


Abstract
Peritoneal carcinomatosis can be difficult to diagnose, as CT is insensitive, with peritoneal biopsy and lavage often subject to problems of sampling error. The aim of our study was to evaluate the role of 18F-FDG PET in detecting peritoneal carcinomatosis in patients with stomach, ovarian, and adrenal cancer and mesothelioma and to compare the results with CT scans in the same patient group. Our secondary aim was to identify characteristic patterns of abdominal 18F-FDG uptake in biopsy-proven peritoneal disease and to correlate these patterns with available histologic and anatomic findings after surgery and structural imaging. Methods: The medical records of 88 patients with stomach (n = 48), ovarian (n = 13), and adrenal cancer (n = 6) and mesothelioma (n = 21) were reviewed for the presence of peritoneal tumor on 18F-FDG PET and CT scans. The results were correlated with either contemporaneous peritoneal biopsy or ascitic aspirate or with radiographic or clinical follow-up if histology was negative or unavailable. Of 24 patients with suspected peritoneal tumor, 17 had biopsy-proven findings of peritoneal disease. Results: Of the 24 patients with suspected peritoneal tumor, 18F-FDG PET was positive in 14 patients, with 1 of these scans being false-positive, CT was positive in 10 patients, and either PET or CT was positive in 18 patients. This yielded sensitivities of 57% (13/23), 42% (10/23), and 78% (18/23), with uniformly high positive predictive values of 93% (13/14), 100% (10/10), and 95% (18/19), respectively. We identified 2 distinctly abnormal scintigraphic patterns of focal and uniform 18F-FDG uptake corresponding to nodular and diffuse peritoneal disease on pathologic examination. Conclusion: 18F-FDG PET adds to conventional imaging in the staging of peritoneal carcinomatosis. It is also a useful diagnostic tool when peritoneal biopsy is either unavailable or inappropriate. We have identified 2 distinct scintigraphic patterns that appear to predict the presence of either nodular or diffuse peritoneal pathology.
The peritoneum is a preferred site of metastasis of several primary malignancies, principally colorectal carcinoma in men and ovarian cancer in women, as well as primary gastric, pancreatic, and adrenocortical carcinoma. Distant metastases to the peritoneum from malignant melanoma and from breast and lung carcinoma are also not uncommon. The peritoneum may also be affected by primary tumors, the most common being mesothelioma, which may arise in the peritoneum or may metastasize there from the pleura.
The presence of peritoneal tumor alters tumor staging, with implications regarding primary treatment and patient outcome. Peritoneal involvement is one of the most significant prognostic indicators in ovarian carcinoma (1) and, in colorectal carcinoma, has the greatest independent prognostic significance, more powerful than the extent of local spread or lymph node involvement (2). Early diagnosis of peritoneal tumor is important because low-volume disease may be suitable for cytoreduction before surgery (3). In the posttreatment setting, accurate monitoring of tumor response to chemotherapy and detection of tumor recurrence is critical in planning the management algorithm. Peritoneal disease, however, may remain occult for some time because imaging procedures can be variable in their detection of tumor deposits, with laparoscopic techniques limited by sampling error (4). CT, the preoperative gold standard for detection of peritoneal carcinomatosis, has varying reported sensitivities depending on factors such as size, site, and morphology of tumor deposit, presence of ascites, paucity of intraabdominal fat, adequacy of bowel opacification, and concomitant use of peritoneography (5–7). Some recent studies have demonstrated improved lesion detection with MRI (6,8,9), although others have not confirmed this (10).
At our center, staging 18F-FDG PET scans are performed on numerous patients with a variety of primary malignancies. Not infrequently, we identify metabolic abnormalities within the abdomen and pelvis suspicious for tumor, which correspond to CT findings of peritoneal disease.
The aim of our study was to assess the role of 18F-FDG PET in the evaluation of peritoneal carcinomatosis in patients with various malignancies and to compare the results of 18F-FDG PET with CT scans in the same patient group. In addition, we set out to identify the metabolic patterns of 18F-FDG PET uptake in patients with biopsy-proven disease and to correlate these patterns with both structural imaging and histologic examination in an attempt to identify features that were likely to have influenced the appearance and sensitivity of the PET scan.
MATERIALS AND METHODS
Patients
We conducted a retrospective review of the medical records of patients who were referred for staging 18F-FDG PET scans from 1996 to 1999 for evaluation of various tumors. A total of 88 patients with gastric (n = 48), ovarian (n = 13), and adrenocortical (n = 6) carcinoma and mesothelioma (n = 21) were included in the study as these primary tumors have a known predilection for the peritoneum and commonly presented to our department. Patients with colorectal carcinoma were excluded from this study because they were to be evaluated in a future, larger, prospective study. There were 50 men and 38 women, ages ranging from 28 to 84 y (mean age, 54 y).
Reports of the patients’ 18F-FDG PET and CT scans were reviewed for the presence of peritoneal tumor and were compared with available results of peritoneal biopsy or fine-needle aspiration of ascitic fluid as the gold standard. When biopsy was negative or had not been performed, clinical or colocated radiographic evidence of peritoneal disease on patient follow-up was used. A final diagnosis of peritoneal carcinomatosis was made if suspicious PET or CT scans had coexistent evidence of disease either on pathologic examination or on radiographic or clinical follow-up. Sensitivities and positive predictive values for PET and CT were subsequently determined.
In addition, where histologic evidence was available, we reviewed the operative notes and pathology reports in detail for tumor size, morphology, density, and degree of tumor differentiation and other features to determine if these factors may have influenced the appearance of the PET study.
Imaging
All 18F-FDG PET scans were performed on a high-resolution dedicated whole-body PET camera, GE ADVANCE (General Electric Medical Systems), consisting of 336 bismuth germanate detector units arranged to form 18 rings. The average axial resolution (full width at half maximum) is 4.0 mm at r = 0 cm, 5.5 mm at r = 10 cm, and 6.6 mm at r = 20 cm. Total system sensitivity is 6 kcps/Bq/mL (223 kcps/μCi/mL) with septa in and 32 kcps/Bq/mL (1,200 kcps/μCi/mL) with septa out (11). Scanning was generally performed from the neck to the proximal thighs. In 1 patient, scanning included the chest and upper abdomen only. Emission studies were commenced approximately 45 min after the intravenous administration of 370 MBq 18F-FDG followed by a transmission study covering the same area. Studies were reconstructed using filtered backprojection alone or with iterative reconstruction and segmented attenuation correction. All patients had CT scans of the abdomen and pelvis, which were correlated with the PET scan.
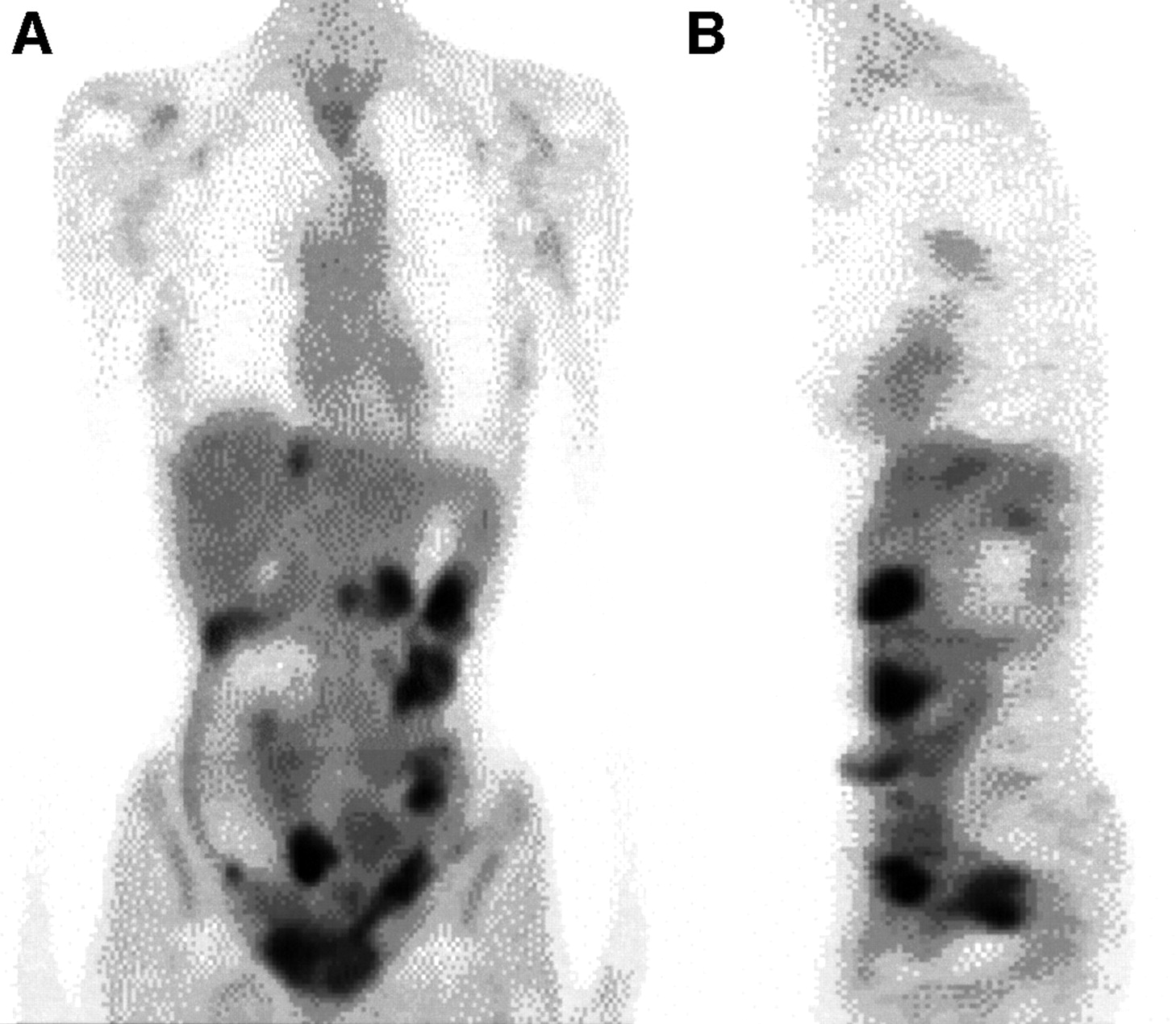
Peritoneal tumor was suspected on 18F-FDG PET when certain focal or diffuse metabolic abnormalities were identified in the abdomen or pelvis. Focal abnormalities were considered positive for peritoneal tumor if discrete foci of increased 18F-FDG metabolism were located randomly and anteriorly within the abdomen or dependently within the pelvis, unrelated to solid viscera or nodal stations (Fig. 1A). The anterior location of these lesions within the abdomen was often best appreciated on the sagittal image (Fig. 1B).

An 80-y-old woman with stage IIIC ovarian carcinoma after 6 cycles of neoadjuvant chemotherapy. Preoperative 18F-FDG PET scan shows focal pattern of peritoneal carcinomatosis. (A) Coronal section demonstrates hypermetabolic foci distributed randomly throughout abdomen and pelvis, unrelated to solid viscera or nodal stations. (B) Sagittal section demonstrates their typical anterior location. After debulking procedure, including total abdominal hysterectomy and bilateral salpingo-oophorectomy and partial omentectomy, peritoneal implants progressed on subsequent PET scans.
Foci of 18F-FDG uptake confined only to the posterior abdomen or pelvis, clustered in the region of the celiac, paraaortic, or iliac nodal stations, suggested nodal metastases and were not included in the study.
The pattern of diffuse, low-grade glucose hypermetabolism spreading uniformly throughout the abdomen and pelvis obscuring visceral outlines—particularly the normal serpiginous pattern of the large and small bowel and physiologic hepatic and splenic uptake—was also suggestive of peritoneal tumor (Fig. 2).

A 47-y-old woman with poorly differentiated adenocarcinoma of stomach (linitis plastica type), 6 mo after sub-total gastrectomy, with persistent nausea and vomiting, referred for exclusion of disease recurrence. 18F-FDG PET scan, coronal section, demonstrates metabolic pattern characteristic of diffuse peritoneal carcinomatosis with uniform low-grade 18F-FDG uptake throughout entire abdomen and pelvis obscuring normal, discrete, visceral outlines, particularly bowel, liver, and spleen. Her demise was precipitated by gastric outlet obstruction and progressive cachexia.
CT scans were suggestive of peritoneal tumor if they demonstrated infiltration, thickening, or studding of the peritoneum, bowel wall, mesentery, or omentum with or without ascites. Neither ascites alone nor the presence of abdominal or pelvic lymphadenopathy was considered representative of peritoneal carcinomatosis.
A PET scan was true-positive if findings suggestive of peritoneal tumor, as described above, were confirmed by a positive tissue diagnosis or clinical or colocated radiographic abnormalities on subsequent follow-up; a PET scan was true-negative if neither the PET study, histology, radiographic, nor clinical follow-up demonstrated peritoneal carcinomatosis. A PET scan was false-positive if it demonstrated findings suggestive of peritoneal carcinomatosis, with negative findings on pathology and follow-up; a PET scan was false-negative if either histology or follow-up demonstrated evidence of peritoneal tumor, whereas the PET study remained negative.
A CT scan was true-positive if it demonstrated findings of peritoneal disease that were confirmed by peritoneal pathology; other radiographic findings, including PET; or clinical follow-up. A false-positive CT scan was characterized by positive findings of peritoneal tumor that were not supported by other evidence of peritoneal disease. A true-negative CT scan occurred when other correlative investigations failed to identify peritoneal disease. If a CT scan was negative for peritoneal disease, whereas other investigations such as peritoneal pathology, radiographic, PET or clinical follow-up suggested otherwise, this constituted a false-negative CT scan.
RESULTS
Peritoneal tumor was suspected in 24 of the 88 patients on the basis of the 18F-FDG PET or CT scan. A final diagnosis of peritoneal tumor was made in 23 patients based on peritoneal biopsy or cytology of ascitic fluid or on radiographic or clinical follow-up. Seventeen of the 23 patients had histologic confirmation of peritoneal disease. A further 6 patients (2 with a negative biopsy, 4 without concurrent biopsy) were diagnosed with peritoneal disease on the basis of radiographic or clinical follow-up. Of these 6 patients, 3 had progressive peritoneal disease demonstrated on serial CT scanning alone, 2 patients had progressive CT scans in addition to worsening abdominal symptomatology and positive aspiration cytology performed at 13 and 20 mo after the PET scan, and 1 patient had a positive 111In-satumomab pendetide (OncoScint CR/OV; Cytogen Corp.) scan.
18F-FDG PET was positive in 13 of the 23 patients who were ultimately diagnosed with peritoneal disease: confirmed in 8 patients by biopsy, by radiographic follow-up in 4 patients, and in 1 patient by combined clinical and radiographic follow-up. In 1 patient, although peritoneal tumor was suspected on 18F-FDG PET, other investigations did not confirm this suspicion. The other 10 of the 23 patients who were diagnosed with peritoneal disease demonstrated a negative PET scan. These findings yielded 13 true-positive, 10 false-negative, and 1 false-positive result on PET imaging.
CT was positive for peritoneal carcinomatosis in 10 of the 23 patients diagnosed with peritoneal disease, this result being confirmed by biopsy and by radiographic and combined clinical and radiographic follow-up in 7, 2, and 1 patient, respectively. CT was negative for peritoneal carcinomatosis in the remaining 13 of the 23 patients, yielding 10 true-positive, 1 true-negative, 13 false-negative, and no false-positive results on CT imaging.
When PET was evaluated together with CT, there were 18 true-positive, 5 false-negative, and 1 false-positive result.
Sensitivities for PET, CT, and both modalities together were 57%, 43%, and 78%, respectively. The positive predictive values for 18F-FDG PET and CT in detecting peritoneal carcinomatosis in our patient group were 93% and 100%. When PET and CT scans were evaluated together, not only was sensitivity increased but also a high positive predictive value of 95% was maintained (Table 1).
Imaging Results in Peritoneal Carcinomatosis
A total of 10 patients had congruent PET and CT findings, 5 positive and 5 negative for peritoneal disease. The remaining 14 patients had incongruent findings on PET and CT. Of this group, PET was positive in 9 patients who had a negative CT scan (only 1 of these PET scans was false-positive), and CT was true-positive in 5 patients with a negative PET scan. Had either the PET scan or the CT scan been evaluated alone, 13 patients may have been misdiagnosed on the basis of their imaging findings.
The peritoneum was not surgically explored in 64 of the initial 88 patients because of the retrospective nature of this study. As such, biopsy confirmation of peritoneal normality was not available, and neither a true-negative nor a false-positive status in this group could be accurately established.
18F-FDG PET Patterns
In the 8 PET-positive studies with histologic diagnosis of peritoneal tumor, we identified 2 distinctively abnormal, but entirely different, patterns of glucose metabolism on 18F-FDG PET within the abdomen, which suggested 2 different forms of malignant tumor invasion. A nodular pattern was identified in 6 patients, whereas 2 patients demonstrated a diffuse metabolic pattern, corresponding to focal, nodular and diffuse, infiltrative peritoneal involvement, respectively, seen on concurrent CT scans and subsequent biopsy specimen (Figs. 1 and 2).
Lesion Characteristics and PET Detectability
We identified a strong correlation between 18F-FDG PET positivity and certain histologic features that were likely to have influenced the appearance and sensitivity of the PET scan. The 8 PET-positive individuals with histologically proven peritoneal tumor at surgical exploration had mostly a large volume of disease, with extensive involvement of tumor into adjacent soft tissues such as omentum, mesentery, and fibroadipose tissue. In 4 patients, resected tumor nodules that were available for pathologic inspection were large, measuring 0.5–4.0 cm (average dimension, 1.2 cm). Small nodules were visualized when they were clustered in aggregates of >0.5 cm, which was the case in 1 patient. Four of these 8 patients had tumor involving adjacent soft tissues (such as omentum and fibroadipose tissue), 2 patients had a poorly differentiated histology, and 1 patient with the diffuse pattern of peritoneal spread on PET imaging demonstrated diffuse and extensive gastric tumor of the linitus plastica type, infiltrating surrounding organs, without nodularity.
Of the 10 false-negative cases on PET imaging, 9 had biopsy correlation, which demonstrated low-volume disease in all patients. Peritoneal implants were typically small, ranging from 0.2 to 0.5 cm (average diameter, 0.3 cm). Foci were microscopic in 1 patient and flat in another patient, and in 3 patients microscopic disease was limited to the ascitic fluid; the morphologic characteristics of most of these foci were clearly below the resolving power of the PET camera.
Not all true-positive or false-negative PET patients had pathologic confirmation, with some diagnoses being made on the basis of follow-up. As such, in these patients the PET scan appearance could not be correlated with specific lesion characteristics.
DISCUSSION
Peritoneal tumor deposits are often low in volume, are individually small, and may be few in number and variable in their gross morphology, developing either as discrete masses or smaller nodules, studs, flat plaques or large sheets of tumor only several cells thick (12). Early disease may be microscopic and limited only to the ascitic fluid. More advanced disease may extend along the parietal peritoneum, stud visceral surfaces, or cause omental or mesenteric caking (13). Peritoneal tumor seeding may be a result of hematogenous, lymphatic, or direct local spread (13). Such variability in tumor morphology, site, and mode of spread within the abdomen may help to explain why the diagnosis of peritoneal carcinomatosis remains a challenge.
Open laparotomy with peritoneal biopsy is the gold standard for diagnosis of peritoneal carcinomatosis, because the peritoneum may be assessed visually and examined carefully by hand. Although a greater number of diagnostic biopsies may be performed and ascitic fluid easily sampled, this technique is invasive. Some authors have described metastases along the laparoscopic tracts in some patients, suggesting seeding at the time of surgery (14). Laparascopic staging is commonly used in staging of patients at diagnosis (4), but its invasive nature suggests a limited role in regular patient follow-up.
Conventional CT scanning, currently the preoperative imaging procedure of choice for diagnosis of peritoneal metastases, has varying sensitivity with study results ranging widely from 17% (5) to 54% (6), but usually falling in the lower range (7,13). More reliable detection of tumor with CT may depend on site, size, and tumor morphology as well as other features. Gryspeerdt et al. reported an overall sensitivity of 38% for CT in the diagnosis of peritoneal metastases with higher sensitivities for tumors located paravertebrally or in the right paracolic gutter. Nodular lesions were more easily detected than flat lesions (100% vs. 21% detection) and were less commonly detected if associated with omental metastases, ascites, or history of prior abdominal surgery (7). Adachi et al. reported (15) that peritoneal and nodal metastases could be overlooked on CT examinations in patients with advanced gastric cancer. Double-contrast MRI (6), CT peritoneography (6), and video-laparoscopic staging (16) have yielded higher sensitivity, specificity, and accuracy than conventional CT. However, CT remains widely available at most centers, is less expensive than other imaging modalities, and is less invasive than surgical procedures.
The role of MRI in peritoneal carcinomatosis is still under evaluation. Recent reports (17,18) suggest that reasonable accuracy can be achieved, however, often at a cost of significant patient preparation and use of specific imaging sequences. As such, it has so far been unable to replace CT as the gold standard for preoperative evaluation of peritoneal carcinomatosis. Low et al. (6) report a sensitivity of peritoneal metastasis detection of 85% with delayed, gadolinium-enhanced, breath-hold, fast, mutiplanar sequence with fat saturation with gradient-recalled acquisition in the steady state compared with a sensitivity of 33% for standard T1-weighted sequences. Others (8) have reported sensitivities of 91% when artifact reduction and peritoneal contrast enhancement are performed. One study reports comparable MRI and CT results in the detection of peritoneal spread in pancreatic (10) and ovarian carcinoma with accuracy for both of approximately 70% (19). Others report complete nonvisualization of peritoneal implants in ovarian cancer with CT or MRI, either in the mesentery or in the small bowel wall (20).
Although the role of 18F-FDG PET in the evaluation of the peritoneal tumors is not yet established, experience is increasing, largely in metastatic tumors. Tanaka et al. (21) have demonstrated sensitivities far superior to CT in the evaluation of colorectal tumor peritoneal recurrence in a retrospective study. The results in the evaluation of other tumors (18,22) appear similarly promising.
Our study demonstrates a limited sensitivity for detection of peritoneal carcinomatosis with 18F-FDG PET or CT scanning alone (57% and 43%, respectively). Adding PET to CT increased sensitivity further (78.0%) than could have been achieved with either modality, while maintaining a high positive predictive value (95%).
This result strongly suggests that, in an appropriate clinical setting, an abnormal metabolic pattern in the peritoneum can rule in a diagnosis of peritoneal disease, even though little can be said about a negative study.
One of our patients had a false-positive 18F-FDG PET scan, with sampling error most likely responsible for this result. In this patient, the PET scan was strongly positive for nodular disease at multiple sites in the abdomen, including the peritoneum. Only a peritoneal tap had been performed without biopsy. Accurate CT-guided localization and biopsy may have confirmed the true-positive status of this patient and, hence, improved sensitivity as well as increasing the positive predictive value of PET to 100%.
Familiarity with the patient’s history as well as the metastatic characteristics of tumor—whether the peritoneum is a preferred site—and histologic staging of the primary tumor at diagnosis may all help to determine the pre-test likelihood of peritoneal metastasis.
Knowledge of the diverse morphologies of peritoneal tumor also is critical and, in our patients, contributed to the recognition of 2 distinct patterns of abdominal 18F-FDG uptake, typical of nodular and diffuse peritoneal disease on pathologic examination. We believe that familiarization with these 2 patterns of glucose metabolism is important in increasing detectability and diagnostic accuracy of peritoneal carcinomatosis with PET and, particularly, to distinguish tumor from physiologic activity of other abdominal viscera.
The study had some limitations. Because of the retrospective nature of this study, we were unable to obtain histologic data on all patients. In fact, 64 of the initial 88 patients were excluded on the basis of missing peritoneal biopsy or ascitic tap, with follow-up also inadequate in many. Although most patients in this group did not have a PET scan with suspicious finding(s), CT abnormalities did occur and they could not be corroborated with a suitable gold standard. Without an accurate true-negative value, neither specificity nor negative predictive value could be determined. To resolve these issues, a large, prospective study is a goal of future research in this area, including other tumors where peritoneal implants are more common, such as colorectal carcinoma. Indeed, up to 50% of all patients undergoing further surgery for recurrent colorectal carcinoma have been reported with peritoneal seeding (23). This study would also aim to include larger patient numbers; accurate, contemporaneous, and targeted biopsies in all patients; and CT scans timed to the PET images or acquired simultaneously with PET/CT hybrid cameras to provide more accurate information and, therefore, greater statistical power.
CONCLUSION
Evaluation of peritoneal carcinomatosis with 18F-FDG PET is possible and rewarding. Our study demonstrates that 18F-FDG PET adds substantially to CT scanning in the detection of this disease. It is a useful diagnostic tool when peritoneal biopsy is either unavailable or inappropriate. We have identified 2 distinct patterns of glucose metabolism that appear to predict either nodular or diffuse peritoneal pathology and should alert the clinician to the possibility of peritoneal carcinomatosis in the appropriate clinical setting. We believe that awareness of these metabolic patterns is crucial for accurate interpretation of both abnormal and physiologic metabolic findings in the abdomen and pelvis when cancer patients are staged with 18F-FDG PET.
Footnotes
Received Dec. 16, 2002; revision accepted May 1, 2003.
For correspondence contact: Alla Turlakow, MD, Department of Nuclear Medicine, Alfred Hospital, Commercial Rd., Prahran, Victoria 3181, Australia.
E-mail: aturlakow{at}ozemail.com.au
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 68Ga-FAPI-04 positron emission tomography/CT and laparoscopy for the diagnosis of occult peritoneal metastasis in newly diagnosed locally advanced gastric cancer: study protocol of a single-centre prospective cohort study
- Accuracy of FDG-PET/CT in Colorectal Peritoneal Carcinomatosis: Potential Tool for Evaluation of Chemotherapeutic Response
- The Role of 18F-FDG PET in Assessing Therapy Response in Cancer of the Cervix and Ovaries
- The Role of 18F-FDG PET/CT in the Evaluation of Ascites of Undetermined Origin
- Accuracy of endoscopic ultrasonography in diagnosing ascites and predicting peritoneal metastases in gastric cancer patients
- Oncologic Imaging in Gynecologic Malignancies
- Comparison Between 18F-FDG PET, In-Line PET/CT, and Software Fusion for Restaging of Recurrent Colorectal Cancer