


Abstract
This review outlines the technical aspects and diagnostic performance parameters of nuclear medicine procedures used on patients with disorders of the lower gastrointestinal tract, with the exclusion of techniques using tumor-seeking radiopharmaceuticals. Chronic disorders of the lower gastrointestinal tract often reduce the quality of life because of discomfort from constipation or diarrhea. Five classes of radionuclide procedures are used to characterize these disorders: transit scintigraphy, searches for ectopic gastric mucosa in Meckel's diverticulum, scintigraphy of active inflammatory bowel disease, scintigraphic defecography, and scintigraphy to detect sites of gastrointestinal bleeding. Protocols for these procedures and their relative merit in patient management are discussed, with special emphasis on their potential for semiquantitative assessment of the pathophysiologic parameter investigated. Quantitation is particularly relevant for prognostic purposes and for monitoring the efficacy of therapy.
In 2004, a review in the Journal of Nuclear Medicine summarized nuclear medicine procedures to characterize motor disorders of the esophagus and stomach (1). This review will focus on radionuclide studies of the small and large bowel, excluding techniques to detect tumors.
Local logistics and the availability of different medical specialties dictate how diagnostic algorithms are applied in the clinical routine when patients present with disorders of the lower gastrointestinal tract. The approach to patients with disorders of the lower gastrointestinal tract should include a team of health-care experts in medical and surgical gastroenterology, nutrition, and imaging (radiologists and nuclear physicians).
CLINICAL BACKGROUND
In 2001, the American Gastroenterological Association estimated the total cost of care for patients with gastrointestinal diseases at $41.8 billion in the United States (2). The clinical manifestations of small- and large-bowel disease most frequently are constipation or diarrhea, sometimes with alternating phases between these 2 extremes. Pain can accompany both conditions, whereas bleeding (presenting either as an acute, clinically obvious sign or as an indolent, chronic event) is less frequent and usually represents a warning sign for the occurrence of more severe diseases. To help the reader understand why this occurs, we will begin with a review of the anatomy and pathophysiology of the lower gastrointestinal tract.
ANATOMY AND PHYSIOLOGY
Small Intestine
The small intestine, a 6-m-long tube extending from the pylorus to the cecum, comprises 3 major segments: The duodenum adds secretions from the pancreas and liver to chyme passing through the pylorus and absorbs chlorine, bicarbonate ions, and calcium. The jejunum absorbs chlorine and bicarbonate in particular, plus a variety of nutrients (carbohydrates, amino acids, and lipids). The ileum absorbs a vast variety of nutrients.
An intrinsic neural network consisting of the myenteric (Auerbach) and the submucosal (Meissner) plexus coordinates motor activities, to facilitate mixing and therefore aid enzymatic digestion in the lumen. If viewed as a simple pipe, the luminal surface area of the small intestine would be about half a square meter. But in reality, its absorptive surface area is roughly 250 square meters, the size of a tennis court, because of 3 features: mucosal folds (circular folds of the inner surface increasing surface area and also aiding to mix the ingesta by acting as baffles), villi (multitudes of mucosal projections that protrude into the lumen and are covered with epithelial cells), and microvilli (the luminal plasma membrane of absorptive epithelial cells, studded with densely packed microvilli, or the “brush border”).
Although goblet cells secrete lubricating mucus into the intestinal lumen, enteroendocrine cells sense the luminal environment and secrete peptide hormones such as cholecystokinin, ghrelin, and gastrin into the blood. Cholecystokinin regulates relaxation of the lower esophageal sphincter, gastric secretion and emptying, gallbladder contraction, and intestinal and colonic motility and also plays a role in the regulation of food intake. Ghrelin, a ligand of the growth hormone secretagogue receptor, regulates energy balance and glucose homeostasis. Gastrin primarily stimulates the secretion of gastric acid.
The 2 most important functions of the small intestine are absorption of nutrients and maintenance of orderly aboral movement of chyme. Smooth muscle cells regulating motor function are controlled by the enteric nervous system, the motor autonomic nervous system, and spinal and vagal extrinsic sensory neurons. Furthermore, several hormones modulate the frequency and patterns of small-intestine contraction.
Colon
The colon (a tubular muscular organ approximately 125 cm long in vivo) performs 3 important functions: concentration of fecal effluent by absorbing water and electrolytes, storage and controlled evacuation of fecal material, and digestion and absorption of food.
The right colon (cecum and ascending colon) plays a major role in water and electrolyte absorption and the fermentation of undigested sugars; the left colon (descending colon, sigmoid colon, and rectum) is involved in the storage and evacuation of stool.
The colonic mucosa presents a relatively smooth surface with numerous crypts composed predominantly of mucus-secreting goblet cells. The longitudinal muscle is organized in 3 bands, called taeniae coli, which run from the cecum to the rectum, where they fuse to form a uniform outer muscular layer. Enteric nervous system neurons are organized into ganglia with interconnecting fibers, which form the submucosal and myenteric plexi. Local neural reflex circuits modulate motility, secretion, blood flow, and probably immune function. Neurotransmitters such as acetylcholine, substance P, and serotonin activate local circuits regulating muscle contractions. The major inhibitory neurotransmitter is nitric oxide. Parasympathetic nerves are predominantly excitatory, and sympathetic nerves inhibitory. Brain–gut connections are important both for perception of visceral stimuli and for modifying colonic function in response to central stimuli.
The contraction patterns in the right colon cause significant mixing, facilitating the absorption of water, whereas in the left colon they slow the movement of formed stool, forming a reservoir until reflexes activate contractions to advance and evacuate stool.
CLINICAL MANIFESTATIONS OF DISORDERS
Diarrhea
Diarrhea is a common outcome of many lower gastrointestinal disorders. It is usually considered a modification of normal bowel function with an increase of bowel movements and fluidity of feces. Because stool consistency is difficult to quantify, stool weight is considered a surrogate marker of diarrhea. Three or more bowel movements per day are considered to be abnormal, and the upper limit of stool weight is generally agreed to be 200 g per day in western countries.
Diarrhea can be associated with other symptoms, such as abdominal pain, fever, rectal emission of blood and mucopus, tenesmus, malabsorption, and dehydration. Diarrhea can be classified into 4 major types: exudative, osmotic, secretory, and secondary to dysmotility.
The incidence of diarrheal diseases is highest in developing countries, with an estimated 4.6–6 million deaths per year in Asia, Africa, and Latin America (3). Although deaths from gastroenteritis are not as common in developed countries, non–food-borne gastroenteritis and other gastrointestinal infections are among the most prevalent digestive diseases in the United States, and the top 2 in terms of indirect costs (4).
Irritable bowel syndrome, lactose intolerance and other dietary factors, inflammatory bowel disease (IBD, which includes ulcerative colitis and Crohn's disease), and colon cancer are the most common causes of chronic diarrhea encountered in primary clinical practice (5).
Irritable bowel syndrome affects up to 20%–25% of the population in western countries, and in 47% of the patients it alternates with constipation (6). The total direct and indirect U.S. costs incurred by the estimated 380,000–480,000 IBD patients has been estimated at around $2 billion per year. Drugs account for only 10%–25% of the total costs, whereas surgery and hospitalization account for approximately half (7).
Constipation
Chronic constipation is a worldwide problem. Its prevalence is estimated to range from 2% from 28% (2), is higher in women than men, and increases with age (8). In the United States, constipation accounts for 2.5 million annual physician visits, an overall expense of about $800 million for laxatives (9), and an estimated annual cost of about $6.9 billion for diagnostic testing (2). In addition to the direct costs, the economic impact of constipation includes reduced work performance, premature retirement, and reduced quality of life (9).
Chronic constipation can be idiopathic, secondary to drugs (especially opioids and anticholinergic agents), or associated with various medical conditions (2). Idiopathic chronic constipation can be further divided into 3 subgroups (10,11): low-transit constipation, dyssynergic defecation, and normal transit constipation (functional constipation and irritable bowel syndrome with constipation).
Gross Gastrointestinal Bleeding
Upper and lower gastrointestinal bleeding leads to more than 300,000 hospitalizations per year in the United States. Lower gastrointestinal bleeding is less common than upper gastrointestinal bleeding, with an estimated annual hospitalization rate of 27 per 100,000 adults at risk (12). The rate of acute gastrointestinal bleeding rises in patients taking aspirin (13). Lower gastrointestinal bleeding accounts for one fourth to one third of all bleeding events, is more common in men than in women, increases in incidence with age, and has a reported mortality rate of approximately 4% (12). Early diagnosis of patients with severe bleeding, and early interventional techniques, lower mortality rates (14,15).
Colonic diverticulosis is by far the most common cause of lower gastrointestinal bleeding, with gross bleeding in almost 5% of patients with this condition, either in the right or in the left colon. Other possible causes of acute lower gastrointestinal bleeding include angiodysplasia and, rarely, small-bowel sources or other colonic lesions, such as colon cancer (12).
Angiodysplasia is a common cause of both acute major lower gastrointestinal hemorrhage and slow intermittent blood loss (10%–40% of the events) (16). Angiodysplastic lesions involve primarily the cecum and right colon. Although angiography and spiral CT frequently identify the lesions (without, however, demonstrating active bleeding), colonoscopy has the advantage of a therapeutic potential.
Neoplastic lesions occur predominantly in the elderly and are the cause of acute lower gastrointestinal bleeding in 2%–26% of cases (17). Hemorrhoids and anal fissures are the most common causes of minor intermittent bright red blood per rectum. Although anal fissures are often painful, bleeding from internal hemorrhoids is usually painless and occurs with straining or the passage of hard stool.
Ischemic colitis, most commonly affecting the splenic flexure, descending colon, and sigmoid colon, causes up to 9% of all cases of major lower gastrointestinal bleeding (12,18). Although the etiology of ischemic colitis includes thrombosis and emboli, the disorder usually develops in the absence of vascular obstruction (19). Ischemic colitis occurs more frequently in the elderly, with conditions such as decreased cardiac output, arrhythmia, trauma, coagulation disorders, and use of drugs causing vasospasm (18). Acute ischemic colitis has a good prognosis and can be treated with medical therapy. Infectious colitis often presents with bloody diarrhea, though the degree of blood loss is rarely significant. Bleeding from IBD accounts for 2%–6% of all cases of acute lower gastrointestinal bleeding (12,18) and is usually minimal to moderate.
In approximately 2%–3% of the general population, a diverticulum occurs in the distal ileum. This diverticulum was initially described by the German surgeon Wilhelm Fabricius Hildanus in 1598 but was recognized and described by Meckel as an embryonic remnant nearly 2 centuries ago (20). In addition to normal ileal mucosa, about 50% of these diverticula contain gastric ectopic mucosa or may occasionally contain duodenal, colonic, or pancreatic mucosa. The gastric mucosa is capable of acid secretion, which can result in ulceration of adjacent ileal mucosa, leading to bleeding. Bleeding usually occurs in infancy or early childhood, although it may occasionally present in adults.
Intussusception, an uncommon cause of bleeding in adults, usually has a leading point, such as a polyp or a malignancy. Ileal or colonic varices (often associated with portal hypertension) may present with massive lower gastrointestinal bleeding, as may rectal varices.
Other rare causes of lower gastrointestinal bleeding are solitary rectal ulcer, aortoenteric fistulae not associated with prosthetic grafts, and nonsteroidal antiinflammatory drugs. Anticoagulants seem to uncover bleeding from preexisting lesions rather than produce bleeding per se (21).
NUCLEAR MEDICINE PROCEDURES
Intestinal Transit Scintigraphy
It is often problematic to determine whether dyspeptic symptoms are caused by dysfunction of the upper or lower gastrointestinal tract. Transit studies are helpful for localizing the potential site of disease and guiding therapy (22). In particular, gastrointestinal transit scintigraphy is the only imaging procedure that allows us to measure both total and regional transit times, defining whether dysmotility is generalized or localized and quantifying its severity.
Small-bowel transit scintigraphy is useful when symptoms such as bloating, early satiety, dyspepsia, or nausea appear soon after the meal and are accompanied by postprandial diarrhea. Also, symptomatic patients with prior intestinal resection should be evaluated for the possibility of an abnormally rapid small-bowel transit, because physiologic control of transit depends on the intact jejunal and ileal brakes (23,24). Small-bowel transit scintigraphy is typically performed in conjunction with gastric-emptying or colonic transit studies.
Colonic transit scintigraphy is used to characterize patients with symptoms of altered colonic transit including constipation, abdominal bloating, and refractory irritable bowel syndrome. This procedure is useful for identifying the presence and severity of transit abnormalities (including information on specific colonic regions) and for assessing response to therapies.
Because it sometimes is helpful to evaluate motility throughout the entire gastrointestinal tract, whole-gut transit scintigraphy was developed. This test is useful for assessing diffuse dysmotility involving both the upper and the lower gastrointestinal tract and frequently leads to changes in diagnosis and patient management (25).
Several techniques have been proposed. Because there is no single best protocol for performing this study, centers are encouraged to comply with what can be defined as a best-practice procedure with regard to patient preparation, radiopharmaceutical, diet (calorie, fiber, carbohydrate, fat, and protein content), protocol of acquisition, and data elaboration. Considering the complex pathophysiology of gastrointestinal motility, it might be advisable to adopt a protocol that measures both gastric emptying and intestinal transit, such as a dual-labeled solid–liquid meal.
111In-Diethylenetriaminepentaacetic acid (DTPA) is not absorbed in the gastrointestinal tract. The 67-h physical half-life of 111In allows imaging over several days. To be delivered to the cecum as a solid, the tracer is adsorbed on a solid-phase material. Two different methods are currently applied for colonic transit scintigraphy using this radiopharmaceutical. The Mayo Clinic protocol is based on oral ingestion of a single methacrylate-coated capsule containing the radiolabeled agent (currently 3.7 MBq [100 μCi] of 111InCl3 or 111In-DTPA adsorbed on activated charcoal particles) (26,27). The methacrylate coating dissolves in the relatively alkaline environment of the ileum (pH 7.4), so that the distal ileum delivers the pellets in a bolus fashion to the cecum. Commercially available enteric capsules designed to deliver drugs to the region of the cecum and colon also offer a suitable and simpler alternative.
To evaluate the upper gastrointestinal tract (gastric and small-bowel transit), one should perform both solid- and liquid-phase emptying studies. 99mTc-Sulfur colloid–labeled scrambled eggs and ingestion of 111In-DTPA (4.6 MBq) mixed with 300 mL of water (Temple University Hospital protocol) (25) can be imaged simultaneously (using multiple energy windows) to measure gastric emptying and small-bowel transit simultaneously (28).
Imaging for gastrointestinal transit studies is performed with large-field-of-view γ-cameras equipped with medium-energy collimators (if using 111In either alone or as part of a dual-tracer study), or, if the study is performed with a 99mTc tracer only (typically gastric emptying with tracer-labeled scrambled eggs), a low-energy collimator can be used. Radioisotopic markers placed on the xiphoid process and iliac crests may help better define the anatomy. Gastric-emptying data, if needed, should be acquired as described previously (1). All protocols for gastrointestinal transit scintigraphy are based on sequential imaging after ingestion of the radiolabeled meals, with simultaneous images recorded in both the anterior and the posterior projections (analyzed after the images are combined to produce a geometric mean image). The timing of acquisitions varies with the region of the gastrointestinal tract to be evaluated; for example, the small bowel requires more frequent imaging in the first few hours, whereas the colon requires delayed imaging up to 48 or even 72 h.
Quantification is based on region-of-interest counts of geometric mean images derived from the anterior and posterior acquisitions, correcting for radioactive decay and for downscatter of the 111In counts in the 99mTc window in the case of a dual-isotope meal. Various parameters for characterizing small-bowel and colonic transit are described later in this article.
The small-bowel transit time can be calculated from deconvolution of gastric emptying and of the colonic filling curves (median values being 160–170 min in healthy volunteers for either 131I-fiber or liquid 99mTc-DTPA) (29). The orocecal transit time is defined as the time for initial arrival of an orally administered tracer to the cecum, with the normal time being 297 ± 65 min (95% confidence interval, 154–440 min) (25,30). The 10% small-bowel transit time is calculated by subtracting the time for 10% gastric emptying from the time to 10% colonic filling. This simple evaluation also corrects for delayed gastric emptying and yields average reference values of about 280 min for solids (approximate range, 240–320 min) and 295 min for liquids (approximate range, 255–335 min) (30,31). The small-bowel transit index is calculated as the percentage of small-bowel activity at the terminal ileum–cecum/ascending colon at 6 h relative to total small-bowel activity (the index is >40% in healthy individuals) (25). This index, along with the 10% small-bowel transit time, is currently the most widely adopted parameter for clinical purposes.
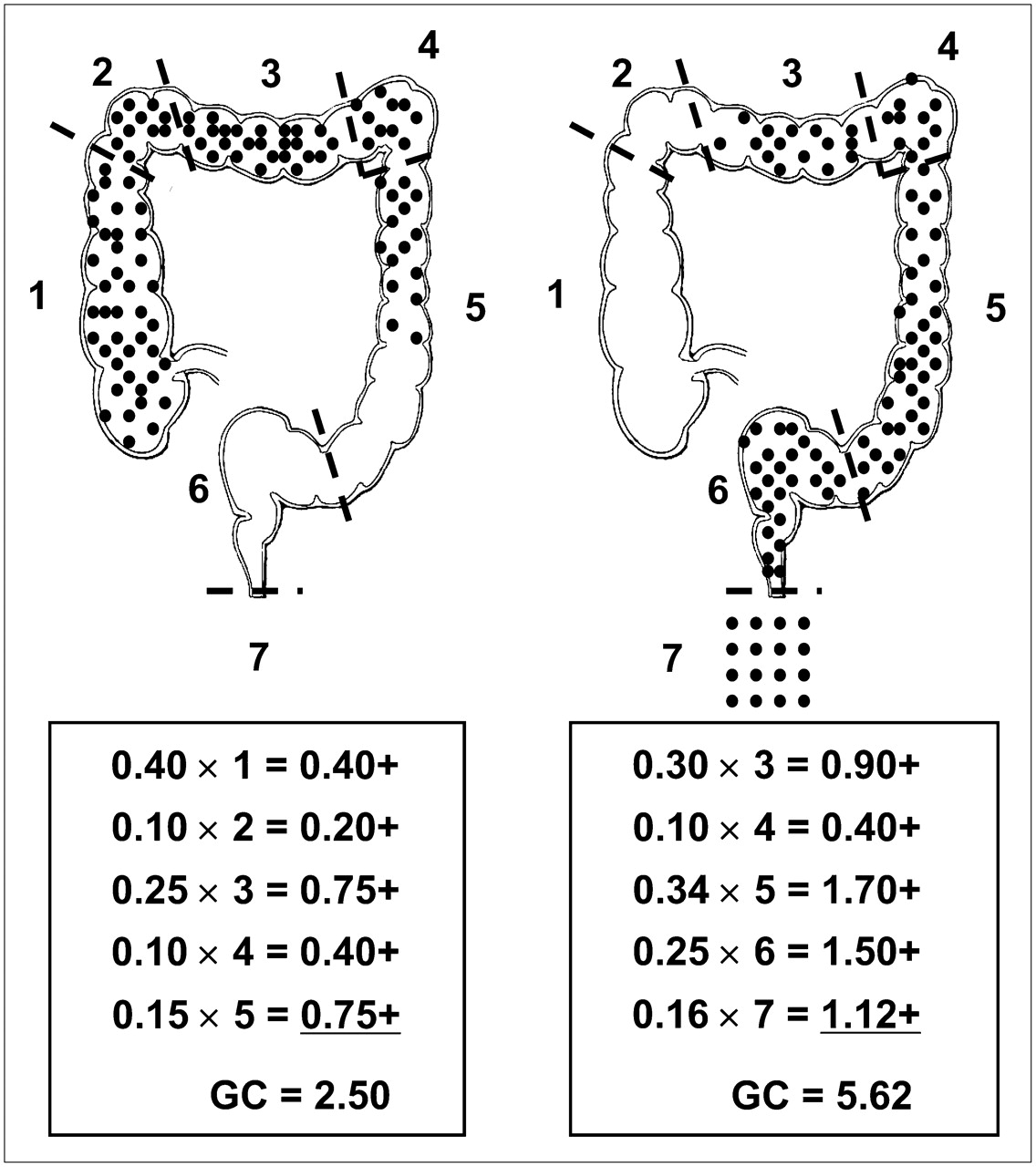
The geometric center, commonly adopted as a parameter of colonic transit, is the weighted average fraction of counts in different colonic regions, that is, (region-of-interest counts)/(administered counts) (25,32). The Mayo Clinic and the Temple University protocols differ in the number of regions into which they divide the colon, 4 and 6, respectively (with an additional “virtual” region represented by evacuated radioactivity). The weighting factor increases from 1 to 5 (Mayo Clinic protocol) or from 1 to 7 (Temple University protocol) in a proximal-to-distal fashion (e.g., from cecum to rectosigmoid and to evacuated stool). Therefore, a low value for geometric center indicates that most radioactivity is in the cecum, whereas a high value means that activity is in the rectosigmoid region or has been evacuated (Fig. 1).

Diagrammatic representation of geometric center approach for estimating colonic transit time. According to Temple University protocol, colon is subdivided into 6 regions with weighting factors increasing from 1 to 6 proximally to distally (cecum and ascending colon to rectosigmoid). Highest weighting factor (7) is assigned to radioactivity unaccounted for in images, which is therefore assumed to have been evacuated in stools. Each black dot represents 1% (or 0.01 fraction) of radioactivity that has reached colon. Examples of calculation are given in inserts for 2 different geometric centers, 2.50 on left and 5.62 on right. In actual colonic transit study performed on healthy individual, most radioactivity would be seen in transverse colon at 24 h (geometric center, approximately 3), progressing to descending colon at 48 h (geometric center, about 5), and being mostly evacuated at 72 h (geometric center, about 6–7). In patient with colonic inertia, radioactivity would not significantly progress past hepatic flexure at 48 h or at 72 h (geometric centers, about 1.5–2 and 2–3, respectively). In patient with functional rectosigmoid obstruction, progression of radioactivity would be nearly normal until 48 h after ingestion, combined however with little further progression at 72 h (geometric center, about 5–6), thus indicating obstructed defecation.
The primary parameter of interest is the geometric center at 24 h (reference range, 1.6–3.8). The reference values for the geometric center according to the Mayo Clinic protocol are no more than 1.4 for 4 h and 1.7–4.0 for 24 h (26). Slow colonic transit is defined as a geometric center lower than the reference value at 24 h. With the solid–liquid meal of the Temple University protocol, the reference values for geometric center mean are 4.6 ± 1.5 at 24 h, 6.1 ± 1.0 at 48 h, and 6.6 ± 0.2 at 72 h.
As a practical rule, the colon should be imaged at 24 and 48 h. A geometric center less than 4.1 at 48 h obviates further imaging, because colonic transit is obviously delayed. When geometric centers are in the 4.1–6.4 range at 48 h, imaging at 72 h is useful for excluding functional outlet obstruction. Accelerated colonic transit, as in patients with diarrhea, results in a geometric center greater than 6.1 (at or beyond the rectosigmoid tract) at 24 h. The geometric center is the best predictor of delayed colonic transit and has a significant impact on patient care, often leading to changes in both diagnosis and treatment (25). Furthermore, this semiquantitative score of colonic transit can be used to compare different patients or groups of patients, as well as serial evaluations of the same patient, for such assessments as the efficacy of prokinetic therapy or the unwanted side effects of analgesic drugs.
Scintigraphic transit studies have been used to characterize transit and motility in patients with functional bowel syndromes, particularly in those patients who do not have a secondary form of constipation and have refractory symptoms after a high-fiber diet and laxatives (10). The scintigraphic study can elucidate if a patient with functional constipation has colonic inertia or functional rectosigmoid obstruction. Alternatively, finding a normal scintigraphic transit pattern in a patient complaining of obstinate constipation may indicate that the patient has psychogenic abnormalities or a misconception of normal bowel movements (33).
In small-bowel transit scintigraphy, an abnormal 6-h transit index may reveal small-bowel dysmotility in patients with functional dyspepsia and normal gastric emptying (34) or patients with a panenteric motor disorder. In addition, accelerated transit through the small bowel or colon has been found in patients with diarrhea-predominant irritable bowel syndrome (35). Slow colonic transit justifies therapy with prokinetic agents or laxatives, or with biofeedback in patients with functional rectosigmoid obstruction, or even with subtotal colectomy in severe colonic inertia. On the other hand, diffuse dysmotility is a contraindication to colectomy.
Gastrointestinal Bleeding Scintigraphy
Because gastrointestinal bleeding is typically intermittent, scintigraphy offers the advantage of continuous monitoring of patients to localize sites of gastrointestinal bleeding throughout the entire gastrointestinal tract. In many cases, the bleeding site can be identified with sufficient confidence to direct surgical intervention or to guide subsequent diagnostic testing (36–38). Scintigraphy may also provide prognostic information because those patients who require urgent care (surgery or transfusion) often have their bleeding site identified in the first hour (39). Positive findings on gastrointestinal bleeding scintigraphy are associated with higher hospital morbidity and mortality than are negative findings (40).
The ability of gastrointestinal bleeding scintigraphy to detect bleeding at low flow rates (0.04 mL/min in an animal model) (41) is a distinct advantage over angiography, which detects bleeding only if it occurs during the procedure, with a minimum detectable blood flow rate of 0.5–1 mL/min (42). The sensitivity of 99mTc-red blood cell (RBC) imaging is actually linked to the volume of extravasated RBCs at the bleeding site. A focal volume of approximately 3 mL can readily be detected. However, if the patient has hyperactive peristalsis, the volume may be distributed over a substantial length of bowel, reducing the sensitivity of the procedure.
Although both 99mTc-sulfur colloid and 99mTc-labeled RBCs have been used for gastrointestinal bleeding scintigraphy, clinical studies comparing the 2 radiopharmaceuticals in the same patients demonstrate the clear superiority of the 99mTc-RBC procedure (43,44). The Society of Nuclear Medicine procedure guidelines for gastrointestinal bleeding scintigraphy recommend the use of in vitro labeled 99mTc-RBCs to minimize elution of the label from the RBCs (36). Table 1 summarizes various drug-related factors that may affect RBC labeling with 99mTc. Even with in vitro labeled RBCs, a small amount of activity is excreted in the urine, and it is important not to confuse this bladder activity with activity extravasated in the rectum.
Drug-Related Factors That May Affect RBC Labeling with 99mTc
The exact mechanism of RBC labeling has not been fully elucidated (45). All procedures use a stannous ion (stabilized in a complex such as pyrophosphate, medronate, or DTPA). It is postulated that Sn+2 diffuses freely into erythrocytes and remains bound to intracellular components. 99mTc-pertechnetate diffuses across the RBC membrane. In the presence of Sn+2, intracellular pertechnetate is reduced from +7 valence to +4, thus binding mainly to the β-chain of hemoglobin. It has also been suggested that most 99mTc-pertechnetate is not associated with hemoglobin but rather remains in a more labile intracellular pool or on the cell membrane (46). Because the levels of Sn2+ are critical for efficient labeling, insufficient amounts of Sn2+ will not reduce all 99mTc, thus leading to the persistence of free 99mTc-pertechnetate. On the other hand, excess Sn2+ can reduce 99mTc-pertechnetate at other sites in the extracellular compartment, thus making it unavailable to RBCs. Kits are available for 99mTc-RBC labeling, and adherence to manufacturers' instructions regarding storage and incubation time is strongly recommended. Table 2 lists the technical factors that may interfere with labeling.
Technical Factors Associated with Poor 99mTc Labeling of RBCs
Gastrointestinal bleeding scintigraphy commonly uses serial images after an intravenous bolus injection of the radiolabeled, washed RBCs. The exact timing and modalities of dynamic imaging vary from center to center, but recording the initial phase (1–2 min after injection) as an abdominal blood-flow study (1–5 s/frame) may help with recognizing a vascular mass in the abdomen and with localizing the site of bleeding more precisely. After the initial radionuclide angiogram, serial images are commonly recorded at 1 min per frame for 60–90 min. Images can be reviewed as a cinematic display (47) or by summing the images to make multiple sets of 10–15 min each (or shorter, if needed). If no bleeding site is identified within the first 90 min, delayed images are usually acquired, typically at 2–6 h or 18–24 h after injection (38,48,49).
Acquisition of SPECT images can be helpful for localizing bleeding sites, especially if the imaging is performed with hybrid SPECT/CT (Fig. 2) (50,51). However, because intraluminal blood is an irritant, radioactivity can move quickly in the intestinal lumen (sometimes with alternating anterograde–retrograde movements) during the relatively long SPECT acquisition, which may make it difficult to accurately localize the bleeding site.
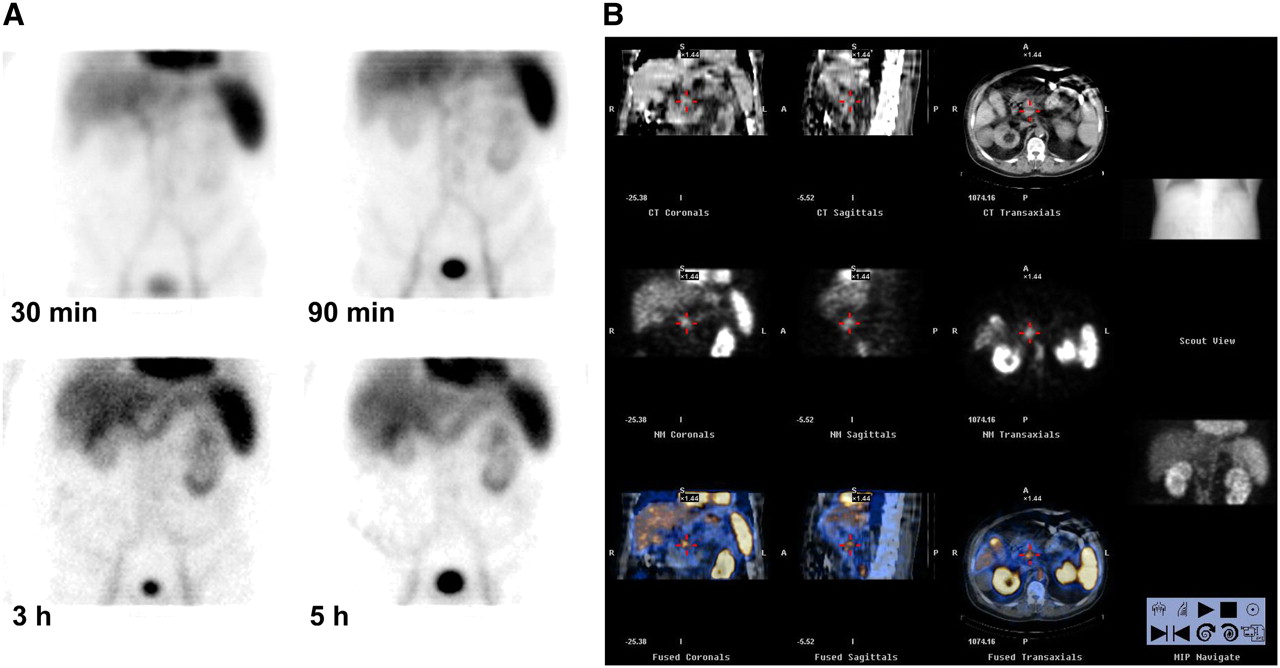
(A) Sequential static 5-min images of abdominal area recorded at various times after 99mTc-RBC injection. Abnormal accumulation of radioactivity is obvious already in early images (elongated horizontal area in upper abdominal region). Although accumulation of radioactivity increases with time, no obvious progression along intestinal tract is detectable. Localization of bleeding site is equivocal in planar images, being possibly consistent either with transverse colon or with duodenal localization. (B) SPECT/CT images after 99mTc-RBC injection demonstrate that radioactivity accumulation is not localized in anterior abdominal area (as transverse colon would be) but rather in mid region, thus indicating duodenal localization of bleeding. (Courtesy of Dr. Elena Lazzeri, Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa, Italy.)
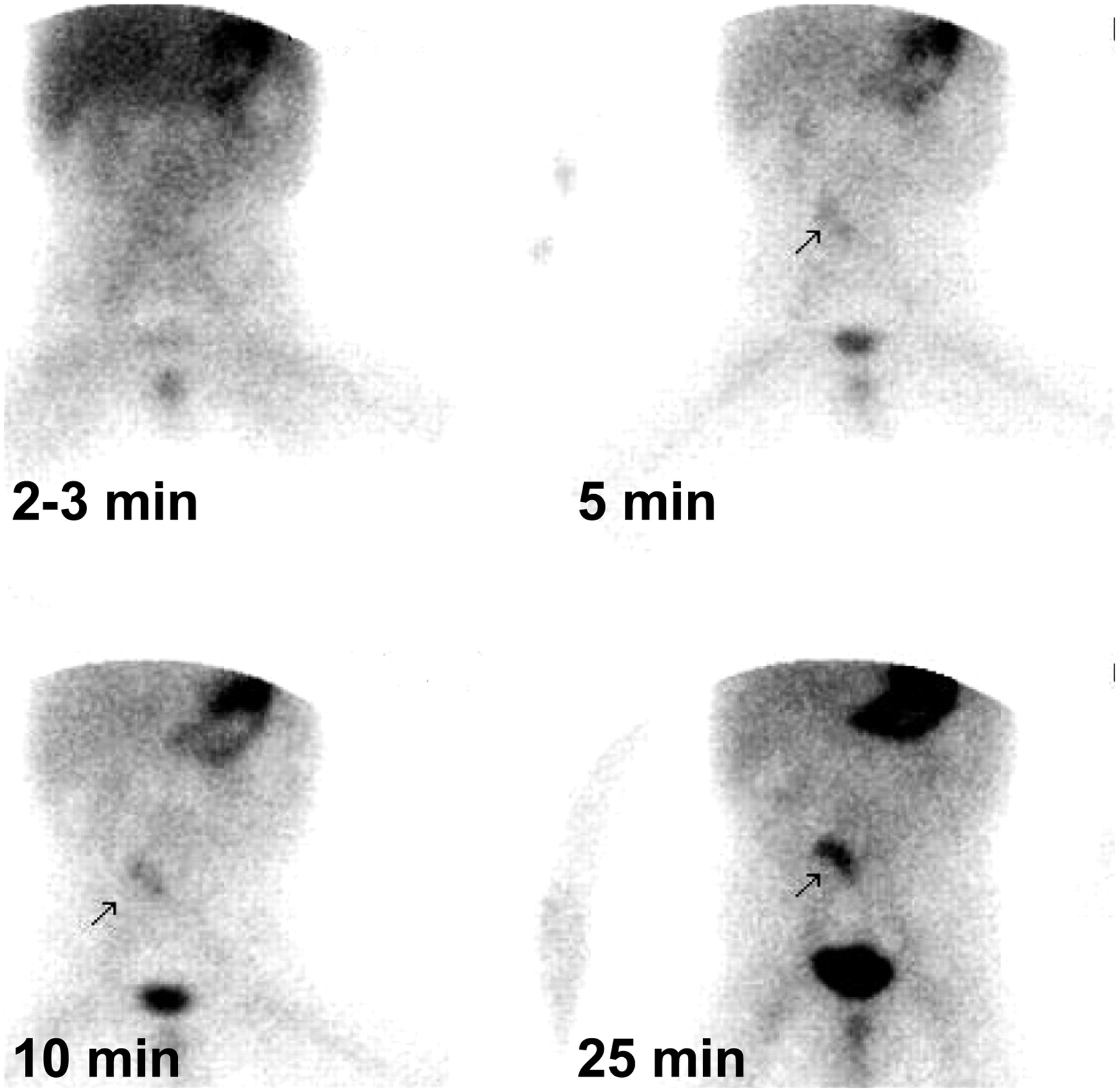
The key sign of gastrointestinal bleeding is the presence of an area of extravascular activity that increases in intensity over time or the presence of a focus of activity that moves in a pattern corresponding to bowel (Fig. 3). Movement of activity in the lumen might be anterograde or retrograde because of the irritating characteristics of intraluminal blood. Localization of bleeding is based on the identification of the focus of initial blood extravasation and on subsequent movement of activity, making dynamic imaging essential for correct localization. Colonic bleeding occurs at the periphery of the abdomen, and extravasated blood often pools in haustra. Bleeding in the small intestine occurs in the central abdomen, and the radioactivity progresses rapidly through the small curvilinear intestinal loops.

Bleeding scintigraphy performed on 82-y-old man whose presenting symptom was intermittent bright rectal bleeding. (A) Early dynamic imaging sequence after intravenous administration of 99mTc-RBCs (each frame is summed image of 5-min sequence) shows no definite area of abnormal radioactivity accumulation. (B) Later dynamic sequence starting 60 min after injection of 99mTc-RBCs clearly shows abnormal accumulation of radioactivity initiating in proximal descending colon and extending to whole descending colon, as also confirmed by subsequent SPECT (image not shown).
Ectopic Gastric Mucosa in Meckel's Diverticulum
Meckel's diverticulum, a remnant caused by incomplete closure of the omphalomesenteric duct, is located in the ileum about 50–80 cm from the ileocecal valve. Gastric acid and pepsin produced by ectopic gastric mucosa can cause mucosal damage and bleeding (52). Because 99mTc-pertechnetate avidly accumulates in gastric mucosa, it can reveal ectopic gastric mucosa in a Meckel's diverticulum. Scintigraphy with 99mTc-pertechnetate is therefore used to localize ectopic gastric mucosa in a Meckel's diverticulum as the potential source of unexplained gastrointestinal bleeding (36,53). Scintigraphy with 99mTc-RBC remains instead the optimal radionuclide procedure for visualizing active bleeding per se.
The test is the most accurate noninvasive technique for identifying ectopic gastric mucosa in Meckel's diverticulum, with high specificity and positive predictive value (close to 100%) both in children and in adults (54,55).
After intravenous injection of 99mTc-pertechnetate, serial images of the abdomen are recorded for at least 30 min, usually at the rate of 30–60 s per frame, in the anterior view. These images may be summed to make multiple sets of 10–15 min each, to facilitate interpretation of the data. Additional static images, anterior oblique projections, lateral projections, and posterior projections are recommended at the end of the dynamic acquisition. Similarly to bleeding scintigraphy, SPECT can greatly aid localization of the lesion in Meckel's diverticulum (56).
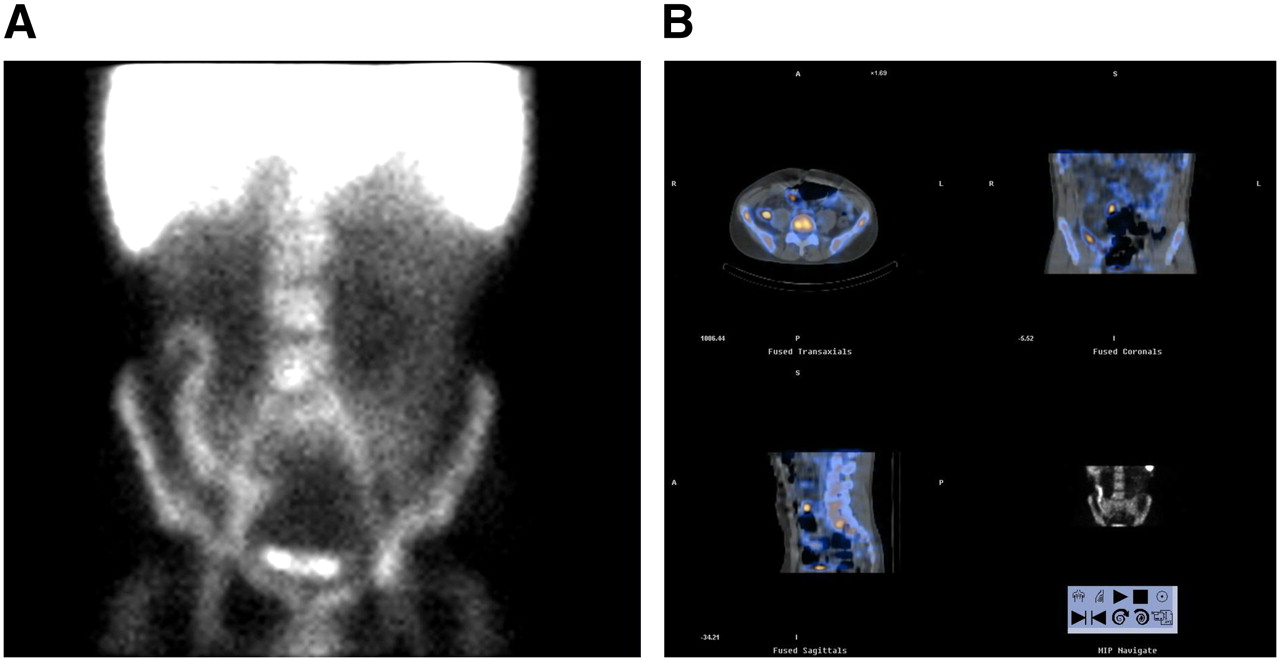
A positive scan shows activity in the ectopic gastric mucosa at the same time as activity in the normal gastric mucosa (Fig. 4), although a small Meckel's diverticulum may seem to appear later than the stomach. Although Meckel's diverticulum may appear anywhere within the abdomen, it is most frequently seen in the right lower quadrant. The activity most often mistaken for Meckel's diverticulum is activity in the kidneys, ureter, or bladder, which, however, usually appears after activity is seen in the normal gastric mucosa. Although the procedure can be performed with pharmacologic provocation, studies with pentagastrin, histamine-H2 blockers, or glucagon are rarely performed (57).
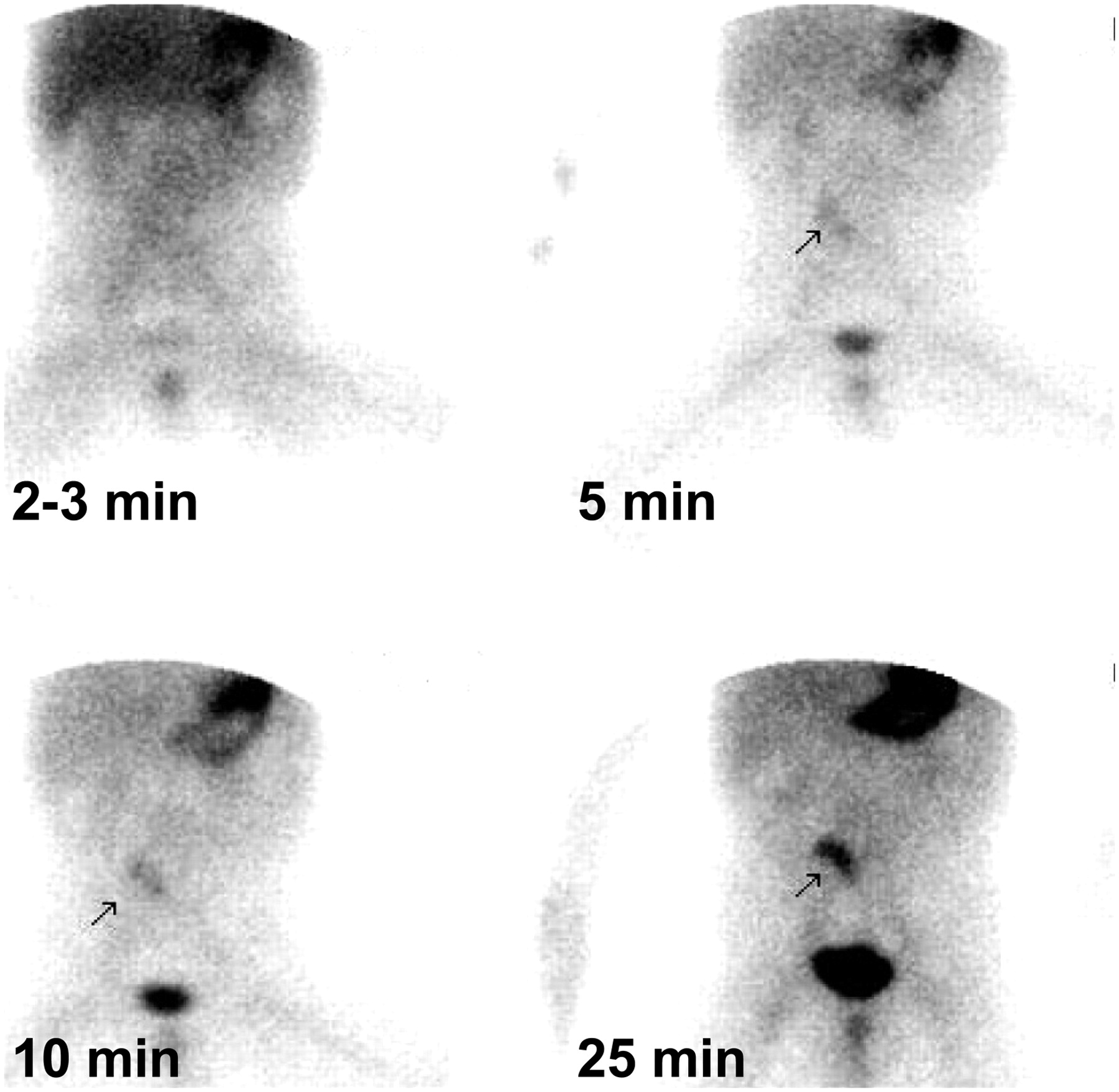
Meckel's diverticulum scintigraphy performed on 2-y-old boy with intermittent bleeding (bright red blood) and no other accompanying symptom. Sequential images obtained after injection of 99mTc-pertechnetate show obvious accumulation of radioactivity in right lower paraumbilical region, consistent with most frequent location of Meckel's diverticulum. Time-course pattern of radioactivity accumulation in possible Meckel's diverticulum mirrors pattern of tracer concentration in gastric region. Diagnosis of Meckel's diverticulum was confirmed at surgery, which was followed by complete disappearance of gastrointestinal bleeding. (Courtesy of Drs. Pham Thi Minh Bao and Le Ngoc Ha, Department of Nuclear Medicine, Tran Hung Dao General Hospital, Hanoi, Vietnam.)
IBD
IBD includes 2 different clinical entities causing inflammation of the intestines: ulcerative colitis and Crohn's disease. Both diseases are chronic but frequently relapse after periods of remission. Circulating leukocytes are recruited at the site of disease through a multistep process: adhesion to microvascular endothelium, transmigration through the vessel wall, and further migration in extravascular tissue and into the bowel lumen (58). This is the pathophysiologic basis for using labeled autologous leukocyte scintigraphy for characterizing activity of the disease.
In fact, the nuclear medicine imaging method initially used for characterizing active IBD is based on autologous radiolabeled leukocytes, either 111In-oxine leukocytes or, more recently, 99mTc-hexamethylpropyleneamine oxime (HMPAO) leukocyte scintigraphy (59–63) (Fig. 5). With both 111In-oxine leukocytes and 99mTc-HMPAO leukocytes, scans in the upright position help to separate hepatic activity from the transverse colon. A pelvic outlet view can be especially helpful in assessing rectal disease, particularly because of bladder activity. SPECT studies (and especially SPECT/CT) at 1.5–2 h after injection of radiolabeled leukocytes are helpful for separating superimposed activity in the bone marrow or in other sites of physiologic accumulation of radioactivity (Fig. 6). In positive scans, abnormal bowel activity is seen early, usually increasing in intensity over the next 2–3 h.

Planar imaging of abdomen performed on patient with active Crohn's disease approximately 45 min after injection of autologous 99mTc-HMPAO–labeled leukocytes. Accumulation of radioactivity is obvious in section of small bowel that can be identified as preterminal ileum.

Planar imaging (A) and SPECT/CT (B) performed on patient with active Crohn's disease approximately 45–90 min after injection of autologous 99mTc-HMPAO–labeled leukocytes. Obvious accumulation of radioactivity in terminal ileum is seen on planar imaging. However, SPECT/CT also demonstrates IBD involvement of preterminal ileum, which was obscured on planar imaging because of superimposition with circulating blood pool and with accumulation in underlying bone marrow. (Courtesy of Dr. Paola A. Erba, Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa, Italy).
A recent metaanalysis of 49 studies published between 1984 and 2004 (totalling nearly 4,400 patients) emphasized the high diagnostic accuracy of either 111In-oxine leukocyte or 99mTc-HMPAO leukocyte scintigraphy in IBD, with sensitivity and specificity around 90% (64). In particular, a negative leukocyte scan virtually rules out diagnosis of this disease. In addition to IBD, a scan can be positive in infectious enteritides, mesenteric ischemia, gastrointestinal bleeding, and colonic cancer. The sensitivity of leukocyte scintigraphy for detecting IBD in untreated patients is high even in the early stages of disease, when radiologic or endoscopic findings are often normal or equivocal. Although leukocyte scintigraphy is generally not considered to be a first-line diagnostic procedure in patients with IBD, it is of value in acutely ill patients with severe diarrhea, in whom an endoscopic study might be contraindicated. An additional specific indication is the early diagnosis of postsurgical recurrences on preanastomotic loops.
Although leukocyte imaging is useful, PET with 18F-FDG is becoming the new standard for nuclear medicine imaging in patients with IBD, based on the localization of this tracer in inflammatory lesions (65,66). The field started with a few occasional observations, whereas more systematic studies have better clarified the value of 18F-FDG PET in patients with IBD (67). In a group of 25 pediatric patients, 18F-FDG PET had 81% sensitivity and 85% specificity for detecting IBD, based on a 4-point scale for 18F-FDG uptake in 5 bowel segments (68). In a more recent report on 55 children with newly diagnosed IBD or symptoms suggestive of recurrent disease, sensitivity of 18F-FDG PET was 80%, and there was no evidence of inflammation in children with recurrent abdominal pain without IBD (69). Even better results have been described by Loffler et al. in pediatric patients (aged 2–6 y), with an average sensitivity of 98% (higher than both endoscopy and abdominal ultrasound) and overall accuracy comparable to the invasive procedure (83% vs. 82%) (70).
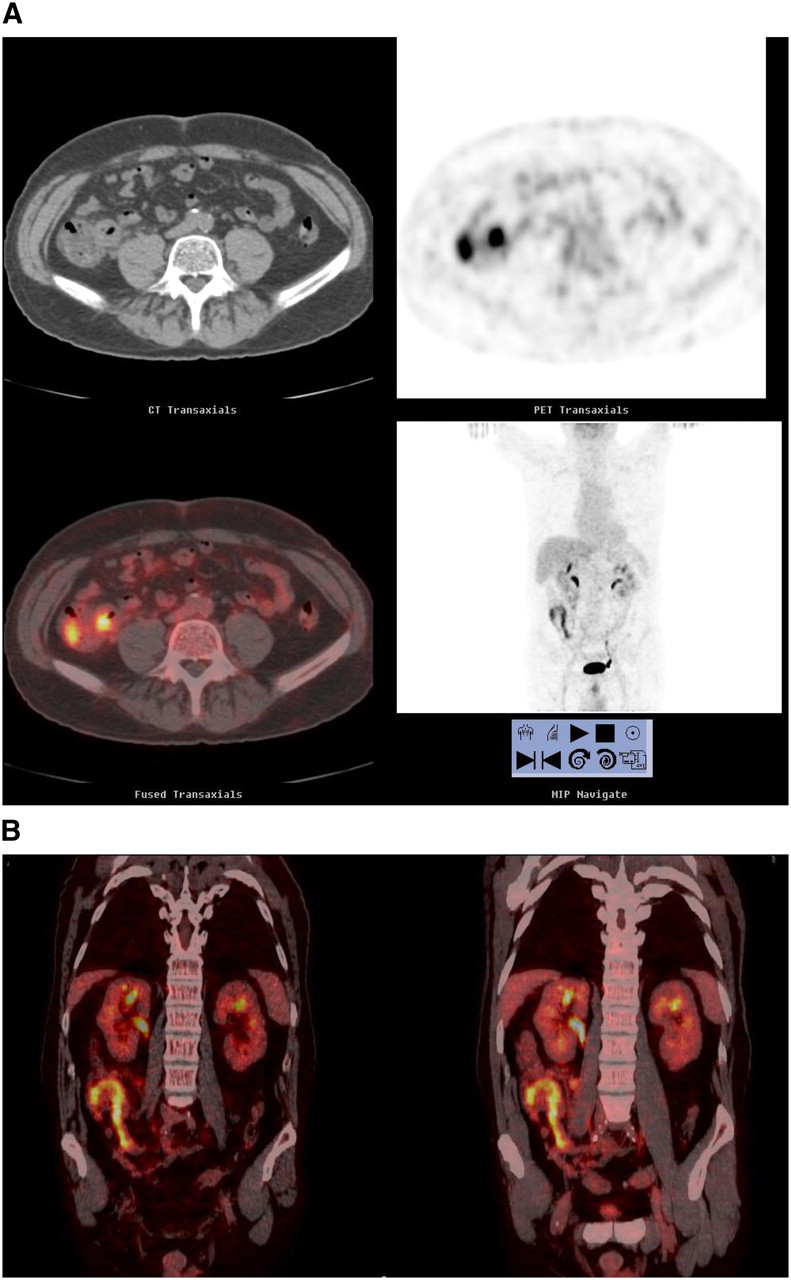
Considering that the diagnostic performance of 18F-FDG PET is excellent and that this technique avoids the cumbersome and time-consuming preparation of radiolabeled autologous leukocytes, 18F-FDG PET may offer a definite clinical advantage for adult patients (71). In this regard, the combination of metabolic imaging (PET) with better anatomic localization (CT) represents a further advance for increased specificity (Fig. 7). Louis et al. have recently demonstrated the high prognostic value of 18F-FDG PET/CT in a group of adult patients with IBD (72). In particular, in addition to visual analysis (with 100% sensitivity for detecting severe endoscopic lesions), they developed a global PET/CT score based on the maximum standardized uptake value. Median maximum standardized uptake values of the affected segments were in the 4–6 range but reached levels as high as 12–14. This score significantly correlated with the endoscopic index of severity of Crohn's disease, with a global index of severity of disease, and with the C-reactive protein serum levels. Finally, logistic regression analysis showed that the index of metabolic activity (ratio of standardized uptake value in the affected segment to standardized uptake value in the liver) was significantly associated with the presence of severe endoscopic lesions, in contrast to wall thickening alone (a classic CT-based marker).
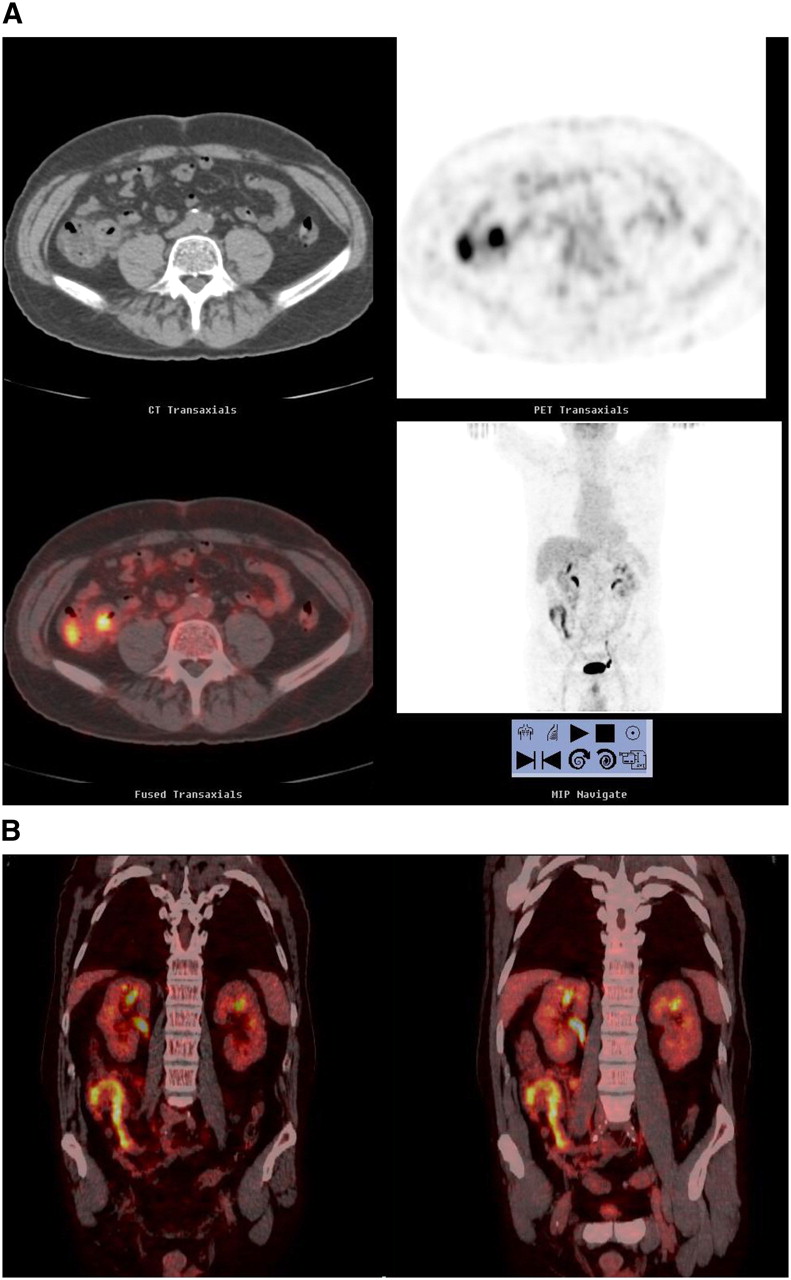
18F-FDG PET/CT performed on patient with active Crohn's disease. Both transaxial sections (A) and coronal sections (B) show focally increased tracer uptake in region easily identified on CT images as section of small bowel (with increased thickness of intestinal wall), clearly distinct from tracer accumulation in urinary excretory routes. Standardized uptake value of small-bowel segment with highest radioactivity accumulation was 10.4 in this patient. (Courtesy of Dr. Paola A. Erba, Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa, Italy.)
Scintigraphic Defecography
Disorders of evacuation account for a significant proportion of people seeking medical attention for constipation and for a large percentage of those who fail to respond to colectomy with ileorectal anastomosis; indeed, a considerable proportion of patients with severe constipation actually have dyschezia (73).
Dynamic scintigraphic defecography can quantitatively evaluate emptying efficiency in patients with disordered evacuation. This technique involves considerably less radiation than x-ray proctography (gonadal dose approximately 7% of the dose of the corresponding radiologic examination) (74). Artificial stool (rehydrated potato labeled with 99mTc-pertechnetate or methyl-cellulose paste labeled with 99mTc-ethylene diphosphonate, 180–200 MBq in either case) is instilled into the rectum up to a volume causing impending evacuation (75). Preevacuation images are recorded with the patient sitting on a commode, the γ-camera head against the left, right, and posterior pelvis (1 min per view). A postevacuation scan is then recorded in the same positions and the evacuated fraction calculated using fixed regions of interest from the pre- and postevacuation scans.
In a group of patients with ulcerative colitis who underwent ileal pouch–anus anastomosis, this semiquantitative parameter correlated well with excreted stool volumes, and anatomic detail was satisfactory (74). A tracer-filled balloon has also been used to quantitate anorectal and pouch–anus angle during squeezing and straining (75). In a study using an enema of labeled potato mash to assess pelvic floor movement, alteration in the anorectal angle, and expulsion time, 5 of 12 patients with longstanding constipation exhibited prolonged expulsion times (76). In a larger series including patients with either obstructed defecation or slow transit, incomplete rectal emptying was observed in patients with obstructed defecation (77). Wald et al. compared scintigraphic defecography with both anorectal manometry and colonic transit using radioopaque markers in 20 healthy controls and in 38 adult patients with chronic constipation. Although the correlation with the findings for colonic transit and anorectal manometry was poor, over half the patients had abnormal findings on radionuclide defecography (78).
By administering a radiolabeled meal in divided doses over 6 h and imaging defecation 24 and 48 h later, Lubowsky et al. demonstrated that during defecation significant emptying of the left colon commonly occurs, and even of the right colon (79).
Selvaggi et al. used scintigraphic defecography to evaluate the efficiency of defecation in 16 patients with severe ulcerative colitis bearing an ileal pouch (80). The patients were classified into 2 groups according to the presence of good (group A) or poor (group B) pouch function, percentage emptying being higher in group A than in group B (81% ± 9% vs. 71% ± 9%, P < 0.05), although the mean maximum tolerated volume was similar in the 2 groups.
In patients with an ileal pouch performed for ulcerative colitis, an increased frequency of defecation without any evidence of pouch dysfunction may be correlated with an alteration of emptying efficiency. Scintigraphic defecography is appropriate for investigating this condition with no relevant discomfort for the patients.
CONCLUSION
Although most studies of the gastrointestinal tract deal with the esophagus and stomach, transit studies can also be used for the lower gastrointestinal tract. Similarly, studies of small- and large-bowel inflammatory disease, detection of Meckel's diverticula, and identification of lower gastrointestinal bleeding are valuable in the appropriate clinical setting. In some countries, several practical and regulatory issues have retarded the growth and more widespread use of radionuclide procedures for evaluating patients with disorders of the lower gastrointestinal tract. Most notably in the United States, intestinal transit scintigraphy (including scintigraphic defecography) and 18F-FDG PET for imaging IBD are not reimbursed, and 99mTc-sulfur colloid is the only agent approved for oral administration. As the population ages, it is likely that the demand for lower gastrointestinal transit studies will increase, and longer-lived radiopharmaceuticals, such as 111In-charcoal, for the performance of this study will be approved. Similarly, 18F-FDG PET studies of inflammation, although still in their infancy, require wider validation in large-scale, specifically designed clinical trials.
Acknowledgments
We thank Dr. Marco Anselmino (Fourth Division of General Surgery, Regional Center for Diseases of the Esophagus, “S. Chiara” University Hospital, Pisa, Italy) for helpful discussions in the preparatory phase of the manuscript. Thanks are also due to Drs. Fiammetta Pesella and Alice Lorenzoni (residents in nuclear medicine at the University of Pisa Medical School, Pisa, Italy) for their contribution to various sections on radionuclide procedures. We also acknowledge the contribution of Dr. Cristina Stasi (Gastroenterology Unit, Department of Internal Medicine, the University of Pisa Medical School, Pisa, Italy) to the section on clinical manifestations of the lower gastrointestinal tract.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH MAY 2009.
-
No potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.
- 61.
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- Received for publication August 24, 2007.
- Accepted for publication December 7, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The SNMMI Procedure Standard/ACNM Practice Guideline for Gastrointestinal Bleeding Scintigraphy 3.0
- Advancing human gut microbiota research by considering gut transit time
- The SNMMI Procedure Standard/EANM Practice Guideline for Gastrointestinal Bleeding Scintigraphy 2.0
- The SNMMI and EANM Practice Guideline for Small-Bowel and Colon Transit 1.0
- 13-Year-Old Boy with a 3-Day History of Melena