


Article Figures & Data
Figures
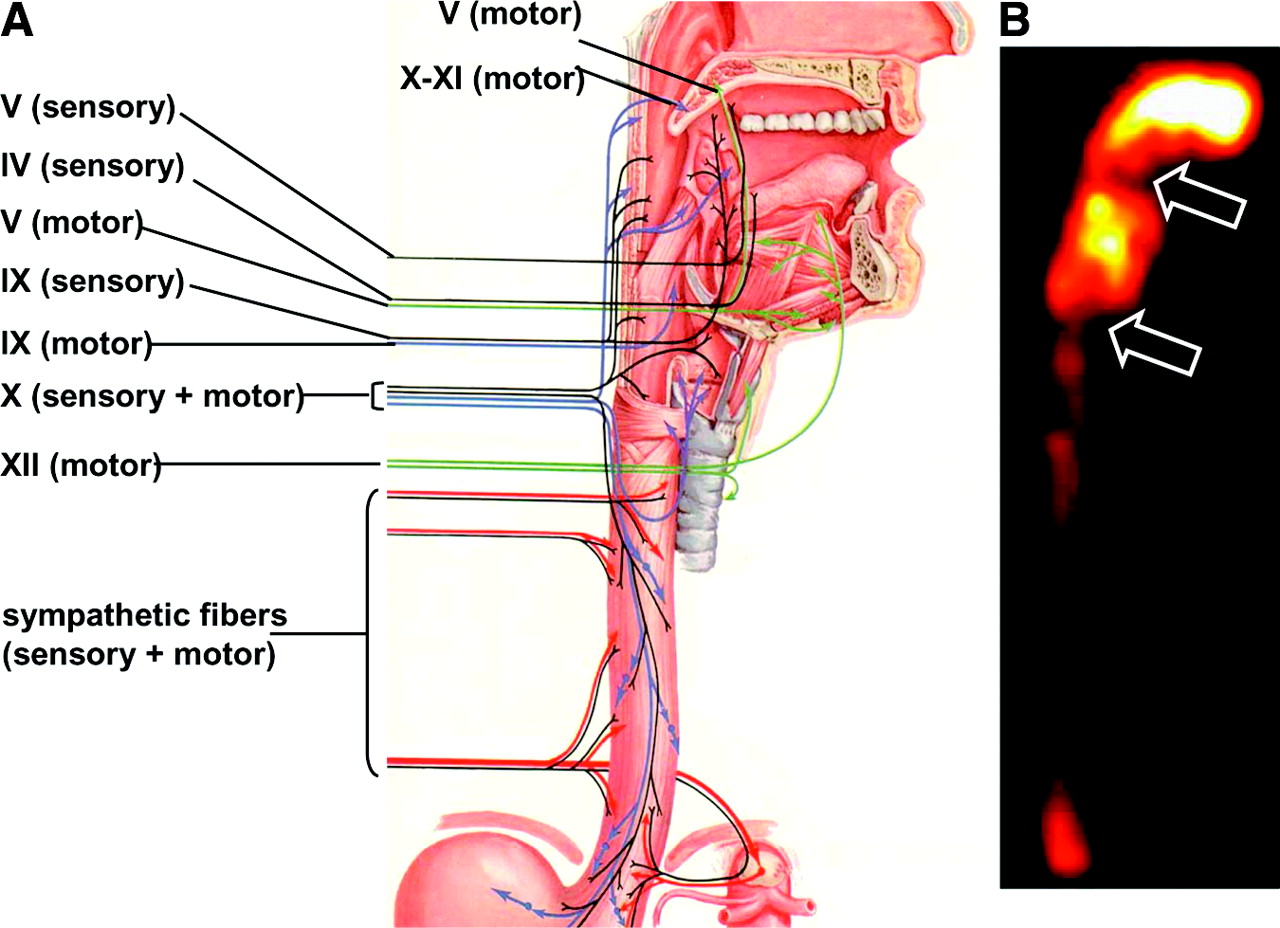
- FIGURE 1.
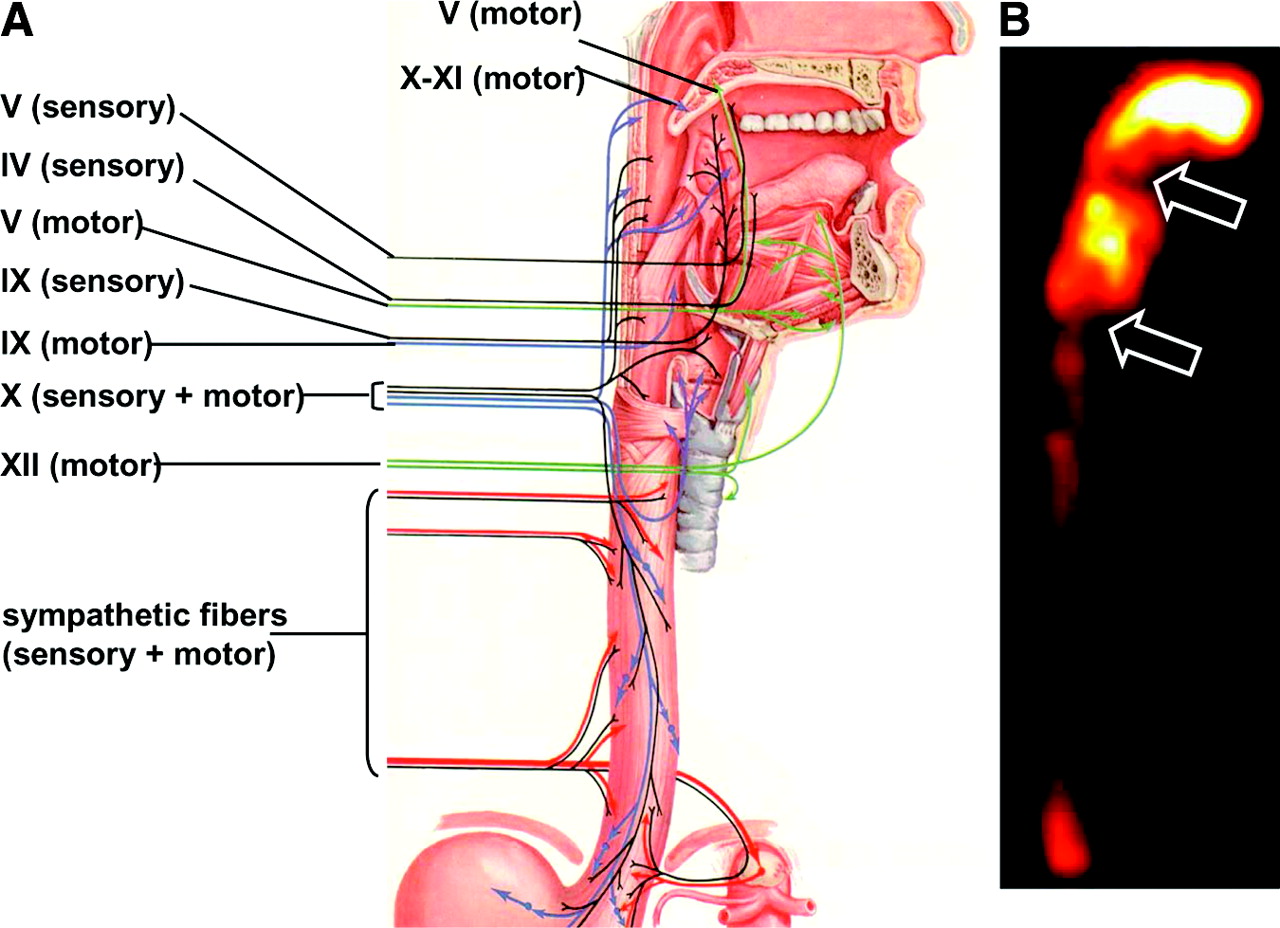
(A) Anatomic drawing shows the complex afferent and efferent neuroregulation of deglutition (sensory fibers in black, motor fibers in different colors) and cranial nerves participating in the system. (B) Summed image from dynamic recording of oropharyngoesophageal radionuclide transit study (liquid bolus) allows clear identification of the various anatomic regions. Upper arrow indicates posterior mouth sphincter, lower arrow indicates upper esophageal sphincter, and space between arrows is pharyngeal region. During scintigraphic acquisition, patient stood facing collimator surface for an anterior view of the chest, with head and neck tilted left. (Modified from (235).)
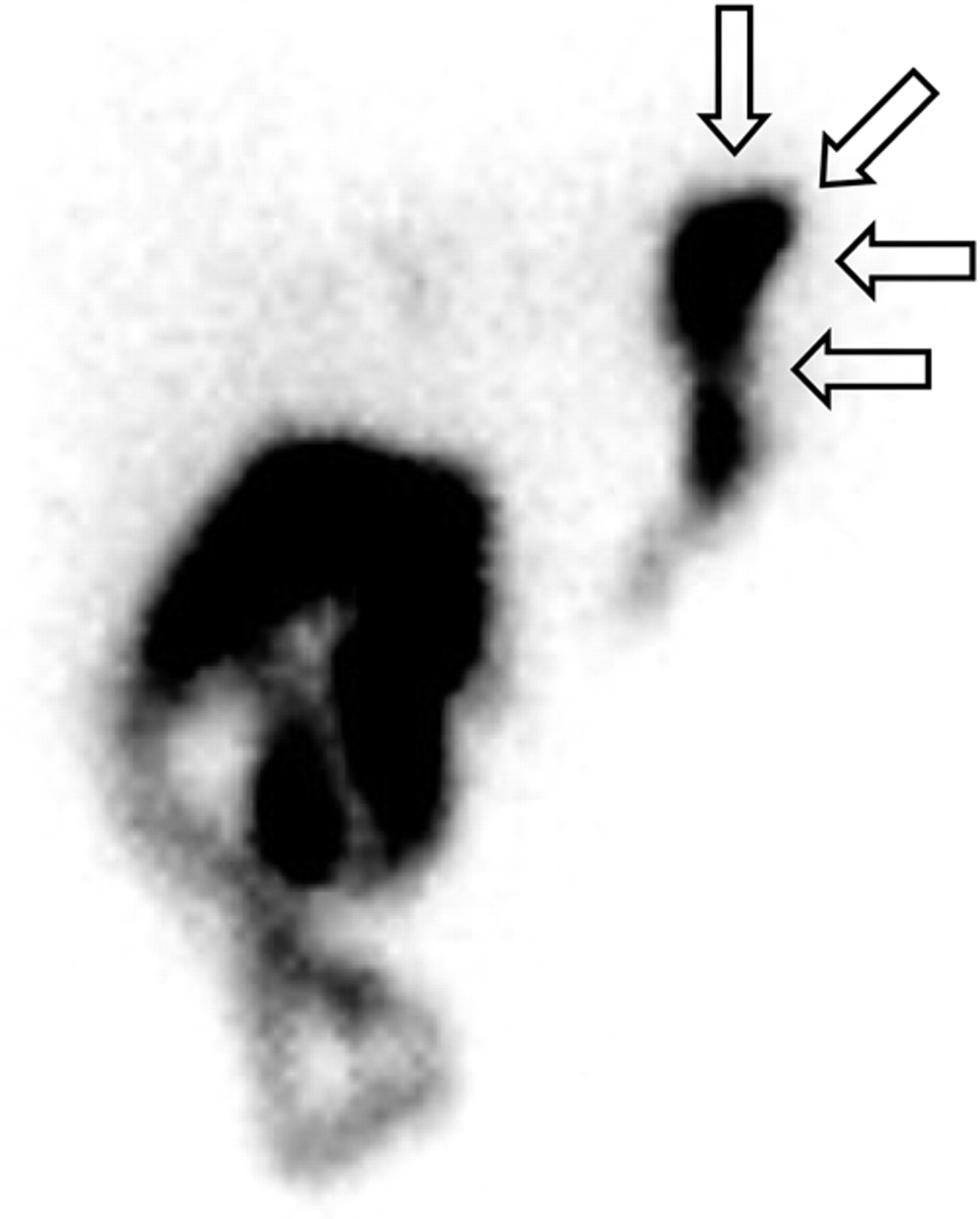
- FIGURE 2.
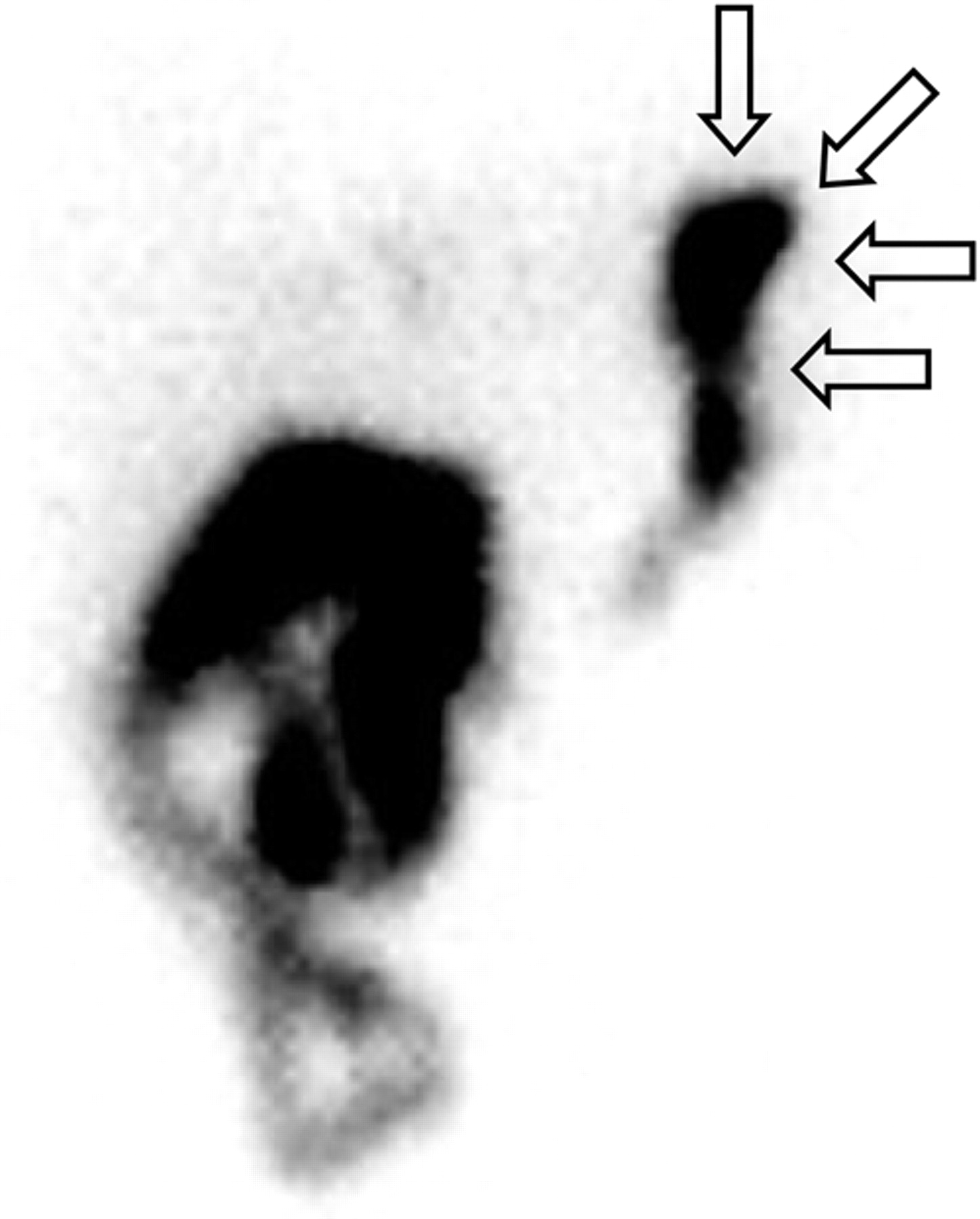
Delayed abdominal hepatobiliary scan (45 min after injection, when radioactivity has almost cleared from hepatocellular compartment) obtained with a 99mTc-iminodiacetic acid analog for a patient with persisting dyspepsia after endoscopic cholecystectomy. Reflux of radioactive bile from duodenum into stomach is obvious (arrows), possibly explaining persistence of symptoms.
- FIGURE 3.
Typical time–activity curves obtained for oropharyngoesophageal radionuclide transit study (10-mL liquid bolus, upright, anterior view) of healthy subject. Shown are curves for mouth (A), pharynx (B), and whole esophagus (C) and for upper third (D), middle third (E), and lower third (F) of esophagus. Summed image at center defines the 3 esophageal ROIs.
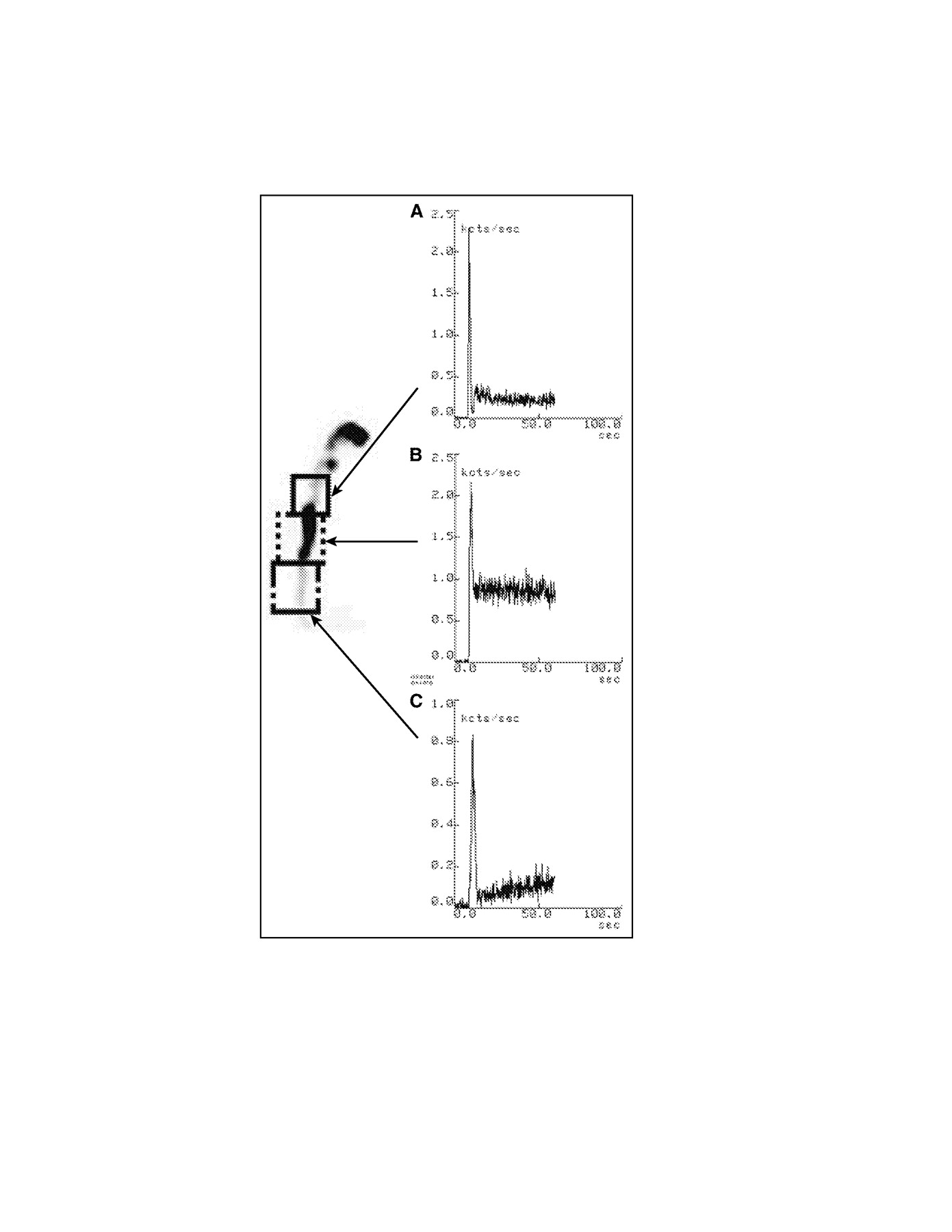
- FIGURE 4.
Examples of radionuclide swallow studies of patients with oropharyngeal dysphagia. (A) Time–activity curve for ROI drawn over oral region of patient with amyotrophic lateral sclerosis after patient swallowed liquid bolus (10 mL, upright, anterior view) shows significant retention and markedly delayed clearance of activity from mouth, with double swallow (piecemeal deglutition because entire bolus could not be swallowed at once). (B) Static image of patient with severe oropharyngeal dysphagia after total thyroidectomy (damage of upper left laryngeal nerve). Dynamic recording of the swallowing of a liquid bolus (10 mL, upright) was impossible because of wide movements due to coughing. Aspiration in trachea is obvious. (C) Semisolid bolus (10 mL, upright, anterior view) did not cause gross aspiration, thus permitting dynamic recording. Time–activity curve obtained for ROI drawn over pharyngeal region on completion of semisolid transit study shows markedly delayed, irregular, and incomplete clearance of radioactivity from pharynx.
- FIGURE 5.
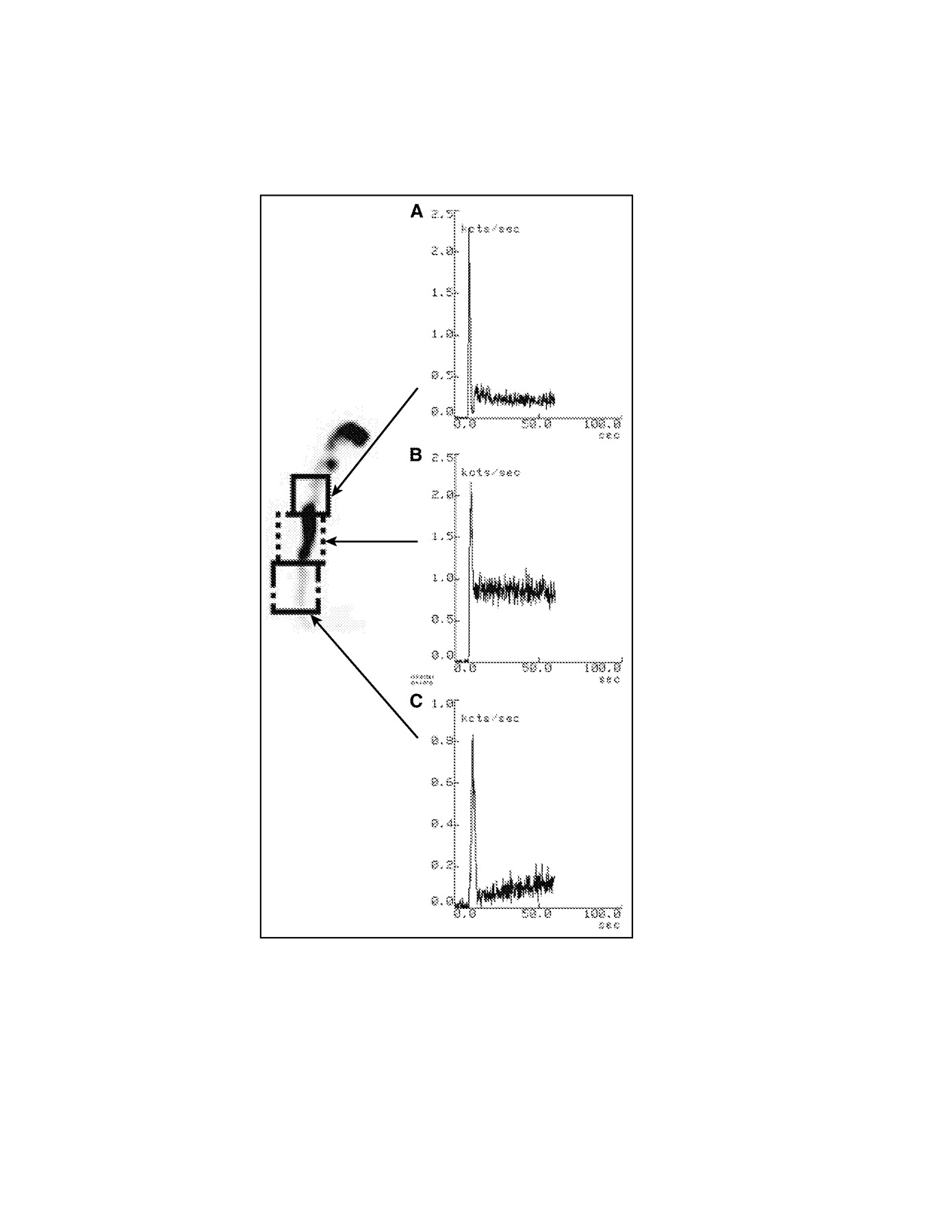
Radionuclide esophageal transit study (15-mL semisolid bolus, upright, anterior view) of patient with amyotrophic lateral sclerosis. Shown are time–activity curves for upper third (A), middle third (B), and lower third (C) of esophagus. Summed image at left defines the 3 esophageal ROIs. All 3 portions of the esophagus clear initially with a normal-appearing pattern, but there is marked retention of radioactivity, mainly in mid esophagus but also somewhat in proximal third, and slow subsequent passage of radioactive bolus to lower third. A similar scintigraphic pattern with delayed clearance of esophageal radioactivity is also seen in patients with achalasia or with scleroderma, but with retention in distal rather than middle portion of esophagus (Fig. 7).
- FIGURE 6.
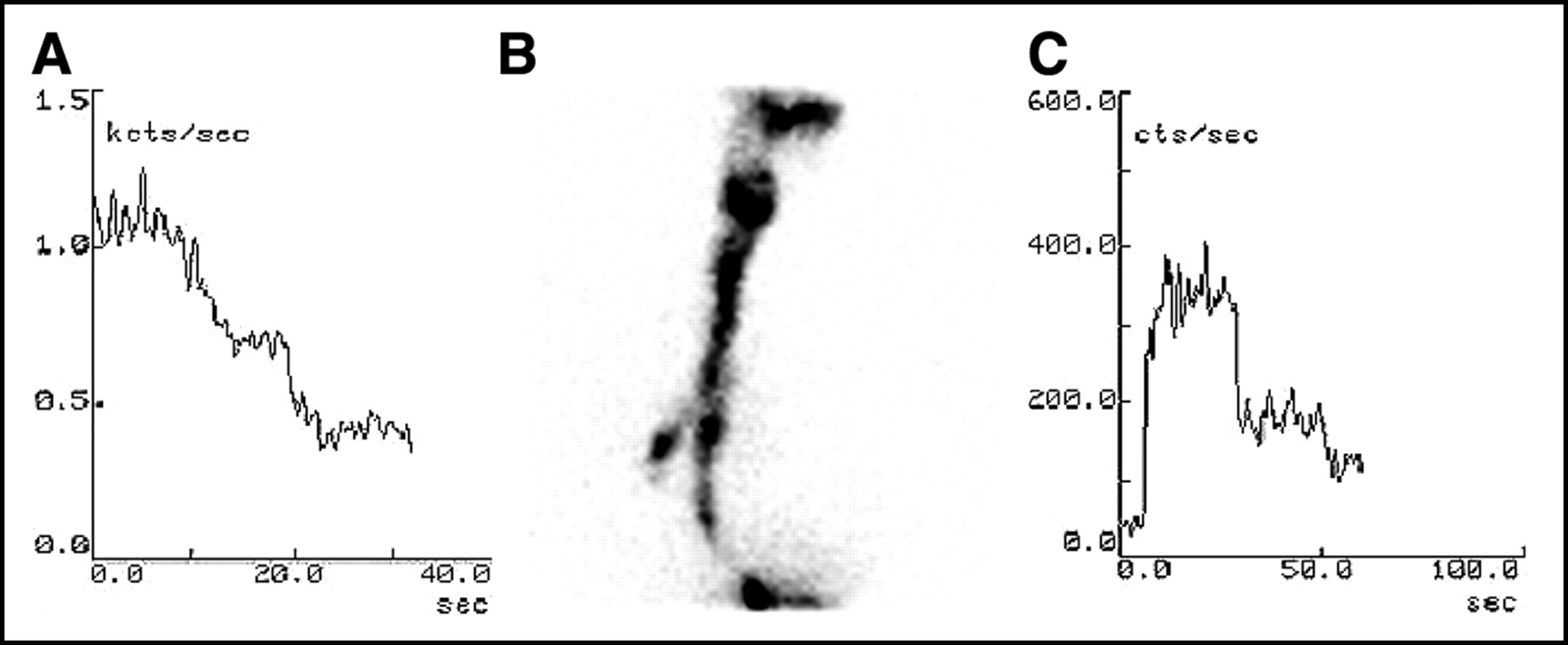
Radionuclide esophageal transit study (10-mL liquid bolus, upright, anterior view) of patient with esophageal dysphagia. (A) One-second frames from dynamic recording show irregular movements of radioactive bolus up and down the esophagus. (B) Time–activity curve for ROI drawn over pharynx shows the normal efficiency of a single swallow without regurgitation. (C) Time–activity curve for ROI drawn over entire esophagus shows incoordinate clearance of radioactivity, the typical pattern for a patient with diffuse esophageal spasm. Review of the dynamic recording in cine mode excluded gastroesophageal reflux as an alternative cause of the irregular, multiple-peak pattern in the esophageal time–activity curve.
- FIGURE 7.
Radionuclide esophageal transit study (15-mL liquid bolus, supine, posterior view, 1 wet swallow followed 30 s later by 3 dry swallows at 15-s intervals) of a patient with achalasia. (A) Summed image of whole esophagus, with ROI. (B) Time–activity curve shows marked retention of radioactivity in the esophagus. Marked esophageal retention of radioactivity remained virtually unchanged after patient stood upright for some minutes. In contrast, esophageal scintigraphy of patients with scleroderma shows similar pattern of radioactivity retention, which, however, clears after they stand.
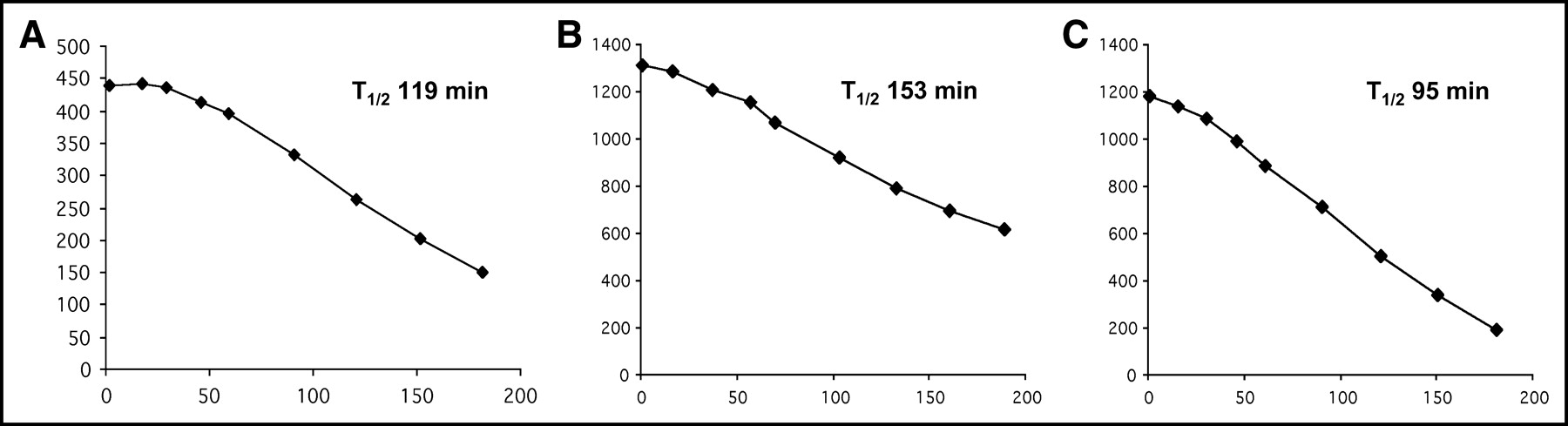
- FIGURE 8.
Examples of gastric-emptying curves (corrected for physical radioisotopic decay) obtained by sequential imaging at discrete intervals after ingestion of radiolabeled solid meal. (A) Results for healthy volunteer (in our institution, T1/2 values of gastric time–activity curves for healthy subjects range from 110 to 120 min). Curve is characterized by distinct lag phase lasting about 20–30 min before emptying begins. (B) Results for patient with gastroesophageal reflux; this curve shows virtually no lag phase and shows markedly delayed gastric emptying, as observed in an average 40% of these patients (236,237). On the basis of this finding, the surgical treatment chosen was fundoplication and pyloroplasty, instead of isolated fundoplication, which would have induced postoperative symptoms (e.g., bloating) with no obvious lag phase. (C) Gastric-emptying curve obtained for same patient after surgical treatment demonstrates slightly accelerated gastric emptying (due to pyloroplasty), with reappearance of a discernible lag phase.
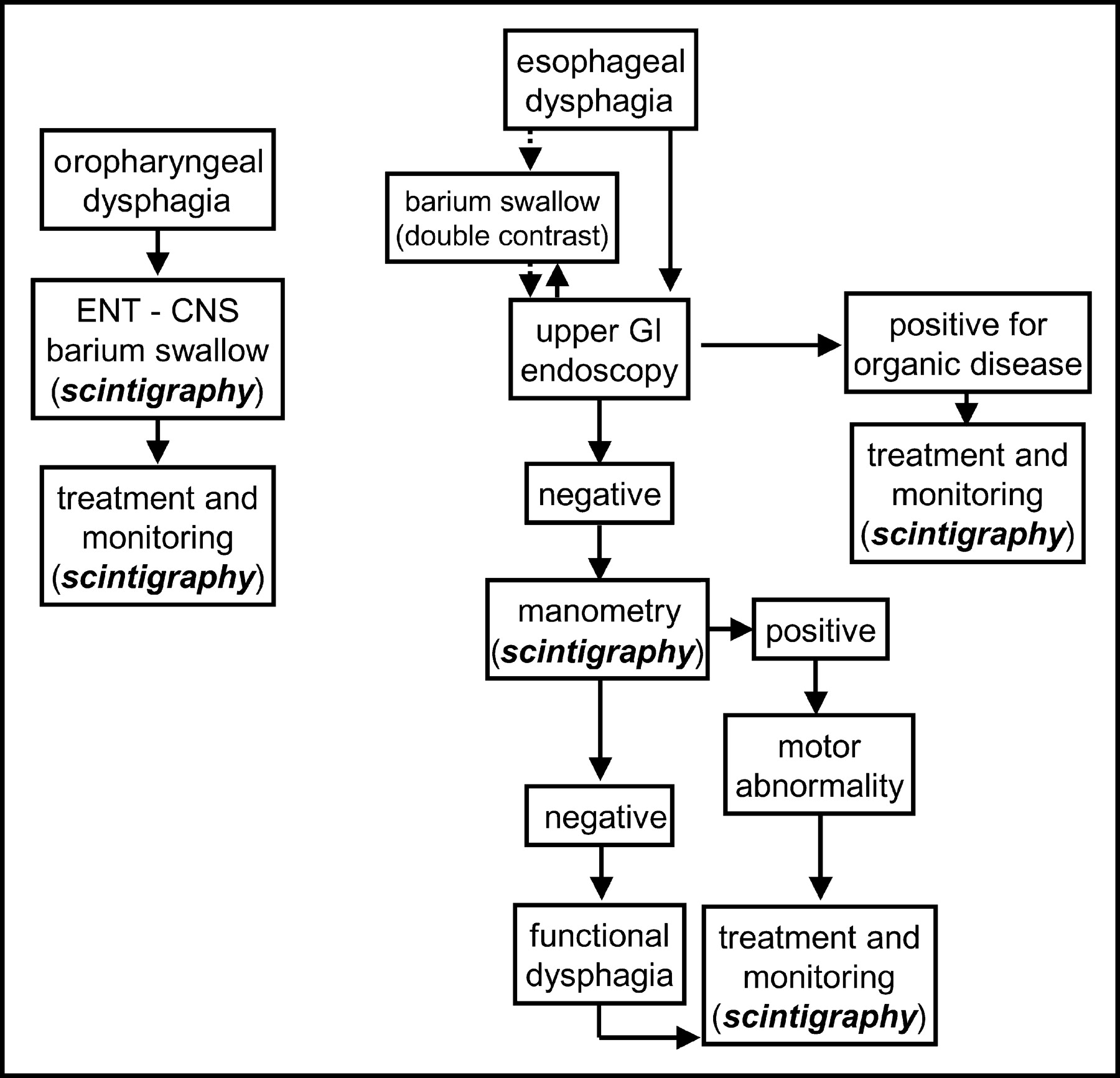
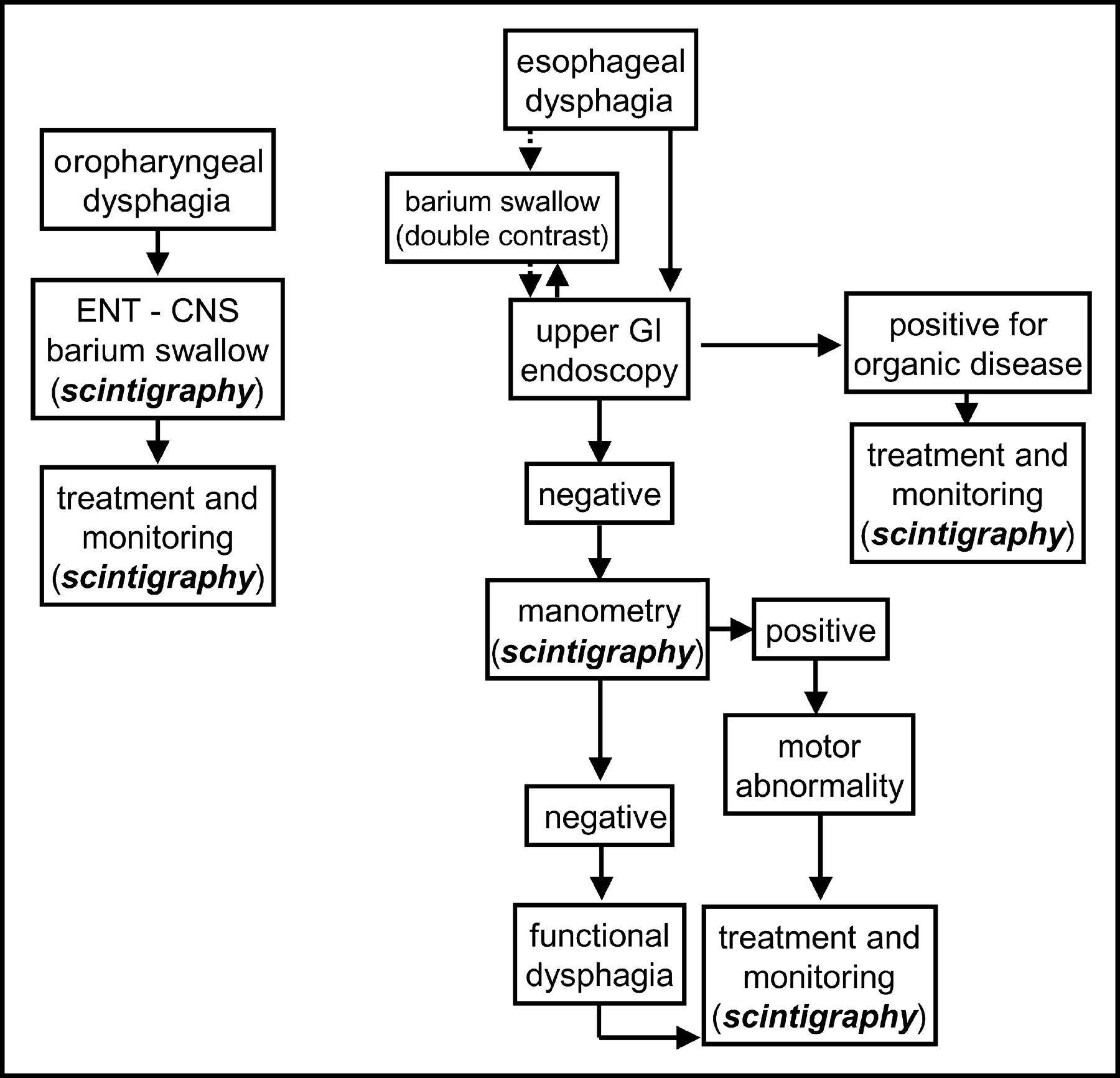
- FIGURE 9.
Proposed diagnostic–therapeutic algorithm for patients with dysphagia of either oropharyngeal or esophageal origin. Oropharyngeal dysphagia is defined as the occurrence of choking, coughing, and nasal regurgitation in association with the initiation of a swallow. Esophageal dysphagia is defined as a sensation of food stuck in the esophagus a few seconds after swallowing. Barium swallow for suspected oropharyngeal dysphagia is best performed as cineradiography. ENT - CNS = otolaryngologic and neurologic evaluation; GI = gastrointestinal.
- FIGURE 10.
Proposed diagnostic–therapeutic algorithm for patients with symptoms suggestive of GERD. Alarm symptoms are defined as pain, dysphagia, anemia, weight loss, fever, and hematemesis. Positive pH-metry is prolonged exposure of the esophagus to a pH of <4 for >5% of the total time. Negative pH-metry is exposure of the esophagus to a pH of <4 for <5% of the total time. A positive symptom index is ≥50% of the symptoms arising simultaneously with drops of esophageal pH to <4, even if extending over <5% of the total time; a negative symptom index is <50% of the same parameter. Full reevaluation is based on the entire set of diagnostic tests available, such as manometry, bilimetry, scintigraphy, upper gastrointestinal series, or multichannel impedance. GI = gastrointestinal; H2-blockers = histamine-2 receptor inhibiting/antagonist drugs; NERD = nonerosive reflux disease; PPI = proton pump inhibitors.
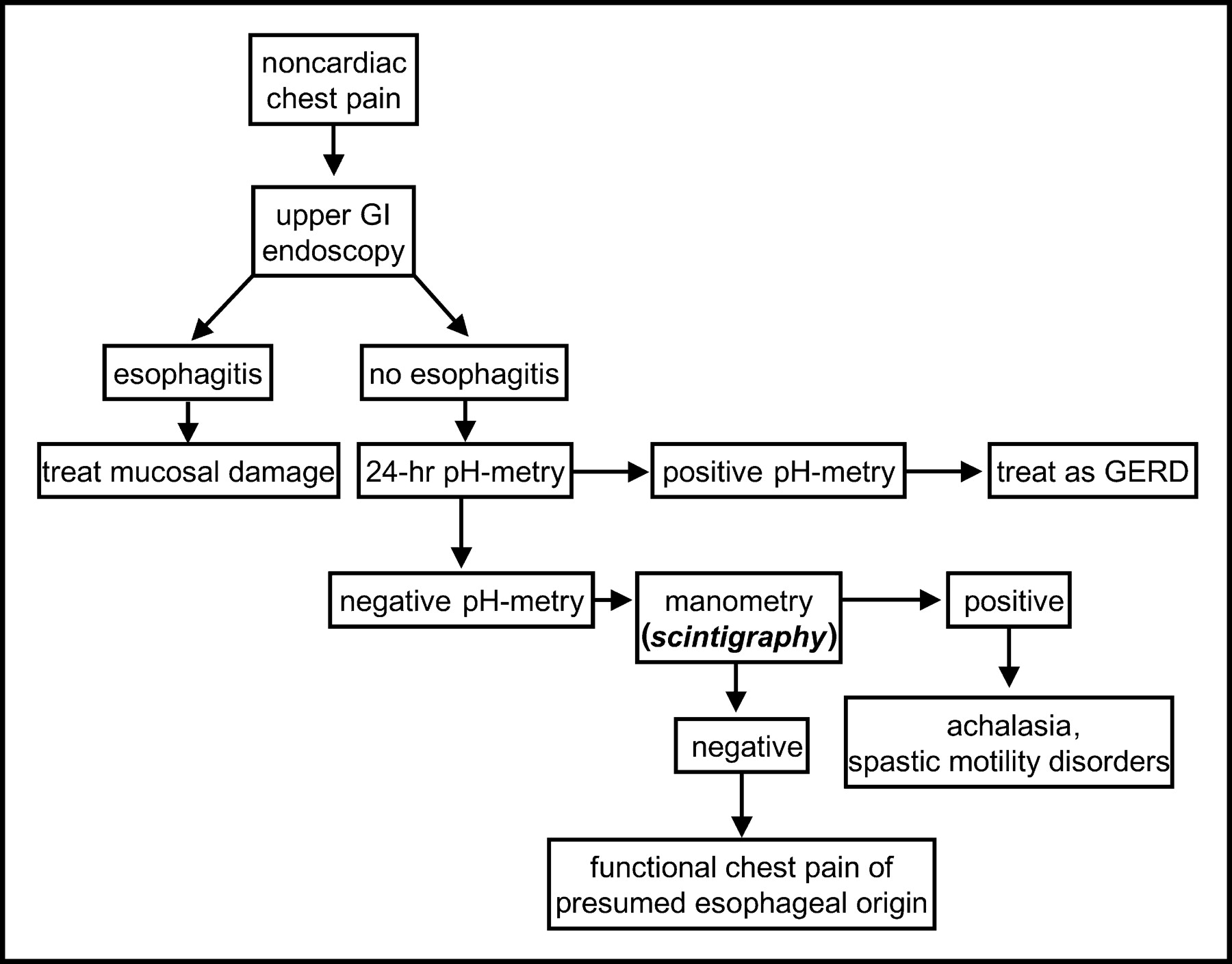
- FIGURE 11.
Proposed diagnostic–therapeutic algorithm for patients presenting with recurrent noncardiac chest pain. Positive pH-metry is prolonged exposure of the esophagus to a pH of <4 for >5% of the total time. Negative pH-metry is exposure of the esophagus to a pH of <4 for <5% of the total time. GI = gastrointestinal.
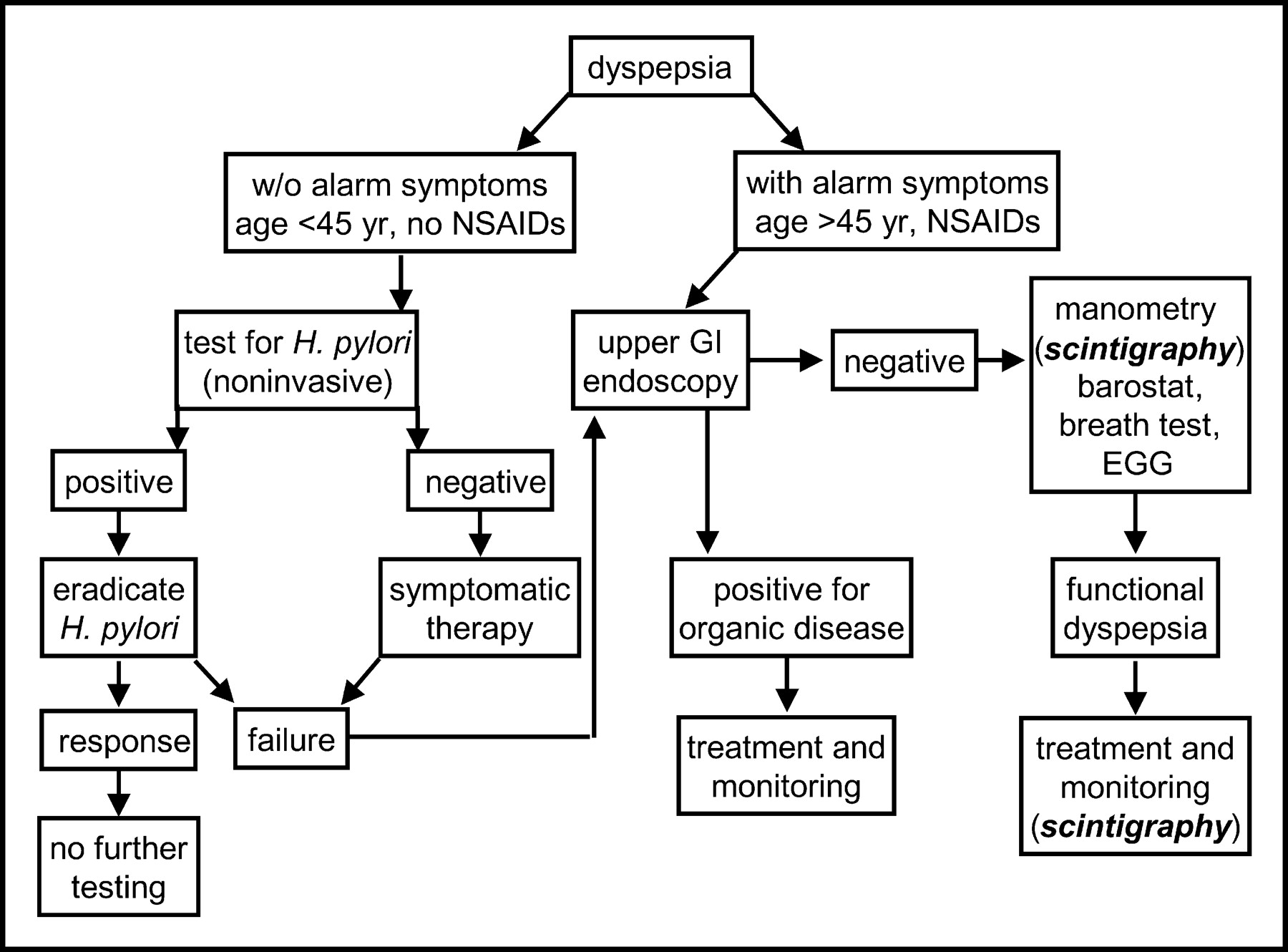
- FIGURE 12.
Proposed diagnostic–therapeutic algorithm for patients presenting with dyspeptic symptoms (epigastric pain or upper-abdominal discomfort). Alarm symptoms are defined as pain, dysphagia, anemia, weight loss, fever, and hematemesis. The breath test is a test for gastric emptying. Organic disease is defined as the presence of tumor or other gross anatomic abnormality. EGG = electrogastrogram; GI = gastrointestinal; NSAIDs = nonsteroidal antiinflammatory drugs.






Tables
Demonstrable abnormality Clinical entity Associated disorder 1. Esophageal dysmotility Category 1: Well-defined entities 1.1.1 Excessive acid exposure GERD Scleroderma, diabetes mellitus 1.1.2 Manometric pattern of achalasia Achalasia Chagas’ disease, enteric neuropathy 1.1.3 Spastic manometric pattern Esophageal spasm Diabetes mellitus, enteric neuropathy Category 2: Entities with variable dysfunction-symptom relationship 1.2.1 High-amplitude peristalsis Nutcracker esophagus Enteric neuropathy 1.2.2Low-amplitude peristalsis Failed peristalsis Low-amplitude simultaneous contractions Ineffective esophageal motility Scleroderma, enteric myopathy, diabetes mellitus, amyloidosis, GERD 1.2.3 Low LES pressure Hypotensive LES Scleroderma, diabetes mellitus, GERD 1.2.4 Incomplete LES relaxation LES dysrelaxation After fundoplication Category 3: Questionable entities 1.3.1 High LES pressure Hypertensive LES Category 4: Entities associated with behavioral disorders 1.4.1 Forced regurgitation Rumination syndrome Anorexia nervosa (purging type), bulimia nervosa (purging type) 1.4.2 Excessive air swallowing Excessive belching Aerophagia GERD 2. Gastric dysmotility Category 1: Well-defined entities 2.1.1 Accelerated gastric emptying Dumping syndrome After resection dumping, or vagotomy dumping Category 2: Entities with variable dysfunction-symptom relationship 2.2.1 Delayed gastric emptying Gastroparesis GERD, diabetes mellitus, scleroderma, after vagotomy, enteric neuropathy, enteric myopathy, anorexia nervosa (restricting type) Modified from (39).
Disorder Definition Esophageal disorders A1. Globus Sensation of a lump, something stuck, or tightness in the throat A2. Rumination syndrome Regurgitation of recently ingested food into the mouth with subsequent remastication and reswallowing or spitting out, in the absence of structural disease A3. Functional chest pain of presumed esophageal origin Episodes of chest pain, usually midline, of visceral quality A4. Functional heartburn Episodic retrosternal burning in the absence of pathologic gastroesophageal reflux, pathology-based motility disorders, or structural explanations A5. Functional dysphagia Sensation of abnormal bolus transit through the esophageal body, in the absence of structural abnormality, pathologic reflux, or pathology-based motility disturbance A6. Unspecified functional esophageal disorder Gastroduodenal disorders B1. Functional dyspepsia B1a. Ulcer-like dyspepsia B1b. Dysmotility-like dyspepsia B1c. Unspecified (nonspecific) dyspepsia B2. Aerophagia B3. Functional vomiting Modified from (17).
- TABLE 3
Comparative Diagnostic Performance of Esophageal Scintigraphy vs. Videoesophagography in Patients with Dysphagia Caused by Various Esophageal Disorders
Disorder Sensitivity (%) Specificity (%) Positive predictive value (%) Esophageal transit scintigraphy Achalasia 91 98 95 Diffuse esophageal spasm 33 99 67 Scleroderma 75 99 75 LES dysfunction 25 99 67 NSEMD 71 76 48 Videoesophagography Achalasia 100 98 96 Diffuse esophageal spasm 67 100 100 Scleroderma 75 100 100 LES dysfunction 25 98 50 NSEMD 62 85 57 NSEMD = nonspecific esophageal motility disorder.
Data are from (234).
Solid meal % bound in gastric juice (3 h) 99mTc chicken liver (in vivo) 98 99mTc-Sulfur colloid whole egg 82 99mTc-Sulfur colloid white egg >95 99mTc surface-labeled chicken liver 84 99mTc-chelex resin 98 (24 h) Data are from (151).
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Gastric Emptying Solid-Meal Content and Misinformation on Social Media Platforms
- Gastric Emptying Scintigraphy
- Compliance with Gastric-Emptying Scintigraphy Guidelines: An Analysis of the Intersocietal Accreditation Commission Database
- Comprehensive Radionuclide Esophagogastrointestinal Transit Study: Methodology, Reference Values, and Initial Clinical Experience
- Imaging of non-malignant disease of the oesophagus and stomach
- The Added Diagnostic Value of Liquid Gastric Emptying Compared with Solid Emptying Alone
- Oesophageal dilatation on high-resolution computed tomography scan of the lungs as a sign of scleroderma
- Radionuclide Evaluation of the Lower Gastrointestinal Tract
- Oesophageal dysmotility in systemic sclerosis: comparison of HRCT and scintigraphy