


Abstract
18F-FDG PET imaging is now established as a valuable tool for evaluating cancer patients. However, a limitation of 18F-FDG is its absence of specificity for tumor. Both protein synthesis and amino acid transport are enhanced in most tumor cells, but their metabolism is less affected in inflammation. We therefore decided to evaluate the ability of PET with 2-18F-fluoro-l-tyrosine (18F-TYR) to visualize cancer lesions in patients compared with 18F-FDG PET. Methods: 18F-FDG PET and 18F-TYR PET were performed on 23 patients with histologically proven malignancies (11 non–small cell lung cancers (NSCLCs), 10 lymphomas, and 2 head and neck carcinomas). Fully corrected, whole-body PET studies were obtained on separate days. 18F-FDG studies were performed after routine clinical fashion. 18F-TYR studies were started 36 ± 6 min after tracer injection and a second scan centered over a reference lesion was acquired after completion of the whole-body survey—on average, 87 min after injection. Standardized uptake values (SUVs) were calculated for all abnormal foci and for various normal structures. Results were compared with pathologic or correlative studies. Results: 18F-FDG PET correctly identified 54 malignant lesions, among which 36 were also visualized with 18F-TYR (67%). 18F-TYR did not detect any additional lesion. Tumor SUVs (SUVbw, 5.2 vs. 2.5), tumor-to-muscle (7.4 vs. 2.7), and tumor-to-mediastinum activity ratios (3 vs. 1.4) were higher with 18F-FDG than with 18F-TYR. Two of 11 NSCLCs and 4 of 10 lymphomas were understaged with 18F-TYR compared with 18F-FDG. Although the NSCLC lesions missed by 18F-TYR PET were small, several large lymphoma lesions did not accumulate the tracer. In 4 patients, 18F-TYR–positive lesions coexisted with 18F-TYR–negative lesions. There was a high physiologic 18F-TYR uptake by the pancreas (average SUVbw, 10.3) and the liver (average SUVbw, 6.3). Muscle and bone marrow uptakes were also higher with 18F-TYR than with 18F-FDG: average SUVbw, 1 versus 0.7 and 2.6 versus 1.8, respectively. There was no change over time in the 18F-TYR uptake by the tumors or the normal structures. Conclusion: 18F-TYR PET is not superior to 18F-FDG PET for staging patients with NSCLC and lymphomas.
During the past decade, PET imaging has become an essential tool in the management of a growing number of cancer patients (1). 18F-FDG is by far the most common radiopharmaceutical in clinical use and has shown a high sensitivity for diagnosing and staging a wide variety of malignant diseases. However, there are several well-known limitations for the use of 18F-FDG in oncology. Glucose metabolism is not significantly increased in some tumor types, such as prostate carcinoma (2). The most significant drawback of 18F-FDG for oncologic purposes results from its absence of specificity for tumor. Infection, inflammation, granulomatous diseases, and many other physiologic or pathologic conditions can all show high 18F-FDG uptake (3).
Protein metabolism is also highly modified in tumor cells. Both amino acid transport and protein synthesis rate are enhanced in malignancies (4,5). In contrast to 18F-FDG, amino acids appear to play a marginal role in the metabolism of inflammatory cells (6). Radiolabeled amino acids may thus be more suited than 18F-FDG for tumor imaging (7). Although the majority of the amino acids that were proposed as radiopharmaceuticals for evaluating protein metabolism with PET were labeled with 11C (7), 18F has a longer physical half-life, which improves its availability and potential for clinical use.
The synthesis of 2-18F-fluoro-l-tyrosine (18F-TYR) was first reported in 1988, and initial studies showed the potential of the tracer for evaluating protein synthesis in brain tumors (8,9). Recently, Lemaire et al. (10) modified the synthesis so that the tracer can now be produced as a no–carrier-added compound, with high yields and high specific activity. We therefore decided to conduct the first clinical investigation of 18F-TYR as a tracer for whole-body tumor imaging.
MATERIALS AND METHODS
Radiopharmaceutical Preparation and Purity
No–carrier-added 18F-TYR was produced via a multistep procedure (10). The first part of the synthesis involves the nucleophilic substitution of a 2-trimethylammonium-4-methoxy-benzaldehyde triflate with 18F-fluoride produced by the 18O(p,n) nuclear reaction. The 18F-fluorobenzaldehyde derivative was trapped on a solid support and then converted into the corresponding 18F-fluorobenzyl bromide by treatment with NaBH4 and HBr. The last steps of the synthesis imply alkylation of a (diphenylmethylene)glycine tert-butyl ester compound by phase-transfer catalysis with a C2-symmetric chiral catalyst (11), acid hydrolysis and high-performance liquid chromatography purification. 18F-TYR was then obtained with a radiochemical yield of 25%–40% (decay corrected, 100 min). This procedure affords at the end of the synthesis 4.9−7.8 GBq 18F-TYR of high specific activity.
Enantiomeric purity was determined on a CrownPak CR(+) column (Daicel, Tokyo, Japan) eluted at a flow rate of 0.8 mL/min with HClO4 (pH 4). In all cases, enantiomeric purity and radiochemical purity were >95% and >99%, respectively. Other quality controls (pH, osmolality, γ-purity, solvent, and so forth) were also realized.
18F-FDG was synthesized according to Lemaire et al. (12) using an automated 18F-FDG synthesis system (Coincidence Technologies S.A., Liège, Belgium).
Patients
Twenty-three patients (15 men, 8 women; mean age, 67 ± 8 y) were enrolled in this prospective study. All subjects had a pathologically proven malignancy. There were 11 non–small cell lung cancers (NSCLCs), 10 lymphomas, and 2 head and neck carcinomas. In all but 1 case, PET scanning was performed before any treatment was initiated. One patient with an intermediate-grade non-Hodgkin’s lymphoma (NHL) received chemotherapy (etoposide-dexamethasone) 6 wk before the PET. At that time, she was being reevaluated because of an apparent lack of response to this treatment. The patients’ characteristics are listed in Table 1. The medical ethics committee of our institution approved the research protocol, and all patients gave a written informed consent.
Patient Characteristics
PET
All studies were performed using the C-PET scanner (UGM-Philips, Milpitas, CA). The system has been fully described elsewhere (13). 18F-FDG and 18F-TYR PET studies were performed within 1 wk of each other. All patients fasted for at least 4 h before tracer injection. The blood glucose level was measured in each case and did not exceed 7.7 mmol/L. Patients with lymphoma received Diazepam (Valium; Roche S.A., Brussels, Belgium), 5 mg orally, 15 min before injection of 18F-FDG to limit muscle uptake. Patients were injected intravenously with 2.8 ± 0.5 MBq/kg (0.07 ± 0.01 mCi/kg; mean ± SD) 18F-FDG through an indwelling catheter. Acquisition was started 72 ± 17 min after injection and consisted of 5 or 6 bed positions. Five minute-emission scans, 1 min-transmission scans using a 137Cs point source, and 8-s emission contamination scans were interleaved. On a separate day, patients received 2.2 ± 0.2 MBq/kg (0.06 ± 0.01 mCi/kg) 18F-TYR through an indwelling catheter. Acquisition was started 36 ± 6 min after injections and followed the same procedure as for 18F-FDG scanning. In addition, a second emission scan centered on a reference lesion was started after completion of the whole-body survey, 87 ± 9 min after injection. The time interval between the 2 acquisitions was thus 51 ± 7 min. Images were reconstructed using the ordered-subsets expectation maximization algorithm and corrected for decay, scatter, random events, and attenuation.
Data Analysis
For the purpose of this study, 18F-FDG and 18F-TYR PET scans were concurrently analyzed with full knowledge of all clinically relevant data. PET studies were first visually analyzed using the standard UGM software (UGM-Philips). Any focus visualized in the 3 planes that did not correspond to physiologic activity was considered as abnormal. Regions of interest (ROIs) were placed over these foci and followed an isocontour at 60% of the maximum pixel value. In addition, ROIs were placed over normal structures, including muscle (right deltoid), mediastinum, lungs, liver, bone marrow (body of a lower thoracic vertebra), and pancreas, only for 18F-TYR. In all patients, these ROIs had similar sizes and were placed at similar levels. Standardized uptake values (SUVs) normalized for body weight (SUVbw), for body surface area (SUVbsa), and for lean body mass (SUVlbm) were calculated using the following equations (14,15):

 where BSA = 0.007184 × body weight0.425 × body height0.725.
where BSA = 0.007184 × body weight0.425 × body height0.725.
 where LBM (women) = (1.07 × body weight) −148 (body weight/body height)2 and LBM (men) = (1.1 × body weight) −120 (body weight/body height)2.
where LBM (women) = (1.07 × body weight) −148 (body weight/body height)2 and LBM (men) = (1.1 × body weight) −120 (body weight/body height)2.
Statistical Analysis
SUVs and activity ratios were compared in the different groups using 1-way ANOVA. Relationships between continuous variables were assessed using the Pearson product–moment correlation coefficient. In all cases, the level of significance was set at 0.05.
RESULTS
Whole-Body Distribution of 18F-TYR
Uptake values in various organs, as well as their evolution over time and the corresponding SUVs obtained with 18F-FDG, are shown in Figure 1. High uptake was seen in the pancreas and, to a lesser extent, in the liver and salivary glands. 18F-TYR uptake was mild in the bone marrow, but significantly higher than 18F-FDG. Muscle and liver uptakes were also higher with 18F-TYR than with 18F-FDG. Except for the SUVbw measured in the bone marrow, 18F-TYR uptake did not significantly increase over time.

Uptake values in various organs (SUVbw; mean ± 1 SD). F-TYR 1 = 18F-TYR PET images taken at first time point; F-TYR 2 = 18F-TYR PET images taken at second time point. *Statistically significant difference with 18F-FDG. †Statistically significant difference between 2 18F-TYR time points. Because pancreas is normally not visualized on 18F-FDG PET images, no regions were drawn. Except for bone marrow, where no difference was seen between 18F-TYR 1 and 18F-TYR 2, results obtained with SUVbsa and SUVlbm were similar to those obtained using SUVbw and are not represented.
18F-FDG Versus 18F-TYR
18F-FDG PET correctly identified 54 malignant lesions confirmed by pathologic analysis (n = 29) or correlative studies (n = 25). 18F-TYR PET visualized 36 of 54 lesions (67%). Three additional lesions were seen only with 18F-FDG: One mediastinal lymph node turned out to be benign (silicosis) on pathologic examination and the 2 other lesions, located in the lungs, remained unconfirmed. There was no false-positive result with 18F-TYR. 18F-FDG and 18F-TYR scans provided similar results in terms of patients’ staging in 6 of 11 lung cancers, in 2 of 2 head and neck carcinomas, and in 6 of 10 lymphomas, including 1 low-grade, stage I NHL that was missed by both modalities. One 11-mm large squamous cell carcinoma of the right upper lobe was not seen with 18F-TYR PET (18F-FDG SUVbw, 2). One right lower lobe adenocarcinoma was visualized with 18F-TYR PET (SUVbw, 3.3) but not the extensive hilar and mediastinal involvement (18F-FDG SUVbw, ranging from 3 to 4.3). All nodal lesions were <1 cm on CT. Among 4 low-grade lymphomas, 1 was missed by both modalities, and 3 were similarly staged. There were 2 intermediate-grade NHLs. One patient had a large abdominal mass clearly seen with both 18F-FDG and 18F-TYR, but a biopsy-proven bone marrow involvement was equally missed. The other patient had stage III disease with matched results with both methods for all lymph node stations except the cervical, which was not visualized with 18F-TYR. Two patients had high-grade NHLs. In a stage IV disease, 18F-TYR missed a massive splenic involvement and cervical nodes, whereas bilateral axillary nodes were clearly seen. In the second patient, bilateral cervical, abdominal, and right iliac nodes were missed by 18F-TYR, which identified axillary, mediastinal, and left iliac nodes. There were 2 patients with Hodgkin’s disease. One stage II was equally staged with both tracers. In a stage IV disease, 18F-TYR was taken up by cervical and axillary nodes, but not by an extensive, biopsy-proven esophageal involvement or by a large vertebral spread confirmed by MRI.
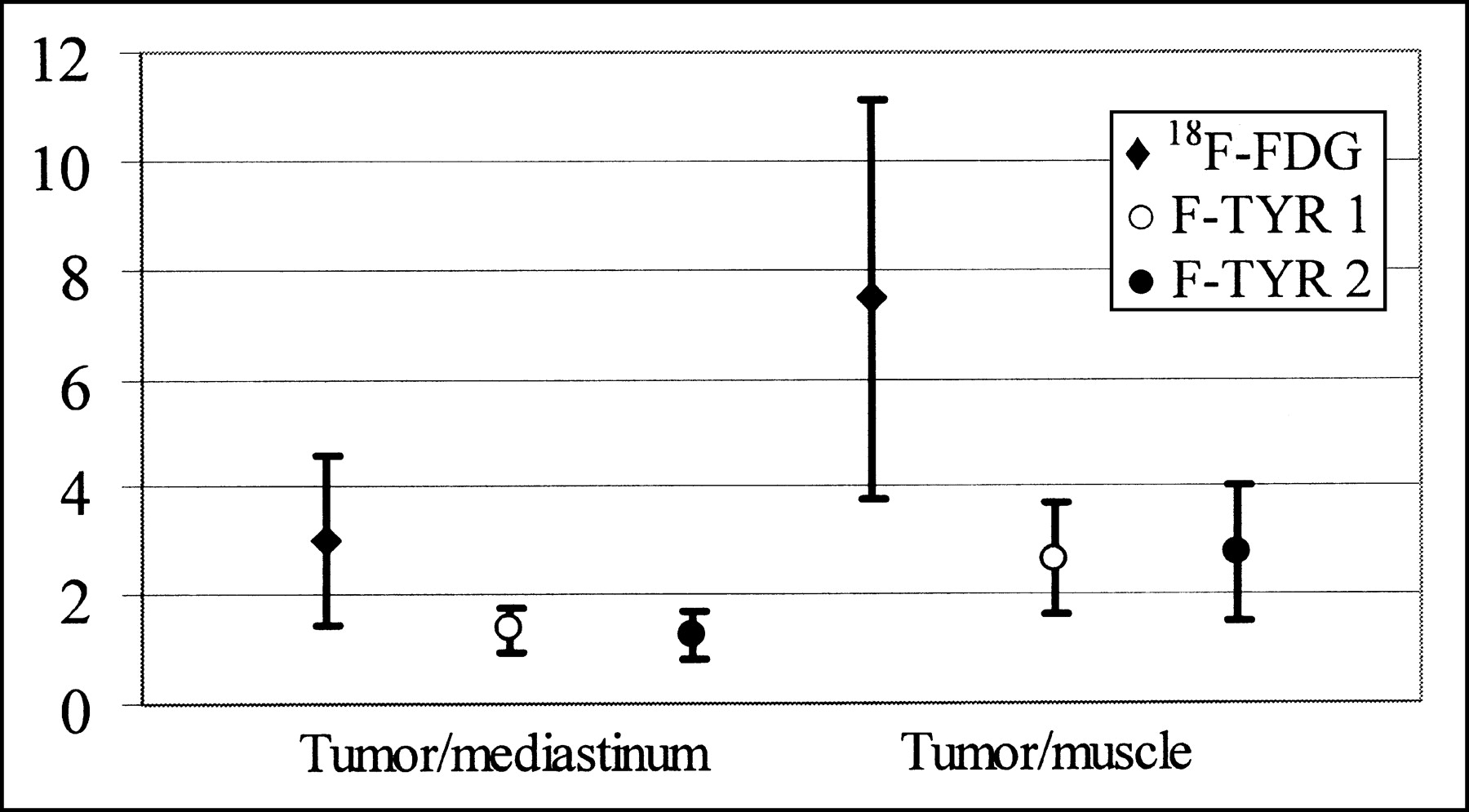
Overall, SUVs were higher with 18F-FDG than with 18F-TYR. Both tumor-to-muscle and tumor-to-mediastinum activity ratios were also higher with 18F-FDG than with 18F-TYR. Detailed results are given in Table 1 and shown in Figures 2 and 3. Representative PET images are shown in Figures 4 and 5.

SUVs normalized for body weight (SUVbw; A), lean body mass (SUVlbm; B), and body surface area (SUVbsa; C) in lesions that were seen with both tracers. Adenoc. = adenocarcinomas; LCC = large cell carcinomas; SCC = squamous cell carcinomas; F-TYR 1 = 18F-TYR PET images taken at first time point; F-TYR 2 = 18F-TYR PET images taken at second time point. Data are expressed as mean ± 1 SD.
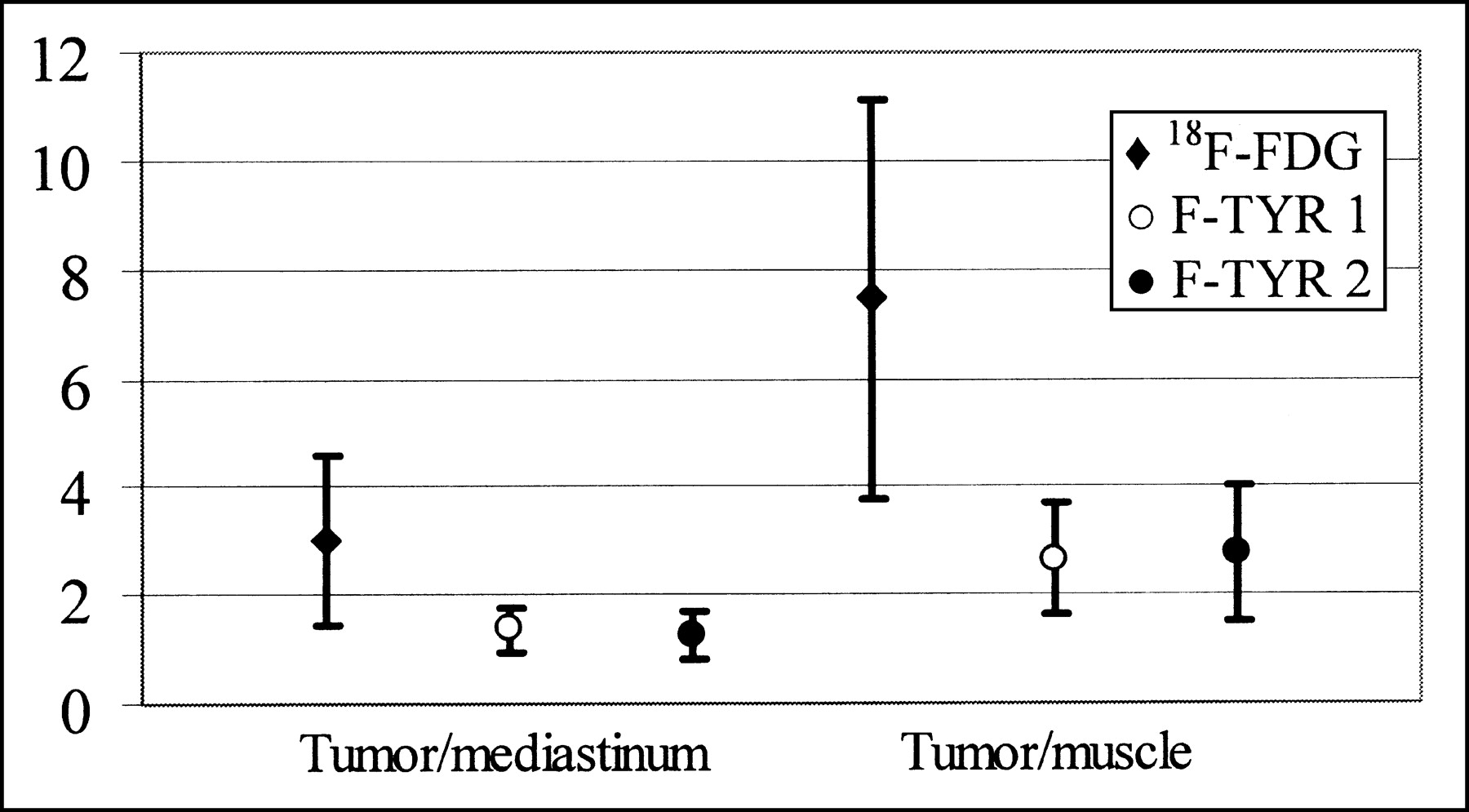
Activity ratios within tumors. Data are expressed as mean ± 1 SD.
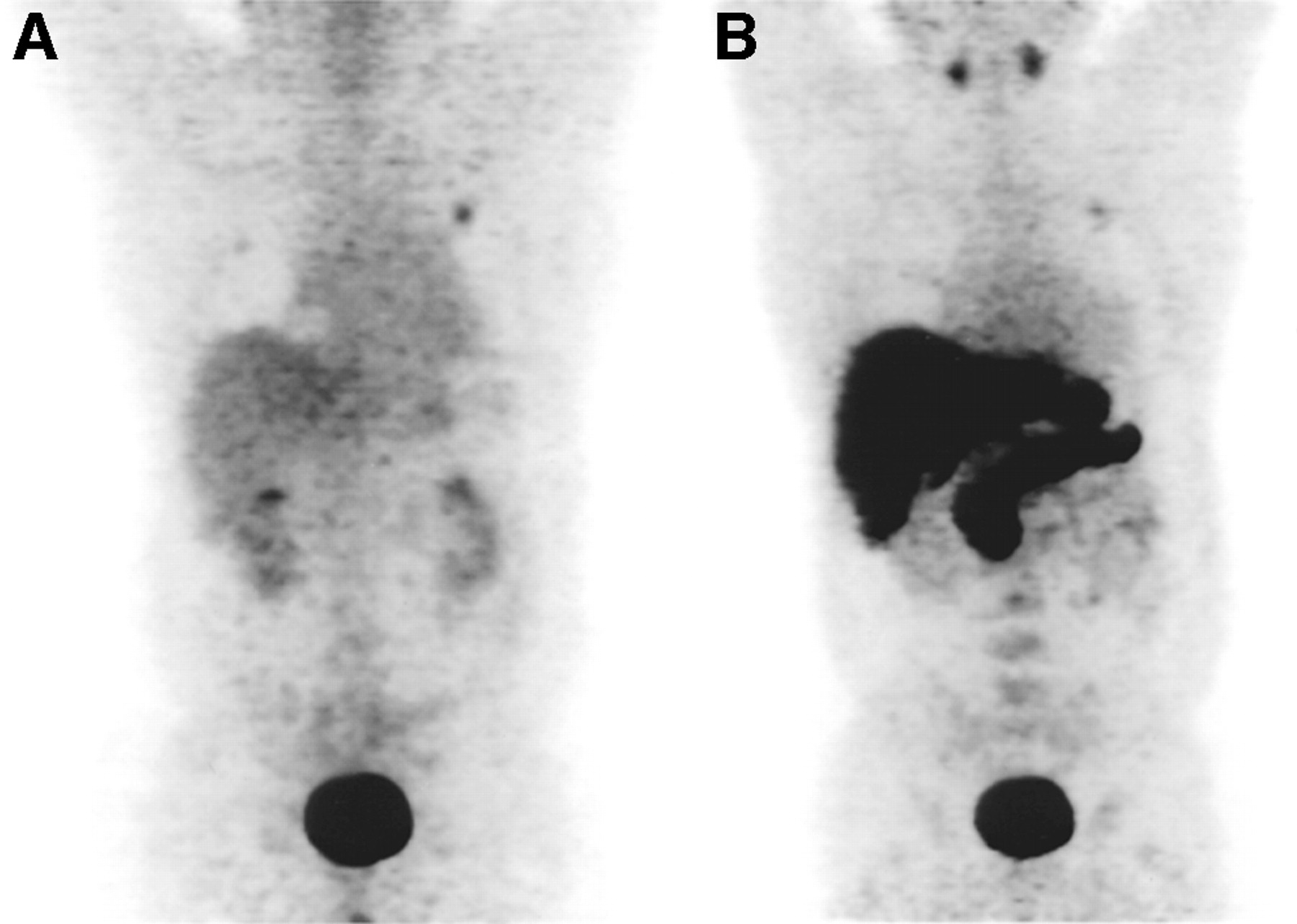
Three-dimensional projection PET images with 18F-FDG (A) and 18F-TYR (B) show 15-mm left upper lobe adenocarcinoma. 18F-TYR uptake is high in pancreas, liver, and salivary glands and mild in bone marrow.

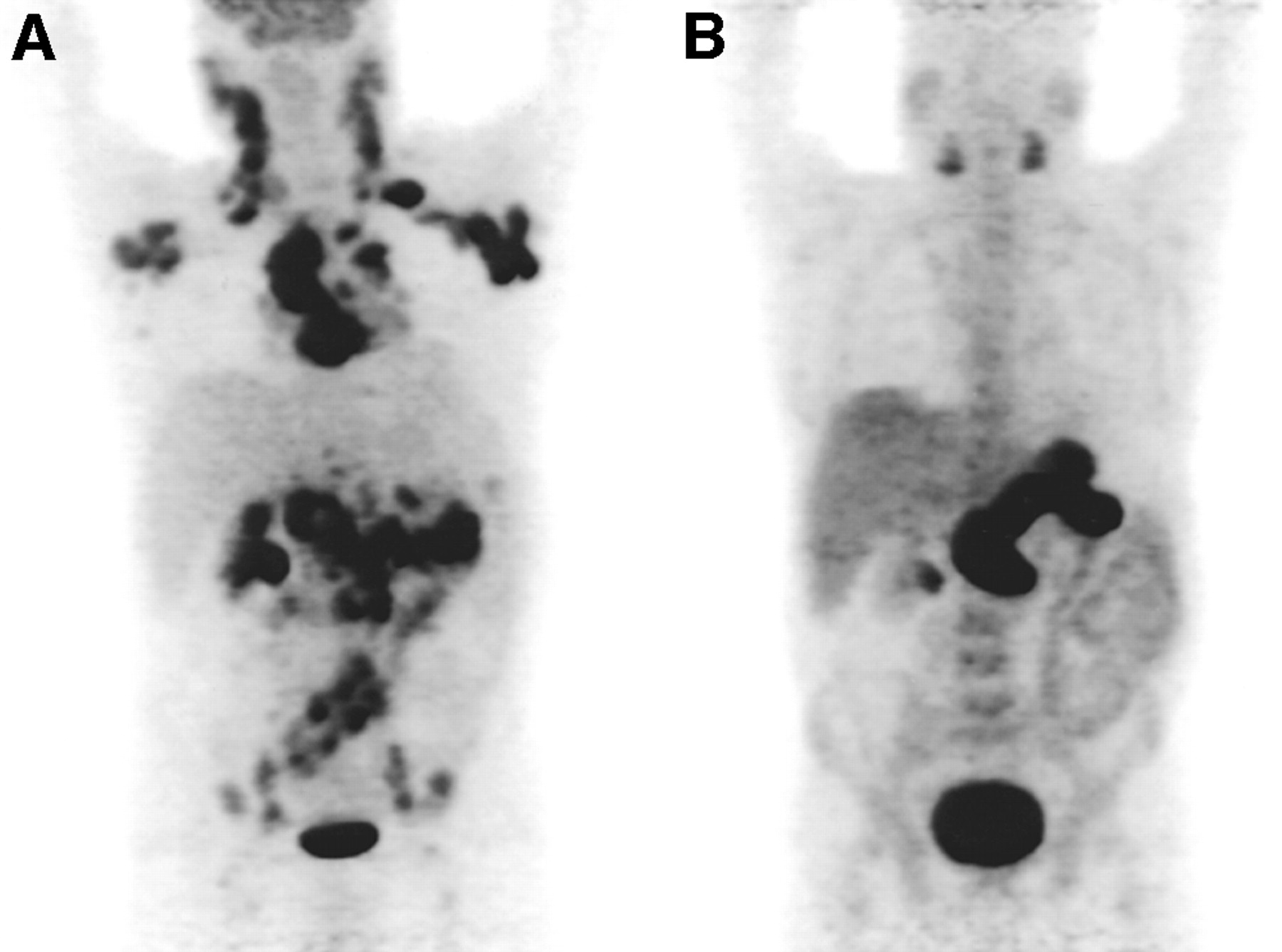
Three-dimensional projection PET images with 18F-FDG (A) and 18F-TYR (B) in patient with high-grade NHL. There is extensive nodal involvement on 18F-FDG PET, whereas only mild uptake is seen in both axillary regions, upper mediastinum, and, using only centered 3-section viewing (not shown here), left iliac nodes with 18F-TYR. Without extremely careful examination and without knowledge of 18F-FDG results, 18F-TYR scan could easily have been read as negative.
Correlation Between 18F-FDG and 18F-TYR
There was a strong correlation between 18F-FDG and 18F-TYR uptake in the muscle, mediastinum, and lungs, regardless of the 18F-TYR time point. A weak but signification correlation existed between 18F-FDG and 18F-TYR uptake measured at the initial time-point in the tumors. No correlation was found in the liver.
DISCUSSION
The nonspecific uptake of 18F-FDG by inflammatory cells or granulation tissues is well known and has even led to widening its indications to various inflammatory or infectious diseases (16). However, this also limits its capability to accurately distinguish tumors from benign conditions, such as postradiation changes. Thus, a large number of other compounds—in particular, radiolabeled amino acids—has been investigated as an alternative or a complement to 18F-FDG (7,17). Among these, 11C-methyl-methionine (MET) has been most extensively studied and has been shown to be valuable in brain tumors—in particular, for delineating the extent of the tumor (18). However, the tracer undergoes extensive nonprotein metabolism, with large amounts of circulating metabolites (19). The short half-life of 11C also limits both the tracer availability and its whole-body imaging capability. Another 11C-labeled compound that was extensively studied is l-1-11C-tyrosine (11C-TYR). Investigators at Groningen University obtained encouraging results with 11C-TYR for evaluating primary brain tumors, breast, head and neck carcinomas, and sarcomas (20–24). It was not sensitive for detecting nonseminoma lesions (25). 11C-TYR has established itself as a reliable tracer for assessing the rate of protein synthesis, but it shares with 11C-MET the limitations of the short-lived isotope 11C.
18F-TYR was initially produced by Coenen et al. (8) using electrophilic radiofluorination of O-acetyltyrosine in CF3CO2H, with a radiochemical yield of 17% and a specific activity of 10–20 GBq/mmol. They first used a rodent model to demonstrate that the tracer is rapidly incorporated into proteins (>80% at 60 min after injection), with a small transfer RNA–bound fraction (1.5%–2%) and virtually no labeled metabolites. 18F-TYR was thus featured as a tracer for evaluating the protein synthesis rate. Further studies in patients clearly showed that 18F-TYR uptake was significantly higher in brain tumors than in the normal tissue, with better contrast obtained early on after injection because of the increase in plasma protein-bound 18F-TYR over time (9). To date, however, there is no report of the use of 18F-TYR for whole-body tumor imaging with PET.
We developed the synthesis of no–carrier-added 18F-TYR by chiral catalytic phase-transfer alkylation, which improved both the radiochemical yield (25%–40%) and the specific activity (10). In patients, we found that most NSCLC and head and neck tumors were visualized as early as 30 min after injection. 18F-TYR PET was less sensitive for detecting NHL and Hodgkin’s disease lesions. However, overall, regardless of the normalization method (for body weight, body surface area, or lean body mass), the SUVs were higher with 18F-FDG than with 18F-TYR. On average, the SUVs and the tumor-to-mediastinum activity ratios were twice as high, and the tumor-to-muscle activity ratios were 3 times higher with 18F-FDG than with 18F-TYR. This was true for all tumor types except adenocarcinomas, where there was no significant difference (SUVbw, 3.1 vs. 2.8 for 18F-FDG and 18F-TYR, respectively). It should be noted that only 3 lesions were seen with both modalities in this group, which greatly limits the significance of the average values. In the nonlymphoma tumors, all lesions missed with 18F-TYR were small: There was one 11-mm primary adenocarcinoma and several metastatic nodes, also from an adenocarcinoma but in another patient. These nodes were also missed on CT. These false-negative results for 18F-TYR can thus be attributed to the low tumor-to-background activity ratios observed with 18F-TYR, which become critical in small lesions, rather than to a low protein synthesis rate or amino acid transport in these tumors. The average size of the lesions visualized with 18F-TYR PET, as assessed by CT or pathologic examination, was 33 ± 17 mm in largest diameter.
In lymphoma patients, we observed a different pattern of results. Not only could 18F-FDG–positive/F-TYR–positive lesions coexist with 18F-FDG–positive/F-TYR–negative lesions in the same patient, but also the false-negative results with 18F-TYR were not related to the lesions’ size. This observation, quite unsettling, is clearly illustrated in Figure 5, which shows massive nodal involvement totally devoid of 18F-TYR uptake, except in few regions. Although the series is limited and heterogeneous, no relationship was found between tumor grade or aggressiveness and tracer uptake. In these patients, we could not find any satisfactory explanation for the results obtained, which may be related to the heterogeneity that can arise among lymphomas and lead to clinical, biologic, or morphologic changes during the course of disease (composite lymphomas, lymphoma progression) (26). Differences in the local environment of the various tumor sites (angiogenesis, for instance) may also diversely influence the uptake of 18F-TYR, whose mechanism in malignancies has yet to be fully understood. Experimental data are missing to sustain these hypotheses. To definitely answer this question would require obtaining pathologic samples from all lesions in all patients, which is obviously not possible.
The physiologic uptake of 18F-TYR by normal structures can also limit the readability of the images and further decrease the sensitivity of the test. The high uptake in the pancreas and, to a lesser extent, the liver may limit the detection of lesions located in these organs. Similarly, the significant uptake in salivary glands could hamper the staging of head and neck tumors, although de Boer et al. (27) recently reported 100% sensitivity with 11C-TYR and PET for detecting primary carcinomas of the larynx and hypopharynx. On the other hand, we found that the 18F-TYR uptake was fairly homogeneous in the soft tissue of the head and neck regions, which could constitute an advantage compared with 18F-FDG, where intense uptake can be seen in lymphoid and muscular structures. Another concern is the significant uptake in the bone marrow, with an average SUVbw of 2.6 ± 0.5 compared with 1.8 ± 0.5 with 18F-FDG. Although Coenen et al. (8) found a significant amount of free 18F-fluoride in the plasma at 40 min after injection, the uptake distribution observed in our patients clearly matched the normal bone marrow distribution. In particular, there was no uptake in long bones such as the humerus and femurs. There was only 1 case of bone marrow involvement in our population, and it was missed by both 18F-FDG and 18F-TYR PET studies. Because of the high physiologic uptake, 18F-TYR is probably not the most appropriate tracer for evaluating pancreatic masses or for detecting bone or liver metastases.
There were no demonstrated false-positive results for 18F-TYR in our series. Three lesions did take up 18F-FDG but not 18F-TYR and were considered false-positive: There were 2 lung lesions, unconfirmed by any other method, and 1 benign hilar lymph node, corresponding to silicosis on pathologic examination. The question of the specificity of radiolabeled amino acids remains unsettled. Initial studies reported low MET accumulation in inflammatory and granulation tissues (6,28,29). However, clinical studies using MET in lung cancer patients failed to improve the specificity over 18F-FDG (30); recently, Rau et al. (31) found a higher MET uptake in inflamed lymph nodes than in tumor-infiltrated nodes in a murine model. These authors demonstrated that O-(2-18F-fluoroethyl)-l-tyrosine (FET) did not accumulate into chronic and acute lymphadenitis models, with no overlap between tumor and inflammation uptake values (31). FET uptake by tumor cells depends on the L-transport system and it is not incorporated into proteins (32). Few data are available regarding the specificity of other amino acid analogs and, although our results are encouraging, no definite conclusion can be drawn.
In this study, the sensitivity for detecting various malignant lesions was relatively low, with only 67% of the lesions visualized with 18F-FDG PET. This may be related to the biochemical processes studied with 18F-TYR. Although initial studies showed a high and rapid incorporation of 18F-TYR into newly formed proteins (8), further experiments from the same group using kinetic modeling indicated that an increase in the transport rate constant was primarily responsible for the high uptake in tumors (9). In the normal brain, the results fitted a 2-tissue compartment model (free intracellular 18F-TYR and protein-bound 18F-TYR). In tumors, however, a 3-tissue compartment model was better suited to explain the results. Ishiwata et al. (33) studied 18F-TYR, l-methyl-3H-MET, and l-1-14C-leucine (11C-LEU) in tumor-bearing mice. They found comparable protein incorporation for all 3 tracers, but the rate was much faster with 14C-LEU. In another set of experiments, they showed that only 14C-LEU uptake was decreased after inhibition of protein synthesis by cycloheximide, whereas the uptake of all 3 tracers was decreased after the amino acid transport was inhibited with ouabain (34). They also found significant amounts of radioactivity from 18F-TYR in the lipid fraction of the tumor extracts. Along with the compartment modeling, these findings suggest, for 18F-TYR, the presence of metabolic pathways distinct from the protein synthesis. These pathways remain unidentified. Therefore, in vivo, 18F-TYR uptake is likely to represent both amino acid transport and protein synthesis, and possibly a third metabolic process, still unknown, in proportions that remain to be evaluated.
Furthermore, it has yet to be fully established whether protein synthesis or amino acid transport is the most appropriate phenomenon to evaluate for oncologic purposes. Although some studies showed a good correlation between transport, as measured by MET uptake, and the tumor-proliferating fraction (35,36), other work showed no correlation between tumor growth and transport (37). Amino acid metabolism is complex and non–protein synthesis pathways may also be significantly increased in tumor cells (38). Thus, tracers for transport may be as good as or even superior to synthesis tracers for in vivo imaging.
CONCLUSION
In our limited series, PET imaging with 18F-TYR was less sensitive than 18F-FDG for staging NSCLCs and lymphomas. Specificity may be improved with 18F-TYR, but there were not enough false-positive results with 18F-FDG to clearly establish any superiority. We thus believe that 18F-TYR PET has, at best, a limited role for staging purposes, at least in these types of tumors.
Acknowledgments
The authors express their appreciation to the staff of the PET center at the Centre Hospitalier Universitaire, Liège, and to the clinicians who participated to the recruitment of the patients. Part of this work was presented at the 49th Annual Meeting of the Society of Nuclear Medicine, Los Angeles, CA, June 15–19, 2002.
Footnotes
Received Jul. 15, 2002; revision accepted Oct. 24, 2002.
For correspondence or reprints contact: Roland Hustinx, MD, PhD, Service de Médecine Nucléaire, CHU du Sart Tilman, B35, 4000 Liège 1, Belgium.
E-mail: rhustinx{at}chu.ulg.ac.be
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/CT of Skull Base Meningiomas Using 2-18F-Fluoro-L-Tyrosine: Initial Report
- PET with O-(2-18F-Fluoroethyl)-L-Tyrosine in Peripheral Tumors: First Clinical Results
- SPECT and PET Amino Acid Tracer Influx via System L (h4F2hc-hLAT1) and Its Transstimulation
- PET Scans in the Staging of Lymphoma: Current Status