


Abstract
O-(2-18F-Fluoroethyl)-l-Tyrosine (18F-FET) PET has shown promising results in brain tumor diagnosis. The aim of this prospective study was to evaluate 18F-FET PET in comparison with 18F-FDG PET in patients with peripheral tumors. Methods: Forty-four consecutive patients with suspected malignant tumors underwent 18F-FET PET and 18F-FDG PET within 7 d. Whole-body PET studies were performed 1 h after intravenous injection of 370 MBq of 18F-FET or 18F-FDG. Six patients were excluded from the analysis because a malignant tumor could not be verified. In 38 patients (7 with colorectal cancer, 6 with pancreatic cancer, 9 with head-neck cancer, 4 with lymphomas, 3 with lung cancer, 3 with ovarian cancer, 4 with breast cancer, and 2 with prostatic cancer), 18F-FET PET and 18F-FDG PET were compared. Results: 18F-FET was positive in only 13 of 38 patients (8 with head-neck cancer, 3 with breast cancer, and 2 with lung cancer), whereas 18F-FDG exhibited increased uptake in 37 of 38 patients. All squamous cell carcinomas were found to be 18F-FET-positive tumors (8 head-neck cancer and 2 lung cancer), whereas most adenocarcinomas were found to be 18F-FET-negative tumors. In patients with colorectal cancer, pancreatic cancer, ovarian cancer, prostatic cancer, and lymphomas, no increased 18F-FET uptake could be identified. All lesions that exhibited increased 18F-FET uptake also showed increased 18F-FDG uptake. No additional lesion was identified by 18F-FET PET but not by 18F-FDG PET. A subgroup analysis of patients with head-neck carcinomas allowed a better distinction between malignant and inflammatory tissues with 18F-FET than with 18F-FDG. Conclusion: 18F-FET is inferior to 18F-FDG as a PET tracer for general tumor diagnosis. Our preliminary results suggest rather selective uptake of 18F-FET in squamous cell carcinomas. Compared with 18F-FDG PET, 18F-FET PET may allow a better distinction between tumors and inflammatory tissues in patients with squamous cell carcinomas.
Radiolabeled amino acids have proven to be useful tracers in nuclear medicine, especially for the diagnosis of brain tumors as well as for peripheral tumors, such as lymphomas (1,2). In the majority of studies, PET with [methyl-11C]-l-methionine (MET) or [1-11C]-l-tyrosine has been applied; however, because of the short physical half-life of the 11C label (20 min), the use of these tracers remains restricted to a few PET centers with a cyclotron on site. SPECT with l-3-123I-iodo-α-methyltyrosine (IMT) has been shown to be an alternative for the investigation of cerebral gliomas (1,3,4); however, because of the poorer spatial resolution of SPECT, the diagnostic potential of the method remains inferior to that of PET.
In order to overcome the logistic disadvantages of 11C-labeled amino acids, several attempts have been undertaken to label amino acids with 18F (half-life, 110 min) (5,6). A very promising 18F-labeled amino acid is O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET), which can be synthesized with high radiochemical yields, allowing large-scale production for clinical purposes (7,8). Although 18F-FET is not incorporated into proteins, uptake into mammalian cells is stereospecific and is mediated by sodium-independent transport via system L as well as sodium-dependent transport via a system similar to system B0,+ (9,10). Initial clinical studies with 18F-FET PET in human brain tumors have shown results similar to those obtained with MET PET and IMT SPECT (11,12). A superior delineation of human solid gliomas by 18F-FET PET compared with MRI has been demonstrated by use of stereotactic biopsy samples as a reference (13,14). Furthermore, it has been shown in animal experiments that, compared with MET and 2-18F-FDG (18F-FDG),18F-FET exhibits low uptake in nonneoplastic inflammatory cells and in inflammatory lymph nodes and therefore promises high specificity for the detection of tumor cells (15,16). The purpose of this study was to investigate the diagnostic potential of 18F-FET for a series of peripheral tumors.
MATERIALS AND METHODS
Patients
Forty-four consecutive patients believed to have malignant peripheral tumors participated in this study. Six patients were excluded from further analysis because a malignant tumor could not be verified. Of the remaining 38 patients (14 women and 24 men; mean ± SD age, 61 ± 13 y; age range, 30–81 y), 7 had colorectal cancer, 6 had pancreatic cancer, 9 had head-neck cancer, 4 had lymphomas, 3 had lung cancer, 3 had ovarian cancer, 4 had breast cancer, and 2 had prostatic cancer. Individual data for the patients are given in Table 1. The study was approved by university ethics committees and by federal authorities. All subjects gave written informed consent for participation in the study.
Patient Data, Histologic Diagnosis, and Staging by 18F-FDG PET and 18F-FET PET
Radiopharmaceuticals
The amino acid derivative 18F-FET was produced by anion-activated nucleophilic 18F-fluorination of N-trityl-O-(2-tosyloxyethyl)-l-tyrosine tert butyl ester and subsequent deprotection to yield a specific radioactivity of >200 GBq/μmol by optimization of a previously described method (8). The uncorrected yield was about 35%, and the radiochemical purity was >98%. The tracer was administered as an isotonic neutral solution.
18F-FDG was synthesized as previously described (17). The average specific radioactivity was >200 GBq/μmol.
PET
All patients fasted for at least 12 h before the PET studies. After intravenous injection of 370 MBq of 18F-FET, whole-body PET scans were obtained starting at 1 h after injection. The duration of the whole-body PET scans ranged from 50 to 100 min, depending on the number of bed positions acquired. All patients underwent comparative investigations after intravenous injection of 370 MBq of 18F-FDG within 1 wk by use of the same scanning protocol. Blood glucose levels were checked before 18F-FDG injection to ensure that they were <130 mg/dL.
The studies were performed with a CTI ECAT Exact HR+ scanner (optimum full width at half maximum, 4.5 mm; 15-cm transaxial field of view). For attenuation correction, transmission scans with 3 68Ge/68Ga rotating line sources were used. After correction for random and scattered coincidences, dead time, and decay, image data were obtained by iterative reconstruction. Data were reconstructed with the manufacturer-supplied ordered-subset expectation maximization algorithm including attenuation correction (18).
Data Analysis
The data were evaluated in 2 separate sessions. In the first session, 18F-FDG and 18F-FET PET scans of all patients were visually analyzed for the presence of increased tracer uptake by 2 experienced nuclear medicine physicians with knowledge of clinical data. 18F-FET PET and 18F-FDG PET images were coregistered (MPI tool 3.28; ATV) (19) before evaluation to enable a direct comparison of the anatomic regions. A standardized uptake value (SUV) threshold of >2.5 was used for increased 18F-FDG uptake as reported previously (20). The cutoff for increased 18F-FET uptake (SUV > 2.0) was derived from whole-body distribution studies (21). The numbers of regions with abnormal tracer uptake indicative of a tumor were documented by consensus (1 to 5 or >5). Scan findings were staged according to the International Union Against Cancer (22) with modification of the T status as follows: T(+) for primary tumor present and T(−) for primary tumor absent. A quantitative comparison of 18F-FDG and 18F-FET in all patients was not performed because no pathologic 18F-FET accumulation could be detected in the majority of patients. 18F-FDG PET scans were used as a reference because histologic confirmation was not available for all lesions.
In the second session, quantitative data analysis was done for a subgroup of patients with head-neck carcinomas that demonstrated increased uptake of 18F-FET, in contrast to most other tumor types. For these patients, analyses of correlations with CT, clinical findings, and histologic results were performed.
On the coregistered CT, 18F-FDG PET, and 18F-FET PET images, regions with increased tracer uptake were identified by computed analysis (MPI tool) with the above-mentioned thresholds. Regions of interest (ROIs) were drawn manually over the corresponding anatomic structures on the coregistered CT scans. Identical ROIs were transferred to the 18F-FDG and 18F-FET images for quantification to enable the comparison of 18F-FDG uptake and 18F-FET uptake in the same anatomic structure. SUVs for 18F-FET uptake and 18F-FDG uptake were calculated by dividing the mean radioactivity (kBq/mL) of the ROIs by the radioactivity injected per gram of body weight in the corresponding PET scans. For comparison of the SUVs for 18F-FET uptake and 18F-FDG uptake, the nonparametric Mann-Whitney U test was used. Differences were considered significant at a P level of <0.05.
RESULTS
18F-FET PET and 18F-FDG PET in All Patients
Similar results for staging by 18F-FDG PET and 18F-FET PET according to the International Union Against Cancer were found for 8 of 38 patients, and discordant results were found for 30 of 38 patients.
18F-FDG PET showed increased 18F-FDG uptake in 37 of 38 patients, and only 1 head-neck mucoid adenocarcinoma (patient 35) showed no increased uptake of 18F-FDG.
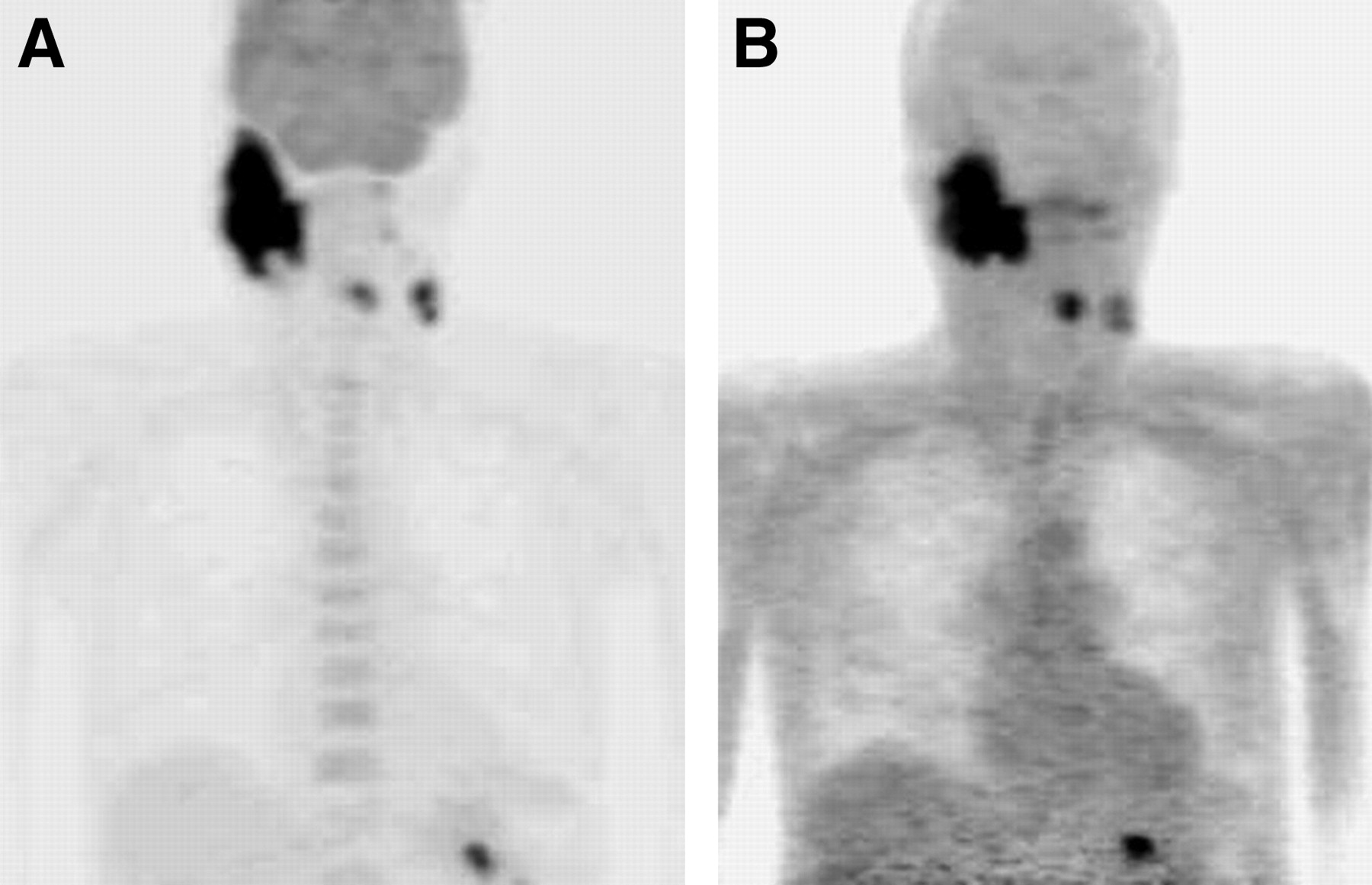
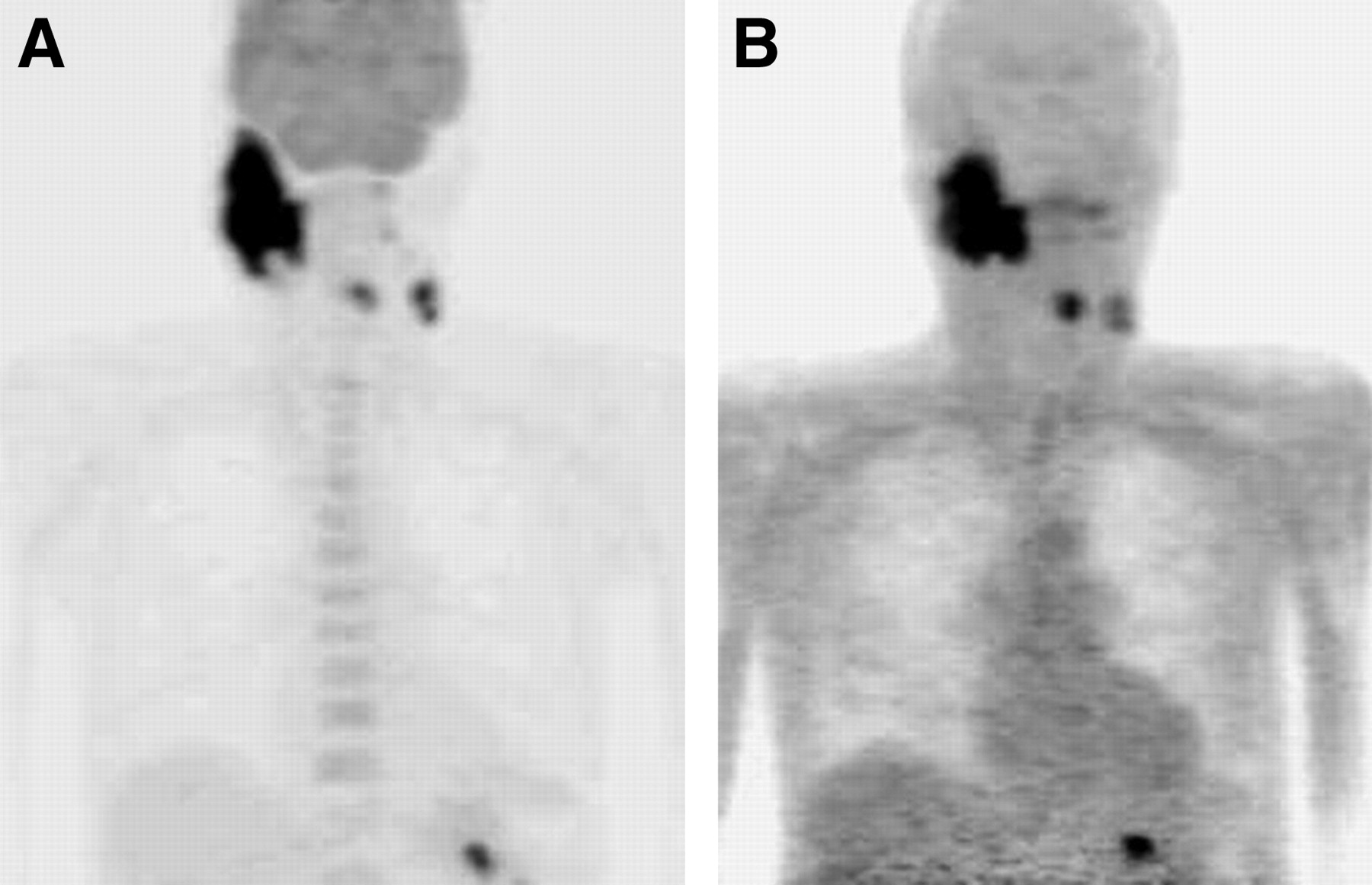
In contrast, 18F-FET PET was positive in only 13 of 38 patients (34%); these included 2 of 3 patients with lung carcinomas, 3 of 4 patients with breast carcinomas, and 8 of 9 patients with head-neck carcinomas. Increased 18F-FET uptake could not be identified in any of the patients with lymphomas, colorectal carcinomas, pancreatic carcinomas, ovarian carcinomas, or prostatic carcinomas (Fig. 1). Interestingly, all squamous cell carcinomas were found to be 18F-FET-positive tumors (8 head-neck carcinomas and 2 lung carcinomas), whereas most adenocarcinomas were found to be 18F-FET-negative tumors (in only 3 patients with infiltrating duct carcinomas of the breasts was increased 18F-FET uptake seen).

18F-FDG PET (A) and 18F-FET PET (B) of 81-y-old man (patient 2) with high-grade lymphoma (non-Hodgkin’s lymphoma). 18F-FDG shows high uptake in multiple lymph nodes, whereas 18F-FET uptake is negative in all lymph nodes.
All lesions with increased 18F-FET uptake exhibited concordant 18F-FDG accumulation, and no additional lesion was identified by 18F-FET PET but not by 18F-FDG PET. Detailed data for each patient are given in Table 1.
18F-FET PET and 18F-FDG PET in Patients with Head-Neck Carcinomas
Among patients with head-neck carcinomas, 8 of 9 patients were found to have squamous cell carcinomas and 1 of 9 patients was found to have an adenocarcinoma by subsequent histologic analyses. The adenocarcinoma was missed by both 18F-FDG PET and 18F-FET PET.
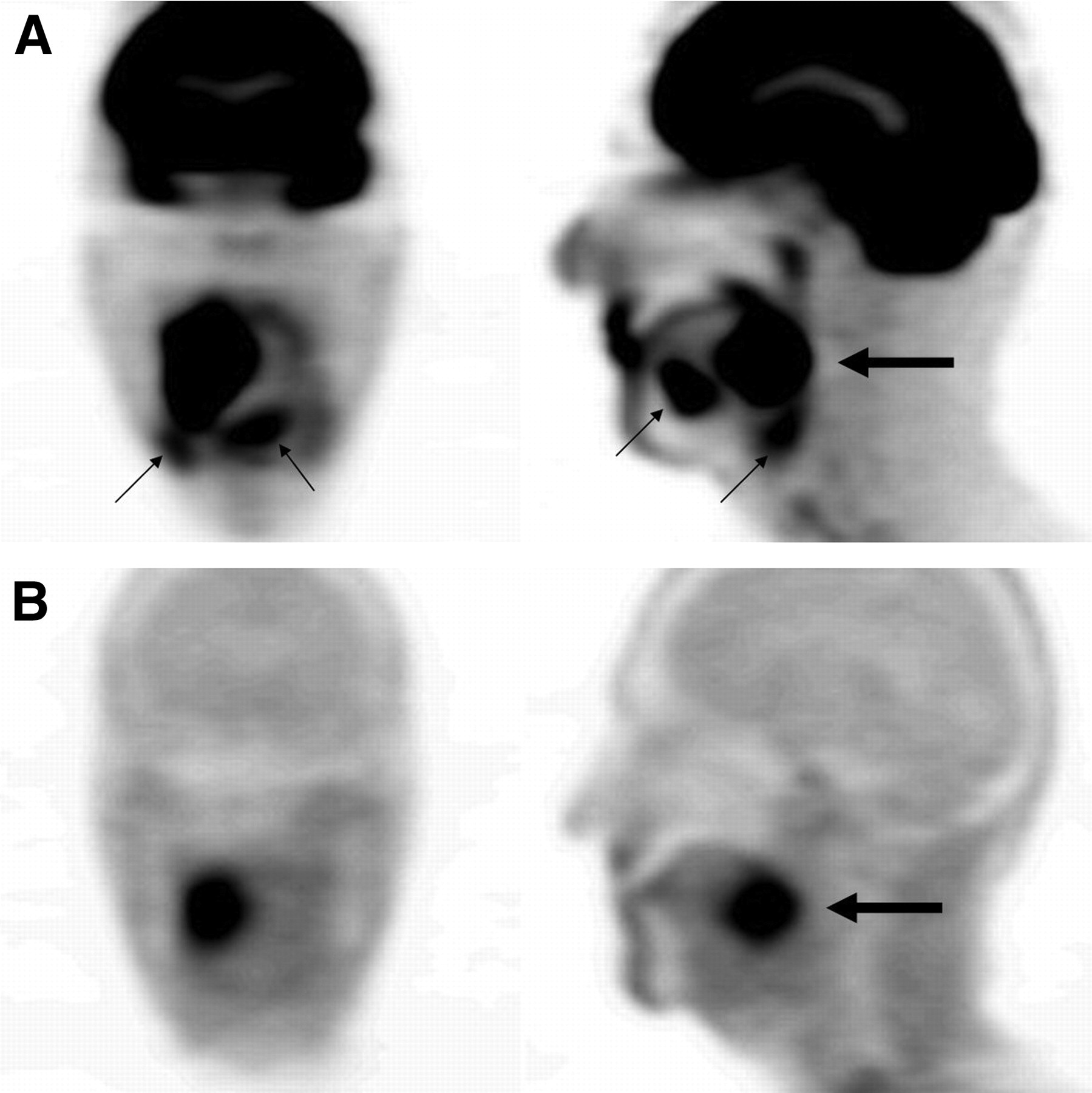
On 18F-FDG PET scans of patients with head-neck carcinomas, 31 lesions showing increased 18F-FDG uptake (SUV ≥2.5) were identified. Of the 31 lesions, 16 were tumorous and 15 were nontumorous, according to CT, clinical findings, and histologic results. On 18F-FET PET scans, 15 of the 16 tumorous lesions exhibited increased 18F-FET uptake and were correctly identified (Fig. 2); only 1 lymph node metastasis was missed on 18F-FET PET scans (SUV for 18F-FDG uptake, 3.3; SUV for 18F-FET uptake, 1.7). Among the nontumorous lesions, 18F-FET PET was superior to 18F-FDG PET; increased 18F-FET uptake was seen in only 2 of 15 lesions, and normal uptake was seen in 13 of 15 lesions (Fig. 3).
18F-FDG PET (A) and 18F-FET PET (B) of 63-y-old man (patient 32) with head-neck carcinoma (squamous cell carcinoma). Primary tumor and lymph node metastases are positive for both 18F-FDG and 18F-FET.

18F-FDG PET (A) and 18F-FET PET (B) of 61-y-old man with cancer of tongue (squamous cell carcinoma). Increased 18F-FDG uptake was noted in tumor (large arrow), and additional uptake was demonstrated in inflammatory tissues (small arrows). Increased 18F-FET uptake was noted only in tumor (large arrow).
The mean ± SD SUVs for 18F-FET uptake were significantly lower (P < 0.001) in tumorous (3.9 ± 2.1) and nontumorous (1.5 ± 0.4) lesions than the SUVs of 10.4 ± 6.3 and 3.7 ± 0.9, respectively, for 18F-FDG uptake.
DISCUSSION
In this study, we investigated the diagnostic potential of 18F-FET for the imaging of peripheral tumors. PET studies with 18F-FET for brain tumors have demonstrated high diagnostic accuracy (11–14), and experimental studies have shown a higher specificity of 18F-FET than of 8F-FDG and MET in the differentiation of inflammatory tissues from malignancies (15,16). Also, experimental colon carcinomas in mice exhibited increased 18F-FET uptake (9), but to date no clinical data are available concerning the behavior of 18F-FET in human tumors outside the brain.
Surprisingly, we found no increased uptake of 18F-FET in the majority of tumors, especially in lymphomas and most adenocarcinomas, in contrast to the results obtained with other tyrosine derivatives, such as 11C-l-tyrosine (23), 2-18F-fluoro-l-tyrosine (20), l-3-18F-fluoro-α-tyrosine (24), and IMT (25). Interestingly, all squamous cell carcinomas were found to be 18F-FET-positive tumors, whereas most adenocarcinomas were found to be 18F-FET-negative tumors.
The tumor-to-background contrast was significantly lower in PET scans with 18F-FET than in those with 18F-FDG, and some smaller lesions may have been missed in the 18F-FET PET studies because of the partial-volume effect. All of the primary tumors and the majority of the lymph node metastases, however, were large enough to be detectable by PET even in the presence of low 18F-FET uptake (Fig. 1).
We suggest that the absence of tracer uptake in most peripheral tumors is caused by different transport characteristics of 18F-FET and other tyrosine derivatives and is not attributable to the fact that 18F-FET, unlike 11C-l-tyrosine and 2-18F-fluoro-l-tyrosine, is not incorporated into proteins (7). Experiments with mice demonstrated that the inhibition of protein synthesis did not influence the uptake of MET in tumors and brains (26), suggesting that alterations in amino acid transport rather than increased protein synthesis caused increased uptake in tumors. Concordantly, a PET study with 2-18F-fluoro-l-tyrosine and kinetic modeling showed that the difference in uptake between tumors and normal tissues was attributable to an increase in tracer transport whereas binding to the metabolic compartment was not altered or even decreased in tumors (27).
Data on the transport characteristics for 18F-FET are still limited. Compared with the d-isomer, l-18F-FET showed 24-fold-higher uptake in the brains of nude mice, indicating stereoselective transport (7). An approximate 70% reduction in 18F-FET transport was observed in SW707 colon carcinoma cells with the amino acid analog 2-aminobicyclo-(2,2,1)-heptane-2-carboxylic acid (BCH). Although BCH is often regarded as a specific inhibitor of system L amino acid transport, this scenario is only true when transport assays are performed in the absence of Na+. Under physiologic conditions, BCH also inhibits Na+-dependent general amino acid transport via system B0,+ (28) and system B0 (29). In keeping with this notion, we found that the transport of 18F-FET in F98 rat glioma cells consisted of Na+-dependent activity of approximately 70% and Na+-independent activity of approximately 30% (2,10) and that both activities were sensitive to inhibition by BCH. As a result of our experiments, we suggest that Na+-independent 18F-FET transport occurs via system L and that Na+-dependent activity occurs via system B0,+. The transport of 18F-FET in F98 glioma cells was also inhibited by serine, which is a substrate of system L, system B0,+, and system B0 amino acid transport.
Amino acid transport via system L is currently thought to be mediated by 3 different proteins, namely, LAT1, LAT2, and LAT3 (30–33). The first 2 are composed of a light chain (LAT1 and LAT2) covalently linked to a heavy glycoprotein chain (4F2hc). Both subunits are necessary for functional expression. In contrast to the LAT1 and LAT2 subtypes, LAT3 does not require 4F2hc for functional expression. Although 4F2hc-LAT1 is found quite ubiquitously and is highly expressed in proliferating tissues and in tumors, 4F2hc-LAT2 is found only in tissues containing epithelial barriers (34). LAT3 has a rather restricted distribution and is found in liver, pancreas, and skeletal muscle.
As mentioned above, Na+-dependent transport of 18F-FET is likely to be mediated by amino acid transport via system B0,+ and system B0. The molecular correlates of these transporters are members of the SLC6 family encoded by cDNAs ATB0,+ (28) and B0AT1 (29). Both transporters are able to accumulate substrates several thousandfold.
Expression experiments with Xenopus oocytes showed that the radioiodinated tyrosine derivative IMT was selectively transported via the human LAT1 (hLAT1) subtype of system L, whereas the natural parent tyrosine was transported via both hLAT1 and hLAT2 (35). Recently, it was demonstrated by transstimulation experiments with Xenopus laevis oocytes after the expression of 4F2hc-LAT1 that 18F-FET influx via LAT1 was poor (36).
Several observations suggest that 18F-FET may be selectively transported via hLAT2. First, 18F-FET transport in F98 glioma cells is shared by serine (10), which is a substrate of hLAT2 but not of hLAT1. Second, 18F-FET shows no uptake in inflammatory tissues (15,16), in which hLAT2 is not expressed (37). Third, 18F-FET shows some retention in muscles (21), in which hLAT2 is expressed (38). Fourth, 18F-FET transport can be inhibited by BCH (10), which inhibits both hLAT1 transport and hLAT2 transport (29). In this study, 18F-FET did not accumulate in most adenocarcinomas, but we found increased uptake in all squamous cell carcinomas. As mentioned above, human 4F2hc (h4F2hc)–hLAT2 is highly expressed in tissues containing epithelial barriers (34), in agreement with the hypothesis of selective transport of 18F-FET via h4F2hc-hLAT2. The exact mechanisms of 18F-FET transport remain to be elucidated. Beside uptake via amino acid exchange transporters, such as hLAT2, actively accumulating systems, such as B0,+ and B0, must be considered. Further studies are required to discriminate among these possibilities.
From the clinical point of view, it is important to note that all 18F-FET-positive lesions in patients with squamous cell carcinomas also showed increased uptake of 18F-FDG and that the SUV for 18F-FDG uptake was significantly higher than that for 18F-FET uptake. No additional lesion was identified by 18F-FET PET but not by 18F-FDG PET. Thus, 18F-FET PET is not able to improve sensitivity for the detection of squamous cell carcinomas but may allow better distinction between tumors and inflammatory tissues. This finding must be confirmed with a larger series of patients. In head-neck carcinomas, for example, it is known that 18F-FDG has a low specificity (39,40).
Although 18F-FET is inferior to 18F-FDG for general tumor diagnosis, it is important to note that some amino acids exhibit higher selectivity for certain amino acid transporter subtypes after being labeled with iodine or fluorine than do their natural parents. This property not only may improve specificity in the differentiation of tumors and inflammatory tissues but also may indicate a possible use in the pretherapeutic assessment of antitumor drug selectivity. For instance, IMT and the phenylalanine mustard melphalan are transported by LAT1–4F2hc and accumulate in cancer cells (37,41).
CONCLUSION
18F-FET is inferior to 18F-FDG as a PET tracer for general tumor diagnosis. Our preliminary results suggest a rather selective uptake of 18F-FET in squamous cell carcinomas. Compared with 18F-FDG PET, 18F-FET PET appears to allow better distinction between tumors and inflammatory tissues in patients with squamous cell carcinomas.
Acknowledgments
The authors thank Elisabeth Theelen and Suzanne Schaden for assistance in patient studies and data analysis and Bettina Palm, Erika Wabbals, and Silke Grafmüller for technical assistance in the radiosynthesis of 18F-FET.
Footnotes
Received Jul. 3, 2004; revision accepted Oct. 21, 2004.
For correspondence or reprints contact: Dirk Pauleit, MD, Institute of Medicine, Research Center Jülich, P.O. Box 1913, 52425 Jülich, Germany.
E-mail: pauleit{at}web.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Combined PET Imaging of the Inflammatory Tumor Microenvironment Identifies Margins of Unique Radiotracer Uptake
- Pituitary Incidentaloma Found on O-(2-18F-Fluoroethyl)-L-Tyrosine PET
- Comparison of O-(2-18F-Fluoroethyl)-L-Tyrosine and L-3H-Methionine Uptake in Cerebral Hematomas
- Innovations in Radiotherapy Planning of Head and Neck Cancers: Role of PET
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Tumor Cell Metabolism Imaging
- Differential Uptake of O-(2-18F-Fluoroethyl)-L-Tyrosine, L-3H-Methionine, and 3H-Deoxyglucose in Brain Abscesses
- Fluorine-18-{alpha}-Methyltyrosine Positron Emission Tomography for Diagnosis and Staging of Lung Cancer: A Clinicopathologic Study
- Dynamic Imaging of Transient Metabolic Processes by Small-Animal PET for the Evaluation of Photosensitizers in Photodynamic Therapy of Cancer
- Molecular Imaging with 123I-FIAU, 18F-FUdR, 18F-FET, and 18F-FDG for Monitoring Herpes Simplex Virus Type 1 Thymidine Kinase and Ganciclovir Prodrug Activation Gene Therapy of Cancer
- 18F-FET PET Differentiation of Ring-Enhancing Brain Lesions
- 18F-FET PET Compared with 18F-FDG PET and CT in Patients with Head and Neck Cancer