


Abstract
The distribution of radioiodinated metaiodobenzylguanidine (MIBG) has been studied primarily in patients with neuroendocrine tumors—in pediatrics, particularly with neuroblastomas. Sometimes, symmetric accumulation in which no tumor is identified is seen in the nape-of-the-neck region. We estimated visually whether accumulation was found in the nape of the neck and studied the characteristics of the accumulation. Methods: Retrospectively, we investigated 266 123I-MIBG scintigraphic studies performed on pediatric patients who had been treated for neuroendocrine tumors or who were suspected of having such tumors. Results: Accumulation in the nape of the neck was seen in 32 of 266 studies (12%); in none of these cases was the accumulation identified as a tumor by other imaging modalities or follow-up studies. In the same individuals, the accumulation varied and it was observed more often during winter. Conclusion: Symmetric 123I-MIBG accumulations in the nape-of-the-neck region observed in children are thought to be related to the uptake in brown adipose tissue.
- 123I-metaiodobenzylguanidine
- neuroendocrine tumor
- brown adipose tissue
- nape-of-the-neck accumulation
- children
Metaiodobenzylguanidine (MIBG) is a derivative of guanethidine, and radioiodinated MIBG has been used for the scintigraphic localization of tumors derived from neural crest tissue that produce and store catecholamines (1,2). Radioiodinated MIBG is very helpful in the detection of metastatic or recurrent lesions as well as to diagnose the primary tumor (3,4). 131I-Labeled MIBG has been the medium used most often for identifying neuroendocrine tumors, both because of its commercial availability and because it permits delayed imaging. Presently, 123I-MIBG is also used for tumor imaging because of its lower radiation burden and potential advantages for examination compared with 131I-MIBG. 123I has a characteristic γ-ray photon energy of 159 keV, which is well suited for gamma cameras equipped with low-energy, high-resolution collimators and which also allows clear imaging with SPECT acquisition (5).
Because MIBG acts like norepinephrine, the distribution and the mechanism of accumulation in organs are usually easily interpreted. The normal distribution of radioiodinated MIBG has been well described (6). Though its clear mechanism of accumulation in neuroendocrine tumors seldom causes confusion in interpreting the images, the use of 123I-MIBG has recently demonstrated physiologic accumulations other than the intense accumulations in the myocardium and neuroendocrine tumors.
In our observation of 123I-MIBG studies performed on patients with neuroblastomas, symmetric accumulation is sometimes seen on the nape-of-the-neck region, which seems to have little relationship to tumor tissue. To prevent misdiagnosis of a false-positive lesion, it is necessary to recognize the exact nature of the accumulation. The aim of this study was to retrospectively investigate the characteristics of 123I-MIBG accumulations in the nape-of-the-neck region.
MATERIALS AND METHODS
Patients
Two hundred sixty-six 123I-MIBG studies, which were performed for the evaluation of neuroendocrine tumors after treatment, were included in this study (age range, 0.5 mo to 12 y; mean ± SE, 3.6 ± 3.2 y; 120 boys, 146 girls). The studies with tumor lesions in which 123I-MIBG accumulated were not included in this study. Two hundred sixty were studies performed for follow-up of patients, whose neuroblastoma had been treated, and the accumulation was estimated retrospectively. Most patients with neuroblastoma underwent repeated 123I-MIBG studies several times with an interval of 6–14 mo. The remaining studies were performed on pediatric patients treated for thyroid medullary carcinoma and other abdominal tumors of an unknown origin.
123I-MIBG Scintigraphy
123I-MIBG was injected intravenously at a dosage of 37–185 MBq (dosage [MBq] was adjusted in each case according to body weight: 37 + 1.5 × body weight [kg]). When possible, patients were pretreated with Lugol’s solution to block the thyroid uptake of free 123I. Imaging was performed 6 and 30 h after the administration of the tracer, using dual-head or triple-head gamma cameras (PRISM 2000XP or PRISM IRIX; Marconi-Phillips) with low-energy, high-resolution collimators. Anterior and posterior whole-body images were scanned at a speed of 7 cm/min. SPECT was performed for either the chest or the abdomen, where the tumor was thought to exist. Tomographic images were acquired with 5° per step of 40 s each, 64 × 64 matrix, and were reconstructed using filtered backprojection with a Butterworth filter. Of all SPECT images acquired for the evaluation of tumor lesions, we investigated only the patients whose whole-body images demonstrated nape-of-the-neck accumulation.
Image Interpretation
Whole-body planar images were evaluated visually. Cases of 123I-MIBG accumulation in the nape-of-the-neck region were classified into the following groups: N, no visible accumulation; 1, mild uptake; 2, moderate uptake less than in the liver that might be misinterpreted as a tumor lesion; 3, more uptake than in the liver; and B, bilateral; U, unilateral). The acquired SPECT images of the upper chest were evaluated to clarify the localization of the accumulation.
Patient Data Analysis
The selected patients with 123I-MIBG accumulations in the nape-of-the-neck region were retrospectively analyzed with regard to the following criteria: age, sex, and the season when the examination was performed. It was confirmed that the accumulation did not correspond to tumorous tissue as assessed by the other imaging modalities (CT, ultrasonography), tumor markers (vanillyl mandelic acid, homovanillic acid, or neuron-specific enolase for neuroblastomas, carcinoembryonic antigen for thyroid medullary carcinoma), or subsequent follow-up 123I-MIBG studies.
RESULTS
Nape-of-the-neck accumulations were observed in 32 of the 266 studies (12%). The numbers of the patients of each group were as follows: N, 234 (88%); 1 B, 25 (9.4%); 1 U, 3 (1.1%); 2 B, 4 (1.5%); 2 U, 0; 3 B, 0; 3 U, 0. Representative images are shown in Figure 1. Patients who were positive for nape-of-the-neck accumulation ranged in age from 6 mo to 4 y (mean ± SE, 2.3 ± 1.8 y), and no study performed on patients >5 y old showed the same findings. There was no significant difference in the frequency between boys and girls; 18 were girls, and 14 were boys. All of the positive studies were performed in winter (3 in November, 5 in December, 9 in January, 8 in February, and 7 in March), whereas no similar accumulation was observed in the studies performed in the warm or hot seasons.

123I-MIBG scintigrams (left, anterior image; right, posterior image) of 4-y-old boy who had been treated for neuroblastoma show string-like accumulations on bilateral nape of neck (arrows). Subsequent studies, including CT and tumor markers, failed to detect any evidence of tumors at same site.
Chest SPECT was performed in 4 of the 32 positive studies. In the SPECT images, the accumulation was localized in the nape of the neck toward the upper back region with a plate-like shape.
In patients whose 123I-MIBG scintigraphy demonstrated nape-of-the-neck accumulation, the significance of the finding was evaluated by inspection, palpation, and follow-up 123I-MIBG studies in all cases. In 4 patients, additional CT or ultrasonography was performed. In all cases, the accumulations disappeared on subsequent 123I-MIBG scintigrams that were obtained 6–8 mo later (Fig. 2). Additional CT or ultrasound studies did not demonstrate any tumorous lesions.

123I-MIBG scintigrams obtained in February (A) and follow-up study obtained in August (B) (same case as in Fig. 1). Accumulation observed in winter (arrows) disappeared in summer. Patient had not undergone any treatment between examinations.
The U pattern of accumulation was seen in 3 studies of the same individual, whose resected neuroblastoma had originated from the left thoracic sympathetic nerve trunk. After the operation, the patient had symptoms of heat in the left hand and chest due to a lack of perspiration, thought to be Horner’s syndrome. There was laterality in his 123I-MIBG accumulation in the chest, more intense in the right than in the left side. The SPECT images clearly demonstrated the difference of nape-of-the-neck accumulation between the right and left side (Fig. 3).

123I-MIBG scintigrams. (A) Whole-body scan. (B) SPECT sagittal image (upper) and SPECT coronal image (lower) of 2-y-old boy, who had suffered from Horner’s syndrome after operation for tumor originating in thoracic sympathetic nervous trunk. There is laterality in accumulation in chest. SPECT demonstrated apparent nape-of-neck accumulation only on right (healthy) side (arrows).
DISCUSSION
In children, normal patterns of MIBG distribution sometimes have peculiarities, which may be misinterpreted as tumor-related lesions. In our study, 32 of 266 123I-MIBG examinations in children (12%) demonstrated accumulation in the nape-of-the-neck region, which did not correspond to tumorous tissue. All of the positive results were obtained in studies performed in winter, and the accumulation varied with each examination, even in the same individual.
In our experience, the same accumulation has seldom been demonstrated in similar studies on adults. Some authors have reported similar observations (7–9). Bonnin et al. reported physiologic accumulations in the bilateral upper thorax of some children (7). Lumbroso et al. reported bilateral symmetric supraclavicular MIBG accumulation, which disappeared in subsequent studies (8). They stated that the accumulation corresponded to the pleural apex. Elgazzar et al. reported the same accumulation in 2 of 31 adult patients, and they attributed this accumulation to the uptake by muscles (9). However, none of these authors presented any evidence of the nature of the accumulation. The focal localization limited to the nape-of-the-neck region made it inappropriate to consider the accumulation in the pleura or muscles. In the view of the significant differences in its incidence between children and adults, and the fact that the accumulation was observed more frequently in winter than in summer, we hypothesized that brown adipose tissue (BAT) contributed to the nape-of-the-neck accumulation.
BAT is one tissue that plays an important role in cold-induced and diet-induced thermogenesis (10,11). The activation of BAT in neonates produces heat to maintain the body temperature against the first exposure to a cold environment (12). The thermogenesis of BAT is regulated mainly by the sympathetic nervous system (13,14) and there are abundant β3-adrenergic receptors (15). During cold acclimation, the sympathetic innervation triggers the recruitment of BAT by hyperplasia, which involves the proliferation and differentiation of precursor cells, and by hypertrophy of BAT (16). In humans, even adults (especially outdoor workers in northern Finland), active BAT plays an important role in thermogenesis (17).
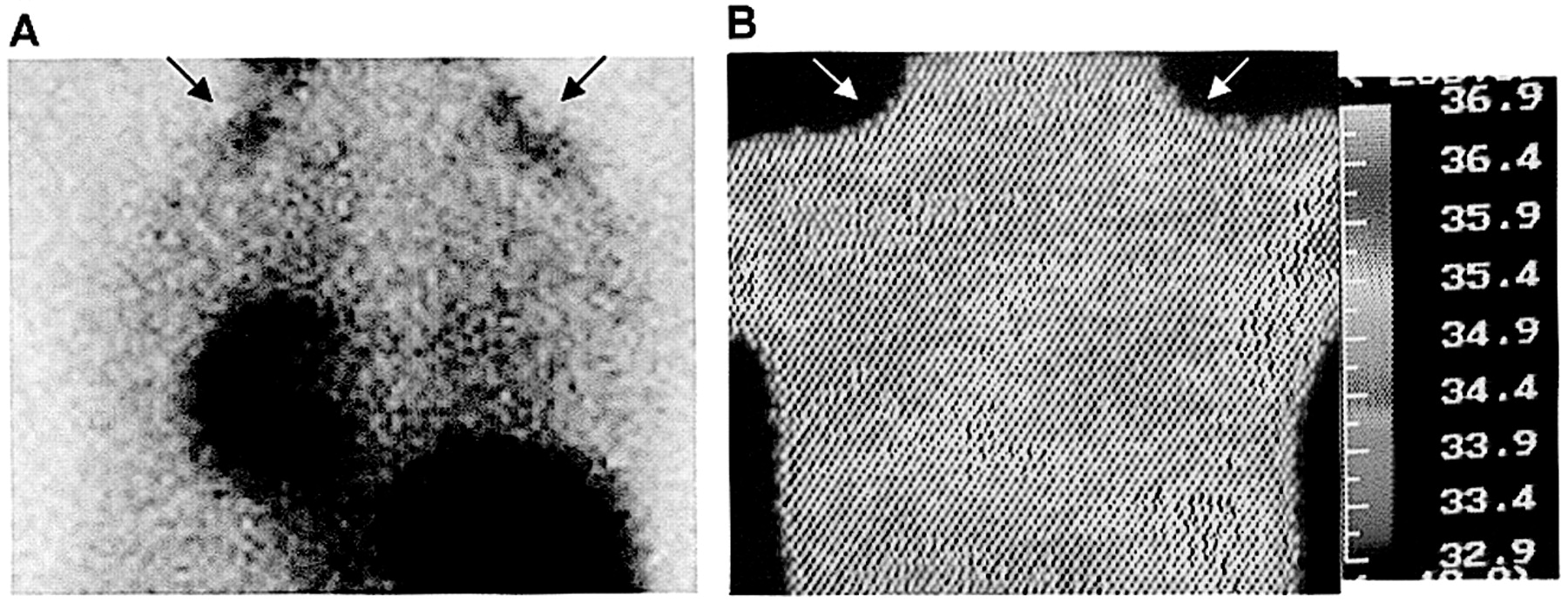
We have already identified physiologic MIBG accumulation in the interscapular BAT (IBAT) of Wistar rats and reported that the percentage injected dose per gram of BAT is as high as that of the heart (18). The accumulation was reduced by the preadministration of 6-hydroxydopamine or reserpine, and activation of the β3-adrenergic receptors increased the accumulation and accelerated the washout of MIBG in BAT. The IBAT was clearly distinguished from the surrounding white adipose tissue on 125I-MIBG autoradiograms. However, we did not perform any imaging coregistration studies on our human subjects. Considering the thermogenic characteristics of BAT, we performed thermography on some patients undergoing 123I-MIBG studies, and we found that the distribution of 123I-MIBG accumulations in the nape of the neck corresponded to the part with a relatively high body temperature (Fig. 4). However, because many factors other than BAT function are thought to contribute to body temperature, we could not find solid evidence that the site of MIBG accumulation on the nape of the neck and posterior neck of human infants and children corresponds to BAT.

123I-MIBG scintigram (A) of 3-y-old girl and her thermogram (B). Distribution of nape-of-neck accumulation resembles distribution of relatively high body temperature (arrows).
Recently, Hany et al. suggested that the symmetrically increased 18F-FDG uptake in the cervical and thoracic spine region is related to BAT (19). In their studies, increased symmetric 18F-FDG uptake in the shoulder region was observed in 17 of 638 patients (2.5%), and the uptake was localized within the fatty tissue of the shoulders as demonstrated by PET/CT coregistration. Cohade et al. also mentioned the same physiologic 18F-FDG uptake and named it “supraclavicular area fat (USA-fat)” (20). In an earlier report, about 123I-MIBG as well, the physiologic source of the 18F-FDG accumulation in the shoulder region was regarded as muscular uptake, because it disappeared after the application of muscle relaxants in subsequent examinations (21). Possibly, because of the superiority of the PET image to single-photon images of 123I, the symmetric accumulation in the shoulder region is clearer than our 123I-MIBG images, and, in some cases, similar accumulations are demonstrated in the neck and the region of the costal-vertebral joints of the thoracic spine. However, the finding of 18F-FDG distribution in the shoulder region, where the accumulation was observed most frequently, resembles the site of 123I-MIBG accumulation in our observations. In the 18F-FDG investigation, the symmetric 18F-FDG uptake in the nonmuscular tissue of the shoulder region was observed more frequently in patients with a low body mass index (BMI) rather than a high BMI; therefore, the authors suggested that BAT could be considered as a factor of the accumulation without confirming the exact nature of 18F-FDG distribution (19,20).
These investigations using 18F-FDG and our previous study using Wistar rats suggest the possibility that 123I-MIBG accumulation of the interscapular region observed in children corresponds to the physiologic accumulation in BAT rather than accumulation in the apical pleura or muscles. This information helps in the interpretation of equivocal MIBG scans.
BAT is thought to be important in metabolism during hibernation, and a comparatively high respiratory activity is maintained even at low temperatures (10–12). Lipids within the brown adipocytes are the primary source of energy, which are directly translated into heat. The BAT mitochondria operate in an uncoupled mode—that is, they reduce their production of adenosine triphosphate (ATP) and increase their oxidation of fatty acids. To compensate for the uncoupling, and to prevent any ATP deficiency, glucose metabolism via anaerobic glycolysis is increased in BAT. Therefore, symmetric 18F-FDG accumulation was interpreted as an increased glucose uptake due to the thermoregulatory system in the BAT. BAT is named for its color, which is attributed to its high vascularity and high cytochrome content, reflecting high mitochondrial density. 99mTc-Labeled myocardial perfusion radiopharmaceuticals—that is, 99mTc-sestamibi and 99mTc-tetrofosmin, which are known to accumulate in mitochondria (22,23)—can be expected to visualize activated BAT.
Recently, further concern has arisen with BAT in terms of its relationship to obesity than to thermogenesis in the infantile period (24). A subgroup of obese persons has low BAT activity, and a mutation of the β3-adrenoreceptor gene is known to cause refractory diabetes mellitus (25). In the study using 18F-FDG, BAT accumulation was increased in underweight patients (19). Our experiments using Wistar rats confirmed that the sympathetic nervous system really contributes to the MIBG uptake in the BAT and a high concentration was elucidated (18). Though the accumulation in the nape-of-the-neck region cannot usually be seen in adults, and even in children it is obscure compared with the accumulation of 18F-FDG, the activation methods using cold exposure, overeating, or β3-stimulation may enable the in vivo estimation of the function of BAT using 123I-MIBG. In the future, the proper management of radiopharmaceuticals—namely, 123I-MIBG (which demonstrates the function of the sympathetic nervous system that plays a primary role in the fundamental control of the BAT), 18F-FDG (which shows the metabolic state of the activated BAT), and 99mTc-sestamibi or 99mTc-tetrofosmin (whose accumulation reflects the vascularity and the density of mitochondria)—may help in the diagnosis of the potentiality of obesity-related characteristics.
CONCLUSION
The characteristics of 123I-MIBG accumulations in the nape-of-the-neck region were investigated. Accumulation, which did not correspond to any tumor, was seen in 32 of 266 studies (12%). The observation was limited in the studies performed on young children in winter. Therefore, the accumulation is thought to be related to active BAT, which is in accordance with our previous animal experimental data.
Footnotes
Received Dec. 31, 2002; revision accepted Apr. 21, 2003.
For correspondence or reprints contact: Chio Okuyama, MD, PhD, Department of Radiology, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, 465 Kajiicho, Kawaramachi Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan.
E-mail: chio{at}koto.kpu-m.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Perspectives on Brown Adipose Tissue Imaging: Insights from Preclinical and Clinical Observations from the Last and Current Century
- Combining 123I-Metaiodobenzylguanidine SPECT/CT and 18F-FDG PET/CT for the Assessment of Brown Adipose Tissue Activity in Humans During Cold Exposure
- A novel approach for reduction of brown fat uptake on FDG PET
- Comparison of Uptake of Multiple Clinical Radiotracers into Brown Adipose Tissue Under Cold-Stimulated and Nonstimulated Conditions
- Brown Fat Imaging with 18F-6-Fluorodopamine PET/CT, 18F-FDG PET/CT, and 123I-MIBG SPECT: A Study of Patients Being Evaluated for Pheochromocytoma
- Brown Adipose Tissue and Nuclear Medicine Imaging