


Abstract
67Ga scintigraphy has been used for years in sarcoidosis for diagnosis and the extent of the disease. However, little information is available on the comparison of 18F-FDG PET and 67Ga scintigraphy in the assessment of sarcoidosis. The purpose of this study was to compare the uptake of 18F-FDG and 67Ga in the evaluation of pulmonary and extrapulmonary involvement in patients with sarcoidosis. Methods: Eighteen patients with sarcoidosis were examined. 18F-FDG PET was performed at 1 h after injection of 185−200 MBq 18F-FDG. 67Ga whole-body planar and thoracic SPECT images were acquired 72 h after injection of 111 MBq 67Ga. We evaluated 18F-FDG and 67Ga uptake visually and semiquantitatively using standardized uptake values (SUVs) and the ratio of lesion to normal lumbar spine (L/N ratio), respectively. The presence of pulmonary and extrapulmonary lesions was evaluated histopathologically or by the radiologic findings. Results: Five patients had only pulmonary lesions, 12 patients had both pulmonary and extrapulmonary lesions, and 1 patient had only an extrapulmonary lesion. Both 67Ga planar and SPECT images detected 17 of 21 (81%) clinically observed pulmonary sites. The mean ± SD of the L/N ratio was 1.97 ± 1.09. 67Ga planar images detected 15 of 31 (48%) clinically observed extrapulmonary sites. The mean ± SD of the L/N ratio was 1.17 ± 0.33. 18F-FDG PET detected all 21 (100%) clinically observed pulmonary sites. The mean ± SD of the SUV was 7.40 ± 2.48. 18F-FDG PET detected 28 of 31 (90%) clinically observed extrapulmonary sites. The mean ± SD of the SUV was 5.90 ± 2.75. Conclusion: The results of this clinical study suggest that 18F-FDG PET can detect pulmonary lesions to a similar degree as 67Ga scintigraphy. However, 18F-FDG PET appears to be more accurate and contributes to a better evaluation of extrapulmonary involvement in sarcoidosis patients.
Sarcoidosis is a multisystem inflammatory disease of unknown origin, characterized by the presence of noncaseating epithelioid cell granulomas in the affected tissue (1). Correct assessment of disease activity is critical for initiating an optimal management plan because a small percentage of patients may die without treatment soon after diagnosis, although most patients will have a self-limited course (1).
Traditionally, although 67Ga has been used in scanning for the detection of sarcoidosis, it has serious limitations. First, patients must be injected with the radiolabeled material at least 48−72 h before image acquisition (2). Second, there is significant interobserver variability in the interpretation of 67Ga scans (3,4). Third, although certain patterns noted on 67Ga scans are considered to be unique to sarcoidosis (e.g., the λ-panda pattern), the overall sensitivity and specificity of 67Ga vary significantly (5,6). Some researchers have reported that this tool is highly accurate, whereas others have failed to observe similar findings (5,6). Thus, at present, 67Ga scanning is generally considered to have a limited role in the evaluation and management of sarcoidosis (7).
PET with 18F-FDG is a well-established functional imaging technique for diagnostic oncologic imaging that provides data on glucose metabolism in lesions (8). However, 18F-FDG PET allows the visualization not only of the malignant cells but also of the inflammatory cells (9,10). Lewis and Salama first observed 18F-FDG uptake in sarcoid lesions in 2 patients (11). Increased 18F-FDG accumulation in patients with sarcoidosis was subsequently reported by multiple other groups (12–14).
To our knowledge, with the exception of a sporadic case report, the literature contains no data on the potential advantages of 18F-FDG PET over 67Ga scintigraphy in the detection of granulomatous sites in patients with sarcoidosis. Therefore, the aim of this study was to compare 18F-FDG PET and 67Ga scintigraphy in the evaluation of pulmonary and extrapulmonary involvement in patients with sarcoidosis.
MATERIALS AND METHODS
Patients
The research study protocol was approved by the University Hospital Institutional Review Board. Written informed consent was obtained from each patient before entry into the study.
Eighteen consecutive patients with sarcoidosis (6 men, 12 women; mean age, 58.8 y; age range, 29−82 y) who underwent both 18F-FDG PET and 67Ga scintigraphy between February 2003 and December 2005 were retrospectively selected. Except for heart, the sarcoidosis was diagnosed by histologically proven noncaseating epithelioid granuloma on transbronchial hilar or mediastinal lymph node biopsy in 6 patients, scalene node biopsy in 2 patients, skin biopsy in 2 patients, and gastric biopsy in 1 patient. According to The Japanese Ministry of Health and Welfare's Guideline for Diagnosis of Cardiac Sarcoidosis described in Table 1 (15), 7 patients were diagnosed as having cardiac sarcoidosis. Of these 7 patients, the sarcoidosis was diagnosed by histologically proven noncaseating epithelioid granuloma on transbronchial hilar or mediastinal lymph node biopsy in 5 patients, scalene node biopsy in 1 patient, and skin biopsy in 1 patient. Pulmonary involvement was assessed by chest radiographic imaging, including CT findings. Extrapulmonary involvement was considered present if ocular, skin, muscle, lymph node, or other extrapulmonary manifestations of sarcoidosis were documented. The serum angiotensin-converting enzyme level was measured. None of the patients was receiving corticosteroids at the time of the study or had received them within the previous 3 mo. No patient showed evidence of diabetes mellitus.
Guideline for Diagnosis of Cardiac Sarcoidosis from The Japanese Ministry of Health and Welfare (15)
18F-FDG PET and Reconstruction
All patients were instructed to fast for at least 5 h before PET. Unfractionated heparin (50 IU/kg) was preadministered intravenously to all patients with cardiac sarcoidosis in an attempt to reduce physiologic 18F-FDG uptake by the myocardium (16). To obtain a consistent effect, injection of 18F-FDG was performed 15 min after administration of heparin. Serum glucose levels were measured at the time of 18F-FDG administration. Patients were instructed not to speak or chew after 18F-FDG administration to avoid unwanted artifacts.
All 18F-FDG PET examinations were performed with an ECAT EXACT HR+ camera (Siemens/CTI Inc.). This camera acquires 63 planes simultaneously over a 15.5-cm field of view. In-plane resolution was approximately 4.6 mm, with an axial resolution of approximately 3.5-mm full width at half maximum. Images were acquired in 3-dimensional mode. A transmission scan was obtained using a 68Ge rod source for the purpose of attenuation correction. The emission scan began at 60 min after injection of 185−200 MBq 18F-FDG. Seven or 8 bed positions were used to scan from the skull base to the midthighs. PET images were reconstructed with ordered-subsets expectation maximization (OSEM) using 2 iterations and 8 subsets.
67Ga Imaging and Reconstruction
67Ga scintigraphy was performed at 72 h after injection of 111 MBq 67Ga-citrate. Imaging was performed with a large-field-of-view γ-camera (Prism 2000; Picker International) with medium-energy and a general-purpose collimator. Twenty-percent windows were placed symmetrically around each of the 3 main photo peaks of 67Ga (93, 184, and 296 keV). Whole-body imaging was performed with both anterior and posterior view images at a speed of 15 cm/min. The spot images were obtained by collecting 300,000−500,000 counts at the preset time of 5 min. Thoracic SPECT was performed on all patients except for 1 patient with an extrapulmonary lesion. SPECT was performed on a 64 × 64 matrix at 120° at 30 s each over a range of 360°. Transverse, coronal, and sagittal sections were reconstructed. SPECT images were reconstructed with OSEM using 2 iterations and 12 subsets.
18F-FDG PET and 67Ga Image Interpretation
Two experienced nuclear physicians retrospectively reviewed attenuation-corrected transaxial, coronal, sagittal, and 3-dimensional PET images using a dedicated computer workstation (Siemens/CTI, Inc.). The same nuclear physicians retrospectively reviewed 67Ga planar and SPECT images using another dedicated computer workstation (FX; Shimadzu). Readers were unaware of CT scan findings and accompanying reports, although they knew the diagnosis of sarcoidosis. 67Ga images were read before 18F-FDG PET images, with an interval of several days between interpretations. Images were evaluated independently and, in the case of disagreement, the final decision was made by consensus.
Pulmonary and extrapulmonary involvement on conventional evaluation, on 18F-FDG PET, or on 67Ga scintigraphy was evaluated. For visual analysis, in the mediastinum/hilum, focal radioactivity that was greater than the surrounding background mediastinal activity was interpreted as spread of sarcoidosis. Focal increases in radioactivity seen in locations unaccounted for by the normal biodistribution of the agent were interpreted as pulmonary parenchyma and spread of extrapulmonary disease. The increased accumulation in the salivary glands was identified by tracer uptake greater than that in the normal nasopharynx. For the analysis of sarcoidosis involvement, evaluation was done using 2 sites: pulmonary and extrapulmonary. The pulmonary site included mediastinal/hilar lymph nodes and pulmonary parenchyma. The extrapulmonary site included nonpulmonary lesions. Bilateral organs—including salivary glands, cervical or supraclavicular lymph nodes, axillary lymph nodes, paraaortic lymph nodes, inguinal lymph nodes, and muscles—were considered as only 1 organ site (even when the extent was unilateral) for sarcoidosis involvement. Multiple lesions in the skin were defined as a single lesion.
For lesions visualized on 18F-FDG PET, regions of interest (ROIs) were placed over the entire 18F-FDG–avid lesion including the largest amount of radioactivity. The standardized uptake value (SUV) was calculated by using the following formula: where cdc is the decay-corrected tracer tissue concentration (in Bq/g), di is the injected dose (in Bq), and w is the patient's body weight (in g). The maximal SUV value in the lesion ROI was calculated. For lesions visualized on 67Ga scintigraphy, ROIs were placed over the entire 67Ga-avid lesion (L) including the largest amount of radioactivity and the normal lumbar spine (N) on the planar image. The mean values of the ROIs (total counts/total pixels) were calculated, and the ratio of the lesion to normal lumbar spine (L/N ratio) was obtained.
where cdc is the decay-corrected tracer tissue concentration (in Bq/g), di is the injected dose (in Bq), and w is the patient's body weight (in g). The maximal SUV value in the lesion ROI was calculated. For lesions visualized on 67Ga scintigraphy, ROIs were placed over the entire 67Ga-avid lesion (L) including the largest amount of radioactivity and the normal lumbar spine (N) on the planar image. The mean values of the ROIs (total counts/total pixels) were calculated, and the ratio of the lesion to normal lumbar spine (L/N ratio) was obtained.
18F-FDG PET and 67Ga scintigraphy findings were compared with the results of biopsy or clinical−radiologic follow-up as the reference standards. A hypermetabolic 18F-FDG or 67Ga lesion was considered true-positive for sarcoidosis involvement if proven by biopsy or if resolved after corticosteroid therapy on follow-up 18F-FDG PET, 67Ga scintigraphy, or other imaging.
Statistical Analysis
For statistical comparison of data obtained from 18F-FDG PET, 67Ga planar imaging, and SPECT, the Fisher exact test was used. Results were considered to be statistically significant if the probability P of a first-degree error was <0.05.
RESULTS
The median time interval between 18F-FDG PET and 67Ga scintigraphy was 6.6 d (range, 2−20 d). The mean ± SD blood glucose level at the time of 18F-FDG injection was 101.6 ± 11.7 mg/dL (range, 82−123 mg/dL).
Twenty-one pulmonary involvements (17 mediastinal/hilar lymph node and 4 pulmonary parenchyma) were identified in 17 of the 18 patients (Table 2). Eleven pulmonary involvements had histologic verification and the remaining 10 were correlated with clinical−radiologic follow-up. 18F-FDG or 67Ga pulmonary uptake in these 10 lesions was decreased after corticosteroid therapy. All 17 mediastinal/hilar lymph nodes had bilateral involvement. The prevascular region was not involved and calcification was not present on CT in all patients with pulmonary involvement. All 21 pulmonary involvements were visually identified with 18F-FDG PET. The mean ± SD of the SUV was 7.40 ± 2.48. Thirteen mediastinal/hilar lymph nodes and 4 pulmonary parenchymal involvements were visually identified with both 67Ga planar imaging and SPECT. The mean ± SD of the L/N ratio was 1.97 ± 1.09. Neither 18F-FDG PET nor 67Ga scintigraphy showed any false-positive results in the pulmonary area. No significant difference in the detection of pulmonary involvement was found between 18F-FDG PET, 67Ga planar imaging, and 67Ga SPECT.
18F-FDG PET and 67Ga Scintigraphy Findings in 18 Patients with Sarcoidosis
Thirty-one extrapulmonary involvements (10 lymph node, 7 heart, 6 muscle, 3 salivary gland, 3 skin, 1 spleen, and 1 stomach) were identified in 13 of the 18 patients (Table 2). Eight extrapulmonary involvements had histologic verification and the remaining 23 were correlated with clinical−radiologic follow-up. 18F-FDG or 67Ga extrapulmonary uptake in these 23 lesions decreased after corticosteroid therapy. Of the extrapulmonary involvements, 28 were visually identified with 18F-FDG PET. The mean ± SD of the SUV was 5.90 ± 2.75. Fifteen extrapulmonary involvements were visually identified with 67Ga planar scintigraphy. The mean ± SD of the L/N ratio was 1.17 ± 0.33. Two salivary gland involvements were visually identified with 67Ga planar scintigraphy but not with 18F-FDG PET. One stomach involvement was not visually identified with both 18F-FDG PET and 67Ga planar scintigraphy. Neither 18F-FDG PET nor 67Ga scintigraphy showed any false-positive results in the extrapulmonary area. No significant difference in the detection of extrapulmonary involvement was found between 18F-FDG PET and 67Ga planar scintigraphy.
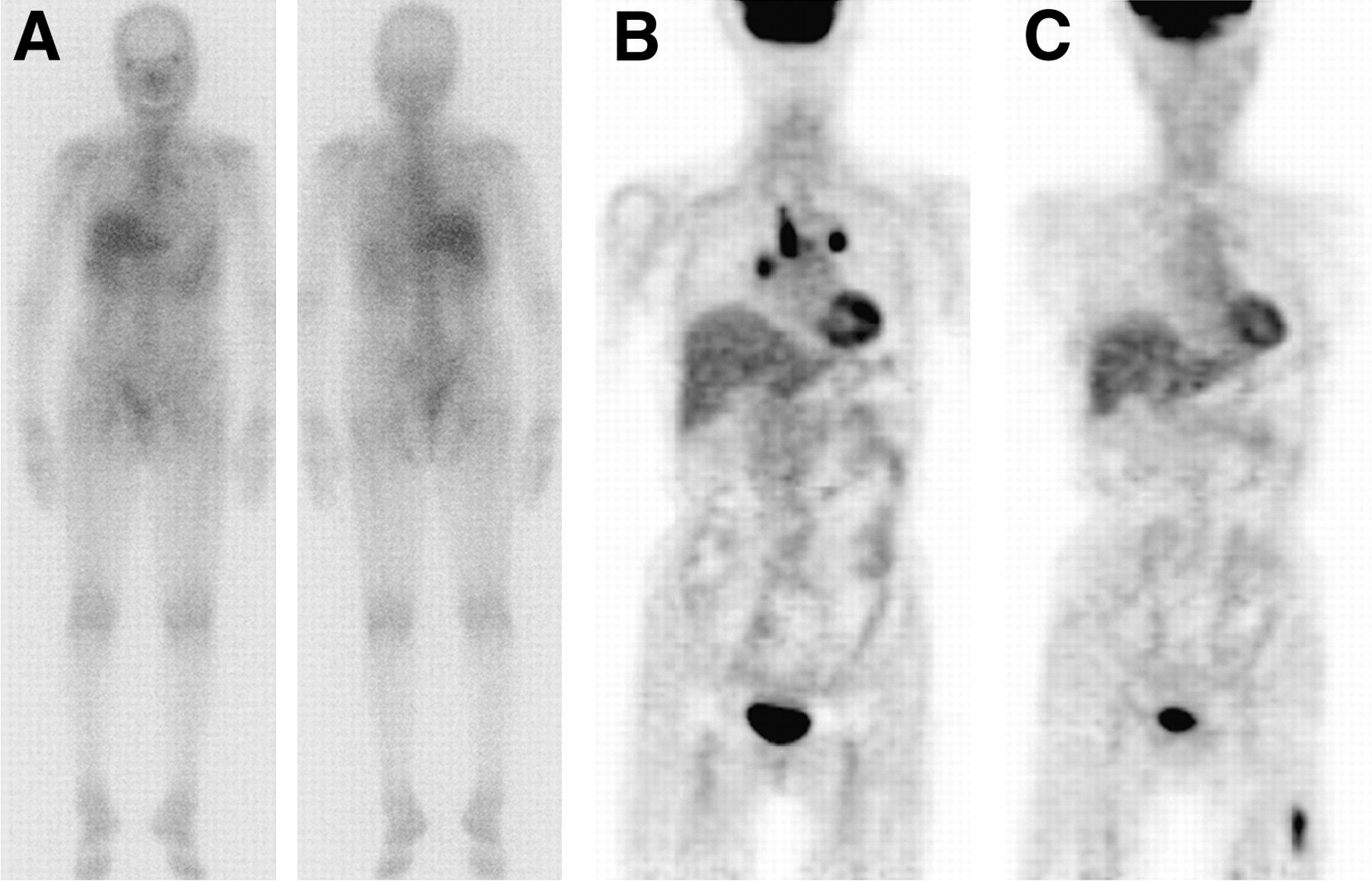
Figure 1 illustrates 67Ga scintigraphy and 18F-FDG PET images of a patient with pulmonary and extrapulmonary sarcoidosis.
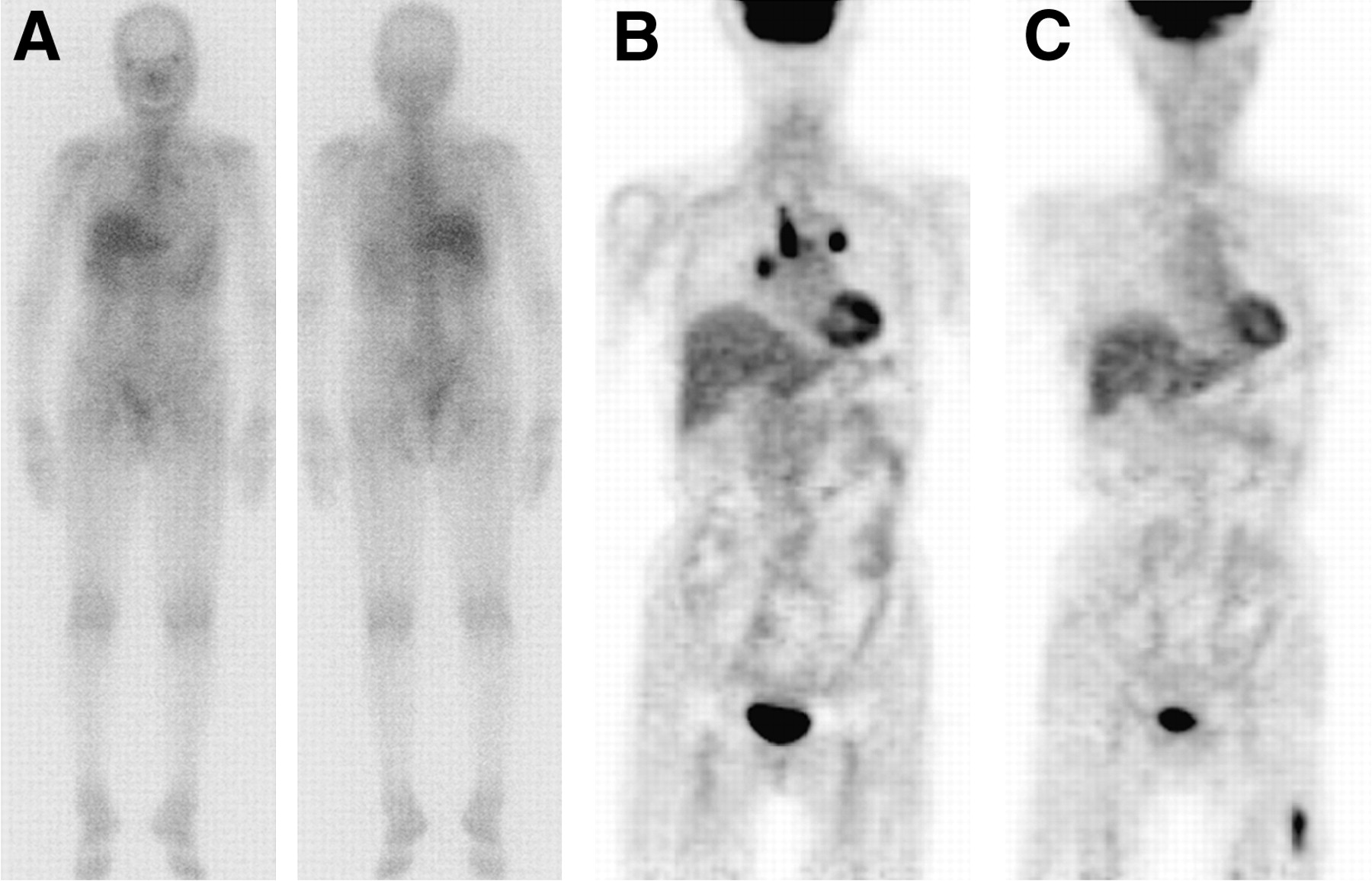
67Ga scintigraphy and 18F-FDG PET images of 70-y-old woman with pulmonary and extrapulmonary sarcoidosis (patient 10 in Table 1). (A) Anterior and posterior 67Ga whole-body images show no abnormal uptake. (B) 18F-FDG PET image shows increased uptake at mediastinal and bilateral hila. (C) Increased uptake is also observed at left upper thigh on 18F-FDG PET image.
DISCUSSION
This study, although limited in the number patients, involves a direct comparison of 67Ga scintigraphy and 18F-FDG PET in the same sarcoidosis group. 18F-FDG PET appears to be preferable in patients with sarcoidosis because of at least comparable and perhaps even better sensitivity of 18F-FDG PET in addition to several practical advantages (less radiation exposure, shorter duration between injection and diagnosis).
Previous lymphoma studies suggest that 18F-FDG PET should be used in place of 67Ga scintigraphy because the former detects significantly more disease sites (17), defines active disease more accurately (18), and leads to improved detection of intraabdominal nodal disease (19). Compared with 67Ga scintigraphy, 18F-FDG PET has several advantages: Because of the favorable physical conditions of positron emitters, PET enables higher spatial resolution than do conventional nuclear medicine imaging techniques. This higher spatial resolution enables the acquisition of excellent-quality images within 2 h, whereas the acquisition of a 67Ga scintigram can be performed 48−72 h after injection. Furthermore, the good image quality of 18F-FDG PET enables the detection of even small lesions. In the future, 18F-FDG PET might prove to be a sensitive marker of disease activity in sarcoidosis patients and replace 67Ga scintigraphy as in case of lymphoma diagnosis.
In patients with pulmonary sarcoidosis, 18F-FDG uptake of lung has been reported to be concordant with histopathologic activity of pulmonary sarcoidosis and was found to be decreased after high-dose steroid therapy (14). The ability to visualize 18F-FDG accumulation by activated inflammatory cells makes PET a promising modality for the management of sarcoidosis. Some reports demonstrated that 18F-FDG PET was superior to 67Ga scintigraphy in evaluation of fever of unknown origin (20,21). These reports in combination with the results of the present study suggest that 18F-FDG PET has the potential to become the single most-effective imaging modality in the evaluation of nonmalignant disorders.
The use of SPECT considerably increases the accuracy of 67Ga imaging in the staging of malignant lymphoma (22). In the present study, 17 of 21 pulmonary involvements were visually identified with both 67Ga planar imaging and SPECT. In this study, 67Ga SPECT appeared to offer no additional information. 67Ga is known to be more sensitive for lesions in superficial location, such as skin and muscle regions (22). However, in our study, 67Ga imaging was false-negative in 2 skin and 3 muscle lesions. This finding may, in part, be due to the characteristics of the studied patient population. Recently, whole-body SPECT has become possible (23). In the present study, only thoracic SPECT was performed. In this respect, further studies are needed to compare 18F-FDG PET and whole-body 67Ga SPECT in patients with sarcoidosis.
There are no standard, accepted approaches for the evaluation of suspected extrapulmonary sarcoidosis. Somatostatin analog scintigraphies (99mTc-depreotide, 111In pentetreotide) represent a novel alternative to 67Ga scintigraphy in extrapulmonary sarcoidosis (2,3). 201Tl scintigraphy, which has been studied in cardiac sarcoidosis patients, frequently demonstrates heterogeneous cardiac uptake in patients without clinical disease (24). Recent studies have revealed that 18F-FDG PET is a useful method for identification of cardiac sarcoidosis (16,25). Okumura et al. (25) compared 18F-FDG PET with 67Ga scintigraphy in 11 patients with cardiac sarcoidosis. The sensitivity of 18F-FDG PET (100%) in detecting cardiac sarcoidosis was significantly (P < 0.01) higher than that of 67Ga scintigraphy (36%). In our investigation of 7 patients with cardiac sarcoidosis, although the study group was small, all (100%) exhibited myocardial 18F-FDG uptake and only 3 (43%) exhibited 67Ga uptake in the heart. These results are similar to those obtained by Okumura et al. (25). Thus, 18F-FDG PET seems to be a promising alternative to 67Ga scintigraphy for evaluating the extent of extrapulmonary sarcoidosis. However, we evaluated even cardiac sarcoidosis using only whole-body 18F-FDG PET. Neither cardiac 18F-FDG PET nor perfusion PET was performed in this study. In this respect, further studies are needed to evaluate cardiac involvement.
The value of the data from the present study is limited by the retrospective nature of the study and the small number of sarcoidosis patients. Also, the results were not all proven by a histologic gold standard. It may be difficult to differentiate between physiologic and pathologic uptake, such as gastric uptake, by 18F-FDG PET. The selection of patients with more severe disease is possible for performing both 18F-FDG PET and 67Ga scintigraphy instead of only one of these procedures. However, more extrapulmonary involvement was detected with 18F-FDG PET than with 67Ga scintigraphy, despite the fact that in most cases the field of view for 67Ga scintigraphy was larger than that for 18F-FDG PET. At the same time, PET is time-consuming for a whole-body survey from head to toe. However, a modern PET/CT hybrid scanner can greatly reduce the scanning time. Further evolution of PET scanner technology—including the PET/CT hybrid scanner, larger-field-of-view scanners, better detector material, and superior processing methods—should provide superior diagnostic performance. Further studies involving a larger number of patients are required to clarify further the clinical usefulness of 18F-FDG PET and 67Ga scintigraphy in sarcoidosis patients.
CONCLUSION
The results of this clinical study suggest that 18F-FDG PET can detect pulmonary lesions to a similar degree as 67Ga scintigraphy. However, 18F-FDG PET appears to be more accurate and contributes to a better evaluation of extrapulmonary involvement in sarcoidosis patients.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 2, 2006.
- Accepted for publication July 25, 2006.





{kind=link}
Jump to section
Related Articles
Cited By...
- Distinguishing neurosarcoidosis from multiple sclerosis based on CSF analysis: A retrospective study
- Differential diagnosis of granulomatous lung disease: clues and pitfalls: Number 4 in the Series "Pathology for the clinician" Edited by Peter Dorfmüller and Alberto Cavazza
- PET/CT in nononcological lung diseases: current applications and future perspectives
- Osseous Sarcoidosis
- Is There an Association Between Clinical Presentation and the Location and Extent of Myocardial Involvement of Cardiac Sarcoidosis as Assessed by 18F- Fluorodoexyglucose Positron Emission Tomography?
- Imaging the inflammatory activity of sarcoidosis
- The Utility of 18F-FDG PET/CT for Diagnosis and Adjustment of Therapy in Patients with Active Chronic Sarcoidosis
- The Use of 18F-FDG PET in the Diagnosis of Cardiac Sarcoidosis: A Systematic Review and Metaanalysis Including the Ontario Experience
- Intraocular sarcoidosis: association of clinical characteristics of uveitis with findings from 18F-labelled fluorodeoxyglucose positron emission tomography
- Noninvasive Detection and Localization of Vulnerable Plaque and Arterial Thrombosis With Computed Tomography Angiography/Positron Emission Tomography