


Abstract
The sensitivity of 18F-FDG PET to localize epileptogenic zones in frontal lobe epilepsy was evaluated by both visual assessment and statistical parametric mapping (SPM). Methods: Twenty-nine patients with frontal lobe epilepsy were examined. All patients showed good outcome after surgical resection (Engel class I or II). On pathologic examination, 22 patients had cortical dysplasia, 4 had tumors, 1 had cortical scars, and 2 had an old infarct. Hypometabolic lesions were found on 18F-FDG PET images by both visual assessment and SPM analysis. On SPM analysis, the cutoff threshold was varied and sensitivity to find epileptogenic zones was compared. Results: MRI showed structural lesions in 15 patients and normal findings in 14. 18F-FDG PET correctly localized the epileptogenic zones in 16 patients (55%) by visual assessment. The sensitivity of 18F-FDG PET was 36% in patients without structural lesions on MRI and 73% in patients with structural lesions. On SPM analysis, using an uncorrected probability value of 0.005 as the threshold, the sensitivity of SPM analysis was 66%, which was not statistically different from the sensitivity of visual assessment. The sensitivity decreased according to the decrease in probability value. Conclusion: 18F-FDG PET was sensitive in localizing epileptogenic zones by revealing hypometabolic areas in nonlesional patients with frontal lobe epilepsy as well as in lesional patients. SPM analysis showed a comparable sensitivity to visual assessment and could be used as an aid in diagnosing epileptogenic zones in frontal lobe epilepsy.
Frontal lobe epilepsy (FLE) is the second most common type of seizure after temporal lobe epilepsy. The prevalence of FLE has been reported to be 6%–30% among patients who underwent epilepsy surgery because of medically intractable seizures (1–6). Diagnosing neocortical epilepsy is more difficult than diagnosing medial temporal lobe epilepsy, either by ictal electroencephalography (EEG) or by neuroimaging studies. Not infrequently in FLE, scalp ictal EEG yields limited information mainly because of rapid propagation of an ictal discharge to the relatively larger distinctive anatomic areas (3,5–7). MRI often does not reveal structural abnormalities in patients with FLE, in contrast to patients with temporal lobe epilepsy (8–12). Variable structural abnormalities such as tumors, hamartoma, cortical dysplasia, vascular abnormality, gliosis, cerebromalacia, and posttraumatic changes cause FLE. MRI could localize only 50%–60% of these structural abnormalities.
18F-FDG PET has been used to localize the seizure focus by showing hypometabolism in the epileptogenic dysfunctional neuronal tissue. In medial temporal lobe epilepsy, the reported sensitivity of 18F-FDG PET for localizing the seizure focus is 85%–90%, with false lateralization being extremely rare (1,4, 13–15). However, in neocortical epilepsy, diagnostic accuracy and sensitivity were significantly lower. Later reports have suggested 45%–60% sensitivity (12,16–18). Compared with medial temporal lobe epilepsy, the location of the epileptogenic foci in FLE is more variable and in a larger area. Complicated functional interactions of the frontal lobes with other cortical areas may lead to diffuse changes in glucose metabolism in the other related areas.
For assessing an 18F-FDG PET image, visual inspection has been common in clinical practice. The results can be highly dependent on the observer’s expertise. Statistical parametric mapping (SPM) can provide an objective interpretation through an automated voxel-based analysis. SPM has already been successfully adopted in the interpretation of medial temporal lobe epilepsy (19–21). How to choose an area of hypoperfusion on the basis of the optimal threshold has yet to be determined in SPM analysis of epileptogenic zones.
In this study, the diagnostic performance of 18F-FDG PET in FLE was examined. SPM analysis as well as visual interpretation was applied to assess 18F-FDG PET images of FLE. We tried to determine the diagnostic performance of 18F-FDG PET and SPM and the optimal threshold of SPM in diagnosing hypometabolic zones in FLE.
MATERIALS AND METHODS
Patients
Twenty-nine patients (18 male, 11 female; age range, 12–51 y; mean age, 26 ± 10 y) with FLE were included in this study (Table 1). All were diagnosed as having FLE by a presurgical evaluation and had a good surgical outcome (Engel class I or II) after a mean follow-up (±SD) of 20 ± 11 mo after surgery. The mean duration of the disease was 12 ± 7 y. For presurgical evaluation of these patients, a careful clinical history was taken and a neurologic examination, prolonged scalp EEG in both the interictal and the ictal period, video monitoring of the seizure, brain MRI, and 18F-FDG PET were performed. Except for 3 cases of brain tumor, an invasive EEG study was performed using a subdural strip and grid electrodes. When the study results were discrepant, the surgical sites were determined on the basis of the invasive EEG studies.
Summary of Clinical, Neuroimaging, and Pathologic Findings
The control group for SPM analysis comprised 22 healthy volunteers (17 male, 5 female; mean age, 27 ± 8 y). All volunteershad no abnormal findings on MRI; had no history of neurologic disease, psychologic disease, or severe medical illness; and were taking no drugs known to affect brain 18F-FDG uptake.
18F-FDG PET Image Acquisition
The PET images were acquired using an ECAT EXACT scanner (CTI, Knoxville, TN/Siemens Medical Systems, Inc., Hoffman Estates, IL), which had an intrinsic resolution of 5.2 mm in full width at half maximum. The transmission scans were performed using 69Ge rod sources for 5 min to yield the attenuation maps. 18F-FDG (370 MBq) was injected intravenously, and the patients lay still with their eyes open in a quiet and dimly lit room. The emission image was acquired for 25 min with a 2-dimensional acquisition mode, 30–40 min after tracer injection. Forty-seven slices of the transaxial images were reconstructed using a filtered backprojection method with a Shepp-Logan filter (cutoff frequency, 0.35 cycle per pixel). The reconstructed images were corrected for attenuation using attenuation maps. The transaxial images were then realigned to yield sagittal and coronal images.
Visual Interpretation of 18F-FDG PET
The cerebral cortex was divided into 5 areas in each hemisphere (frontal, parietal, lateral temporal, medial temporal, and occipital). Two nuclear physicians who were unaware of the clinical findings and final diagnosis assessed the regional metabolism. The most hypometabolic region on the 18F-FDG PET scan was determined to be the epileptogenic zone.
Analysis of 18F-FDG PET by SPM
Spatial preprocessing and statistical analysis were performed using SPM 99 software (Institute of Neurology, University College of London, London, U.K.) implemented in Matlab 5.3 (The MathWorks, Inc., Natick, MA). All reconstructed 18F-FDG PET images were spatially normalized into Montreal Neurological Institute (McGill University, Montreal, Quebec, Canada) standard templates by affine transformation (12 parameters for rigid transformations, zooms, and shears) and nonlinear transformations. The normalized images were smoothed by convolution with an isotropic gaussian kernel having a 16-mm full width at half maximum to increase the signal-to-noise ratio.
The effects of global metabolism were removed by normalizing the count of each voxel to the total count of the brain using proportional scaling. Each patient image was compared with the images of healthy volunteers at every pixel, using an unpaired t test based on 2 contrasts to detect any regional decrease in metabolism. At a variable voxel height threshold that had a probability value with or without a correction for multiple comparisons, clusters consisting of a minimum of 50 contiguous voxels were considered significantly different. The results were displayed on the 3 orthogonal planes of an MRI template. The area with the highest significance was considered to be the seizure focus.
Surgery, Pathologic Findings, and Surgical Outcome
The extent of the resection was determined according to subdural ictal EEG findings. A radical frontal lobectomy was performed on 6 patients, a standard frontal lobectomy on 6, a partial frontal lobectomy on 5, and a lesionectomy on 12. The pathologic examination revealed 22 cases of cortical dysplasia, 4 low-grade tumors (2 oligodendrogliomas, 1 ganglioglioma, and 1 astrocytoma), 1 cortical scar, and 2 old ischemic lesions. Twenty-four patients were seizure free (Engel class I), and 5 patients had rare seizures during the follow-up after surgery (Engel class II).
Statistical Analysis
The Cochran Q test and the McNemar test were performed to examine the difference between the sensitivity of MRI and the visual or various SPM analyses of 18F-FDG PET for localization of the seizure focus. A Fisher exact test was performed to compare the sensitivity of 18F-FDG PET according to the presence of abnormality on MRI. P < 0.05 was considered statistically significant.
RESULTS
MRI Findings
MRI findings were normal in 14 of the 29 patients, and structural lesions were found in the other 15 (Table 1). Of these 15, 12 had localized structural lesions indicating epileptogenic foci. Their MRI diagnosis included focal cortical dysplasia, heterotopia, cerebromalacia, granuloma, calcification, or tumor. For these localized structural lesions, the sensitivity for localizing seizure focus was 41% (12/29) (Fig. 1). The other 3 did not yield localizing findings; one had bifrontal cerebromalacia, another had multifocal lesions, and the last had hemispheric atrophy.
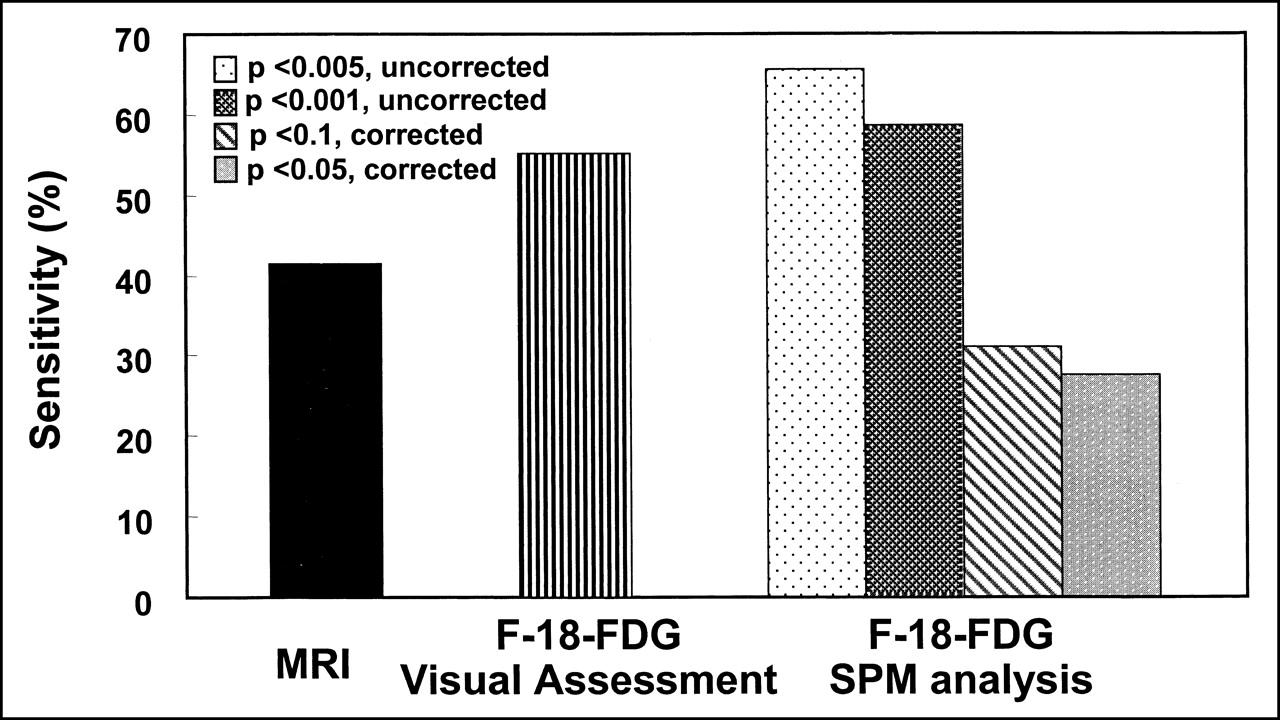
Sensitivities of MRI, 18F-FDG PET by visual assessment, and SPM analysis.
Diagnostic Performance by Visual Interpretation of 18F-FDG PET
Among the 29 patients, the most hypometabolic lesion was found in frontal lobes in 16 patients. The sensitivity for correct localization was 55% (16/29) (Fig. 1). The hypometabolic area extended to the temporal lobe in 2 patients and the entire ipsilateral hemispheric area in the other 2. In these 4 patients, lateralization was successful but localization was not. In another 9 patients, no abnormal hypometabolic areas were found. Lateralization rate was 69% (20/ 29).
Among the 15 patients with structural abnormalities on MRI, localization was successful in 11 on 18F-FDG PET (Table 2). Localization rate was 73%. In patients with multifocal or bifrontal structural lesions, the regional metabolism was lowest at the seizure focus, making possible the correct identification of the seizure focus.
18F-FDG PET Findings (Visual Interpretation) According to MRI Findings
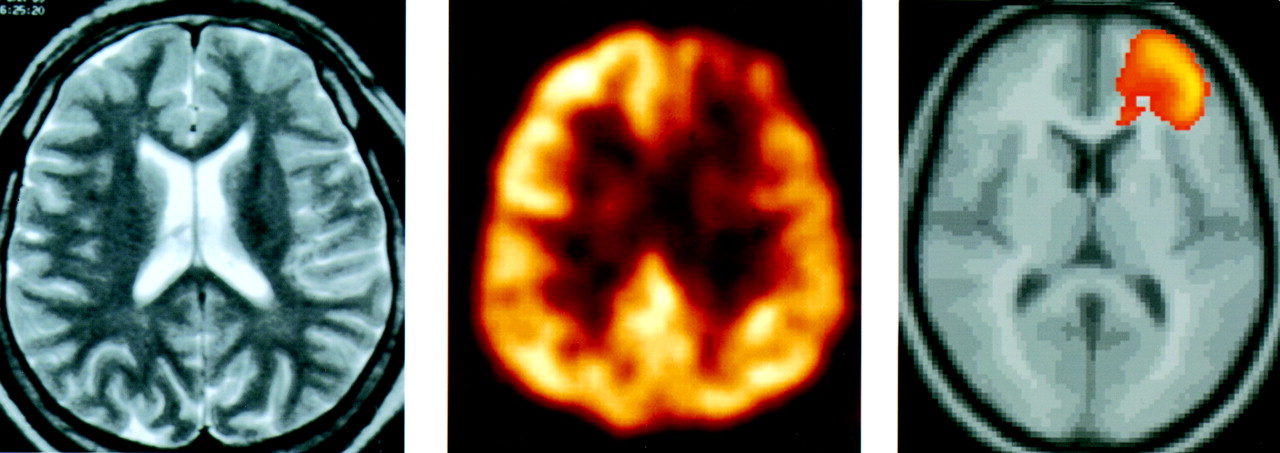
Among the 14 patients without structural lesions on MRI, the hypometabolic area was found in the frontal lobe on 18F-FDG PET in 8 patients (Table 2). Lateralization rate was 57%. Exact localization was possible in 5 patients (Fig. 2). Localization rate was 36%. The sensitivity for localization was higher in patients with structural lesions than in patients with normal MRI findings (P < 0.01).
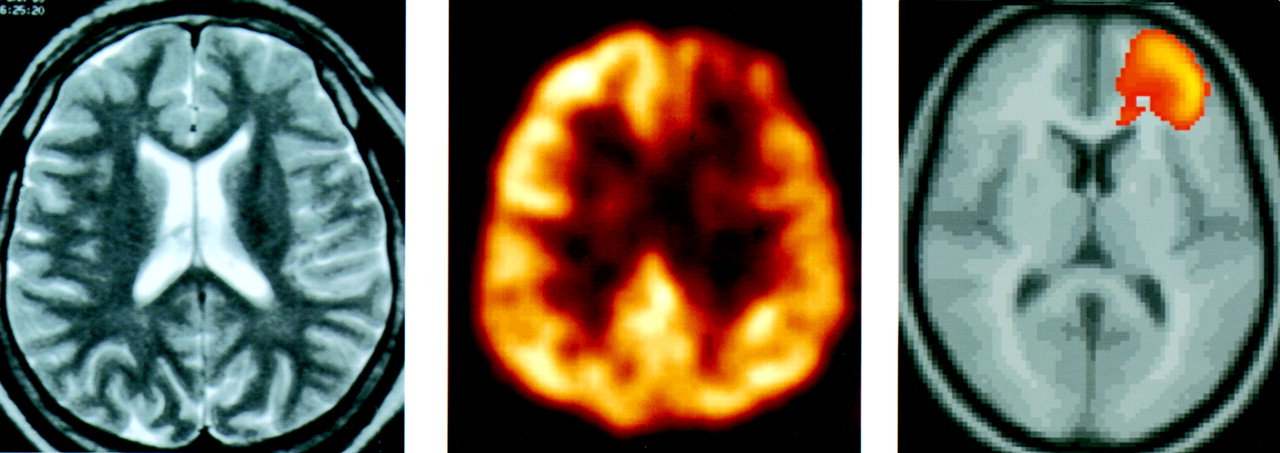
A 16-y-old boy with left FLE (Table 1; patient 2). From left to right, brain MRI findings were normal, 18F-FDG PET showed decreased metabolism in left frontal lobe, and SPM (P < 0.05, corrected) gave same finding. After left frontal lobectomy, he was seizure free during follow-up of 15 mo.
SPM Analysis Results for 18F-FDG PET
Two patients showing severe hypometabolism with tissue atrophy (patients 15 and 17 in Table 1) were excluded from the SPM analysis because the spatial and count normalizations were not acceptable. These 2 were considered as failures in the analysis.
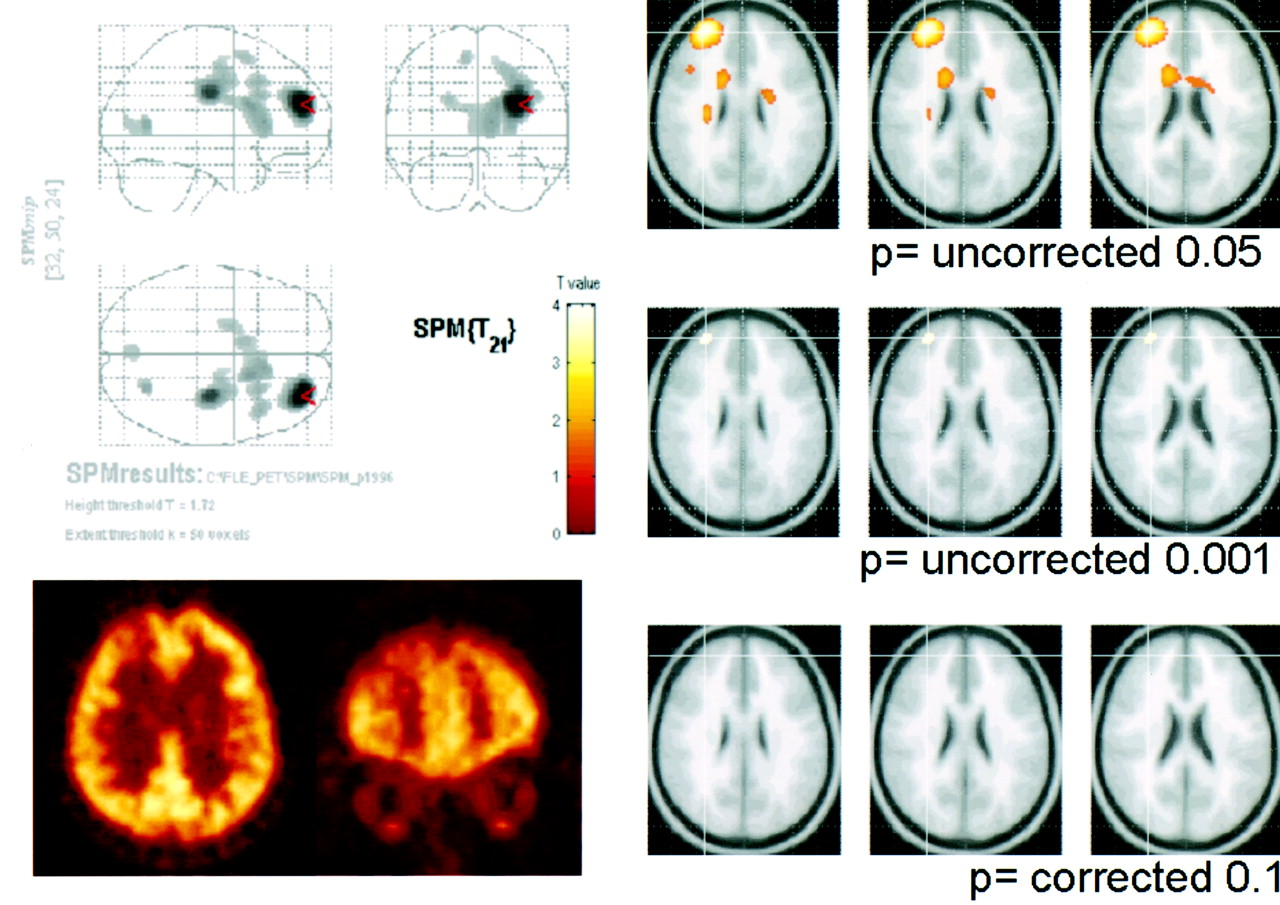
The sensitivity of the 18F-FDG SPM analysis was 66% (19/29) at P < 0.005 (z score, 2.58) and 59% (17/29) at P < 0.001 (z score, 3.09) (Fig. 1). Furthermore, at the threshold of a corrected probability value of 0.1 or 0.05 for multiple comparisons, lateralization of the epileptogenic focus was correct in 9 and 8 patients, respectively. Sensitivity was 31% at a corrected P < 0.1 and 28% at a corrected P < 0.05 (Fig. 1). SPM analysis had a tendency to be more sensitive than visual assessments at the voxel height threshold of P < 0.005 or 0.001 (uncorrected). However, the increase in sensitivity was not statistically significant (McNemar test, P = not statistically significant). Figure 3 is an example of SPM analysis results at varying thresholds.

Example of SPM analysis with varying threshold (Table 1; patient 16). According to cutoff value of voxel height, SPM analysis became less sensitive when stricter criterion was applied.
Comparison of Visual Interpretation and SPM Analysis
With a probability value of 0.005 (uncorrected), a concordant result between the visual and SPM analyses was obtained for 18 patients, with correct localization in 12 patients and failure to localize in 6 (Table 3).
Comparison of Localization Results of Visual Assessment and SPM Analysis of 18F-FDG PET
Of 16 patients with correct localization by visual assessment of 18F-FDG PET images, SPM analysis revealed a significantly hypometabolic area in the epileptogenic frontal lobe in 12 (Table 3). In the other 4 patients, localization failed because of the presence of significant hypometabolic areas in the bifrontal or temporo-occipital lobes at the predetermined threshold (P < 0.005, uncorrected) and also at a more significant threshold (P < 0.001, uncorrected). In 3 of the 4 patients with only possible lateralization by visual assessment, the epileptogenic focus in the frontal lobe was found to be the lowest hypometabolic area in SPM analysis (Fig. 4).
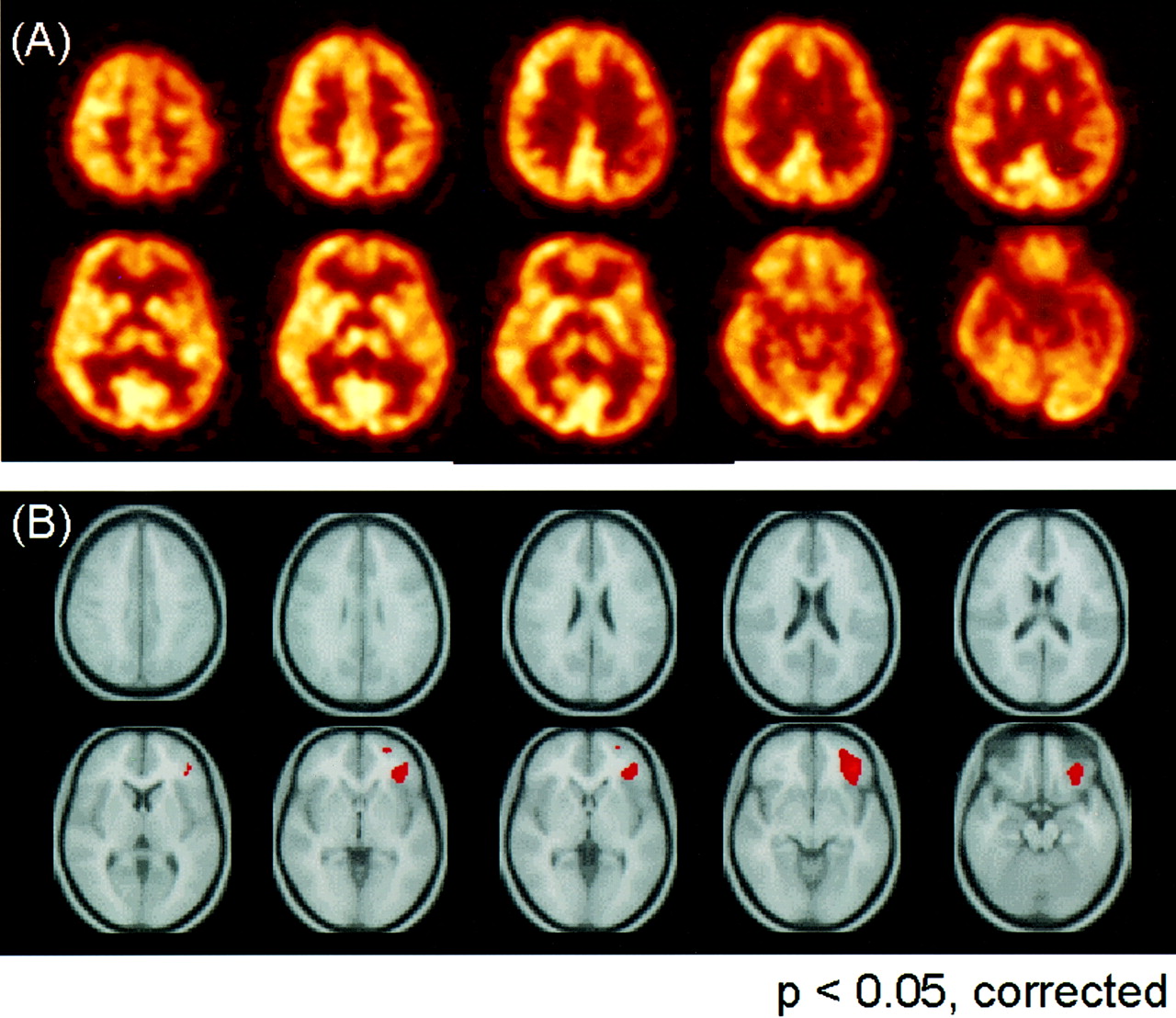
A 24-y-old woman with intractable partial seizure (Table 1; patient 9). Her MRI findings were normal. (A) In 18F-FDG PET scan, widely decreased metabolism in left hemisphere was detected visually. (B) SPM showed localized decrease in metabolism in left inferior frontal lobe (P < 0.005, uncorrected). After left inferior frontal lobectomy, she was seizure free.
In 4 of 9 patients showing no abnormal hypometabolic lesion by visual assessment, the epileptogenic focus could be correctly identified by SPM analysis. In the other 5, correct localization was not possible because the SPM result showed normal or significant hypometabolism in multiple cortical areas and even contralateral lesions.
DISCUSSION
Surgical resection of the epileptogenic focus has gained popularity as a method for treating medically intractable partial epilepsy. The result generally is not as good after FLE surgery as after anterior temporal lobe resection in patients with medial temporal lobe epilepsy (1,5, 22–25). The poor outcome in FLE has been attributed to the difficulty of localizing the seizure focus. FLEs have diverse behavioral manifestations, EEG patterns, and etiologies. The rapid spread of an ictal discharge or a propensity for bilateral presentation of the abnormal neuronal activity often masks the true ictal discharge (3,5–8,26–28). The other conventional diagnostic imaging tools are also not satisfactory for locating the seizure focus in FLE (8–12).
It has been accepted that, like medial temporal lobe epilepsy, neocortical epilepsy with a well-defined structural abnormality has a more favorable surgical outcome (13,25,29). In this study, a hypometabolic lesion as a seizure focus was found more easily by 18F-FDG in patients with structural lesions identified by MRI. The correct localization rate was 73% in patients with structural abnormalities, in contrast to 35% in patients with normal MRI findings.
Approximately 45% of FLE was reported as being idiopathic or cryptogenic. The importance of localizing the seizure focus in patients without structural lesions is increasing. Although almost half of the patients in our series did not show anatomic abnormalities, they underwent surgical resection and had a satisfactory outcome. Recent studies have shown that the presence of hypometabolism on 18F-FDG PET images is an indicator other than the presence of a structural lesion that predicts a good prognosis (29,30).
In FLE, as in other neocortical or medial temporal lobe epilepsies, the metabolic abnormalities identified by 18F-FDG were most prominent in structural lesions; only the extent and degree varied. In FLE, metabolic abnormalities could be observed in the larger area including the temporal, parietal, and ipsilateral basal ganglia and the thalamus (17,19, 31–34). In terms of lateralization, 18F-FDG showed a favorable 57% rate even in nonlesional FLE. However, as for localization rate, visual interpretation was not successful or was subject to operator bias. In the determination of which area is epileptogenic among the larger hypometabolic areas, subjective qualitative visual interpretation needs help from objective quantitative assessment.
Recently, SPM has been accepted as a standard analytic method in functional neuroimaging. Before SPM was introduced to evaluate epilepsy patients, an effort to assess 18F-FDG PET more objectively was made by Swartz et al. (12). They assessed the 18F-FDG PET scans of FLE patients using quantitative normalized analysis by manually drawing 87 regions of interests. The sensitivity of quantitative analysis was 96%—much higher than the 52% sensitivity for qualitative analysis in their studies. However, their regions of interest were subject to operator expertise, and reproducibility has yet to be validated by other investigators.
Afterward, SPM analysis was introduced and shown to be applicable to the interpretation of individual cases of epileptic disorders rather than group controls (35). This SPM analysis has already been applied successfully to assess 18F-FDG PET in medial temporal lobe epilepsy (20, 21,36). Van Bogaert et al. (20) showed that SPM analysis identified hypometabolism in the seizure focus through an individual-to-group comparison. However, in medial temporal lobe epilepsy, we speculate that because the regional glucose metabolic changes are so prominent and localized in the epileptogenic temporal lobes, there would not have been much room for enhancing the sensitivity. Therefore, we hypothesized that for FLE, SPM analysis will improve the sensitivity of 18F-FDG PET, which had a relatively lower sensitivity than for temporal lobe epilepsy. In this study, SPM analysis yielded equivalent results to human experts but did not yield significant incremental information despite its objective and quantitative interpretation. On the contrary, when we tried to decrease type I error by decreasing probability value or by correction for multiple comparisons, the sensitivity in finding epileptogenic zones decreased abruptly.
We supposed there was remote possibility that patients had additional seizure foci besides the focus in the frontal lobe, because all patients had a good surgical outcome. Otherwise, the additional hypometabolic areas might have yielded false-positive areas. Although we used the criterion that the area with the highest significance was considered to be the seizure focus, it is still an open question how one can choose a real epileptogenic zone among several candidate hypometabolic lesions on 18F-FDG SPM images or what the associated hypometabolic lesions would mean.
SPM analysis was helpful in half of the 9 patients whose hypometabolic area was not clearly discernible on visual interpretation (Table 3). In these patients, in a retrospective contemplation, the SPM results increased our confidence than an observed hypometabolic area had possible epileptogenic significance. In addition to visual assessment, SPM was able to identify the seizure focus in 7 of the 29 patients. However, in 3 of 16 patients with a correct visual localization, SPM failed to identify the seizure focus. In these 3 patients, the principal hypometabolic areas were bilateral, with a similar significance in the frontal lobes. SPM analysis could not be performed on 2 patients. Furthermore, SPM sometimes fails in normalizing individual PET images, especially when the structural lesion is large in such cases as severe hemiatrophy and a huge structural lesion. This failure is a failure at the stage of spatial normalization; however, if spatial normalization were performed successfully, statistical inference would still be a problem. With this reasoning, and taking the results of this study into consideration, we suggest that both visual interpretation and SPM analysis should be consulted simultaneously for localizing epileptogenic zones on 18F-FDG PET images in FLE.
CONCLUSION
In this study, the diagnostic performance of 18F-FDG PET in FLE was evaluated and SPM analysis was applied to examine the 18F-FDG PET images. 18F-FDG PET showed good sensitivity for localizing the seizure focus in FLE by visual interpretation. Although the sensitivity for identifying the seizure focus was not significantly improved by SPM analysis, SPM analysis was useful for interpreting cases with equivocal results on visual assessment. SPM analysis provided more objective and easily interpretable results in a presurgical evaluation of FLE patients.
Footnotes
Received Nov. 30, 2001; revision accepted Apr. 26, 2002.
For correspondence or reprints contact: Dong Soo Lee, MD, Department of Nuclear Medicine, Seoul National University Hospital, 28 Yungun-dong, Chongno-gu, Seoul, Korea.
E-mail: dsl{at}plaza.snu.ac.kr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improving 18F-FDG PET Quantification Through a Spatial Normalization Method
- Age-Specific 18F-FDG Image Processing Pipelines and Analysis Are Essential for Individual Mapping of Seizure Foci in Pediatric Patients with Intractable Epilepsy
- Glucose Metabolic Profile by Visual Assessment Combined with Statistical Parametric Mapping Analysis in Pediatric Patients with Epilepsy
- The Role of Radionuclide Imaging in Epilepsy, Part 1: Sporadic Temporal and Extratemporal Lobe Epilepsy
- The Role of Radionuclide Imaging in Epilepsy, Part 1: Sporadic Temporal and Extratemporal Lobe Epilepsy
- A gut feeling about insular seizures
- Multimodality imaging in the surgical treatment of children with nonlesional epilepsy
- FDG-PET improves surgical outcome in negative MRI Taylor-type focal cortical dysplasias
- Objective Detection of Epileptic Foci by 18F-FDG PET in Children Undergoing Epilepsy Surgery
- EEG-fMRI: Adding to standard evaluations of patients with nonlesional frontal lobe epilepsy
- Efficacy Assessment of Cerebral Arterial Bypass Surgery Using Statistical Parametric Mapping and Probabilistic Brain Atlas on Basal/Acetazolamide Brain Perfusion SPECT