


Abstract
The efficacy of cerebral arterial bypass surgery was assessed on brain perfusion SPECT using statistical parametric mapping (SPM) and a probabilistic brain atlas. Methods: Fifteen patients with ischemia in the internal carotid artery (ICA) territory and 21 age-matched healthy volunteers were enrolled. 99mTc-HMPAO basal/acetazolamide brain perfusion SPECT was performed 2 wk before and after bypass surgery and also on a healthy control group. Using SPM analysis, group comparisons were made between pre- and postoperative SPECT for each basal/acetazolamide image, and improvements of perfusion and perfusion reserve were assessed. The number of significant voxels on the SPM analysis was defined as the extent of ischemia. With the use of the probabilistic brain atlas, the counts for the cerebral lobes and the ICA territory were automatically calculated for each image and compared. Results: The group comparisons by SPM between patients and healthy volunteers showed a significant improvement in general perfusion status in the ICA territory. The improvement in perfusion reserve was more extensive than the improvement in perfusion. The extent of ischemia was also significantly decreased after surgery (1,693 ± 2,604 to 371 ± 523 voxels in basal images, P = 0.060; 11,879 ± 6,449 to 5,997 ± 3,864 voxels in acetazolamide images, P = 0.005). In the analysis using the probabilistic brain atlas, the preoperatively decreased perfusion was normalized after surgery, but a residual decrease in the perfusion reserve was also observed in the ICA territory. The counts in the volume of interest of the ICA territory were significantly improved (38.5 ± 4.1 to 41.5 ± 2.7 in basal images, P = 0.024; 34.2 ± 4.4 to 38.8 ± 2.9 in acetazolamide images, P = 0.003). One patient showing a decrease in perfusion had a perioperative cerebral infarct. Conclusion: Using SPM and a probabilistic brain atlas, the perfusion, the perfusion reserve, and changes in both after cerebral arterial bypass surgery were effectively assessed and correlated well with physiologic reasoning.
In the case of cerebral ischemia caused by arterial stenosis, medical treatment alone is insufficient for a good prognosis (1), and bypass surgery or other surgical procedures may prevent an acute cerebral infarct (2–5). However, because such surgical procedures have operation-related risks of infarct or hemorrhage, the surgery should be clearly indicated. Because patients with a decreased perfusion reserve have a much higher risk of an infarct or hemorrhage than do patients with a preserved reserve (1), evaluation of the perfusion reserve is necessary before surgery (1–5).
The perfusion reserve can be evaluated by acetazolamide-challenged brain perfusion SPECT (6–9). With the challenge of acetazolamide, perfusion is increased in the area where the perfusion reserve is preserved, whereas the area of decreased perfusion reserve shows no increase or decrease in perfusion (8). Using basal/acetazolamide brain perfusion SPECT, the pre- and postoperative statuses of the perfusion and perfusion reserve can be evaluated in cerebral arterial bypass surgery (5). However, visual assessment of basal/acetazolamide brain perfusion SPECT is operator dependent and mostly qualitative (10). Although some researchers have tried to draw a region of interest (ROI) and to quantify regional counts for the objective and quantitative evaluations, this is also operator dependent and therefore not reproducible (11).
A recently developed algorithm for image realignment and transformation is now applied to various brain images. Diverse brain images can be spatially normalized to a template and objectively interpreted at the level of voxel region or automatically determined. The methods of statistical parametric mapping (SPM) and probabilistic brain atlas are now generally used for interpreting images in neurocognitive studies. These analytic methods have also been applied successfully to the interpretation of 18F-FDG PET and brain perfusion SPECT (12–16) in cases of epilepsy. However, these methods are not commonly applied to cerebral vascular diseases.
In this study, SPM and a probabilistic brain atlas were applied to basal/acetazolamide brain perfusion SPECT images of patients who underwent external-carotid-to-internal-carotid bypass surgery (EC/IC bypass).
MATERIALS AND METHODS
Patient Population
Fifteen patients (7 men, 8 women; mean age ± SD, 49 ± 17 y) were enrolled in this study. All patients were diagnosed with cerebral ischemia that was due to stenosis in the internal carotid artery (ICA), mainly in the middle cerebral artery (MCA), and underwent bypass surgery of the superficial temporal artery to the MCA (Table 1). To perform group analyses, only the patients with 1-sided (left) lesions were included in the study. Although found in some patients, stenoses in the contralateral side were regarded as insignificant because they were accompanied by neither neurologic symptoms nor perfusion abnormalities on SPECT.
Clinical Characteristics of Patients
As a control group, 21 healthy volunteers (10 men, 11 women; mean age ± SD, 59 ± 5 y) were also enrolled after they gave informed consent. They underwent neurologic examination, the Mini-Mental State Examination, and other neuropsychological tests, with normal results.
Study Protocol
Basal/acetazolamide brain perfusion SPECT was performed 2 wk (17 ± 9 d) before and 2 wk (17 ± 34 d) after the bypass surgery. With the patient resting, basal SPECT was performed 5 min after an intravenous injection of 555 MBq of 99mTc-hexamethylpropyleneamine oxime (HMPAO). Ten minutes before the end of the basal SPECT, 20 mg of acetazolamide per kilogram of body weight were injected intravenously, and another 1,110 MBq of 99mTc-HMPAO were injected at the end. A second SPECT examination was performed 5 min after the end of basal SPECT. A decay-corrected subtraction of the basal image from the second SPECT image was performed, and this image was defined as the acetazolamide SPECT image. All details of the protocol were the same as previously reported (11,17,18).
The SPECT images were acquired using a triple-head γ-camera (Prism 3000; Picker International) with a low-energy high-resolution fanbeam collimator. Forty step-and-shoot images were acquired, with intervals of 3° for 20 s per step. The images (128 × 128 matrix) were reconstructed with filtered backprojection using a Metz filter.
SPM Analysis
SPM99 software (Institute of Neurology, University College of London) implemented in MATLAB 5.3 (The MathWorks, Inc.) was used for spatial preprocessing and analysis. The basal and acetazolamide SPECT images were realigned with each other and were spatially normalized into the standard SPECT template of the Montreal Neurological Institute (McGill University) using affine and nonlinear transformation (12–14). To remove the effect of the difference in the overall counts, the voxel counts were normalized to the mean voxel count of the gray matter in each SPECT image using proportional scaling.
The basal and acetazolamide images were compared between pre- and postoperative SPECT using a group comparison with an unpaired t test. Also, another parametric image of cerebral vascular reserve index (CVRI) was defined in each voxel, as follows, and compared again:
 where Cacetazolamide is the counts on acetazolamide images and Cbasal is the counts on basal images. An uncorrected value of P < 0.01 was set as the threshold, and clusters comprising a minimum of 100 contiguous voxels were considered significant.
where Cacetazolamide is the counts on acetazolamide images and Cbasal is the counts on basal images. An uncorrected value of P < 0.01 was set as the threshold, and clusters comprising a minimum of 100 contiguous voxels were considered significant.
To define the extent of the decrease in perfusion or perfusion reserve, the individual images were compared with those of the control group using the same method on the SPM. The number of significant voxels was defined as the extent of the decrease in perfusion or perfusion reserve.
Quantitative Analysis Using Probabilistic Brain Atlas
A statistical probabilistic anatomic map (SPAM) of the International Consortium for Brain Mapping was applied to objectively draw VOIs. SPAM consists of 98 VOIs in a single image, where each voxel has the probability of belonging to a specific VOI.
After spatial normalization, the counts of each SPECT image were normalized using proportional scaling, with the mean counts of the cerebellum set at 50. The normalized counts were multiplied by the probability of the SPAM and were determined as the count of each VOI. The cerebral lobar counts were then calculated by averaging the counts of the VOIs that had been reclassified into each lobe. The lobar counts of the basal, acetazolamide, and CVRI images were calculated for each pre- and postoperative SPECT image. In addition to these lobar counts, the counts of the ICA territory were directly calculated using another probabilistic brain atlas, including the ICA territory as one of the VOIs (19).
Statistical Analysis
A Wilcoxon test was performed to compare the pre- and postoperative counts, and a Mann–Whitney test was performed to compare the counts of the patient and control groups. A value of P < 0.05 was considered significant.
RESULTS
Evaluation of Perfusion Status Using SPM
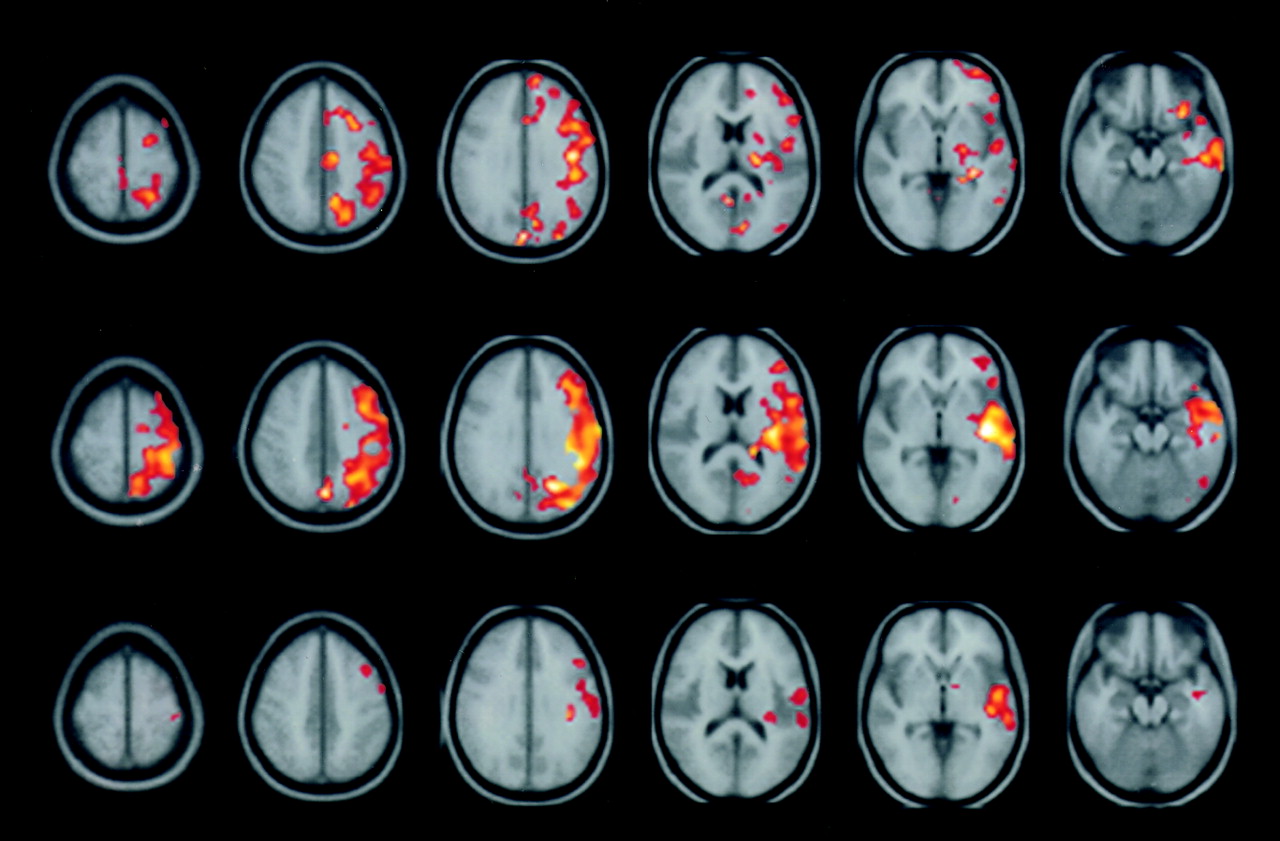
In the group comparison between pre- and postoperative SPECT, scattered improvement in basal perfusion was found throughout the whole left cerebral hemisphere. The improvement was more obvious and extensive on acetazolamide SPECT. However, the improvement was confined to a smaller area around the proximal vascular territory of the MCA in the parametric images of the CVRI (Fig. 1). In an analysis of extent, the numbers of voxels were decreased from 1,693 ± 2,604 to 371 ± 523 in basal images and from 11,879 ± 6,449 to 5,997 ± 3,864 in acetazolamide images (Fig. 2). The decreases was not statistically significant in basal images (P = 0.060) yet were significant in acetazolamide images (P = 0.005). Two patients showed an increase in extent, and one of them had a perioperative cerebral infarct.

Comparison of pre- and postoperative images using SPM. Basal images show scattered areas of improvement, whereas acetazolamide images show more extensive areas of improvement. CVRI images show more confined areas of improvement around the proximal MCA territory.

Changes in the numbers of significant voxels on SPM. The numbers of significant voxels in comparison with the control group represent the extent of the abnormality. The postoperative numbers of voxels were significantly lower than the preoperative numbers.
Evaluation of Perfusion Status Using Probabilistic Brain Atlas
On the preoperative images, the counts for all the cerebral lobes and the ICA territory were significantly lower than in the control group. Although the decrease was evident in all basal, acetazolamide, and CVRI images, it was more prominent in the acetazolamide images than in the basal images (Table 2). The counts were significantly improved postoperatively with the exception of the occipital lobe, which showed mildly decreased preoperative counts.
Counts of Each Lobe in the Analysis Using the Probabilistic Brain Atlas
In the comparison between the images of the control group and the postoperative images, the basal counts were normalized in the temporal, parietal, and occipital lobes and in the ICA territory with the exception of the frontal lobe. However, the perfusion reserve, which was represented in the acetazolamide and CVRI images, was still lower than in the control group, although it was significantly improved from the preoperative state (Table 2).
In the individual analysis, 13 patients showed postoperative improvement of the counts in the basal and acetazolamide images (Fig. 3). One of the 2 patients who showed a decrease in counts also had a perioperative infarct. The increases in counts were significant in both the basal images (38.5 ± 4.1 to 41.5 ± 2.7, P = 0.024) and the acetazolamide images (34.2 ± 4.4 to 38.8 ± 2.9, P = 0.003).

Changes in the ICA territory counts using the probabilistic brain atlas. The basal and acetazolamide counts of all but 2 patients improved after surgery. One patient, showing a significant decrease in counts, was proven to have a perioperative cerebral infarct.
DISCUSSION
About 2 decades ago, EC/IC bypass was reported as ineffective in the prevention of ischemic stroke in cerebrovascular disease (20). However, several authors recently reported that EC/IC bypass is helpful in discreetly selected cases in which transient ischemic attack or unstable hemodynamics is involved (3–5). Because the surgical procedure still has high perioperative morbidity and mortality, strict indication criteria are required. Perfusion reserve is one of the significant prognostic factors (1), and therefore, evaluation of perfusion reserve is critical when planning surgery. Furthermore, assessment of the efficacy of an EC/IC bypass is also important. Schmiedek et al. evaluated perfusion reserve both before and after an EC/IC bypass and reported that the acetazolamide-challenged perfusion was improved whereas the basal perfusion remained unchanged (5). However, in the case of moyamoya disease, another type of cerebrovascular disease, many authors reported that both basal perfusion and perfusion reserve improved after bypass surgery (18,21–23).
Cerebral perfusion and perfusion reserve can be evaluated on basal/acetazolamide brain perfusion SPECT using 133Xe, 123I-isopropyliodoamphetamine, 99mTc-HMPAO, or 99mTc-ethylcysteinate dimer (6–8). However, most studies have been interpreted by visual assessment, which is dependent on the expertise of the physician. Although visual assessment of brain perfusion SPECT is considerably reliable, its objectivity and reproducibility are limited (10). Furthermore, the visual evaluation may be dichotomous—say, with an improvement or aggravation in follow-up studies. Some have used the classic ROI method, in which ROIs are drawn manually, as a way to solve this limitation. But this method has shown significant intraobserver and interobserver variation (11,24).
In this study, SPM and a probabilistic brain atlas were adopted for objective and quantitative evaluation of brain perfusion SPECT. The process of spatial normalization enables a voxel-based statistical comparison of brain images with different morphologies, and the probabilistic brain atlas enables an objective drawing of ROIs. However, because originally developed for neurocognitive studies, in which brains have normal structures, those methods have limitations when applied to studies of brain infarction or cerebral ischemia, images of which show exaggerated deterioration.
This study adopted a protocol of 1-d consecutive acquisitions. Although acquisition of basal and acetazolamide SPECT images on separate days is recommended (25), the 1-d protocol can provide images of satisfactory quality, with an optimized protocol (11,17). With the 1-d protocol, basal and acetazolamide SPECT are performed consecutively, with no change in the position of the patient. The spatial coordinates between the basal and acetazolamide images use the same conditions. Therefore, the same transforming parameters used for the basal image can also be applied to the acetazolamide image. The use of the same transforming parameters is beneficial in an analysis using SPM or a probabilistic brain atlas, as the calculation of the transforming parameters for the acetazolamide images is less reliable because of the greater deterioration of the images.
With such an improved method, SPM and the probabilistic brain atlas worked effectively in this study. The analysis showed the effects of surgery for both the extent and the severity of the perfusion abnormality. Improvement in perfusion and perfusion reserve in the matched territory of the MCA was objectively observed, and residual abnormality in the perfusion reserve, despite the normalized basal perfusion, was also observed. This result is quite physiologic, considering that perfusion reserve is a more sensitive indicator of hemodynamic status. Moreover, the analysis of 1 patient with a perioperative infarct correctly demonstrated a decrease in the counts.
In addition to providing objectivity, SPM and probabilistic brain atlas as analytic methods provide the advantages of quantitative data, especially with regard to both extent and severity. The methods can also easily be applied to other parametric images of absolute values to find the extent and severity of differences in group images compared with control group images, or of differences in the images of an individual who serves as his or her own control.
CONCLUSION
In this study, the efficacy of an EC/IC bypass in cerebrovascular disease was evaluated using SPM and a probabilistic brain atlas. Despite the putative difficulties, image processing and analysis were effective, and the results correlated well with physiologic reasoning. This study demonstrated good applicability of SPM and the probabilistic brain atlas in analyzing images of cerebrovascular disease.
Acknowledgments
This study was supported by the Korean Ministry of Science and Technology. Basal/acetazolamide SPECT studies at our institution were initially made possible by the generous encouragement of Dr. Kohei Hayasida of the National Cardiovascular Center of Japan.
Footnotes
Received Apr. 24, 2003; revision accepted Oct. 9, 2003.
For correspondence or reprints contact: Dong Soo Lee, MD, Department of Nuclear Medicine, Seoul National University College of Medicine, 28 Yeongeon-dong, Jongno-gu, 110-744, Seoul, Korea.
E-mail: dsl{at}plaza.snu.ac.kr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-Term Outcomes After Combined Revascularization Surgery in Adult Moyamoya Disease
- Hypoperfusion and Ischemia in Cerebral Amyloid Angiopathy Documented by 99mTc-ECD Brain Perfusion SPECT
- The Acetazolamide Challenge: Techniques and Applications in the Evaluation of Chronic Cerebral Ischemia
- Subcortical Aphasia After Striatocapsular Infarction: Quantitative Analysis of Brain Perfusion SPECT Using Statistical Parametric Mapping and a Statistical Probabilistic Anatomic Map
- Prediction of the Clinical Outcome of Pediatric Moyamoya Disease With Postoperative Basal/Acetazolamide Stress Brain Perfusion SPECT After Revascularization Surgery