


Article Figures & Data
Figures
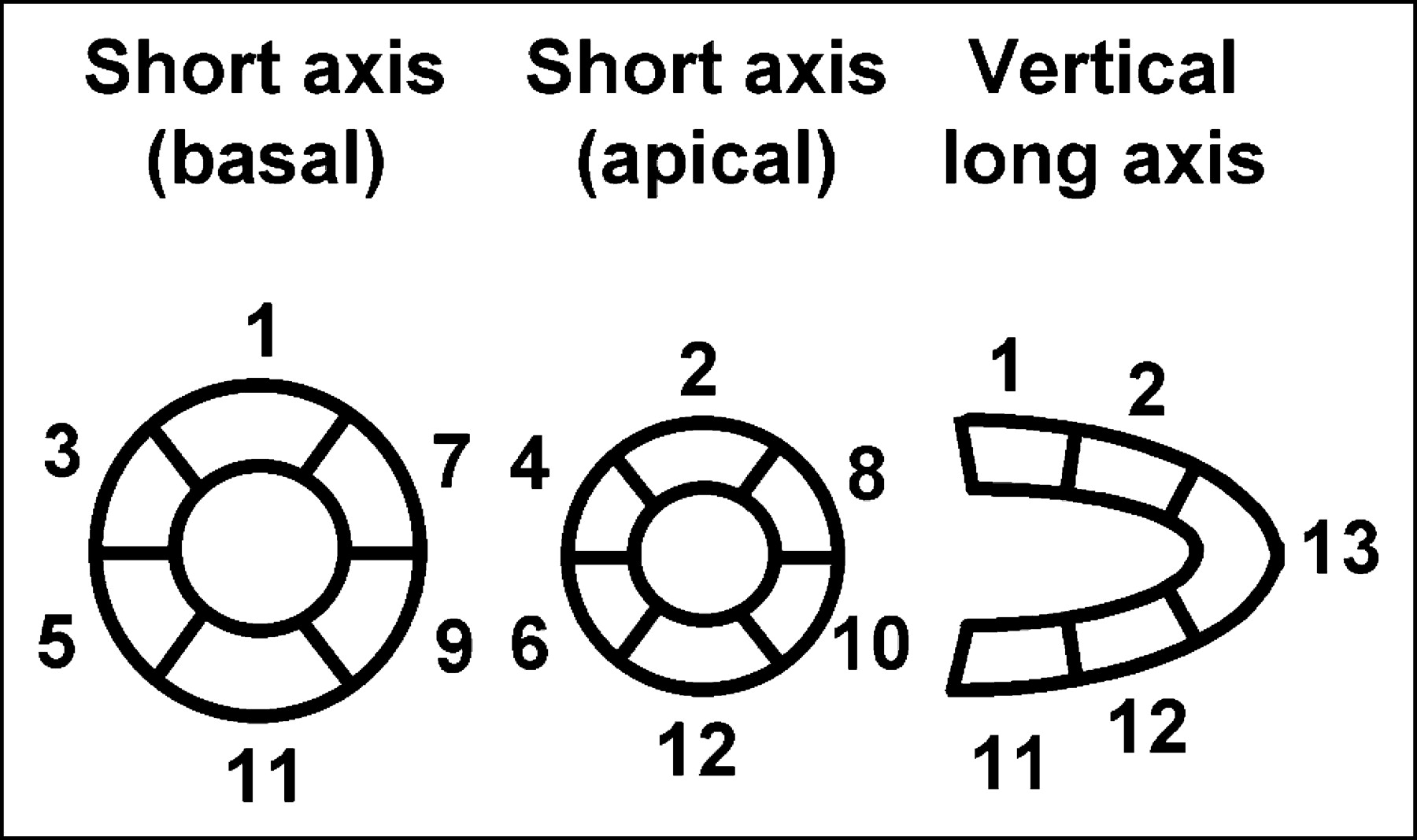
- FIGURE 1.
Short-axis and vertical long-axis slices of myocardial PET and SPECT images were divided into 13 segments.
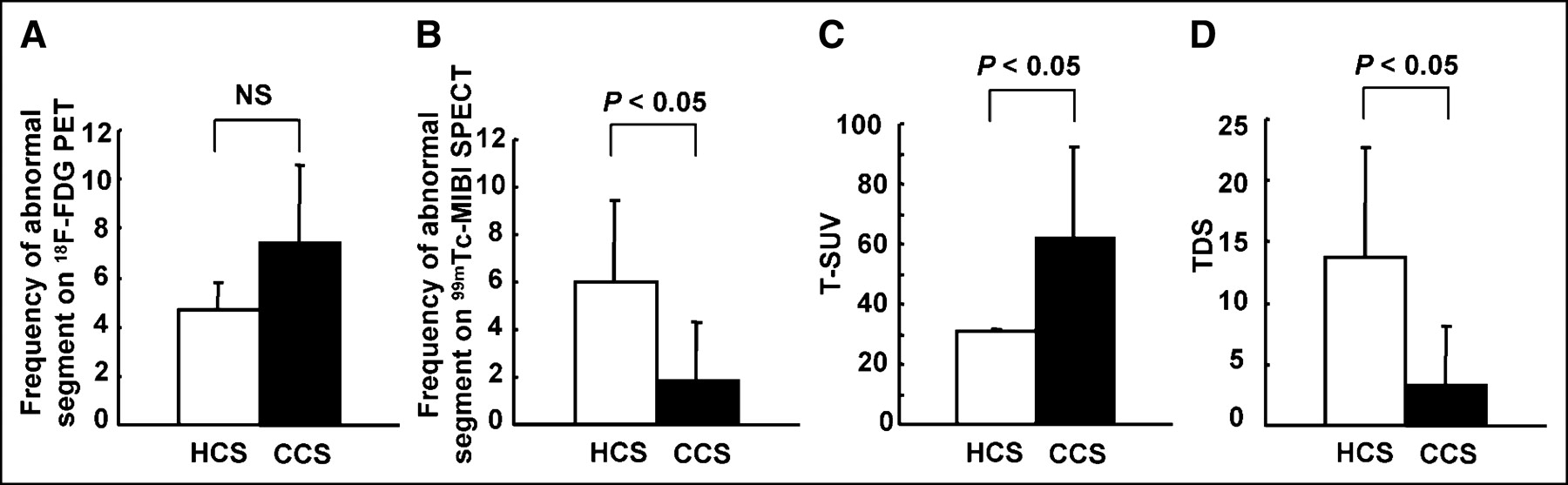
- FIGURE 2.
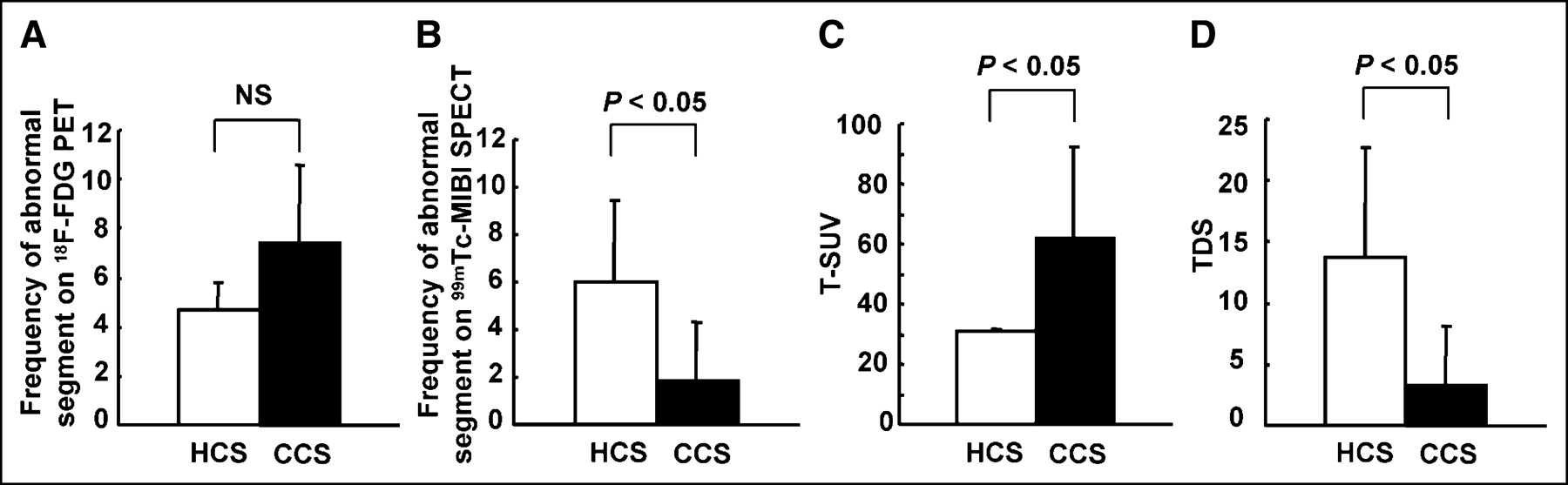
Comparison of nuclear measurements between histologically diagnosed cardiac sarcoidosis (HCS) and clinically diagnosed cardiac sarcoidosis (CCS). Frequency of abnormal segments on 99mTc-MIBI SPECT and TDS in HCS (white bar) was significantly higher than that in CCS (black bar) (B and D). In contrast, frequency of abnormal segments on fasting 18F-FDG PET and T-SUV in HCS were lower than those in CCS, although significant difference could be observed only for T-SUV (A and C). NS = not significant.
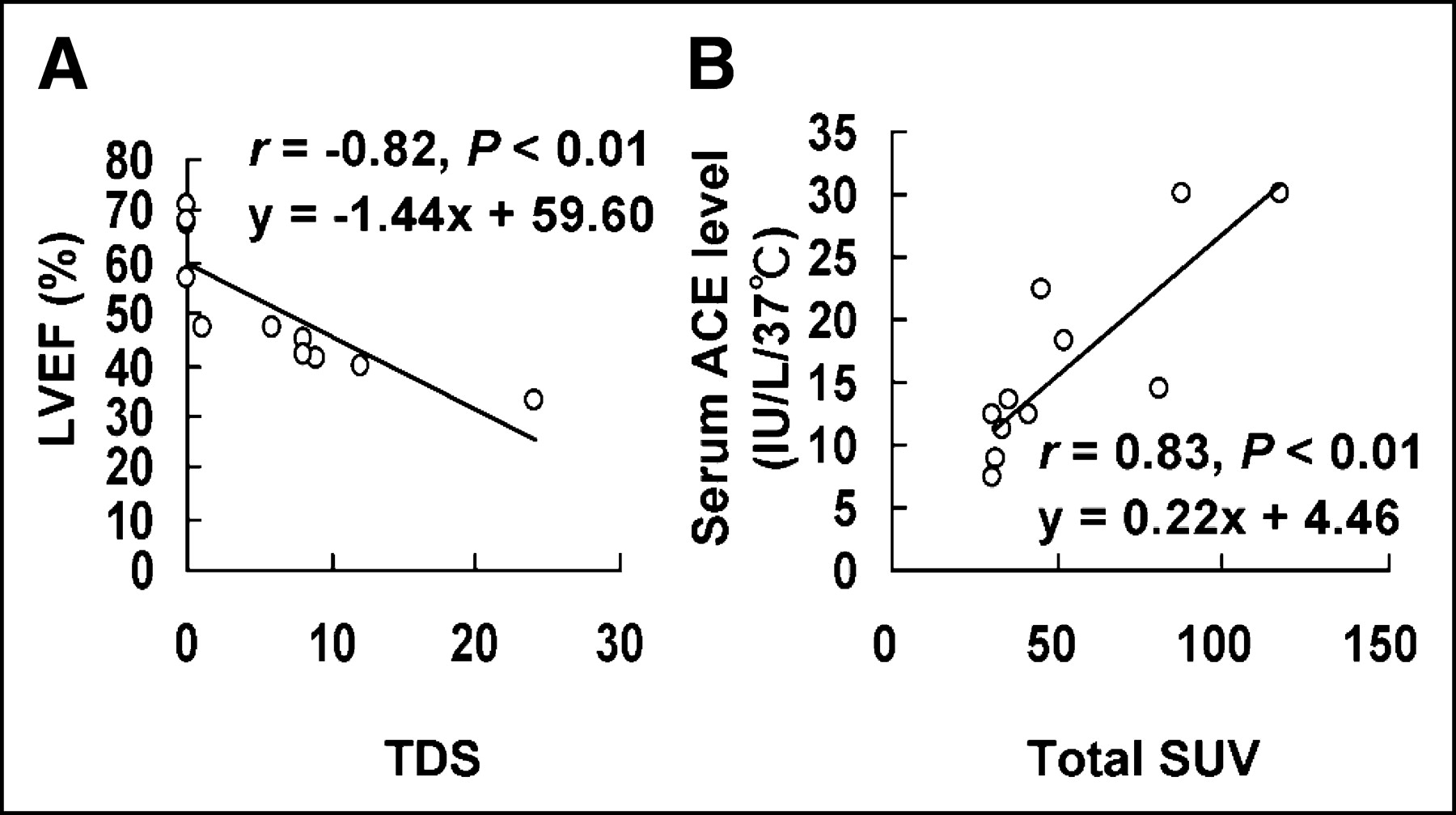
- FIGURE 3.
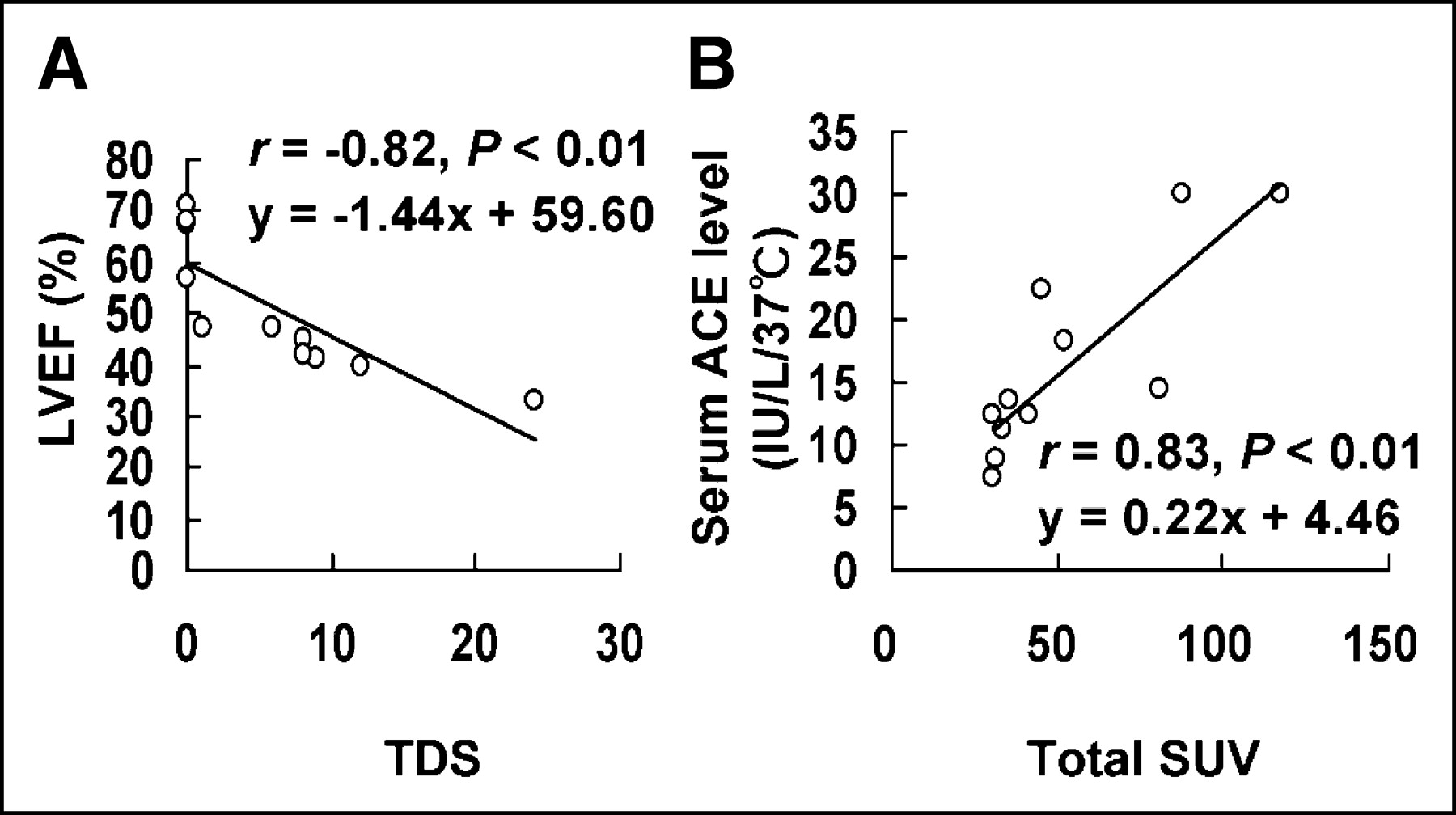
Relationship between nuclear measurements (T-SUV and TDS) and clinical data (LVEF and serum ACE level) in patients with cardiac sarcoidosis (group A). Statistically significant correlations were observed between TDS and LVEF (A) and between T-SUV and serum ACE level (B).
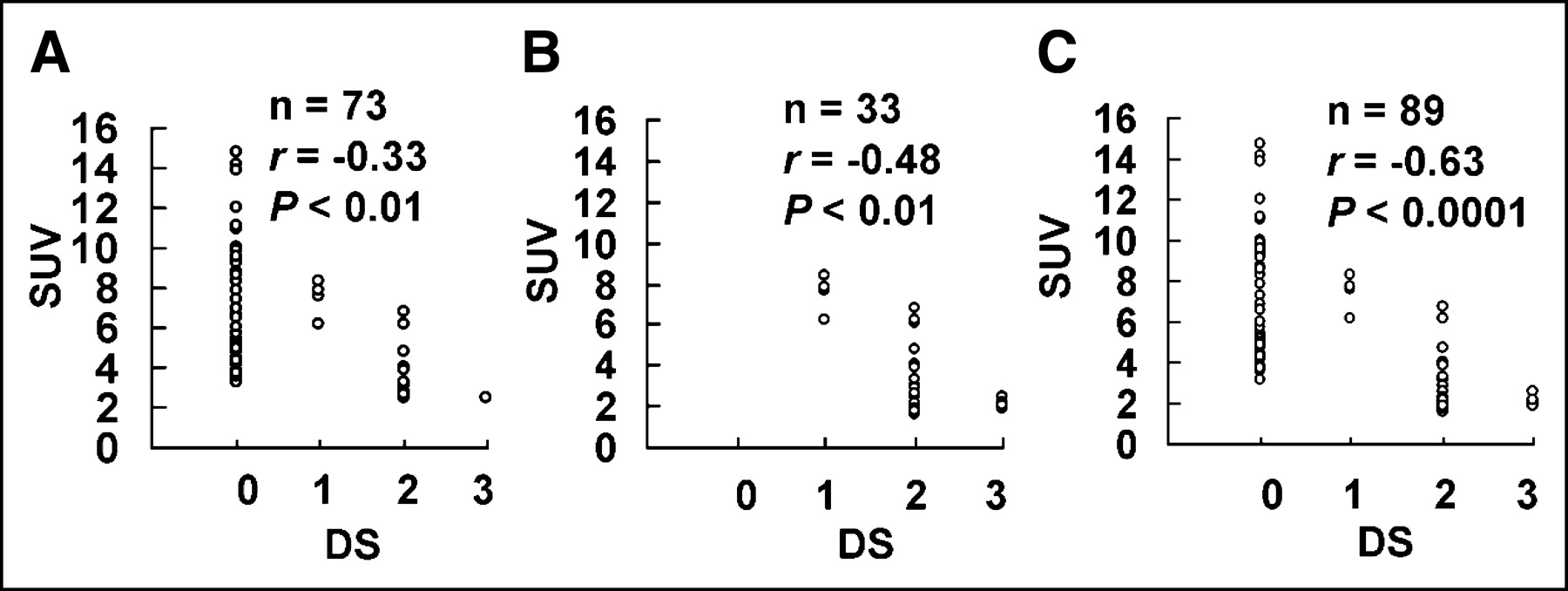
- FIGURE 4.
Correlation between SUV and DS in segments with abnormal 18F-FDG uptake (A), those with abnormal 99mTc-MIBI perfusion (B), and those with abnormal 18F-FDG uptake or 99mTc-MIBI defect (C). Significant negative correlations were observed in all types of abnormal segment.
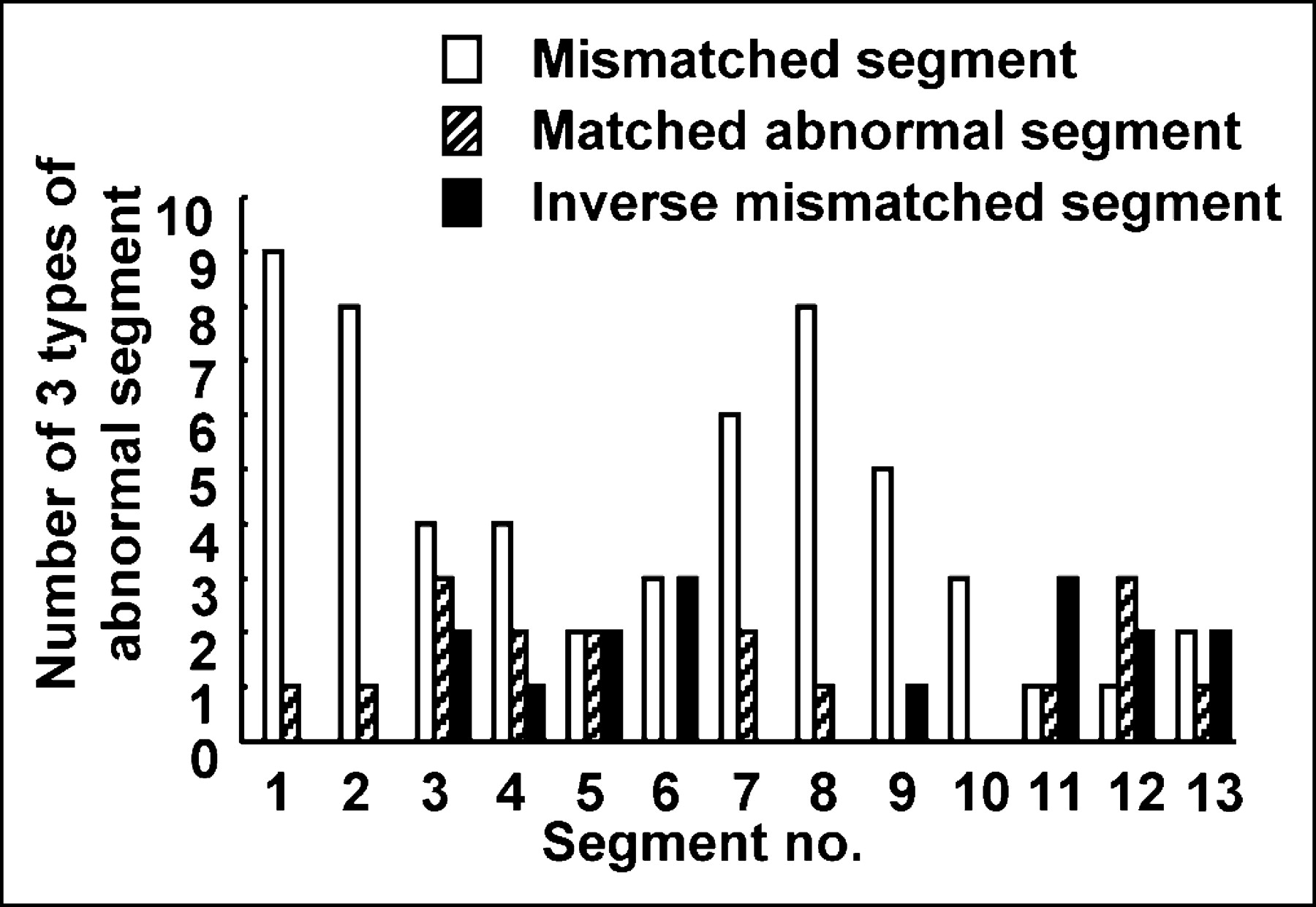
- FIGURE 5.
Localization of 3 types of abnormal segment.
- FIGURE 6.
Fasting 18F-FDG PET images (top) and 99mTc-MIBI SPECT images (bottom) in patient 9. 18F-FDG PET revealed markedly increased uptake of 18F-FDG in segments 1–8, whereas 99mTc-MIBI SPECT revealed no abnormal findings.
- FIGURE 7.
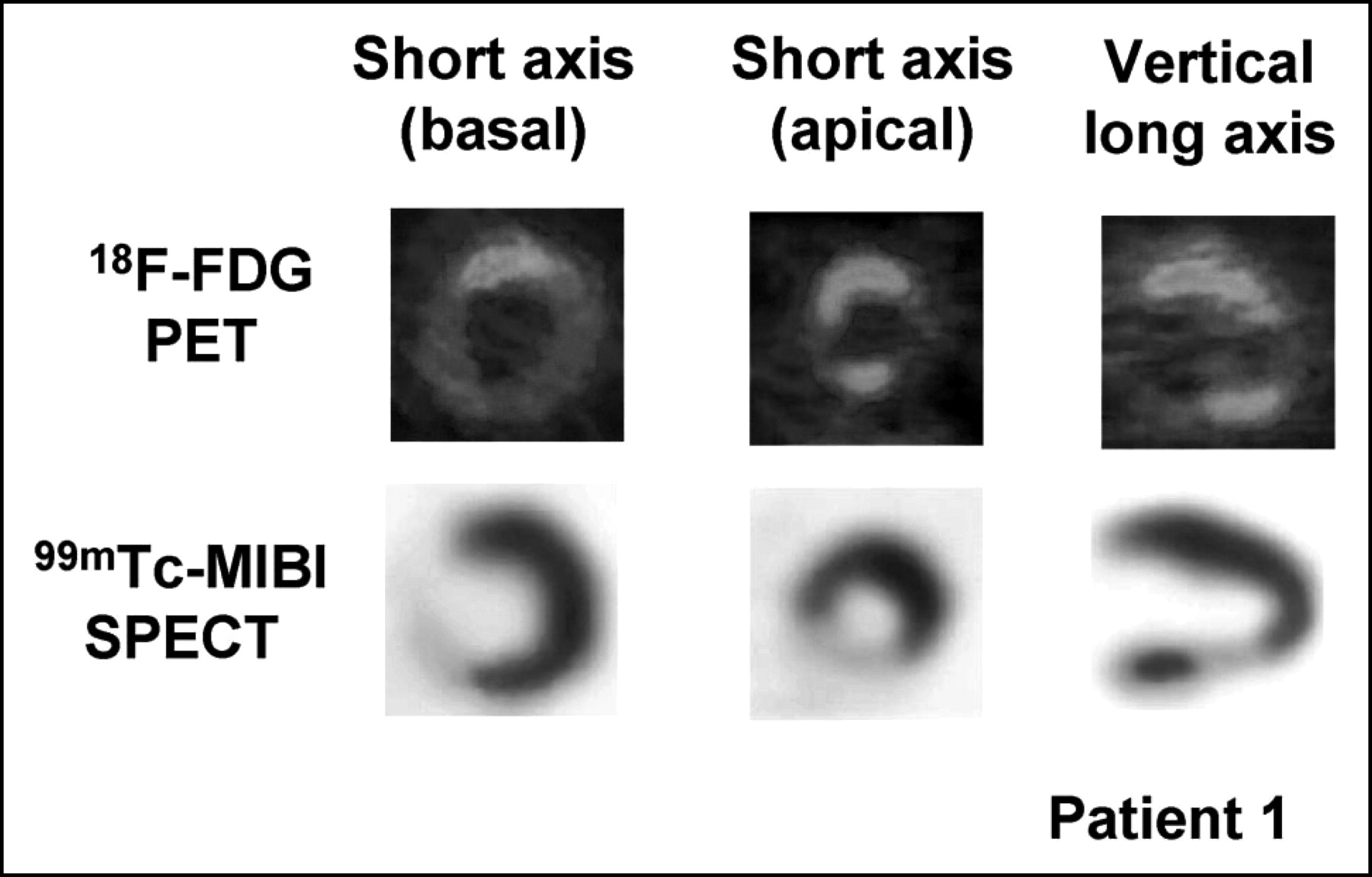
Fasting 18F-FDG PET images (top) and 99mTc-MIBI SPECT images (bottom) in patient 1. 18F-FDG PET revealed slightly increased uptake of 18F-FDG in segments 1, 2, 4, and 12. 99mTc-MIBI SPECT clearly revealed moderate reduction of 99mTc-MIBI uptake in segments 5, 6, and 12 and severe reduction of 99mTc-MIBI uptake in segment 3.


Tables
Patient no. Age (y) Sex ECG findings LVEF (%) Histologic diagnosis of extracardiac sarcoidosis Blood glucose (mg/dL) Serum ACE (IU/L 37°C) Group A 1 69 M Complete AVB 41 Myocardium 103 7.4 2 69 F Second AVB 45 Myocardium 85 8.8 3 65 F ST-T change, VT 33 Myocardium 82 12.3 4 73 F ST-T change, second AVB 47 Intraabdominal LN 91 14.4 5 52 F CRBBB, ST-T change, VT 71 TBLB 76 12.5 6 46 F CRBBB + LAH, second AVB 40 TBLB 74 30.1 7 55 F CRBBB + LAH, first AVB, VT 42 Scalene node 104 11.1 8 78 F ST-T change, second AVB 67 Scalene node 92 13.4 9 73 F Second AVB, PSVT 57 Skin 94 22.4 10 62 F CRBBB + LAH, VT 47 Skin 72 30.0 11 62 F Second AVB 68 Skin 81 18.3 Group B 12 62 F Normal 71 TBLB 95 3.5 13 54 F CRBBB 80 TBLB 85 19.7 14 44 M Normal 78 TBLB 77 30.2 15 37 F Normal 60 TBLB 84 39.3 16 56 F Normal 76 TBLB 102 12.5 17 74 F CRBBB 82 Scalene node 79 20.7 18 67 M Normal 67 Scalene node 101 12.1 19 66 F Normal 67 Skin 92 27.8 20 71 F Normal 68 Skin 74 11.2 21 64 F Normal 75 Skin 82 26.0 22 68 F ST-T change 73 Skin 104 18.0 ECG = electrocardiography; LVEF = left ventricular ejection fraction; ACE = angiotensin-converting enzyme; AVB = atrioventricular block; VT = ventricular tachycardia; LN = lymph node; CRBBB = complete right bundle branch block; TBLB = transbronchial lung biopsy; LAH = left anterior hemiblock; PSVT = paroxymal supraventricular tachycardia.
- TABLE 2
Guidelines for Diagnosis of Cardiac Sarcoidosis from Japanese Ministry of Health and Welfare
Criterion for diagnosis of cardiac sarcoidosis 1: Histologic diagnosis group Cardiac sarcoidosis is diagnosed when histologic analysis of operative or endomyocardial biopsy specimens demonstrates epithelioid granuloma without caseating granuloma. 2: Clinical diagnosis group In patients with histologic diagnosis of extracardiac sarcoidosis, cardiac sarcoidosis is diagnosed when item “a” and one or more of items “b-e” are present. a. Complete right bundle branch block, left-axis deviation, atrioventricular block, ventricular tachycardia, premature ventricular contraction (more than second grade of Lown’s classification), or abnormal Q or ST-T change on electrocardiogram or ambulatory electrocardiogram b. Abnormal wall motion, regional wall thinning or thickening, or dilatation of left ventricle on echocardiogram c. Perfusion defect in 201T1 myocardial scintigraphy or abnormal accumulation in 67Ga-citrate or 99mTc-pyrophosphate myocardial scintigraphy d. Abnormal intracardiac pressure, low cardiac output, or abnormal wall motion or depressed ejection fraction of left ventricle e. Interstitial fibrosis or cellular infiltration over moderate grade in endomyocardial biopsy even if findings are nonspecific Parameter Myocardial segment 1 2 3 4 5 6 7 8 9 10 11 12 13 Mean 1.94 1.92 1.89 1.85 1.87 1.87 1.98 1.95 1.94 1.93 1.93 1.92 1.86 SD 0.20 0.21 0.19 0.23 0.19 0.25 0.20 0.24 0.18 0.20 0.22 0.26 0.16 Mean + 2 SD 2.34 2.33 2.28 2.30 2.26 2.37 2.39 2.42 2.29 2.34 2.37 2.44 2.18 Patient no. 67Ga* 18F-FDG PET and 99mTc-MIBI SPECT segmental analysis† No. of abnormal segments T-SUV of 18F-FDG TDS of 99mTc-MIBI Seg. 1 Seg. 2 Seg. 3 Seg. 4 Seg. 5 Seg. 6 Seg. 7 Seg. 8 Seg. 9 Seg. 10 Seg. 11 Seg. 12 Seg. 13 18F-FDG 99mTc-MIBI Group A 1 + 3.51 (0) 3.54 (0) 2.13 (3) 3.18 (0) 1.84 (2) 1.62 (2) 2.08 (0) 2.14 (0) 1.74 (0) 2.03 (0) 1.77 (0) 2.51 (2) 2.01 (0) 4 4 30.1 9 2 + 3.82 (0) 4.12 (0) 3.08 (2) 4.03 (2) 2.08 (0) 1.87 (0) 2.12 (0) 1.83 (0) 1.94 (0) 1.68 (0) 1.64 (2) 1.60 (2) 1.78 (0) 4 4 31.6 8 3 − 2.84 (2) 3.81 (0) 2.51 (3) 2.82 (2) 1.89 (3) 1.61 (2) 2.64 (2) 3.54 (0) 1.68 (2) 1.83 (0) 1.95 (3) 1.95 (2) 1.87 (3) 6 10 30.9 24 4 − 14.13 (0) 6.20 (1) 8.70 (0) 2.24 (0) 2.13 (0) 2.02 (0) 14.70 (0) 9.41 (0) 6.60 (0) 4.48 (0) 2.06 (0) 2.13 (0) 5.98 (0) 8 1 80.8 1 5 − 5.23 (0) 4.82 (0) 4.47 (0) 2.21 (0) 1.98 (0) 1.71 (0) 4.98 (0) 4.16 (0) 3.88 (0) 1.90 (0) 1.82 (0) 1.80 (0) 2.13 (0) 6 0 41.1 0 6 + 6.88 (0) 7.31 (0) 2.23 (2) 2.20 (2) 4.72 (2) 2.08 (3) 10.94 (0) 11.12 (0) 7.79 (0) 9.32 (0) 9.20 (0) 7.60 (1) 6.11 (2) 10 6 87.5 12 7 + 4.31 (0) 4.97 (0) 2.04 (0) 1.93 (0) 1.73 (0) 1.78 (0) 3.25 (2) 3.82 (2) 1.95 (0) 1.91 (0) 1.83 (2) 1.75 (0) 1.80 (2) 4 4 33.1 8 8 − 2.21 (0) 2.14 (0) 1.95 (0) 1.98 (0) 1.84 (0) 1.78 (0) 5.44 (0) 4.88 (0) 5.13 (0) 2.10 (0) 2.01 (0) 1.83 (0) 1.90 (0) 3 0 35.2 0 9 − 5.74 (0) 5.12 (0) 4.18 (0) 4.24 (0) 3.64 (0) 3.56 (0) 5.01 (0) 4.76 (0) 1.74 (0) 1.95 (0) 2.28 (0) 1.83 (0) 1.78 (0) 8 0 45.8 0 10 − 13.81 (0) 9.94 (0) 6.71 (2) 8.34 (0) 6.15 (2) 8.56 (0) 12.02 (0) 9.78 (0) 9.91 (0) 9.53 (0) 7.78 (1) 8.30 (1) 6.90 (0) 13 4 117.7 6 11 − 9.54 (0) 2.30 (0) 6.51 (0) 4.91 (0) 6.02 (0) 3.71 (0) 2.21 (0) 4.41 (0) 1.97 (0) 2.01 (0) 2.12 (0) 4.25 (0) 1.89 (0) 7 0 51.9 0 Sum 73 33 Group B 12 − 2.10 (0) 1.98 (0) 1.88 (0) 1.71 (0) 1.76 (0) 1.81 (0) 2.14 (0) 2.01 (0) 1.98 (0) 1.89 (0) 1.74 (0) 1.80 (0) 1.89 (0) 0 0 24.7 0 13 − 1.56 (0) 1.61 (0) 1.41 (0) 1.53 (0) 1.43 (0) 1.45 (0) 1.69 (0) 1.79 (0) 1.88 (0) 1.61 (0) 1.79 (0) 1.78 (0) 2.01 (0) 0 0 21.5 0 14 − 1.78 (0) 1.83 (0) 1.88 (0) 1.71 (0) 1.63 (0) 1.72 (0) 1.97 (0) 1.94 (0) 1.93 (0) 2.01 (0) 2.11 (0) 2.01 (0) 1.79 (0) 0 0 24.3 0 15 − 1.91 (0) 1.82 (0) 1.79 (0) 1.85 (0) 1.90 (0) 1.85 (0) 2.15 (0) 2.08 (0) 2.17 (0) 1.83 (0) 1.65 (0) 1.72 (0) 1.89 (0) 0 0 24.6 0 16 − 2.18 (0) 2.08 (0) 1.92 (0) 1.95 (0) 2.08 (0) 1.89 (0) 1.82 (0) 1.79 (0) 1.70 (0) 1.71 (0) 1.94 (0) 1.91 (0) 1.99 (0) 0 0 25.0 0 17 − 1.98 (0) 2.17 (0) 1.91 (0) 2.05 (0) 1.86 (0) 1.99 (0) 1.99 (0) 2.09 (0) 1.80 (0) 1.82 (0) 1.75 (0) 1.72 (0) 1.73 (0) 0 0 24.9 0 18 − 2.04 (0) 1.89 (0) 2.15 (0) 2.08 (0) 1.87 (0) 1.71 (0) 1.65 (0) 1.70 (0) 1.88 (0) 1.99 (0) 2.11 (0) 1.86 (0) 1.98 (0) 0 0 24.9 0 19 − 1.97 (0) 2.13 (0) 2.07 (0) 1.78 (0) 2.05 (0) 1.90 (0) 2.27 (0) 2.29 (0) 2.10 (0) 2.15 (0) 2.19 (0) 2.29 (0) 1.62 (0) 0 0 26.8 0 20 − 1.72 (0) 1.60 (0) 1.85 (0) 1.77 (0) 1.88 (0) 2.07 (0) 1.91 (0) 1.88 (0) 1.67 (0) 1.97 (0) 1.99 (0) 1.96 (0) 1.97 (0) 0 0 24.2 0 21 − 2.03 (0) 1.99 (0) 2.21 (0) 2.08 (0) 2.06 (0) 1.99 (0) 1.79 (0) 2.11 (0) 2.18 (0) 2.20 (0) 2.00 (0) 1.99 (0) 1.81 (0) 0 0 26.4 0 22 − 3.11 (0) 2.81 (0) 3.13 (0) 2.77 (0) 1.91 (0) 2.12 (0) 3.30 (0) 3.13 (0) 3.10 (0) 3.07 (0) 1.81 (0) 1.95 (0) 2.10 (0) 8 0 34.3 0 Sum 8 0 - TABLE 5
Diagnostic Performance of Fasting 18F-FDG PET, 99mTc-MIBI SPECT, and 67Ga Scintigraphy
Parameter Percentage (no. of patients) 18F-FDG PET 99mTc-MIBI SPECT 67Ga scintigraphy Sensitivity 100 (11/11) 63.6* (7/11) 36.4† (4/11) Specificity 90.9 (10/11) 100 (11/11) 100 (11/11) Accuracy 95.5 (21/22) 81.8 (18/22) 68.2* (15/22)
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence of ventricular parasystole in patients with cardiac sarcoidosis: correlation between parasystole and inflammation in ventricular fibrillation
- T2-weighted short-tau-inversion-recovery imaging reflects disease activity of cardiac sarcoidosis
- Predicting risk of sudden cardiac death in patients with cardiac sarcoidosis using multimodality imaging and personalized heart modeling in a multivariable classifier
- Myocarditis in systemic lupus erythematosus diagnosed by 18F-fluorodeoxyglucose positron emission tomography
- Spectrum of Restrictive and Infiltrative Cardiomyopathies: Part 2 of a 2-Part Series
- Hospitalization Rates, Prevalence of Cardiovascular Manifestations, and Outcomes Associated With Sarcoidosis in the United States
- Joint SNMMI-ASNC Expert Consensus Document on the Role of 18F-FDG PET/CT in Cardiac Sarcoid Detection and Therapy Monitoring
- Inter- and Intraobserver Agreement of 18F-FDG PET/CT Image Interpretation in Patients Referred for Assessment of Cardiac Sarcoidosis
- Time Course and Factors Correlating With Ventricular Tachyarrhythmias After Introduction of Steroid Therapy in Cardiac Sarcoidosis
- Additional Heparin Preadministration Improves Cardiac Glucose Metabolism Suppression over Low-Carbohydrate Diet Alone in 18F-FDG PET Imaging
- Advanced Imaging of Cardiac Sarcoidosis
- Is There an Association Between Clinical Presentation and the Location and Extent of Myocardial Involvement of Cardiac Sarcoidosis as Assessed by 18F- Fluorodoexyglucose Positron Emission Tomography?
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Imaging the inflammatory activity of sarcoidosis
- The Use of 18F-FDG PET in the Diagnosis of Cardiac Sarcoidosis: A Systematic Review and Metaanalysis Including the Ontario Experience
- Intraocular sarcoidosis: association of clinical characteristics of uveitis with findings from 18F-labelled fluorodeoxyglucose positron emission tomography
- Monomorphic Ventricular Tachycardia and Mediastinal Adenopathy Due to Granulomatous Infiltration in Patients With Preserved Ventricular Function
- Cardiac Sarcoidosis and Giant Cell Myocarditis as Causes of Atrioventricular Block in Young and Middle-Aged Adults
- Undiagnosed myocardial sarcoidosis presenting as life threatening cardiac dysrhythmia
- Heterogeneous Myocardial FDG Uptake and the Disease Activity in Cardiac Sarcoidosis
- Ventricular tachycardia as the first manifestation of cardiac sarcoidosis
- 18F-FDG PET scan as follow-up tool for sarcoidosis with symptomatic cardiac conduction disturbances requiring a pacemaker
- 18F-FDG PET scan as follow-up tool for sarcoidosis with symptomatic cardiac conduction disturbances requiring a pacemaker
- Detecting cardiac involvement in sarcoidosis: a call for prospective studies of newer imaging techniques
- Comparative Evaluation of 18F-FDG PET and 67Ga Scintigraphy in Patients with Sarcoidosis
- Cardiac sarcoidosis