


Abstract
18F-FDG PET imaging is underutilized in patients with gynecologic malignancies, and its role in current clinical practice has yet to be established. In cervical cancer, it has high sensitivity in detection of nodal disease. Its use is probably most suitable in patients with negative or ambiguous findings on other types of radiographic imaging. Data support its usefulness in asymptomatic cervical cancer patients with high tumor markers and negative conventional-imaging findings, although more data are needed to ascertain whether it has a positive impact on survival. Similarly, its role in monitoring response to therapies needs to be consolidated. In ovarian cancer, 18F-FDG PET holds promise in evaluation of recurrent or residual disease when other radiographic data are uncertain. In endometrial cancer, there are encouraging, although limited, data supporting the use of 18F-FDG PET in patients with recurrent disease. To reduce extensive lymph node dissection in patients and to decrease subsequent morbidity, investigators have advocated applying the sentinel node technique to patients with cervical, endometrial, or vulvar cancers. The overall results are encouraging for the use of LS in planning surgical procedures, although more data and larger planned studies are needed to establish clinical utility in the surgical management of patients with these malignancies.
Gynecologic malignancy is a leading cause of cancer in women and constitutes a significant health issue worldwide. It accounts for approximately 20% of visceral cancers. In 2003, 83,700 gynecologic malignancies were newly diagnosed and 26,800 patients died (1). Although uterine cancer has the highest incidence of all gynecologic malignancies, ovarian cancer has the highest mortality.
Ultrasound, CT, and MRI are routinely used to initially diagnose these tumors and to help stage the disease before specific therapy begins. 18F-FDG PET detects the increased metabolism associated with these lesions. 18F-FDG PET can detect tumor involvement in lymph nodes of normal size and is particularly useful to identify disease in patients in whom normal anatomic landmarks have been lost because of surgery or radiation.
18F-FDG PET is particularly useful because it evaluates the whole body in a single examination, thereby detecting both local and distant involvement. Technologic advances have led to the development of hybrid PET/CT systems that concurrently acquire physiologic and anatomic information, maximizing coregistration and improving lesion localization and specificity, particularly in abdominopelvic malignancies (2).
In this article, the role of PET using 18F-FDG and other tracers in malignancies of the female reproductive tract is reviewed. The use of lymphoscintigraphy for detecting sentinel nodes, another imaging tool with potential, is also outlined.
NORMAL VARIANTS AND LIMITATIONS
The radiolabeled glucose analog 18F-FDG is the most commonly used tracer for imaging tumors. 18F-FDG enters the cells via glucose transporters, in a manner similar to glucose, and accumulates intracellularly after phosphorylation because it cannot undergo further metabolism. Accumulation in cells is related to the rate of cellular metabolism and, thus, the malignant potential.
Applying 18F-FDG PET in the abdominopelvic region is especially challenging because physiologic activity in the bowel and ureters can be difficult to distinguish from sites of tumor from peritoneal, omental, and mesenteric disease or nodal involvement. Increased uptake of 18F-FDG can also be seen in benign lesions and physiologic conditions such as ovulation and menstruation (3). Serous and mucinous cyst adenoma, corpus luteal cyst, dermoid cyst, endometriosis, inflammation, teratoma, and schwannoma can take up 18F-FDG and lead to false-positive findings in ovaries (4–6). It is difficult to differentiate between benign and malignant lesions using PET alone because lesional uptake may be high and the standardized uptake values (SUVs) of malignant and benign lesions overlap. Therefore, the distinction must be made through a detailed clinical history and correlation with corresponding CT. Demonstration of an ovarian cyst on CT and correlation with menstrual history can help in distinguishing the cyst as functional.
Increased physiologic endometrial 18F-FDG uptake in a menstruating patient has previously been reported (7). Lerman et al. studied 246 pre- and postmenopausal women without gynecologic tumors, for patterns of uptake during the 4 phases of the menstrual cycle. Increased endometrial uptake of 18F-FDG was seen during the menstruation and ovulation phases, in benign endometrial abnormalities, and in oligomenorrhea. No significant increase was associated with contraceptives or hormonal therapy. Increased ovarian uptake was detected in 21 premenopausal patients of whom 15 were at mid cycle and 3 reported oligomenorrhea. An ovarian SUV of 7.9 separated benign from malignant uptake with a sensitivity of 57% and a specificity of 95% (8).
The normal menstrual cycle is controlled by the proliferative actions of estrogen and the secretory-transforming effect of progesterone on the endometrium. The first half of the uterine cycle is characterized by more glycolysis under the stimulation of estrogen and glycogen synthetase activity, whereas the second half is characterized by breakdown of glucose under glycogen phosphorylase activity, leading to decreased glycogen levels toward the end of the cycle. The normal balance of synthesis and breakdown of glycogen is disturbed in patients with abnormal functional or pathologic uterine bleeding, leading to increased retention of glycogen and increased activity of glucose-6 phosphate dehydrogenase (9).
Endometrial uptake in postmenopausal women and in nonovulating, nonmenstruating premenopausal women taking oral contraceptives appears to be similar and related to the suppressive effect of oral contraceptives on the endometrial glands and atrophic changes or quiescent state (10).
CERVICAL CANCER
Although the incidence of cervical cancer has decreased over the last few decades, predominantly because of efficient screening procedures such as the Pap test, it is now estimated to be the second most commonly diagnosed cancer in women worldwide and the third most common gynecologic cancer in the United States, with 12,200 new cases and 4,100 deaths in 2003. In the West, most cases are diagnosed early, with almost 47% of invasive cases detected before the age of 35 y. About 10% of patients are more than 65 y old and are more likely to die of the disease because it is not diagnosed until more advanced (11). Risk factors include low socioeconomic class, age at onset of sexual activity, cigarette smoking, oral contraceptives, and human papilloma virus infection. In premenopausal patients, symptoms include intermenstrual bleeding, metrorrhagia, and postcoital bleeding.
In advanced cancers, symptoms of bowel or urinary tract obstruction may be seen at presentation. The disease is staged clinically according to the International Federation of Gynecology and Obstetrics (FIGO) system (12). Histology and imaging studies such as chest radiography, CT, or MRI are routinely used for staging, whereas use of intravenous pyelography and barium enema is usually restricted to selected patients.
In advanced disease, surgical staging is preferred for the assessment of pelvic and aortic lymph node involvement. Scalene nodes can be involved and are seen in about 0%–17% patients who have aortic node disease. Because bone metastases occur infrequently, bone scans are not routinely indicated and are used only in those with bone pain. CT scans provide high-resolution anatomic detail and have become an important part of routine staging. Cervix, uterus, parametrium, adnexa, nodes, and distant organs such as liver and lung can be evaluated with high sensitivity. Subcentimeter disease, however, cannot be detected reliably, because the detection criteria are based on size and often lead to understaging. MRI can predict endometrial involvement in about 84%–96% of cases, as opposed to 55%–80% by CT, and has a high negative predictive value (13–15). Aortic nodal metastasis can be detected with high specificity; however, the sensitivity is only 50% (16). 18F-FDG PET was approved for coverage in January by the Centers for Medicare and Medicaid Services for initial staging of cervical cancer in patients with CT or MRI findings negative for extrapelvic metastatic disease.
Uptake of 18F-FDG in cervical cancer appears to be related to GLUT-1 expression; however, no correlation has been established between SUV or GLUT-1 expression, initial grade of histologic differentiation, and FIGO stage. Higher GLUT-1 expression is seen in recurrent or persistent disease than in metastatic lymph nodes (17).
18F-FDG PET (Fig. 1) is accurate for initial staging, has high sensitivity for detecting distant metastases in restaging, and helps stratify patients for therapy. In a retrospective analysis (n = 41), 18F-FDG PET showed 100% accuracy in detecting disease for initial staging. Restaging sensitivity was 82% and specificity 97% (18). Although MRI provides excellent evaluation of local tumor and parametrial involvement, 18F-FDG PET is more useful for the evaluation of pelvic lymph nodes, though microscopic disease is missed by both (19). Larger scanning areas permit estimation of extrapelvic disease and distant metastases. Tran et al. detected supraclavicular nodal involvement in about 8% of patients, with a positive predictive value of 100% (20). The overall survival for these patients was low, averaging about 7.5 mo. Sensitivity and specificity for detection of recurrence is reported to be up to 86% and 94%, respectively (21). In another study, with 27 patients (22), the sensitivity and specificity of 18F-FDG PET for detecting recurrent cervical cancer were 85.7% and 86.7%, respectively. The positive and negative predictive values were 85.7% and 86.7%, respectively. Detection of small-volume disease is limited because of the lack of resolution; peritoneal disease can, however, be detected when metabolically active (23).
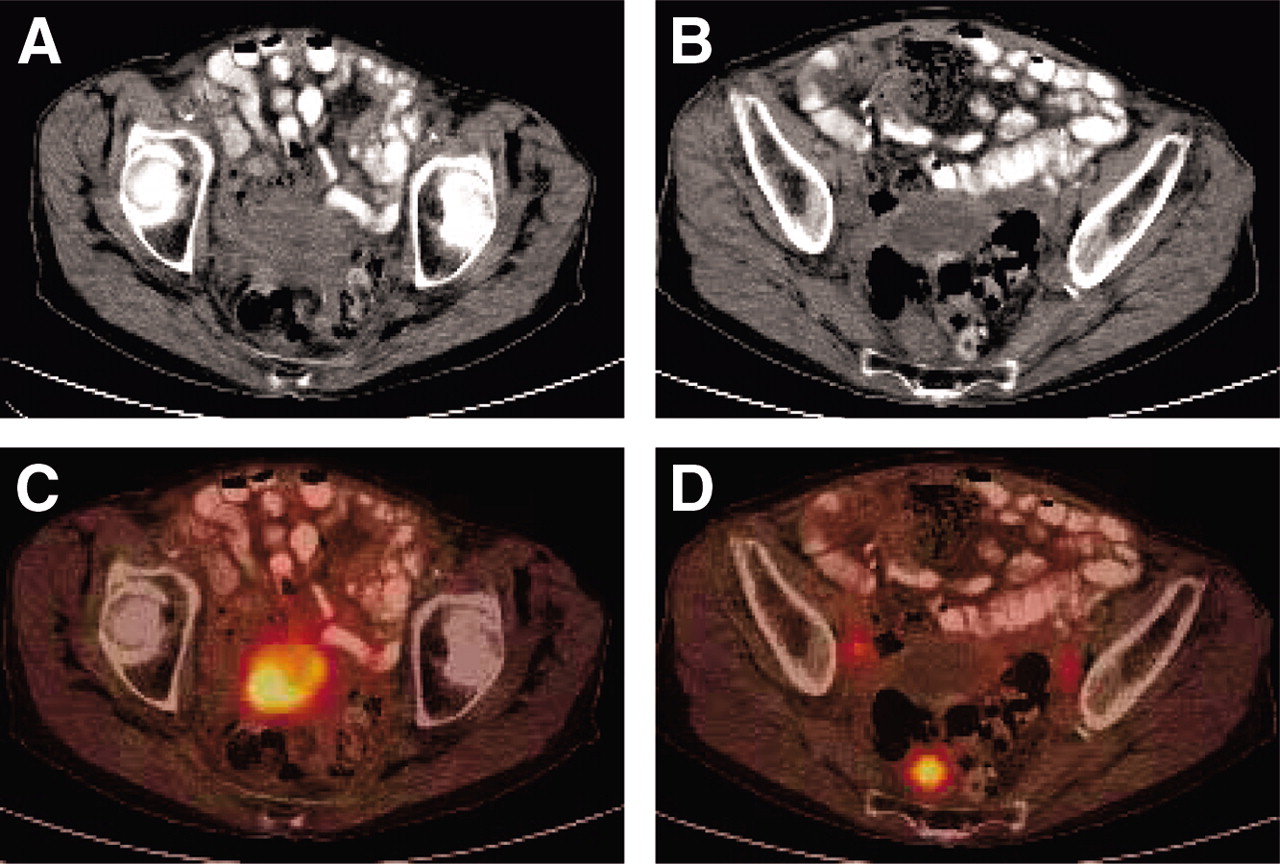
Images of 84-y-old woman with cervical cancer who was referred for evaluation of recurrent disease and for restaging. (A and B) CT shows mass in pelvis and enlarged right iliac node. (C and D) 18F-FDG PET/CT shows uptake in lower pelvic mass (SUV, 9.2), in both pelvic lymph nodes (SUV, 4.5 on right and 3.2 on left), and as a single focus in right presacral region corresponding to soft-tissue nodule (SUV, 6.8).
A metaanalysis of data from 15 studies on 18F-FDG PET in cervical cancer (24) reported a combined pooled sensitivity and specificity of 84% and 95%, respectively, for aortic node metastases and 79% and 99%, respectively, for pelvic node metastases. For clinically suggestive recurrent disease, pooled sensitivity and specificity of 18F-FDG PET were 96% and 0.81%, respectively. For CT, the overall sensitivity was 47%.
Sensitivity for detecting recurrence in asymptomatic women is also high though less than that in symptomatic women (80% vs. 100%) (25). Management of patients with a complete response to prior treatment who present with elevation of serum tumor markers (e.g., squamous cell carcinoma antigen in the absence of detectable disease using conventional imaging) is a clinical challenge. In these patients, additional imaging with 18F-FDG PET can help detect disease and guide management. Chang et al. (26) reported detection of disease in 94% of patients with negative conventional imaging. This helped in early detection of disease in these patients and early initiation of therapy leading to positive effect on survival in comparison to historical data. Diagnostic sensitivity and accuracy, in this situation, have been reported to be as high as 97.5% and 94.0%, respectively (27). Yen et al. suggested use of a scoring system to maximize benefit from 18F-FDG PET (28). The scoring system included 3 factors associated with poor survival: primary radiation, squamous cell carcinoma antigen ≥ 4 ng/mL, and symptoms. These were used to define 3 distinct prognostic groups. PET helped change the treatment plan in 65% of patients. Based on their findings, the authors recommended that it would be most beneficial to use 18F-FDG PET in those with the best prognosis (score ≤ 1), because a change in management due to PET is likely to enhance survival. For those with an intermediate score of 2, PET will be useful in modifying the treatment plan; PET could be avoided in those with a risk score of 3.
Dual-phase 18F-FDG PET with early 40-min images followed by repeated imaging at 3 h after injection improves detection of recurrent cervical carcinoma. Lai et al. compared dual-phase imaging with CT/MRI scans. 18F-FDG PET detected metastatic disease better than CT/MRI (sensitivity, 92% vs. 60%). The accuracy for detecting pelvic lymph node metastasis was 78% for PET versus 67% for MRI. There was no difference in detection of small-volume disease. PET significantly affected treatment modification in 55% of patients (29). Dual-phase imaging also enhances detection of paraaortic nodal lesions. A prospective study with 104 patients with FIGO stages IB–IVB found that, in 18.4% patients with lower paraaortic node metastases, the metastases were detected only at delayed imaging (residence index, 12.6%). The combined early and delayed sensitivity and specificity were 100%; treatment plan was changed in 21.1% of patients and detected more lower paraaortic nodes (30).
In a prospective study in patients with untreated locally advanced (35%) or recurrent (65%) cervical cancer, dual-phase imaging was compared with MRI and CT, and pathology or clinical follow-up was applied as the final determinant. 18F-FDG PET was significantly superior to MRI and CT in identifying metastatic lesions, although the diagnostic accuracy was similar for local tumors. Dual-phase PET (90% detection) was also significantly better than the 40-min PET images (70% detection) for detection of metastatic lesions in peritoneum, bones, and pelvic and iliac nodes, although there was no difference for primary, residual, and recurrent local tumors. Dual-phase PET led to a change in the treatment plan in about 30% of patients (31).
Assessment of paraaortic lymph node metastases is prognostically important and is related to progression-free survival in advanced cervical cancer. 18F-FDG PET has high sensitivity and is useful in detecting and localizing disease in patients with negative CT results (32). The presence of nodal disease on 18F-FDG PET can predict cause-specific survival. Forty-seven patients with FIGO stage IIIB cervical cancer were evaluated before therapy (33). The 3-y cause-specific survival was 73% for those with no lymph node metastases, 58% for those with only pelvic lymph node metastases, 29% for those with pelvic and paraaortic lymph node metastases, and 0% for those with pelvic, paraaortic, and supraclavicular lymph node metastases.
The ability of 18F-FDG PET to assess nodal status can be useful in guiding therapies. In a prospective study of patients with stage IB–IIIB cervical cancer, all had PET findings negative for nodal disease. Five-year survival did not differ between patients treated with radiotherapy alone (n = 15) and patients treated with radiotherapy and concurrent chemotherapy (n = 50). The study concluded that concurrent therapy was of no benefit in those with negative PET findings for nodes (34). Positive PET findings for nodes, irrespective of their size at diagnosis, are likely the most important predictor for distant metastases (35).
Preliminary data in a study with 3 patients also showed the feasibility of using 18F-FDG PET for monitoring neoadjuvant therapy (36). There are encouraging data on the use of 18F-FDG PET in assessing response to primary therapy and prognostication. In a retrospective study of 152 patients with carcinoma of the cervix who underwent pre- and posttreatment scans after combined-modality treatment, the 5-y cause-specific survival estimate was 80% in those without, versus 32% in those with, residual abnormality. Of those with progression of disease, none were alive at 5 y (37).
18F-FDG PET has been used for radiation treatment planning in cervical and endometrial cancers. PET/CT-guided intensity-modulated radiotherapy of the paraaortic lymph nodes has been proposed for patients with cervical carcinoma and paraaortic metastases. Intensity-modulated radiotherapy helps reduce the radiation dose to surrounding normal structures, particularly bowel. Use of PET/CT could significantly reduce radiation dose to various organs such as the stomach, liver, and colon (38). PET/CT is useful in guiding intensity-modulated radiotherapy and brachytherapy treatment planning so that doses can be escalated without harming the surrounding tissues (39,40).
Hypoxia is known to be an important limiting factor in response to radiation therapy. It is associated with an increased likelihood of local recurrence and distant metastasis and heralds a poor response to therapy (41,42). The phenomenon has also been recognized in cervical and uterine cancers and is associated with a more aggressive tumor phenotype (43,44). Measurement of tumor oxygen levels using probes, however, is invasive and perhaps nonreproducible.
Several PET tracers are under investigation for noninvasive assessment of tumor hypoxia. Radiocopper-labeled diacetyl-bis (N4-methylthiosemicarbazone) is a potential tracer for imaging hypoxia (45). In cervical cancer, an inverse correlation between outcome and uptake of this tracer has been demonstrated (46). Hypoxia has also been correlated with angiogenesis in cervical cancer (47). Carbonic anhydrase IX and GLUT-1, which are regulated via hypoxia-inducible factor 1α, may serve as useful intrinsic markers of tumor hypoxia (48,49). In cervical cancer patients receiving curative radiation therapy, overexpression of hypoxia-inducible factor 1α associated with hypoxia is linked to a poor prognosis (50). Patients with hypoxic tumors have a significantly increased risk of nodal or distant metastases, independent of tumor size (51).
Besides 18F-FDG, other PET tracers used in oncologic imaging are 11C-choline, 11C-methionine, and 11C-acetate. Data on the use of these tracers in gynecologic cancer are limited. Choline is used for synthesis of phospholipids in cell membranes, methyl metabolism, and lipid-cholesterol transport and metabolism. Intracellular choline is metabolized to phosphorylcholine by the enzyme choline kinase and is trapped within the cell. Various tumor cells are associated with upregulation of choline kinase, increased choline uptake, and elevated levels of phosphorylcholine (52,53). Because of its rapid blood clearance (approximately 7 min), imaging needs to be initiated as early as 3–5 min after tracer injection.
11C-Choline PET has been compared with 18F-FDG PET in 18 untreated patients. 11C-Choline PET detected primary tumors in 16 of 18 patients, as compared with the 14 of 18 patients in whom 18F-FDG PET detected primary tumors, and was positive in a patient with small uterine cancer and a diabetic patient whereas 18F-FDG PET was negative. False-positive findings were seen for atypical hyperplasia of the endometrium and pelvic inflammatory disease. Overall, SUVs were lower for 11C-choline PET. Detection of microscopic peritoneal disease was limited and periiliac lymph node metastases were missed because of intestinal activity (54). Imaging with 11C-methionine is based on amino acid transport and protein synthesis and may be related to the amount of viable tumor and active proliferation (55,56). It is rapidly cleared from blood, metabolized in the liver and pancreas, and has no significant renal excretion. This makes it more suitable than 18F-FDG in imaging disease in the pelvis (because there is little or no radioactivity in the urinary bladder).
Using 11C-methionine, Lapela et al. imaged 14 patients with either cervical or endometrial carcinoma. All showed increased uptake, with a mean SUV of 8.4 for tumor, versus a mean SUV of 4.6 for normal endometrium. Moderately or poorly differentiated tumor showed greater uptake than well-differentiated tumor; however, physiologic uptake limited evaluation (57). The study was done with PET only, and PET/CT could overcome this limitation.
OVARIAN CANCER
Ovarian cancer represents the second most common gynecologic malignancy, with a prevalence of 30–50 per 100,000 women, and is the cause of more than half of all deaths related to gynecologic cancer (58). There is no reliable screening tumor marker, and most cases present as advanced disease. Surgical debulking followed by chemotherapy is the mainstay of treatment and is associated with longer disease-free survival than is suboptimal debulking. However, recurrence is frequent and the overall 5-y survival for advanced disease is only 17% (59).
18F-FDG PET in ovarian cancer (Fig. 2) has been studied with variable results. In the primary diagnosis and staging of ovarian cancer, Hubner et al. (60) reported a positive predictive value of 86% and a negative predictive value of 76% and Schroder et al. (61) reported overall accuracy of 90%, with sensitivity of 96% and negative predictive value of 75%. Yoshida et al. (62) showed an incremental role for PET to CT in staging ovarian cancer.
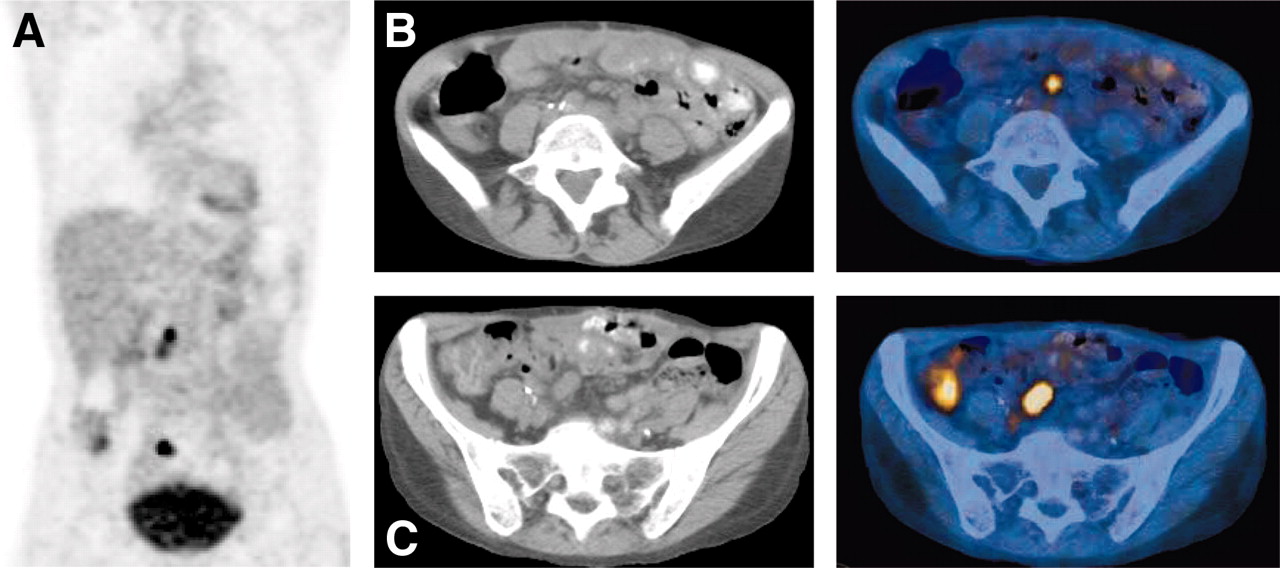
Images of 62-y-old woman with ovarian cancer who had a rising level of CA-125 and was being evaluated for recurrent disease. (A) Maximum-intensity projection coronal 18F-FDG PET/CT image (A) and transaxial CT images at 2 levels (B and C) show active disease in paraaortic and pelvic nodes (SUV, 4.3 and 5.8) and mesenteric disease.
Because ovarian cancer has a propensity to disseminate in the peritoneum, detecting small-volume disease is of prime concern. The low resolution of PET has limited its usefulness in detecting small-volume disease. Rose et al. (63) studied the use of 18F-FDG PET for detecting disease in 17 patients after a complete clinical response before a second look. The sensitivity was only 10% and the specificity 42% despite intravenous hydration, diuretic therapy, and bowel preparation. The study was done on patients with optimal primary cytoreduction, using PET only, and most of the lesions not detected were smaller than 6 mm. Other studies reported better results, with sensitivity ranging up to 66% and a high specificity of 94% after primary debulking (64), and a positive predictive value of 93% for peritoneal disease measuring up to 5 mm from various cancers (65).
Second-look laparotomy or laparoscopy is sometimes performed on patients without clinical evidence of disease to assess tumor response. About 36%–73% of patients may have persistent disease detected at second-look laparotomy. In the absence of disease, adjunctive therapy may be discontinued; otherwise, reductive surgery is done for residual disease, followed by chemotherapy. Second-look laparotomy has proven to be the most accurate way of assessing the presence of both microscopic and macroscopic disease but is not universally adopted. The cost-effectiveness and value of 18F-FDG PET as a substitute have therefore been explored. A detailed cost analysis of management of ovarian cancer with direct comparison of 18F-FDG PET and second-look laparotomy was done by Smith et al. (66), who demonstrated a reduction in unnecessary invasive staging procedures and health care costs after the introduction of 18F-FDG PET. PET led to a decrease in unnecessary laparotomies from 70% to 5%; 35% underwent the less-invasive laparoscopy instead of laparotomy. In a recent study by Kim et al. (67), the prognostic value of 18F-FDG PET was compared with that of second-look laparotomy in 55 patients with advanced ovarian cancer treated with chemotherapy. The positive predictive value was 93% and negative predictive value was 70%, with no significant differences in progression-free interval between the PET group and second-look laparotomy group.
18F-FDG PET has been shown to be superior to CT or MRI in detection of recurrent disease, with a reported sensitivity and specificity of 83%–91% and 66%–93%, respectively, for 18F-FDG PET versus 45%–91% and 46%–84%, respectively, for CT or MRI (68). Takekuma et al. (69) also reported high sensitivity (84.6%) and specificity (100%) for recurrent disease, significantly higher than that of CT/MRI or CA-125 levels. The low negative predictive value was caused by microscopic or cystic lesions. More recent studies have also shown a high sensitivity for 18F-FDG PET in the detection of recurrent disease (70). 18F-FDG PET may be more useful in detecting recurrence when conventional imaging studies show negative results and the CA-125 level is rising (24), although most reports have shown less sensitivity when lesions are less than 5–10 mm. Detection may, however, be better with newer cameras and PET/CT cameras that have better resolution and anatomic correlation allowing detection of lesions up to 5 mm (71). The exact magnitude of the clinical impact of detecting microscopic disease has yet to be properly studied. 18F-FDG PET helps localize sites of disease so that surgery or biopsy can be better directed. This is useful when conventional imaging fails to detect disease (72).
Because PET is more likely to detect macroscopic disease, it can help stratify patients for therapy. Most of the data regarding the prognostic value of consolidation therapy indicate a better prognosis in patients with disease < 1 cm or with no disease, suggesting a role for more aggressive and definitive therapy in those with macroscopic disease. PET/CT is of incremental value to CT alone in detecting viable disease in equivocal cases and in confirming absence of disease after therapy (73). It can also help localize the sites of disease so that surgery or biopsy can be better directed (74).
ENDOMETRIAL CANCER
Carcinoma of endometrium is the most common female pelvic malignancy and the fourth most common cancer in women—after breast, gastrointestinal, and lung cancer. Endometrial cancer is more common in postmenopausal women in Western countries and is linked to estrogen exposure. The most common presenting symptom (80% of patients) is abnormal bleeding. About 15% of postmenopausal women presenting with abnormal bleeding have endometrial carcinoma (11). Spread of the tumor occurs through blood vessels or lymphatics. Prognostic factors include the histologic type; depth of endometrial invasion; extension into the cervix, vascular space, or adnexa; and involvement of the pelvic and aortic nodes. Surgical staging is definitive, and nodal sampling is performed. Adjuvant radiation therapy is given in most cases, and the radiation field generally includes nodal areas. Assessment of the nodal sites for radiation is thus an important clinical issue.
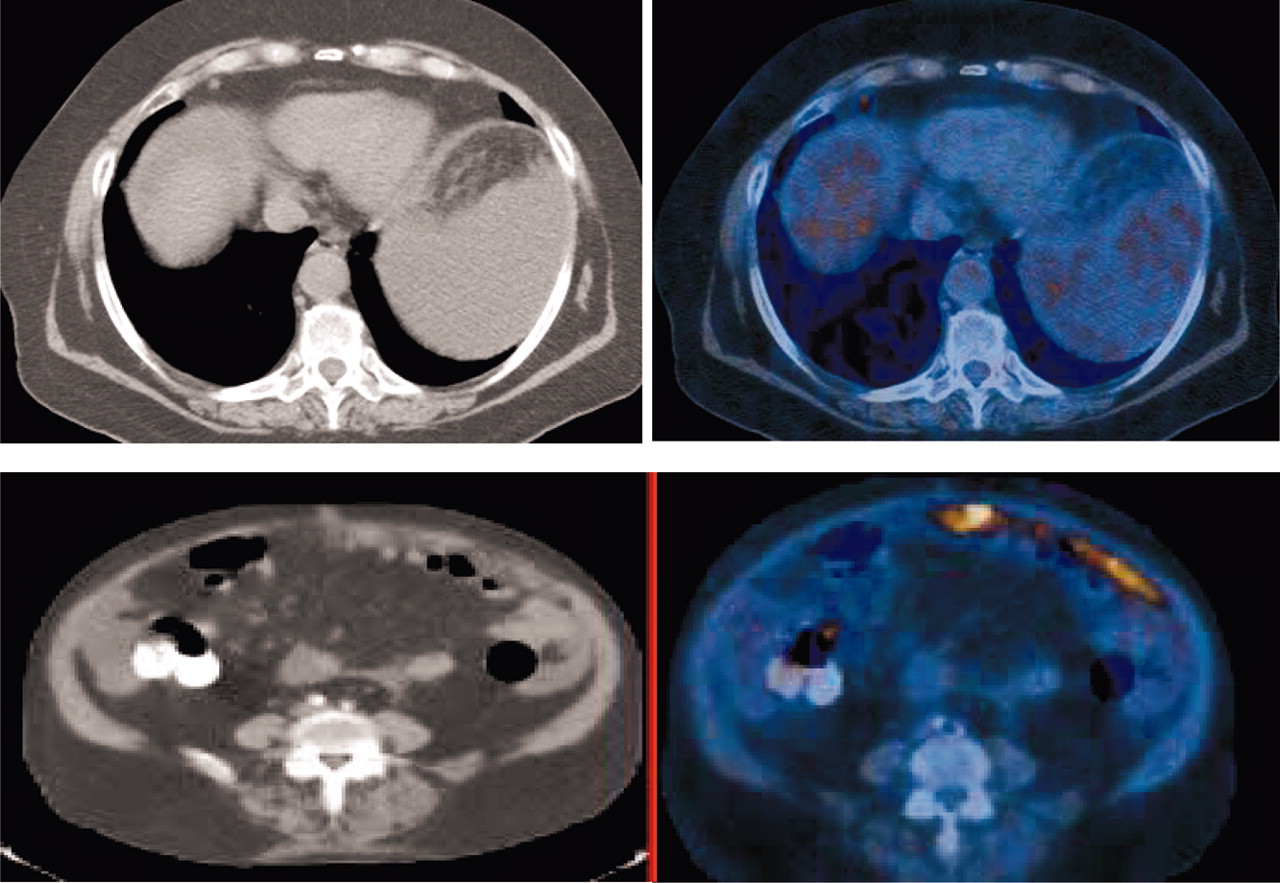
18F-FDG localizes in uterine tumors (Fig. 3) (75,76) and is useful in postsurgical monitoring and surveillance for recurrent disease. Belhocine et al. retrospectively analyzed 41 scans of 34 women with recurrence suspected on the basis of tumor markers or the findings of other radiographic investigations. PET confirmed recurrence in 88% of the cases, helped localize the site of disease, and detected asymptomatic recurrences in 12%. In 9 of 26 patients (35%), additional metastatic sites were detected, significantly altering management. The sensitivity and specificity were 96% and 78% (77). In another study (78), 18F-FDG PET had better sensitivity, specificity, and accuracy than did conventional imaging or tumor markers. 18F-FDG PET affected patient management in one third of the cases, and patients with negative PET results showed a trend to have improved disease-free survival.
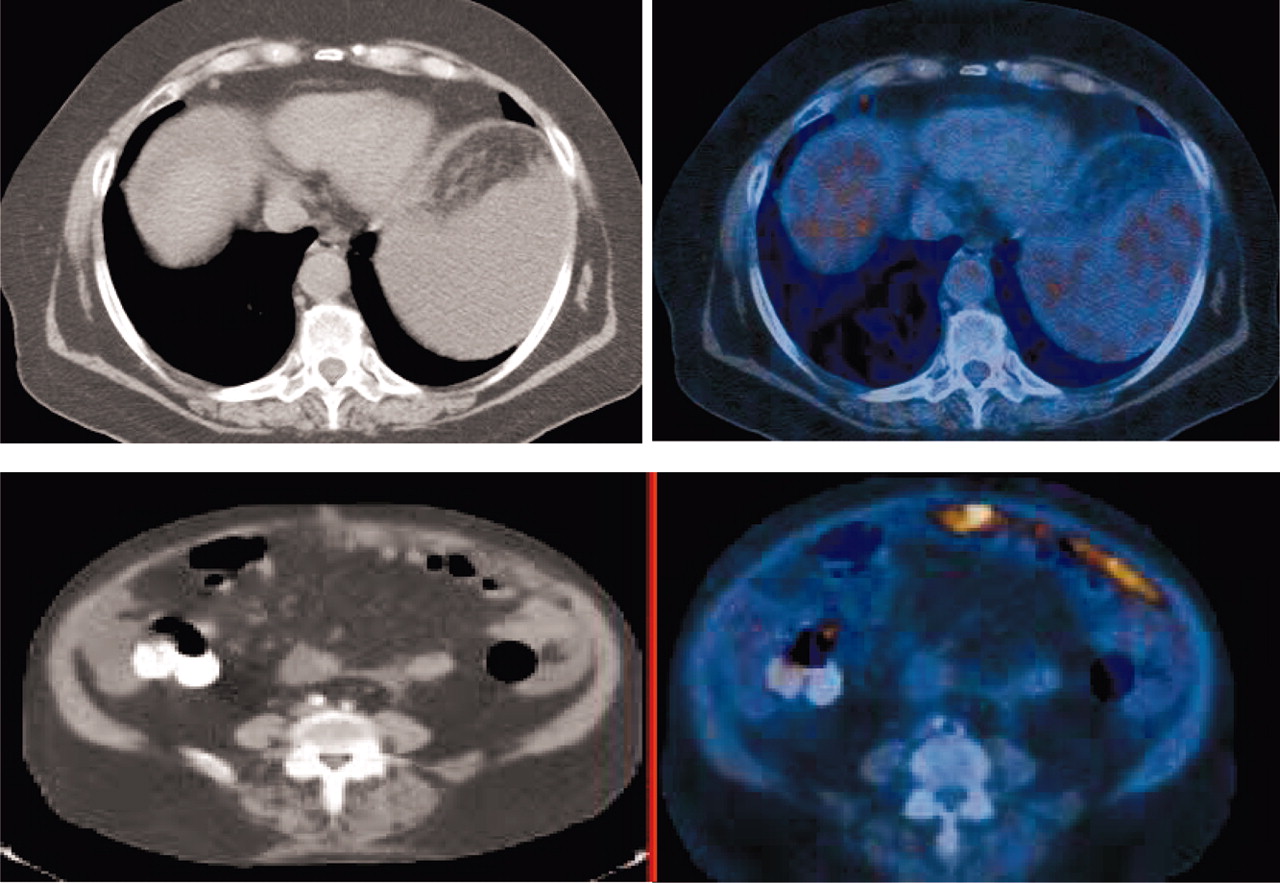
Images of 72-y-old woman with endometrial carcinoma who was being evaluated for recurrent disease. CT scans (left) show questionable node in supradiaphragmatic node. PET scans (right) show increased 18F-FDG uptake in small right supradiaphragmatic lymph node (SUV, 3.5) and in omentum (SUV, 7.1).
Uterine sarcomas constitute fewer than 5% of uterine corpus malignancies, and MRI is presently the imaging modality of choice. Umesaki et al. showed uptake of 18F-FDG PET in leiomyosarcoma (79). 18F-FDG PET was compared, in a small study, with MRI in 5 patients. The PET findings were positive in all 5 patients, whereas the MRI findings were positive in only 4. Uptake in most cases was high, with a mean value of 4.5 ± 1.3 (80). Larger studies are needed to define the role of 18F-FDG PET in the management of these sarcomas.
VULVAR CANCER
Vulvar squamous cell carcinoma accounts for about 5% of gynecologic malignancies and is usually detected in the West at relatively early clinical stages, without obvious metastases. It is surgically staged, and groin nodal dissection is frequently performed because about 10%–20% of patients can have clinically occult groin nodal metastases. Evaluation of groin nodes is important for staging, therapy, and prognosis. The incidence of groin nodal metastases increases when invasion is >1 mm (81). Routine evaluation involves only chest radiography; abdominopelvic CT scans may be obtained when local or distant extension is suspected. In a prospective analysis, Cohn et al. evaluated the use of 18F-FDG PET for detecting groin nodal metastasis and found a sensitivity of 80%, specificity of 90%, positive predictive value of 80%, and negative predictive value of 90% on a per-patient basis, whereas the values were 67%, 95%, 86%, and 86%, respectively, on a groin-to-groin basis. 18F-FDG PET had high specificity and was more accurate for detection of extranodal disease (82). The optimal role of 18F-FDG PET in vulvar cancer remains to be defined.
VAGINAL CANCER
Vaginal cancer is rare. Fewer than 3% of cases of gynecologic cancer are vaginal. It is estimated that in 2005, about 2,140 women will be diagnosed with vaginal cancer in the United States, with an estimated 810 deaths from the disease (83). Vaginal cancer behaves similarly to cervical cancer, with distant spread primarily through lymphatics, and comparable survival rates. Treatment and management are also similar.
Few studies have focused on the use of PET in vaginal cancer only. A recent study of 23 patients reported a high diagnostic utility for 18F-FDG PET in vaginal cancer for primary (100% for PET vs. 43% for CT) and nodal disease (84). PET detected more nodes than did CT. This study found no correlation between positive PET findings and survival; however, the number of patients was small.
LYMPHOSCINTIGRAPHY
Sentinel node mapping was conceptualized by Cabanas in 1977 for penile cancer (85) and was later applied to the intraoperative mapping of nodes in melanoma using isosulfan blue dye (86). Later, radionuclide scintigraphy was used in conjunction with blue dye and showed superior results in breast cancer and melanoma (87,88). Nodal dissection can lead to significant morbidity, which can be reduced by appropriately selecting patients for lymphadenectomy on the basis of confirmed histologic involvement of a sentinel node. Increasingly, lack of malignant involvement of the node leads to cancellation of radical lymphadenectomy. Sentinel node mapping is increasingly being used in gynecologic cancer to prevent morbidity and is being studied in vulvar and cervical cancers, as well as, recently, endometrial cancer. It is a noninvasive, fast, and convenient technique that can be done on either the day of surgery or the day before surgery.
The technique involves injecting 99mTc-sulfur colloid at the lesion site. Intradermal, subcutaneous, submucosal, or superficial intratumoral injections may be performed. Dynamic imaging may be performed, especially when the particle size is small. Blue dye (isosulfan blue) is injected intraoperatively because the transit is fast; often, the initial nodes may not be visualized. Handheld γ-probes have been used for detecting hot nodes for removal during surgery. In vivo and ex vivo counts are done over the node. Generally, those with counts more than 10 times background levels are considered sentinel.
In vulvar cancer, both superficial and deep inguinofemoral dissection is undertaken, with its resultant morbidity. The use of sentinel mapping to reduce dissection of nodes is therefore of interest. Several studies have reported the feasibility and usefulness of sentinel node mapping. Using lymphoscintigraphy, Decesare et al. reported a sensitivity and negative predictive value of 100% in a small number of patients (89). de Hullu et al. (90) used a combination of 99mTc-labeled nanocolloid and blue patent dye to identify the sentinel node. There was 100% identification of sentinel nodes by 99mTc-nanocolloid, versus 56% with blue dye. Several studies subsequently (91,92) have reported high detection rates using both blue dye and radiocolloid scintigraphy, with sensitivity ranging from 90% to 100%. 99mTc-Phytate also has been used for mapping with comparable results (93). With midline vulvar cancer, the drainage is often to bilateral nodes that may evade detection (90,94) and bilateral lymphadenectomy is recommended. Overall, the implication of negative findings for sentinel nodes in gynecologic malignancies is not yet clearly understood.
In cervical cancer, only about 15% of patients in stage IA2–IB1 have lymph node metastases. Routine nodal dissection thus may show no clear clinical benefit. Several studies have demonstrated the utility of lymphoscintigraphy in cervical cancer. External iliac and obturator nodes are more frequently detected, and bilateral nodal drainage is common (Fig. 4). With lymphoscintigraphy alone, the detection rate is between 80% and 93% (95,96). Combined use of blue dye and colloid scintigraphy increases detection, although the overall results of various studies range from 78% to 100% (97,98). False-negative rates are low (<1%). Recent studies have also reported similar results, with a high negative predictive value of 100% (99,100). Use of lymphoscintigraphy in vaginal cancer also appears promising (101).

Images of 52-y-old woman with stage IB1 cervical carcinoma who was referred for sentinel node mapping. Anterior (A), left lateral (B), and right lateral (C) images show uptake in injection site in cervix and focal uptake in right pelvis consistent with sentinel node in iliac region.
Burke et al. proposed that intraoperative lymphatic mapping might identify targets for selective nodal biopsy in women with high-risk endometrial cancer (102). Pelosi and colleagues carried out a feasibility study, using lymphoscintigraphy in combination with blue dye (103). In a later study, a high sensitivity and negative predictive value were reported for lymphoscintigraphy (104). The lymphoscintigraphy is done by hysteroscopic injection of tracer administered subendometrially around the lesion. A recent study showed 100% detection of nodes by lymphoscintigraphy, versus 36% by blue dye (105). Similar results have been shown with 99mTc-phytate (106).
CONCLUSION
The feasibility of applying lymphoscintigraphy to gynecologic cancer has been documented. The overall detection rates with lymphoscintigraphy are high and are better when the technique is used in conjunction with blue dye (which is usually less useful by itself). However, studies on this subject have been small and have had variable results. A multicentric study with more data and that also shows clinical utility for routine use is needed before the procedure can be adopted for such use.
Footnotes
Received Sep. 5, 2005; revision accepted Sep. 14, 2005.
For correspondence or reprints contact: Neeta Pandit-Taskar, MD, Nuclear Medicine Service, Department of Radiology, Memorial Sloan-Kettering Cancer Center, 1274 York Ave., New York, NY 10021.
E-mail: pandi-n{at}mskcc.org
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH NOVEMBER 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}