of PET alone, PET/CT would not be expected to yield dramatic improvements in accuracy. To address this issue, Goerres et al. (43) compared the prognostic value of PET with that of contrast-enhanced CT and PET/CT in patients with GIST. 18F-FDG PET, but not contrast-enhanced CT, provided significant prognostic information. PET/CT was useful because CT detected additional liver lesions that might have changed the surgical approach in the patients with GIST. However, if surgery is not contemplated, then 18F-FDG PET alone should suffice for evaluating treatment responses and establishing prognosis in patients with GIST. In contrast, Antoch et al. (44) suggested that all patients with GIST should be examined with PET/CT because some false-positive PET findings are corrected by CT, resulting in a higher predictive accuracy of PET/CT than of PET alone for patient outcome. Thus, 18F-FDG PET/CT appears to be marginally more accurate than PET alone for predicting treatment responses in patients with GIST.
In summary, PET/CT stages colorectal cancer with a higher accuracy than PET alone. Very preliminary data also suggest that it is more accurate than PET alone for staging of esophageal cancer. Finally, initial reports suggest that it has a cost-effective impact on the management of treatment for patients with liver metastases as well as those with primary pancreatic cancer.
LYMPHOMA
The diagnostic and prognostic accuracy of 18F-FDG PET for detecting lymphoma is exquisitely high and unequivocally superior to that of CT, so that PET/CT would not be expected to improve accuracy further. This notion was confirmed by several investigations with nearly 300 patients (45–48).
In a patient-based analysis of 27 patients (46), 18F-FDG PET/CT proved to be significantly more accurate than CT (93% vs. 78%; P < 0.05) but not superior to PET alone (93% vs. 86%; P = NS) or to PET and CT interpreted side by side (93% vs. 93%). Allen-Auerbach et al. (45) studied 73 patients and reported that PET/CT had a higher staging accuracy than PET alone (93% vs. 84%; P = 0.03). False-positive PET findings were ascribed to, among others, asymmetric brown fat. This study also reported a concordantly false-positive PET/CT scan in a patient with a biopsy-proven granulomalike response after chemotherapy. In a retrospective study, Tatsumi et al. compared PET/CT with CT in a group of 53 patients (48). PET provided accurate staging in 9 patients (17%) for whom CT staging was incorrect. On the other hand, CT provided correct “up-staging” in 2 patients. Another study emphasized that careful side-by-side evaluation of PET and CT images could yield the same diagnostic accuracy as in-line PET/CT (99% vs. 99%) (49). In this study of 100 patients, both in-line PET/CT and side-by-side PET and CT performed about 10% better than CT alone.
Schaefer et al. evaluated the significance of increased 18F-FGD uptake in bone lesions in 50 patients with Hodgkin's disease or Hodgkin's lymphoma (50). Patients were selected on the basis of the presence of abnormal 18F-FDG uptake on PET images. Imaging findings were verified by bone biopsy or bone marrow aspiration. A total of 193 bone lesions were found by PET. Lymphoma was found in all 18 patients (36%) who underwent direct biopsy. Bone marrow aspiration was performed in 11 of these 18 patients but was negative in 7 of these patients. PET/CT was more accurate for identifying bone involvement than CT or biopsy. The authors suggested that PET/CT should be used to guide biopsy. As a limitation of this study, patients were selected on the basis of positive PET findings; hence, the sensitivity of PET/CT for the detection of bone involvement in the general population of lymphoma patients is unknown.
Therefore, the currently available data suggest that PET/CT stages or restages lymphoma with an accuracy similar to or slightly higher than that of PET alone and, as expected, significantly higher than that of CT alone. It is still unclear whether intravenous contrast material is needed for PET/CT studies in lymphoma patients. This issue was investigated by Schaefer et al. (47), who reported that non–contrast-enhanced PET/CT was superior to contrast-enhanced CT alone for staging of lymphoma. However, this study did not directly compare contrast-enhanced with non–contrast-enhanced PET/CT. Until more evidence becomes available, we have adopted a “diagnostic” PET/CT approach for all lymphoma patients in whom there is no medical contraindication against intravenous contrast material administration.
CANCERS OF UROGENITAL SYSTEM
The diagnostic performance of PET/CT in small cohorts of patients with cervical cancer (51) and ovarian cancer (52,53) has been investigated. A prospective study of cervical cancer (51) included 47 women with early-stage disease. As determined in patients before surgery and with histopathology as the gold standard, the overall sensitivity, specificity, and accuracy of PET/CT for lymph nodes larger than 5 mm were 72%, 100%, and 99%, respectively. The patient-based sensitivity, specificity, and accuracy of PET/CT were 73%, 97%, and 89%, respectively. No comparisons between PET/CT and PET or CT were provided. Future studies will need to establish whether and how PET/CT could add to the information derived from PET and CT and how it could alter treatment management.
A small study of ovarian cancer (52) included 19 patients with suspected disease; PET/CT tended to detect sites of recurrence with a higher accuracy than PET or CT alone. In another study, 31 patients with ovarian cancer were studied before second-look surgery (53). As determined with histopathology as the gold standard, the sensitivity, specificity, and accuracy of PET/CT were 78%, 75%, and 77%, respectively. No comparisons between PET/CT and PET or CT were provided. Given the low accuracy of PET alone for detecting ovarian cancer, these data suggest considerable diagnostic improvements through the use of PET/CT.
Another small study of 14 patients suggested a reasonable diagnostic accuracy of 18F-FDG PET/CT for detecting penile cancer (54).
MELANOMA
PET has limited usefulness for regional N staging in melanoma patients. However, whole-body staging can be important, especially for patients in whom solitary metastatic lesions might be resected with curative intent (Fig. 5). Reinhardt et al. included 250 patients, the majority of whom had stage II or III disease, in a retrospective study (55). Readers were unaware of the results of the imaging studies but not of the clinical history. Seventy-five patients underwent initial staging, and the others underwent therapy control (n = 42), restaging (n = 65), or follow-up (n = 68). Histopathology and clinical follow-up served as reference standards for PET/CT findings. For the entire population, PET/CT was superior to CT but not to PET with regard to N staging. Differences in initial N staging among the 3 modalities were marginal. Restaging for metastatic disease was best assessed with PET/CT, which classified 245 of 250 patients correctly, whereas disease for only 209 of 250 patients was correctly assessed with CT. However, CT performed as well as the other imaging modalities for initial M staging. Overall, PET/CT performed best in patients who underwent treatment evaluation or restaging. The overall N and M staging accuracies were 97.2% for PET/CT, 92.8% for PET, and 78.8% for CT (all differences were significant). The authors concluded that PET/CT with 18F-FDG should be the diagnostic modality of choice for melanoma patients with suspected recurrence and those undergoing therapy control.
Coronal PET/CT (A) and axial PET/CT (B), CT (C), and PET (D) images acquired in patient with melanoma. Small focus of moderately increased 18F-FDG uptake corresponded to small soft-tissue nodule on CT (yellow arrows). Biopsy confirmed melanoma, and subsequent surgery for solitary metastasis was performed.
UNKNOWN PRIMARY CANCER
By definition, unknown primary tumors are those that remain undetected after all diagnostic resources have been used. PET alone reportedly detects 20%–40% of such unknown tumors. Tumors that remain undetected are most frequently small and therefore difficult to detect. It is not surprising, therefore, that PET/CT depicted the primary tumor in only 15 (33%) of 45 patients (56). In this study, there were no significant differences in the diagnostic accuracies of PET/CT and PET or CT alone for detecting the primary tumor. As a limitation, the definition of unknown primary tumor might not have applied to all patients. For instance, it is unclear why the primary tumor was not found in a patient with axillary lymphadenopathy (breast cancer) or in another patient with a brain metastasis (lung cancer). In another study of 21 consecutive patients with biopsy-proven metastatic disease and negative findings from conventional diagnostic procedures, 18F-FDG PET/CT detected the occult primary tumor in 12 patients (57% of cases); this rate of detection is higher than that previously reported (57). Unfortunately, it is unclear from the provided data whether PET/CT was superior to PET or CT alone.
SARCOMA
Iagaru et al. (58) evaluated the roles of PET and PET/CT in 106 patients with bone and various histologic types of soft-tissue sarcomas. Pulmonary metastases were detected in 40 patients (38%). PET identified pulmonary metastases with a lower sensitivity than CT (69% vs. 95%; P < 0.05). Eleven lung lesions, all less than 1 cm in diameter, were visualized by CT but not by PET. This study has important implications for appropriately interpreting PET/CT studies not only in sarcoma patients but in other patients as well. To avoid the consequences of false-negative PET studies, suspected lesions—of any size and without increased 18F-FDG uptake—revealed by CT must be observed and monitored with great attention.
INCIDENTAL FINDINGS
As a technique that comprehensively searches the whole body for metabolic and structural alterations, PET/CT can detect and elucidate incidental anatomic abnormalities. In one study (59), non–contrast-enhanced CT performed in conjunction with PET revealed significant findings in 3% of the patients.
Another study reported an incidence of unexpected hypermetabolic abnormalities in the gastrointestinal tract of 1.3% (n = 58) in 4,390 patients with a variety of malignancies (60). Most of the lesions identified were malignant or premalignant, suggesting that careful follow-up and evaluation of such hypermetabolic foci are indicated. Gutman et al. (61) investigated, in 1,716 patients, whether PET/CT was useful for detecting premalignant polyps of the colon. Focally increased 18F-FDG uptake was observed in 45 patients and was verified by colonoscopy or biopsy in 20 patients. In 15 patients, abnormalities were found. These included 13 villous adenomas, 3 carcinomas, and 2 hyperplastic polyps. The 18F-FDG PET findings were false-positive in 5 patients, suggesting that an incidental finding of focally increased 18F-FDG uptake should be monitored by colonoscopy.
CONCLUSION
After its discovery in the mid-1970s (62), PET became an important diagnostic modality in oncology in the early 1990s and mid-1990s. The advent of PET/CT in the late 1990s (63) further increased the visibility and acceptance of PET.
Although the value of PET/CT over PET alone for treatment monitoring has yet to be determined, improvements in the staging and restaging accuracies of PET/CT over PET or CT alone for different cancers are now established. These improvements are frequently statistically significant and average about 10%–15%. Together with convenience for patients and clinicians, these improvements have resulted in the emergence of PET/CT as the most important cancer imaging modality.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- Received for publication October 10, 2006.
- Accepted for publication November 8, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Novel Method to Detect and Characterize 18F-FDG Infiltration at the Injection Site: A Single-Institution Experience
- Radiation Dosimetry of Whole-Body Dual-Tracer 18F-FDG and 11C-Acetate PET/CT for Hepatocellular Carcinoma
- 18F-FDG PET/CT and PET/MRI Perform Equally Well in Cancer: Evidence from Studies on More Than 2,300 Patients
- Fetal and Maternal Absorbed Dose Estimates for Positron-Emitting Molecular Imaging Probes
- PET/MR Imaging: A Critical Appraisal
- Introduction
- Not-So-Random Errors: Randomized Controlled Trials Are Not the Only Evidence of the Value of PET
- Advances in Immuno-Positron Emission Tomography: Antibodies for Molecular Imaging in Oncology
- Doing More Harm than Good? Do Systematic Reviews of PET by Health Technology Assessment Agencies Provide an Appraisal of the Evidence That Is Closer to the Truth than the Primary Data Supporting Its Use?
- Incidental Diagnosis of Thrombus Within an Aneurysm on 18F-FDG PET/CT: Frequency in 926 Patients
- Assessment of a New 18F-FDG PET/CT Protocol in the Staging of Oral Cavity Carcinomas
- Variations in Clinical PET/CT Operations: Results of an International Survey of Active PET/CT Users
- Whole-Body 18F-FDG PET/CT: The Need for a Standardized Field of View--A Referring-Physician Aid
- 18F-FDG Avidity in Lymphoma Readdressed: A Study of 766 Patients
- Targeted In vivo Imaging of Integrin {alpha}v{beta}6 with an Improved Radiotracer and Its Relevance in a Pancreatic Tumor Model
- PET/MRI: The Blended-Modality Choice of the Future?
- Reply: SPECT/CT
- Role of 18F-FDG PET in Assessment of Response in Non-Small Cell Lung Cancer
- Measuring Response with FDG-PET: Methodological Aspects
- Breast Cancer Staging in a Single Session: Whole-Body PET/CT Mammography
- SPECT/CT
- Dual-Modality Imaging: Combining Anatomy and Function
- Modern Radiotherapy as Part of Combined Modality Treatment in Locally Advanced Non-Small Cell Lung Cancer: Present Status and Future Prospects
- PET/CT in Evaluating Pediatric Malignancies: A Clinician's Perspective
- Introduction