


Abstract
99mTc-Labeled white cell scintigraphy (WCS) has been used for the investigation of inflammatory bowel disease (IBD) in adults, but data on children are limited. The most common agent used is 99m Tc-hexamethylpropyleneamine oxime (HMPAO); however, this agent has limitations. In a retrospective study, we assessed the use of 99mTc-stannous colloid WCS for the initial evaluation of children with suspected IBD. Methods: Diagnostic, endoscopic, and contrast radiography results were retrospectively collected from the medical records. Two experienced nuclear physicians unaware of the patient data interpreted the WCS results, with agreement reached by consensus. Statistical analysis was performed on the ability of WCS to detect active disease and localize it topographically and on a comparison of diagnostic methods, using a combination of clinical features and endoscopy as the reference standard. Results: Between 1996 and 1999, 64 patients (35 male and 29 female; mean age, 12.5 y; age range, 2–19 y) had WCS performed, with IBD subsequently diagnosed in 34 patients. 99mTc-Stannous colloid WCS had an 88% sensitivity, 90% specificity, and 8.8 likelihood ratio for initial investigation of IBD. Agreement was poor for topographic localization of disease. Small-bowel series had a 75% sensitivity, 50% specificity, and 1.5 likelihood ratio for detecting endoscopic disease of the terminal ileum and proximal colon. Conclusion: Our results confirm that WCS is a useful imaging technique for the initial evaluation of patients with suspected IBD. 99mTc-Stannous colloid had results at least comparable to those of other WCS agents, and in children, 99mTc-stannous colloid WCS should be preferred in view of lower cost, shorter preparation time, and the smaller blood volumes required.
Inflammatory bowel disease (IBD) is increasingly diagnosed in the pediatric population. In Western Europe and North America, ulcerative colitis and Crohn’s disease are the major causes of chronic intestinal inflammation and are prominent causes of chronic illness in both adults and children. The final diagnosis may be made only after extensive investigations based on clinical, radiologic, endoscopic, and histologic features (1,2).
99mTc-Labeled leukocyte scanning is a relatively noninvasive nuclear medicine procedure. It is useful as an initial investigation for IBD because of its high sensitivity and high specificity and the relative ease of the study (3–6). The most common agent used is 99mTc-hexamethylpropyleneamine oxime (HMPAO); however, the preparation of labeled white blood cells using this agent is both time consuming and expensive (3,4,6). In 1984, Hanna et al. (7) revived interest in the labeling of phagocytic white blood cells with 99mTc-stannous colloid and reported clinical applications using this technique (8).
We therefore undertook a retrospective study to assess the value of 99mTc-stannous colloid white cell scintigraphy (WCS) in detecting disease activity and localizing disease topographically and to compare diagnostic methods in children with suspected IBD.
MATERIALS AND METHODS
Patients
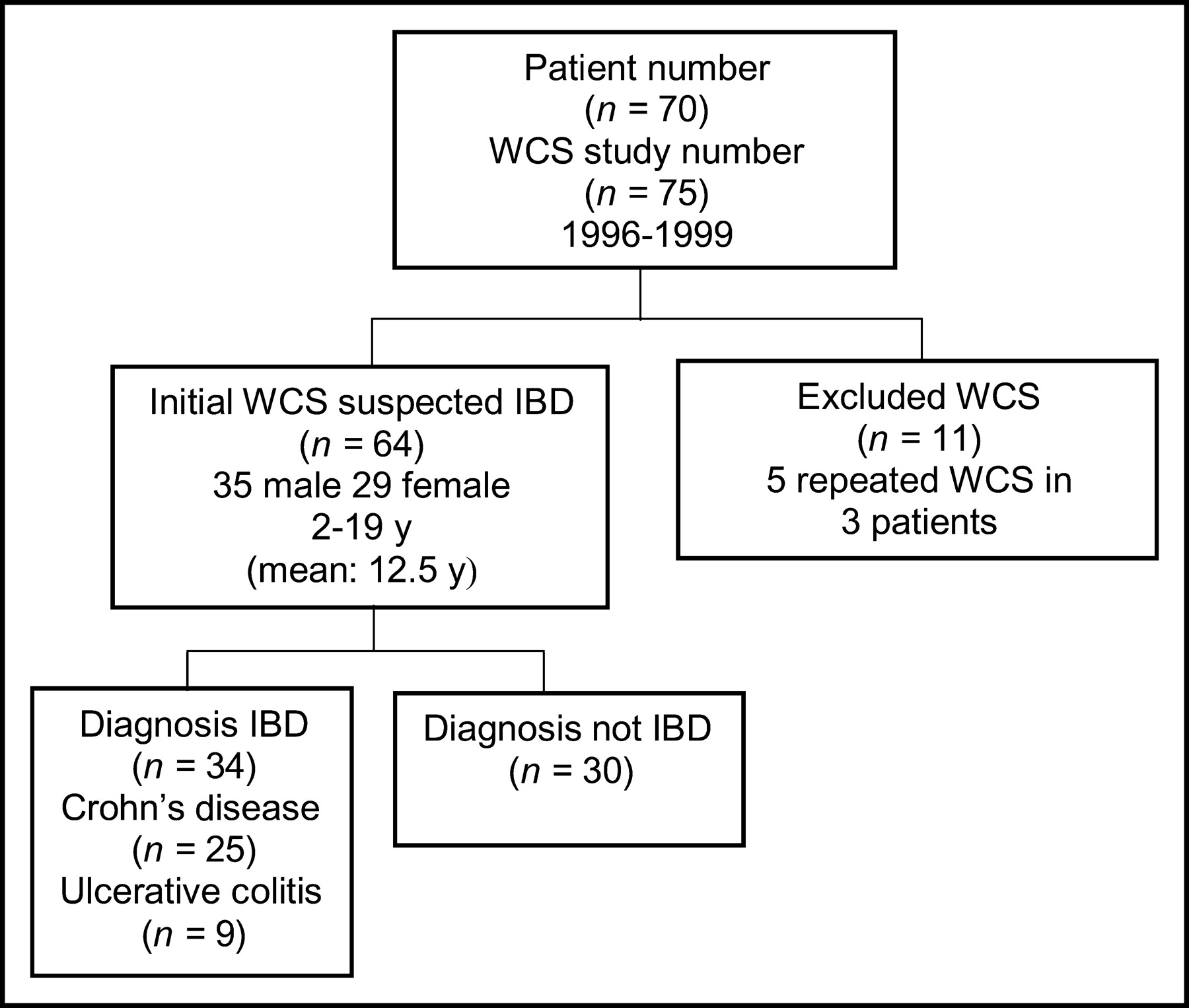
During the period 1996–1999 at The Children’s Hospital at Westmead, Australia, 75 WCS examinations were performed on 70 patients clinically suspected of having active IBD (Fig. 1). Eleven WCS examinations were excluded because they were performed on 6 patients previously diagnosed with IBD and, as such, did not represent an initial investigation. All patients either were symptomatic with what was considered to be clinically active disease, including abdominal pain or diarrhea or blood in the stools, often accompanied by weight loss, or had suspected extraintestinal manifestations of IBD.
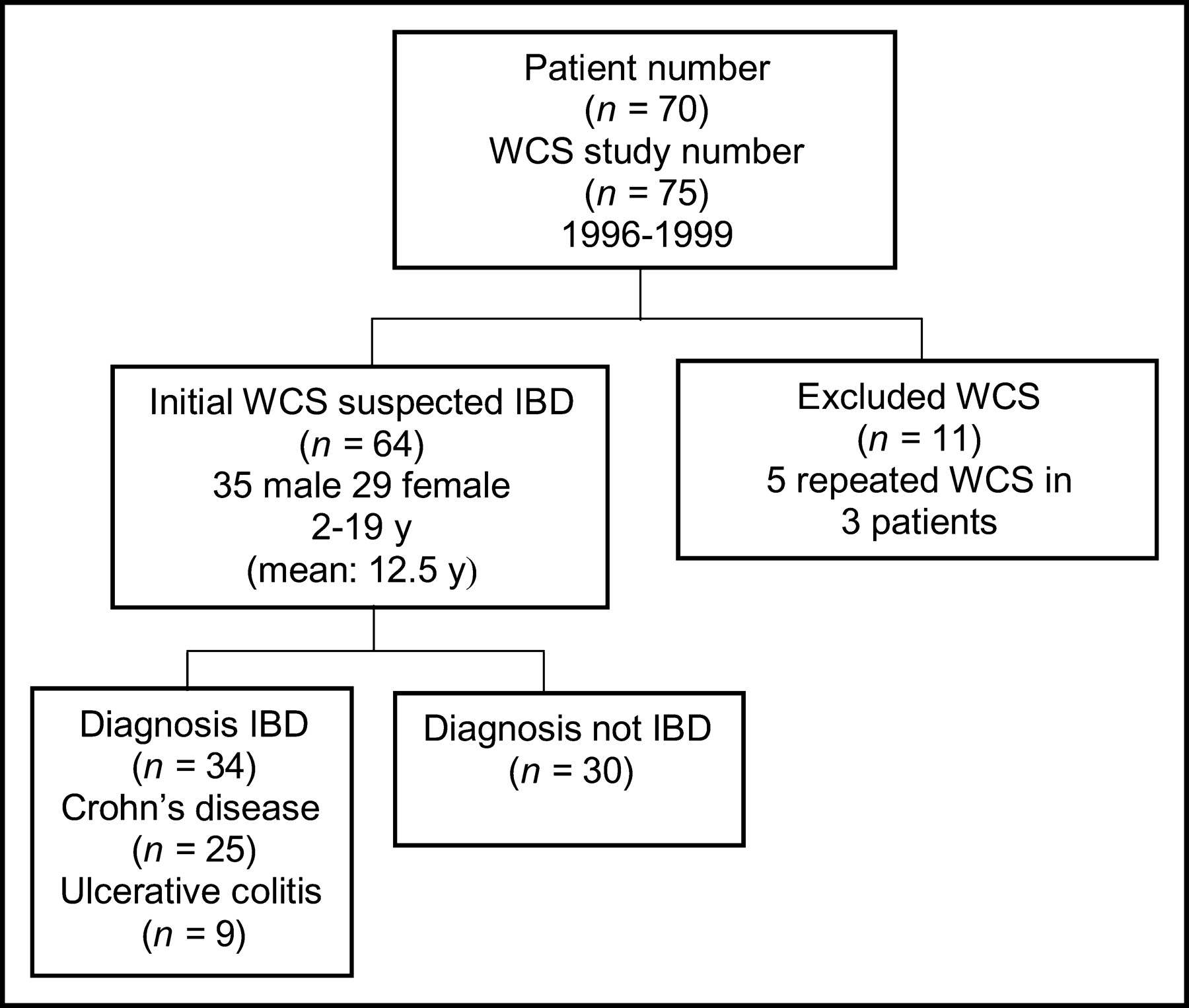
Flow diagram of study population.
Approval was obtained from the Ethics Committee at our institution before data collection began. Subjects were identified from clinical records and the WCS records maintained in the Department of Nuclear Medicine. The medical record and operative reports for each patient were reviewed. Two experienced nuclear physicians, unaware of the diagnosis, endoscopy results, or contrast radiography results, interpreted the WCS results, with agreement reached by consensus.
Labeling Technique
The technique for labeling white blood cells using 99mTc-stannous colloid has previously been described (7) and is summarized here. White blood cell kits were made in house and stored frozen. A vial containing 6.25 mg of sodium fluoride (vial A) was dissolved in 4 mL of water for injection. Four milliliters were withdrawn, added to the vial containing 0.644 mg of stannous fluoride (vial B), and mixed. Two milliliters of vial B were withdrawn into a 2.5-mL syringe, and 0.5 mL of this solution was passed through a 0.22-mm filter into a syringe containing between 1.5 and 2 GBq of 99mTc-pertechnetate in a 5-mL syringe and made up to 2.5 mL with normal saline. The mixture was spun for 60 min by gentle rotation. From 5 to 9 mL of blood were collected from the patient using a 20-mL syringe containing 4.5 mL of heparin saline. Then, 0.8 mL of 99mTc-colloid was transferred into the syringe containing blood and heparin. The blood containing the 99mTc-colloid solution was spun for 60 min by gentle rotation. The suspension was centrifuged at 400g (approximately 2,000 rpm) for 5–10 min, the plasma was removed, and the blood was reinjected intravenously.
Imaging
Planar imaging was performed at 1 h, and planar and SPECT imaging at 3 h, after the injection of radiolabeled leukocytes. A large-field-of-view γ-camera fitted with a low-energy, high-resolution collimator was used.
Endoscopy
The bowel was prepared before colonoscopy using one of several regimes, depending on the individual performing the endoscopy. Biopsies were taken, fixed in formalin, embedded in paraffin, stained with hematoxylin and eosin, and examined by a member of the Department of Pathology.
Contrast Radiography
Barium was ingested orally or through a nasogastric tube. Supine abdominal radiographs were taken, and additional images of suspected areas were acquired with compression if necessary. Evidence of IBD included thick mucosal folds, ulceration, fissuring, stenosis or dilatation, hypomotility of intestinal loops, and abnormal peristalsis. Data from contrast radiography performed within 4 wk of WCS were collected.
Statistical Analysis
Data were stored in a protected database. Diagnostic, endoscopic, and barium radiography data were combined with WCS results at the completion of interpretation of WCS. Data were analyzed using Statistical Package for Social Sciences (version 9; Microsoft). Because no single gold standard for IBD diagnosis exists, the reference standard for IBD was a combination of clinical features and, if endoscopy was performed, endoscopic results. Sensitivity and specificity, including 95% confidence interval (CI), and likelihood ratio were calculated for WCS for the diagnosis of IBD and for contrast radiography in patients with visualization of the terminal ileum. Percentage agreement for topographic localization of IBD sites on WCS was calculated for patients who underwent complete colonoscopy.
RESULTS
In 64 patients between 1996 and 1999, 64 WCS studies were performed as part of an initial assessment of suspected IBD (Fig. 1). There were 35 male and 29 female patients, with a mean age of 12.5 y and an age range of 2–19 y. Eleven WCS studies were excluded from statistical analysis, as these were not performed as an initial investigation. Eighty-three percent (53/64) of WCS referrals were made after consultation with a pediatric gastroenterologist at our institution.
Diagnosis of Active Disease
99mTc-Stannous colloid WCS had an 88% sensitivity (95% CI, 77%–99%), 90% specificity (95% CI, 79%–100%), and 8.8 likelihood ratio for the diagnosis of active IBD (Table 1; Fig. 2). One patient underwent 2 WCS examinations. The results of the first examination were negative and showed no evidence of active IBD, but the second examination, performed when the patient had had clinically proven IBD for 2 y, was positive for IBD (9). The second WCS examination was excluded from our statistical analysis and would not have significantly affected our results. In the remaining 29 patients whose WCS findings were negative for IBD, IBD has not developed to date. Two of the 4 patients with false-negative WCS findings were receiving corticosteroids; excluding these 2 patients increases the sensitivity to 94%.
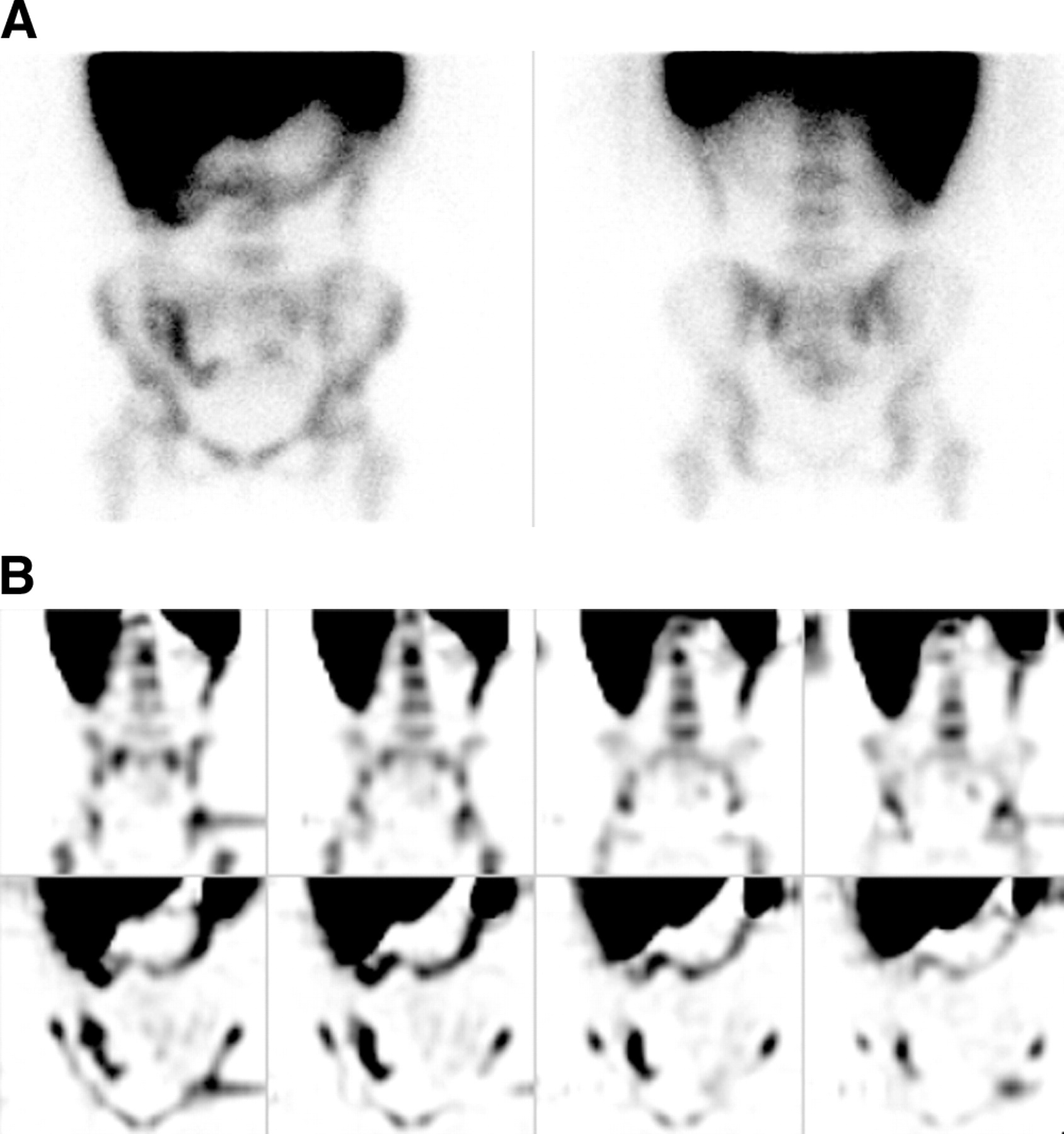
An 8-y-old girl with Crohn’s disease. (A) Anterior (left) and posterior (right) 3-h planar images. Marked uptake of tracer is present in the distal ileum and in the ascending, transverse, and descending colon. Note the high degree of hepatic uptake, which impairs detection of upper gastrointestinal disease. There is no bladder activity. (B) Coronal 3-h SPECT images. Coronal SPECT more clearly delineates the distal ileal disease.
Cross Table of WCS and IBD for All Patients and Endoscopy Patients
Considering only the 45 patients who underwent endoscopy and biopsy, WCS had an 87% sensitivity (95% CI, 75%–99%), 87% specificity (95% CI, 70%–100%), and 6.7 likelihood ratio for the diagnosis of active IBD, with diagnosis based on both clinical features and histologic evidence (Table 1; data in italic type). Endoscopy was delayed in 4 IBD patients because of the severity of the clinical course, including toxic megacolon in 1 patient.
Topographic Localization of Disease by WCS
Forty-five patients underwent colonoscopy. A complete colonoscopy to the terminal ileum was performed on 18 patients. The reasons for the limited study included severe inflammation impeding further instrumentation, and technical limitations such as incomplete bowel preparation. Upper gastrointestinal endoscopy was performed on 26 patients.
The number of sites of uptake on WCS was compared with the number of disease sites found on endoscopy, for those patients with clinical features of IBD who had complete colonoscopy to the terminal ileum. WCS showed the same number of sites of involvement in 21.4%, fewer sites of involvement in 64.3%, and more sites of involvement in 14.3%. WCS was unable to show upper gastrointestinal disease in any patients with endoscopic and clinical evidence of upper gastrointestinal disease.
Comparison of Diagnostic Methods
Nineteen small-bowel series were performed, and only 6 of these included endoscopic visualization up to the terminal ileum. Small-bowel series had a 75% sensitivity (95% CI, 32%–100%), 50% specificity (95% CI, 0%–100%), and 1.5 likelihood ratio for detecting disease of the terminal ileum or proximal colon. Detection of disease at these sites by WCS had a 75% sensitivity (95% CI, 50%–100%), 67% specificity (95% CI, 29%–100%), and 2.3 likelihood ratio (Table 2; Fig. 3).
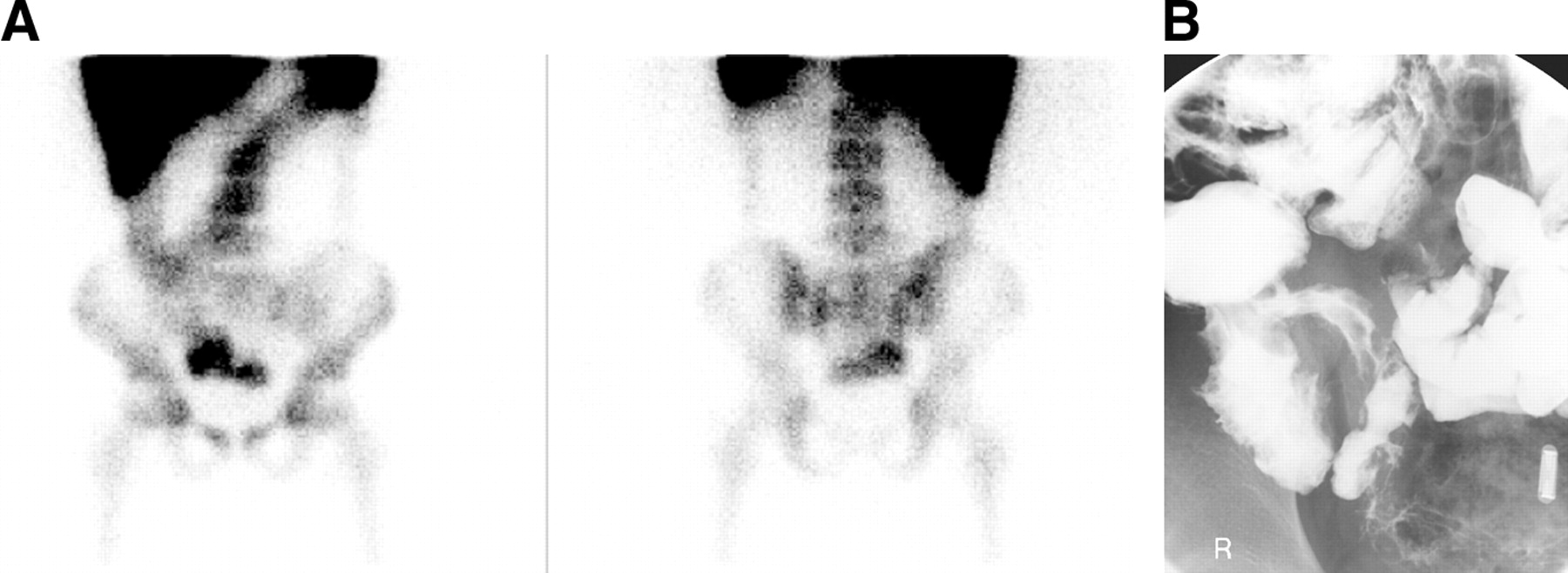
A 13-y-old boy with Crohn’s disease. (A) Anterior (left) and posterior (right) 3-h planar images. Marked uptake of tracer is present throughout the colon, particularly in the distal ileum. (B) Small-bowel series of the terminal ileum. Abnormal separation of bowel loops is seen in the right iliac fossa, with bowel wall thickening. Normal mucosal pattern and terminal ileum peristalsis are present.
Cross Table for Detection of Terminal Ileum/Proximal Colon IBD by Small-Bowel Series and WCS in Complete-Colonoscopy Patients
DISCUSSION
IBD is an increasingly important cause of chronic gastrointestinal disease in children and adolescents. Diagnostic methods with high sensitivity and specificity are required so that the diagnosis can be made rapidly and the extent of disease determined (1,2). The clinical indices do not provide data on disease site or extent and have a significant subjective component. Biochemical and hematologic parameters are not specific. Fluoroscopic radiographic methods will show indirect evidence of inflammation but entail considerable radiation exposure and are uncomfortable for the patient. Barium radiographic studies are also often difficult to interpret because of overlapping loops of small bowel. Endoscopic methods in children usually require general anesthesia or heavy sedation and involve discomfort and some risks from the instrumentation. Endoscopy cannot always adequately examine the entire bowel, particularly the small bowel, and in about two thirds of colonoscopic biopsies may not identify the definitive diagnostic features of ulcerative colitis or Crohn’s disease (1,2).
In view of these diagnostic difficulties and the limitations of other nuclear medicine agents, this retrospective study was undertaken to evaluate the role of WCS using the 99mTc-stannous colloid phagocytic technique for the initial investigation of suspected IBD.
The first described use of radiolabeled white cells in adults applied 111In-labeled cells (10); later, Scholmerich et al. described using 99mTc-HMPAO (11). 111In-Labeled leukocyte scanning creates high radiation exposure, and its long duration makes it a relatively poor technique, particularly for children (10,12). 99mTc-HMPAO WCS has been used successfully for a wide variety of inflammatory diseases and has been shown to be useful in imaging children with IBD (4,6,13–15). Charron et al., in a study comparing 99mTc-HMPAO WCS and endoscopy for the diagnosis of IBD in 215 children, found excellent results for 99mTc HMPAO WCS: 90% sensitivity, 97% specificity, and 93% accuracy (16).
In our study, the ratio of patients with Crohn’s disease to patients with ulcerative colitis was approximately 2.8:1, which correlates well with the ratio typically seen in pediatric practice (17). 99mTc-Stannous colloid WCS had a high sensitivity and high specificity for detecting active IBD (Table 1). To date, IBD has not developed in the 3 patients with false-positive WCS results. In 1 patient, infectious colitis was subsequently confirmed. Recurrent abdominal pain syndrome was diagnosed in the remaining 2 patients. For 1 of these patients, the WCS report described only “minor” changes in the right colon. This finding has previously been recognized as false positive on 99mTc-HMPAO WCS (18). Four patients in our series with IBD had negative WCS findings. In 2 of the 4 patients, these false-negative results were most likely due to concurrent treatment with corticosteroids. Similar false-negative results in patients taking corticosteroids have been reported (14). Corticosteroids inhibit chemotaxis, which is an important component of the mechanism of phagocytosis and is the physiologic basis of the labeling technique (7,19).
Negative WCS findings may, however, also indicate a good response to treatment. A study of adults concluded that assessment of treatment response is an important indication for performing WCS (20). Our study did not specifically examine this issue. Detailed prospective studies to determine the usefulness of WCS as a tool to assess treatment response in children are required.
In our study, 99mTc-stannous colloid WCS showed poor agreement with endoscopy for topographic localization of disease. Cucchiara et al., using 99mTc-HMPAO–labeled cells, reported a significant correlation between scintigraphy and diagnosis; however, they also reported a poor correlation with the number of involved segments (15). The poor agreement may in part represent technical difficulties in the reporting of exact sites of involvement on endoscopy reports and WCS staging but may also represent a limitation of WCS.
One of the main advantages of WCS scanning over other imaging procedures is the ability to evaluate concomitantly both the small and the large bowel. A recent publication suggested that small-bowel disease may be underestimated with WCS because of uptake in bone marrow and the transverse colon (19). However, SPECT, which supplements our technique (Fig. 2), has been found useful in differentiating small-bowel disease from large-bowel disease, in differentiating small-bowel disease from skeletal activity, and in better detailing pelvic activity (5,6,21,22).
99mTc-HMPAO WCS has been shown to be superior to radiology in the assessment of the extent and activity of IBD in both adults and children (4,22,23). In our study, 99mTc-stannous colloid WCS was at least as sensitive as contrast radiography for detection of disease in the terminal ileum or proximal colon (Fig. 3); however, the number of contrast studies performed in our series was small (Table 2). The contrast radiography results may represent chance and are almost certainly affected by selection bias. In view of the accompanying significant radiation exposure and invasiveness of contrast radiography, we do not routinely perform it in the initial evaluation of IBD. We recommended contrast radiography in complicated cases of IBD primarily to exclude anatomic complications such as obstruction, strictures, or fistulae (4).
The main benefits of using 99mTc-stannous colloid WCS, compared with using 99mTc HMPAO, are the lower cost, greater ease of preparation, shorter time for cell preparation, higher and more stable labeling efficiency, and, important in pediatrics, smaller blood volume required (7).
Another potential disadvantage of 99mTc-HMPAO–labeled leukocytes for the detection of abdominal inflammation is nonspecific bowel activity after 3 h, originating from biliary excretion of secondary hydrophilic complexes. These complexes are also excreted in the urine, resulting in bladder activity, which may obscure pelvic disease (5,6). These complexes have not been reported with 99mTc-stannous colloid.
The average labeling efficiency is lower for 99mTc-HMPAO, with reports varying from 56% to 76% (6,14,15). The stannous colloid method in our study had an average labeling efficiency of 96%. A labeling efficiency of greater than 80% for stannous colloid has previously been reported (7,24). As a result, reduced urinary and bladder activity from improved labeling, combined with SPECT imaging, further improves visualization of pelvic structures such as the rectum.
The limitations of our study should be recognized. The lack of a single gold standard for IBD diagnosis makes comparisons difficult. We used a combination reference standard of clinical course and, if endoscopy was performed, endoscopic and histologic evidence. The subjectiveness of clinical features may affect our results, because not all patients underwent endoscopy. However, a similar high sensitivity and specificity were found in patients who underwent endoscopy (Table 1; data in italic type).
Our study was a retrospective analysis of patients presenting to a tertiary referral center. Fifty-three of the 64 patients (83%) were referred for WCS after consultation with a pediatric gastroenterologist and thus represent a “select” sample. The performance of WCS may be considerably different if patients are studied from a broader referral base. Our current clinical practice of using contrast radiography only in suspected complicated cases resulted in small patient numbers and may have furthered the selection bias.
WCS has its own limitations. It is not useful in defining anatomic details such as strictures or fistulas, has difficulty detecting upper gastrointestinal inflammation because of uptake in the liver (Figs. 2 and 3), may show poor agreement with endoscopy for topographic localization of active IBD, and does not provide a histologic diagnosis.
CONCLUSION
99mTc-Stannous colloid WCS is a useful, noninvasive initial study for detecting disease in symptomatic patients and has significant technical advantages over 99mTc-HMPAO. The results for 99mTc-stannous colloid are at least comparable to those for other WCS agents, and 99mTc-stannous colloid WCS should be preferred in children in view of the lower cost, shorter preparation time, and smaller blood volumes required. Compared with other imaging modalities, such as contrast radiography and endoscopy, it is less invasive, at least as accurate, and more economical. Should 99mTc-stannous colloid WCS be routinely used early in the stepwise diagnostic approach to children with suspected IBD? Further prospective studies on children are needed to answer this question and may define the role of 99mTc-stannous colloid WCS in assessing treatment response.
Footnotes
Received Aug. 19, 2003; revision accepted Oct. 23, 2003.
For correspondence or reprints contact: Robert Howman-Giles, Department of Nuclear Medicine, The Children’ s Hospital at Westmead, Locked Bag 4001, Westmead, NSW, 2145, Australia.
E-mail: rhowmang{at}mail.usyd.edu.au
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.